

Abstract
Objectives:
Many studies to evaluate the accuracy of root fracture diagnosis have been conducted. However, there is a scarcity of studies to assess the quality and the sources of heterogeneity in the literature. For this reason, the aim of this study was to conduct systematic reviews and meta-analyses to summarize the available evidence on detection of root fractures by cone beam CT (CBCT) and periapical radiograph (PR) images and the interference of artefact by investigating possible sources of heterogeneity.
Methods:
Studies reporting root fracture detection, from January 2010 to February 2016, were selected. All selected studies were subjected to selection criteria and then, comparative and qualitative analyses by using the quality assessment of diagnostic accuracy studies (QUADAS-2) tool were performed. Pooled sensitivity, specificity and diagnostic odds ratios were calculated. Also, receiver operator characteristics (ROC) curves were built to summarize the results. SROC curve analyses were performed to investigate the heterogeneity among studies.
Results:
Initially, 799 articles were selected. After screening titles and abstracts, 743 articles were excluded. After reading the remaining 56 full-texts, 47 relevant articles were included in this study. Diagnostic odds ratio values revealed a wide range of results across the studies and determined a higher heterogeneity for PR compared with CBCT. The analyses of the SROC curves compared CBCT imaging versus PR in the diagnosis of root fracture, favouring CBCT modality.
Conclusions:
CBCT was the imaging exam that rendered a higher diagnostic accuracy for root fractures.
Keywords: cone-beam computed tomography, imaging diagnosis, root fracture
Introduction
Root fractures are a type of dental damage with unfavourable prognosis,1 which increases the importance of precise initial diagnosis. In some cases, the endodontist first identifies or suspects the presence of fracture in a clinical exam. However, it is necessary to ascertain the extension (complete or incomplete) and direction (horizontal or vertical) of the root fracture. The fracture may involve both proximal surfaces or just involve one proximal surface2 and the radiographic examination should be used to establish this information.3
Periapical radiographs (PRs) are the most used imaging modalities. However, the X-ray beam needs to be set at the same angle of the root fracture line in order to become visible.4 Since this method is suitable in many cases, many authors suggest doing a PR exam with two or three different angles in order to confirm the correct orthogonal angulation fracture line.5–9 On the other hand, cone beam CT (CBCT) images are tridimensional exams, presenting the entire volume for that patient,10 without superimposing anatomic structures over the teeth. This exam gives a perception of dimension and allows the maxillofacial radiologist (MFR) to perform a complete diagnosis of pathologies, facial fractures, surgical planning and root fractures.11 An important disadvantage of CBCT is the artefact interference induced by metallic objects such as metallic posts,12 restorative materials13 and dental implants.14,15 This interference is commonly referred as metallic artefact (MA).
Several studies have evaluated the accuracy of root fracture diagnosis by CBCT and PR, and the range of reported results has been extensive. The data were conflicting: the majority was pro CBCT and a minority was against this imaging method. This discrepancy may be related to different types of tomography equipment used for the researches, presence of artefact in CBCT images, different angulations for PR and the methods used to simulate root fracture for in vitro studies.
Many studies reported a decrease in root fracture diagnosis accuracy in the presence of metallic posts 12,16,17 and endodontic fillings.7,13,18–20 These circumstances may cause artefacts that seriously impair the quality of CBCT images.17 Artefacts are represented by radiopaque, radiolucent and bright tracks that can overlap the tooth root and mimic root fractures.1
Considering that a large number of studies performed root fractures diagnosis and the controversies found among their results, systematic reviews are useful to provide the best evidence on a subject based on the available scientific literature.21 Some previous systematic reviews have investigated this issue.22–24 Nevertheless, one of them has only included vertical root fractures,24 and another one has analysed only clinical studies.22 Recognizing the importance of providing a wider overview on the evidence for diagnosis of root fractures, a meta-analysis on accuracy of relevant methods could be interest to summarize available data about relevant tests. This summary could be helpful in choosing the best modality of imaging exam in order to correctly detect root fracture and it is one of the first steps when investigating diagnostic tests.25 Additionally, possible sources of variability in the methodology of studies could be explored in order to understand the impact of these options in the pooled findings. To the best of our knowledge, this evidence is not available for studies on detection of root fractures.
Therefore, the aim of this study was to synthesize the findings concerning the accuracy of detecting root fractures by imaging diagnose and the interference of artefacts through conducting a systematic review including a meta-analysis and analysis of sources of heterogeneity, investigating possible factors that may influence the performance of the method and evaluate the accuracy of each imaging method. For this systematic review, both types of root fracture (horizontal and vertical) and both in vivo, in vitro and ex vivo studies were considered.
Methods and Materials
To report this review, PRISMA guidelines26 were adopted. The following sections describe the specific methodological aspects of the review. This review was registered with the National Institute for Health Research PROSPERO, International Prospective Register of Systematic Reviews (http://www.crd.york.ac.uk/PROSPERO, registration number CRD42015023521).
Search strategy
Studies reporting root fracture diagnosis by using imaging exam published in Medline, Scopus, Lilacs and Scielo databases were searched. The selection included studies from January 2010 to February 2016.
The PubMed search strategy included a combination of the MeSH terms and text word described as follows: (((((((“cone-beam computed tomography” [MeSH Terms] OR Cone beam computed tomography [Text Word]) OR CBCT [Text Word] OR cone-beam CT [Text Word] OR cone beam CT [Text Word] OR cone-beam [Text Word] OR cone beam [Text Word]) AND root fracture [Text Word]) OR root fractures [Text Word]) OR endodontic fillings[Text Word]) OR canal sealer [Text Word]) OR tooth endodontically treated [Text Word]) OR endodontic treatment [Text Word]. For other databases, this strategy was adapted using appropriate Boolean strategies.
Studies were screened according to the selection criteria. In addition, references of the included articles were also checked manually. Duplicate studies among databases results were manually eliminated.
Evaluated studies and search criteria
The types of study considered eligible for this review were in vivo, in vitro and ex vivo studies. Studies were included if they reported outcomes related to performance of root fracture diagnosis by using CBCT, and if they had been written in English.
Follow-up reports, case reports, narrative review as well as those papers that did not report any data related to the CBCT accuracy (sensitivity, specificity, false and negative values or any data that permit calculation of performance parameters) for the detection of root fractures.
Outcome measures
Outcomes were measured through the assessment of accuracy and/or performance of root fracture diagnosis with or without artefact in CBCT and PR images. When that information was not provided by the study, the authors collected true positive, true negative, false positive and false negative data for accuracy estimative of the methods.
Assessment of validity and data extraction
Two independent reviewers (FCSS and SKV) screened the titles and abstracts of the eligible studies for subject relevance. Studies that could not be definitely excluded based on abstract information were also selected for full text screening.27 When agreement could not be reached after all the inclusion criteria were fulfilled, a third researcher (MGPC) decided if the study was eligible, based on the same criteria of inclusion and exclusion previously described. The full text screening was conducted following the same methodology that was proposed for the title and abstract screening.
The observer extracted the recorded data from each selected study and categorized them on structured table (Supplementary Table 1, supplementary material available online) as follows: sample size, root fracture type (horizontal or vertical, and complete or incomplete), root fracture’s induction methodology (for laboratorial studies or clinical condition for clinical studies), the analysed images parameters [including voxel size, field of view (FOV) and tube voltage/current, when these date were available at the study], observer’s professional experience (MFR, endodontist, if the observer was trained and calibrated, or non-reported), analyses imaging methods (multiplanar reconstructed images from CBCT, more than one PR image and slides presentation) and conclusions.
Risk of bias of individualsstudies
QUADAS-2 (Quality Assessment of studies of Diagnostic Accuracy-2)28 was applied to articles included in the final analysis in order to evaluate the risk of bias of the studies. Two examiners (FCSS and SKV) assessed each study and when agreement could not be reached a third examiner (MGPC) was invited to decide if the article was qualified for the systematic review.
The QUADAS-2 (University of Bristol Resource, Bristol, UK) tool was established upon four domains: patient selection, index test, reference standard, and flow and timing.28 These domains were evaluated in two categories: risk of bias and applicability concerns. Each item had to be answered and scored as low risk “−” (negative answers), unclear “?”(missing information) and high risk “+” (positive answers).
Statistical methods for the meta-analysis
All included studies were carefully read in full, in order to ensure that they presented a clearly defined reference standard (gold standard).Also, in order to perform a meta-analysis, these studies had to report absolute numbers of the true positives, false positives, true negatives and false negatives and/or provided sufficient information to obtain these data.
Meta-Disc software29 (Ramón y Cajal Hospital, Madrid, Spain) was used to perform the analyses. The meta-analyses used random-effect models, and the source of heterogeneity (analysis) used two indexes: Cochran’s Q and I-Square.
All the meta-analyses and source of heterogeneity analysis were performed considering the subgroups as CBCTs and PRs, presence or absence of artefacts in CBCT and PR and the experience of the observers (MFR and endodontist).
The ROC curve space (SROC) analysis was performed using the R version 0.99.902 combined with the Mada package, version 3.5–0 (R Foundation for Statistical Computing, Vienna, Austria) to compare the effect of methodological differences related to the distinct variables by subgroups: presence and absence of artefacts for CBCT and for PR, CBCT vs PR, the influence of type of root fracture (horizontal root fracture vs vertical root fracture) and comparison between MFR and endodontist.
Results
Study selection
The initial database search found 797 articles, as showed on the flow diagram (Figure 1). The manual search resulted in two additional studies. After removing duplication and the title and abstract screening according to the inclusion and exclusion criteria, 743 articles were excluded. Then, the full-texts of the 56 eligible articles were assessed. All in all, 47 articles were included in the systematic review.
Figure 1.

Flow diagram.
Nine articles did not concern with the scope of this study. Four of these were systematic reviews, five were focused on root fracture treatment, and the last one was a letter response from a previous study.
Study characteristics
The vast majority of studies were in vitro or ex vivo studies that simulated the root fractures as the gold standard by applying a mechanical force with a hammer or using a universal testing machine (Instron®, Norwood, MA). Only three studies consisted of in vivo situations and their reference standard were surgical procedures or clinical findings.30–32
The specimens for all the studies developed complete root fractures and two of the studies5,20 entailed the execution of both incomplete and complete root fractures. These studies5,20 did not obtain good accuracy levels for incomplete root fracture.
The studies worked with 14 different types of tomography devices. The most frequently selected equipment was i-CAT (Imaging Sciences International, Hatfield, PA) using all possible protocols for 13 studies, 3D Accuitomo 170 (J Morita Mfg. Corp., Kyoto, Japan) for 12 studies and NewTom Scanner (Quantitative Radiology, Verona, Italy) for eleven studies.
Risk of bias within studies
In assessing the quality of the 47 selected articles according to QUADAS-2 (Figure 2), the great majority (almost 80% of the studies) presented a low risk of bias in the domain related to patient selection, to the reference standard and to flow and timing. However, the performance and interpretation of the index test in almost 20% of the studies was unclear (meaning that there were no concerns regarding the applicability of this topic).
Figure 2.

QUADAS-2 domain.
Results of individual studies
In general, sensitivity and DOR values were higher for CBCT than PR. Table 1 summarizes the pooled sensitivities and specificities with their 95%confidence intervals (CI). Studies were grouped by presence or absence of artefact: for CBCT, for PR, for type of fracture (horizontal or vertical root fracture), and experience of the observer (maxillofacial radiologist—MFR and endodontist).
Table 1.
Pooled sensitivity, specificity and DOR for the studies
| Pooled sensitivity 95% IC |
Inconsistency (I-square)b |
Q-Cochran p valuea | Pooled specificity 95% IC |
Inconsistency (I-square)b |
Q-Cochran pvaluea | Pooled DOR 95% IC |
Inconsistency (I-square)b |
Q-Cochran p valuea | |
|---|---|---|---|---|---|---|---|---|---|
| CBCT with MA | 0.73 (0.70 to 0.76) | 79.4% | 0.002 | 0.72 (0.69 to 0.75) | 83.1% | <0.001 | 6.60 (3.65 to 11.95) | 80.4% | <0.001 |
| CBCT without MA | 0.82 (0.79 to 0.84) | 87.2% | <0.001 | 0.88 (0.86 to 0.91) | 68.5% | <0.001 | 39.05 (17.96 to 84.88) | 80.2% | <0.001 |
| PR with MA | 0.47 (0.42 to 0.53) | 91.9% | <0.001 | 0.91 (0.87 to 0.94) | 82.5% | 0.001 | 14.13 (4.85 to 41.16) | 61.7% | 0.004 |
| PR without MA | 0.51 (0.45 to 0.56) | 91.5% | <0.001 | 0.91 (0.86 to 0.94) | 68.3% | 0.012 | 15.53 (7.41 to 32.52) | 25.8% | 0.185 |
| VRF with MA | 0.56 (0.53 to 0.59) | 95.9% | <0.001 | 0.54 (0.50 to 0.57) | 95.5% | <0.001 | 3.72 (1.63 to 8.48) | 88.5% | <0.001 |
| VRF without MA | 0.47 (0.44 to 0.50) | 97.3% | <0.001 | 0.49 (0.45 to 0.52) | 97.2% | <0.001 | 35.83 (13.07 to 98.21) | 83.8% | <0.001 |
| HRF with MA | 0.26 (0.20 to 0.33) | 74.1% | <0.001 | 0.31 (0.25 to 0.39) | 95.7% | <0.001 | 1.15 (0.13 to 10.34) | 88.5% | <0.001 |
| HRF without MA | 0.93 (0.75 to 0.87) | 66.8% | 0.006 | 0.86 (0.80 to 0.90) | 73.7% | 0.001 | 22.15 (4.65 to 105.51) | 81.8% | <0.001 |
| MFR | 0.83 (0.80 to 0.86) | 76.8% | <0.001 | 0.85 (0.82 to 0.88) | 74.5% | <0.001 | 31.74 (14.14 to 71.25) | 80.1% | <0.001 |
| Endodontists | 0.66 (0.59 to 0.73) | 90.2% | <0.001 | 0.83 (0.77 to 0.89) | 87.7% | <0.001 | 13.30 (2.15 to 82.12) | 86.7% | <0.001 |
DOR, diagnostic odds ratio; HRF, horizontal root fracture; MA,metallic artefact; MFR,maxillofacial radiologist; VRF,vertical root fracture.
Test for heterogeneity.
Level of inconsistency.
Sensitivity and specificity values for CBCT in the presence of MA were lower than for CBCT in the absence of MA (Table 1). Both situations presented a high level of inconsistency.
Specificity values for PR in the presence or absence of MA were similar and sensitivity values were lower for PR in the presence of MA (Table 1). PR presented higher values of inconsistency than CBCT.
Figure 3 shows SROC curves for CBCT and PR in the presence of MA individually. It is possible to observe a wide range of results across the studies with a tendency to higher sensitivity than specificity values in the diagnosis of root fracture by CBCT imaging. In addition, we noticed a tendency of higher sensitivity and specificity values favouring CBCT.
Figure 3.

Summary ROCcurves for detection of root fractures using cone beam CT and periapical radiographs with and without metallic artefacts, as well as, performed by maxillofacial radiologists or endodontists (SROC: central curve; other curves: upper and lower limits of confidence).
It is import to emphasize the difference between the area under the curve (AUC) for CBCT with MA (AUC = 0.783) and CBCT without MA (AUC = 0.936). The difference between the AUC for PR with MA (AUC = 0.870) and PR without MA (AUC = 0.884) was small.
Figure 4 shows the comparison of the SROC curves considering determined subgroups. The comparison between CBCT AUC in the presence of MA and CBCT AUC in the absence of MA resulted in a smaller area at the former subgroup. Also, CI is larger for the curve in the presence of MA. For PR values, the same behavior was observed. SROC values were lower in the presence of MA. However, similar values could be observed for PR in presence or absence of MA (Figure 4).
Figure 4.
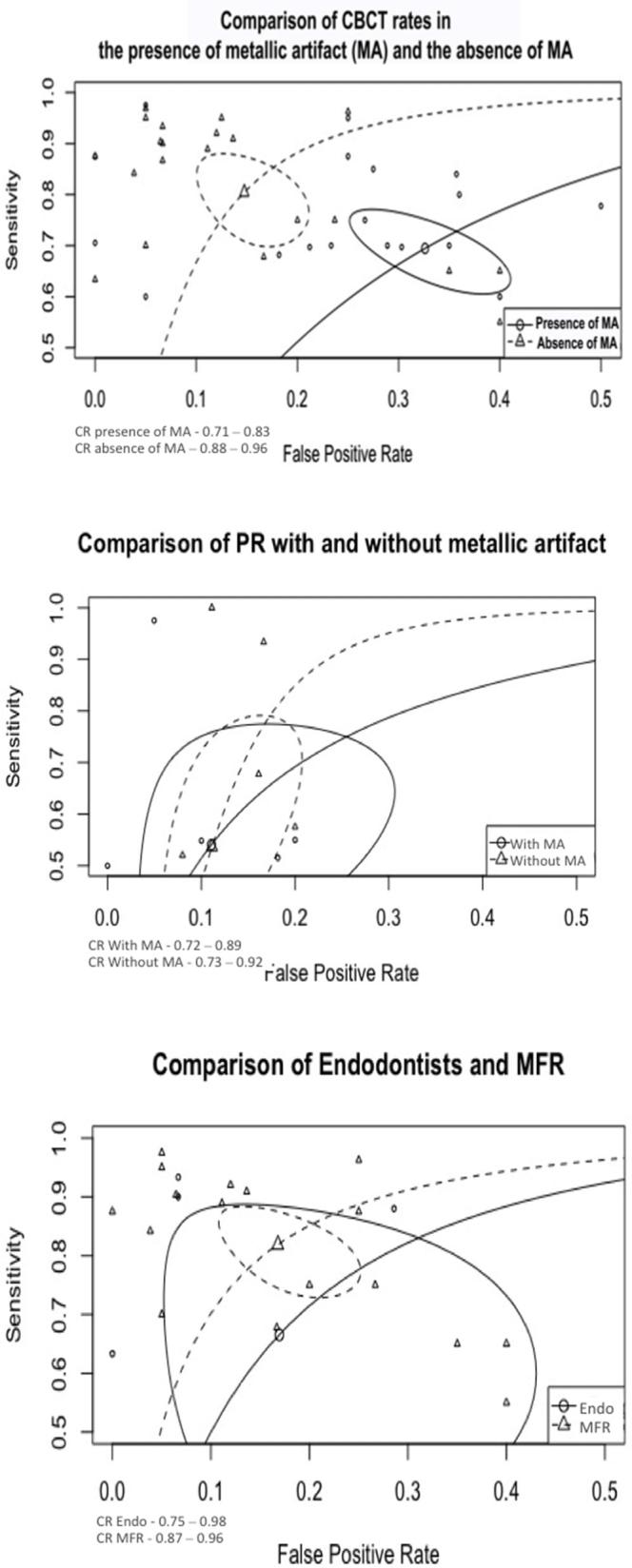
Comparison of summary ROC curves considering: cone beam CT with metallic artefacts vs without metallic artefacts; periapical radiograph with metallic artefacts vs without metallic artefacts and, maxillofacial radiologists vsendodontists performances for detecting root fractures. (Circles related to the curves demonstrate their respective confidence regions (CR).
The observer’s experience demonstrated similar values for specificity and a wide variation for sensitivity (Table 1). The SROC curve for MFR (Figure 3) presented a tendency to higher sensitivity values in root fracture diagnosis than the SROC curve for endodontist. AUC for both endodontist and MFR produced similar numerical results. However, SE (AUC) presented distinct variations when comparing MFR [SE (AUC = 0.025)] and endodontist [SE (AUC = 0.095)] confidence regions (Figure 3). The SROC illustrated the difference between the curves and the extensive confidence regions, corroborating the higher percentage of inconsistency (Figure 4, Table 1).
Additional analysis
The effect on the type of root fracture demonstrated a better performance in the absence of MA and higher level of inconsistency for both types of root fracture (Table 1). The sensitivity and specificity did not influence in the accuracy of root fracture detection. This evaluation criterion agrees with our inclusion criteria (not discriminative according to the type of fracture).
Discussion
All studies included in this review fostered a regard not only with radiation dosage but also with diagnosis accuracy. The ALARA principle must be a concern in the treatment of patients; however, the correct diagnosis influences this principle and some authors have accepted the ALADA (“as low as diagnostically acceptable”)33 concept instead.
We decided to insert horizontal and vertical root fracture without discriminating them since clinically it is not possible to predetermine the type of root fracture that the dentist will detect and consequently treat. Following the results of the meta-analyses, a similar performance for the detection of horizontal and vertical root fracture was observed, corroborating there is no negative impact of analysing data of all types of fracture in conjunction. Another methodological option was to select studies starting in 2010. Before this period, CBCT scan technology was not always available to the clinician in his region. Also, after 2010 we observed an increase in the number of studies adopting CBCT.
Most CBCT machines allow for numerous possibilities of acquisition protocols. Proper selection of these protocols is very important in order to obtain high quality and diagnostically appropriate images.11,34 3D Accuitomo 170 (J Morita Mfg. Corp., Kyoto, Japan) and PreXion (Terarecon, San Mateo, CA) were used to evaluate volumes with a higher number of frames in several studies.5,6,12,20,32,35 Images with more frames increased the radiation dose but gave more information about the area of interest. Consequently, a higher number of projections influences positively on the accuracy level.12 Picasso Trio (E-WOO, Giheung-gu, Republic of Korea), Picasso Trio (Vatech, Hwaseong, South Korea), ProMax® (Planmeca, Helsinki, Finland), Master 3D (Vatech, Hwaseong, South Korea) were used for three studies to analyse the AR (artifacts reduction algorithm) tool.18,36,37 These studies observed that accuracy levels decreased in the presence of this tool. The original image protocol of acquisition in these studies obtained better results.
Some authors used different types of protocols to analyse CBCT performance, thereby testing different voxel and FOV sizes, kVp and mA influence, as well as filters in post-acquisition time.1,5–7,12,31,35,38–45 The authors that applied different sizes of voxel and FOV observed that images with a smaller voxel size rendered better accuracy levels,1,5–8,30,31,35,37,40–43,45 and that voxel and FOV sizes had to be proportionally related.1
Different of diagnostic studies, intervention studies contain a randomization, a hard design and specific outcomes. However, diagnostic studies contain multiple sample variation and aspect that interfere on the heterogeneity. Possible sources of heterogeneity were not identify in previous systematic reviews.22,23 Trying to lead to the heterogeneity, we performed subgroup analysis according to other specifications, such as presence or absence of metallic artefact, imaging exam type, observer experience and fracture type. By doing this, it was possible to analyse each item independently. Table 1 shows that all groups mostly presented a higher percentage of inconsistence (I-square value) and a significant p value, revealing probably these circumstances were not the main responsible for heterogeneity of studies and they should be more related to different protocols, different equipment and methodologies assumed by different studies.
A large number of studies analysed the influence of artefact interference, such as metallic post and endodontic fillings or both, by using CBCT images. Only two articles quantified such interference in CBCT images; one used a method to evaluate the white and black strikes,13 and the other evaluated image density.36 The remaining articles evaluated the influence of artefact interference on the accuracy of root fracture diagnosis. It was observed that a decrease of CBCT accuracy levels occurred in the presence of an artefact.1,7,8,19,20,30–32,37,39,41–48 The pooled accuracy values (AUC) were similar, sensitivity presented close values (0.73 for presence of artefact and 0.82 for absence of artefact), and specificity presented higher values in the absence of artefact (0.88) when compared with analyses with the presence of artefact (0.72). Artefacts seem to decrease both the sensitivity and specificity in approximately 10%. However, the DOR without artefacts is fivefold higher when artefacts are present.
Artefact strikes spread mainly along the axial plane.11 As a result, observers had greater difficulty in analysing axial plane images, thereby making it necessary to also evaluate coronal and sagittal planes images to differentiate the root fracture line from the artefact. It is important to point out that many studies did not use these images on three planes in the software to analyse the CBCT imaging. Two studies employed a Power Point presentation for the observer to perform analyses.5,20 When the authors used this type of analysis, studies had a higher risk of bias because the observer normally evaluates just a single image of the CBCT volume, while the operator who created the Power Point presentation could induce some answers in the process.
Based on inclusion criteria, all studies analysed CBCT images and other types of images. Only one study49 did not report better results using CBCT. In this study, the authors concluded that PRs demonstrated fewer false positive cases (high specificity). In Table 1, the I-square for the inconsistency analysis illustrated higher values for PR on pooled sensitivity than on pooled specificity. Imaging exams with high specificity may not identify some true-positive cases, mostly in the cases with metallic artefact. However, some studies5,39 demonstrated that by performing two or more different angulations in PR might increase this exam accuracy.
Two studies8,9 performed in vitro experiments, demonstrating that CBCT imaging obtained higher scores in detecting vertical root fractures when compared to PR. Nevertheless, these results were not statistically significant. Thus, the authors suggested that the PR should be the first imaging modality to assess the presence or absence of a root fracture. Figure 3 shows a slight decrease on AUC for PR in presence of metallic artefact than CBCT, this occurred by the larger CI. That means that the diagnostic of root fractures by using PR images suffer less artefact interference than CBCT images. If the PR was not efficient to identify the root fracture, the CBCT exam is the exam that could execute detailed analysis.
Concerning with the risk of bias among the selected studies, we decided to use the QUADAS-2 assessment because we intended to evaluate the accuracy of diagnostic method and we could comprehend the studies according to four different domains (patient selection, index test and reference standard flow and timing).
One in vivo study50 in which a risk of bias was observed in the QUADAS-2 assessment (Figure 2), the authors suggested relating clinical examination to the image aspects. The in vivo study did not use a gold standard to compare its findings; in most cases, a mucoperiosteal flap was performed to evaluate if a fracture was present. However, it is possible that in this study the fracture line might be located on another root face that was not exposed during surgery. In other cases, a dental extraction was performed. However, tooth removal may induce a root fracture and result in false-positive cases.
In vitro studies carry the risk of bias for inducing root fractures. It is important for in vitro studies to simulate situations that provide useful information to the clinical practice. Two authors induced a root fracture sectioning each tooth by using diamond-coated steel discs,38,41 which resulted in wide and regular lines of fracture, quite different than fractures found at in vivo situations. At other in vitro studies, the operator induced root fractures by applying force with the aid of a hammer1,12,49 or a universal machine,5,51,52 simulating more irregular and thin lines of fracture.
Selection bias by observers is also a possibility to be considered. The observer’s experience and area of expertise can significantly influence results. Patel et al20 and Jones et al38 only selected examiners with endodontics expertise and accuracy results for CBCT imaging and PR were equal. However, some studies selected radiologists or professionals from two areas of expertise (radiology and endodontics), which were able to discern the high accuracy on CBCT imaging and the high specificity of PR.
The observers’ experience resulted in higher numbers of true positives cases for MFRs than for endodontists. For the inconsistency analysis, it was observed an inferior percentage for MFRs than for endodontists. The amount of selected studies did not represent a good number for meta-regression analysis and the number of observers was different between MFRs and endodontists.
Conclusion
The present study demonstrated the variations in the report of detection of root fractures established by imaging diagnosis. Based on these data, CBCT imaging rendered a higher sensitivity and DOR values for root fractures. In addition, the presence of artefacts as metallic posts or endodontic fillings should serve as alert for choosing the correct exam and protocol because the artefact interference could slightly affect the diagnosis accuracy of root fractures in CBCT images. This implies that the selection of an appropriate imaging exam is a critical factor for detection of root fractures.
Acknowledgments
Supported by the CNPq, Brasília, Brazil (Research Productivity Scholarship grant no. 303847/2009-3, and Universal Research Project grant no. 472895/2009-5 to Marcelo Cavalcanti; Master scholarship to Solange Velasco). CAPES, Brasília, Brazil (PhD scholarship to Fernanda Salineiro).
Contributor Information
Fernanda Cristina Sales Salineiro, Email: f.salineiro@usp.br.
Solange Kobayashi-Velasco, Email: solangekv@usp.br.
Mariana Minatel Braga, Email: mmbraga@usp.br.
Marcelo Gusmão Paraiso Cavalcanti, Email: mgpcaval@usp.br.
References
- 1.Salineiro FC, Pinheiro LR, dos Santos Júnior O, Cavalcanti MG. Detection of horizontal root fracture using four different protocols of cone-beam computed tomography. Braz Oral Res 2015; 29: 1–6. doi: https://doi.org/10.1590/1807-3107BOR-2015.vol29.0067 [DOI] [PubMed] [Google Scholar]
- 2.Rivera E, Walton ER. Cracking the cracked tooth code: detection and treatment of Various Longitudinal tooth fractures. Endodontics 2008: 2–7. [Google Scholar]
- 3.Orhan K, Aksoy U, Kalender A. Cone-beam computed tomographic evaluation of spontaneously healed root fracture. J Endod 2010; 36: 1584–7. doi: https://doi.org/10.1016/j.joen.2010.04.004 [DOI] [PubMed] [Google Scholar]
- 4.Iikubo M, Kobayashi K, Mishima A, Shimoda S, Daimaruya T, Igarashi C, et al. Accuracy of intraoral radiography, multidetector helical CT, and limited cone-beam CT for the detection of horizontal tooth root fracture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009; 108: e70–e74. doi: https://doi.org/10.1016/j.tripleo.2009.07.009 [DOI] [PubMed] [Google Scholar]
- 5.Brady E, Mannocci F, Brown J, Wilson R, Patel S. A comparison of cone beam computed tomography and periapical radiography for the detection of vertical root fractures in nonendodontically treated teeth. Int Endod J 2014; 47: 735–46. doi: https://doi.org/10.1111/iej.12209 [DOI] [PubMed] [Google Scholar]
- 6.Avsever H, Gunduz K, Orhan K, Uzun I, Ozmen B, Egrioglu E, et al. Comparison of intraoral radiography and cone-beam computed tomography for the detection of horizontal root fractures: an in vitro study. Clin Oral Investig 2014; 18: 285–92. doi: https://doi.org/10.1007/s00784-013-0940-4 [DOI] [PubMed] [Google Scholar]
- 7.Khedmat S, Rouhi N, Drage N, Shokouhinejad N, Nekoofar MH. Evaluation of three imaging techniques for the detection of vertical root fractures in the absence and presence of gutta-percha root fillings. Int Endod J 2012; 45: 1004–9. doi: https://doi.org/10.1111/j.1365-2591.2012.02062.x [DOI] [PubMed] [Google Scholar]
- 8.da Silveira PF, Vizzotto MB, Liedke GS, da Silveira HL, Montagner F, da Silveira HE. Detection of vertical root fractures by conventional radiographic examination and cone beam computed tomography – an in vitro analysis. Dent Traumatol 2013; 29: 41–6. doi: https://doi.org/10.1111/j.1600-9657.2012.01126.x [DOI] [PubMed] [Google Scholar]
- 9.Kambungton J, Janhom A, Prapayasatok S, Pongsiriwet S. Assessment of vertical root fractures using three imaging modalities: cone beam CT, intraoral digital radiography and film. Dentomaxillofac Radiol 2012; 41: 91–5. doi: https://doi.org/10.1259/dmfr/49798768 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Scarfe WC, Li Z, Aboelmaaty W, Scott SA, Farman AG. Maxillofacial cone beam computed tomography: essence, elements and steps to interpretation. Aust Dent J 2012; 57(Suppl 1): 46–60. doi: https://doi.org/10.1111/j.1834-7819.2011.01657.x [DOI] [PubMed] [Google Scholar]
- 11.Cavalcanti MGP. Cone beam computed tomographic imaging. J Craniofac Surg 2012; 23: 279–82. doi: https://doi.org/10.1097/SCS.0b013e318241ba64 [DOI] [PubMed] [Google Scholar]
- 12.Costa FF, Pinheiro LR, Umetsubo OS, dos Santos O, Gaia BF, Cavalcanti MG. Influence of cone-beam computed tomographic scan mode for detection of horizontal root fracture. J Endod 2014; 40: 1472–6. doi: https://doi.org/10.1016/j.joen.2014.03.001 [DOI] [PubMed] [Google Scholar]
- 13.Brito-Júnior M, Santos LA, Faria-e-Silva AL, Pereira RD, Sousa-Neto MD. Ex vivo evaluation of artifacts mimicking fracture lines on cone-beam computed tomography produced by different root canal sealers. Int Endod J 2014; 47: 26–31. doi: https://doi.org/10.1111/iej.12121 [DOI] [PubMed] [Google Scholar]
- 14.Pinheiro LR, Scarfe WC, Augusto de Oliveira Sales M, Gaia BF, Cortes AR, Cavalcanti MG. Effect of Cone-Beam computed tomography field of view and acquisition frame on the detection of chemically simulated peri-implant bone loss in vitro. J Periodontol 2015; 86: 1159–65. doi: https://doi.org/10.1902/jop.2015.150223 [DOI] [PubMed] [Google Scholar]
- 15.Benic GI, Sancho-Puchades M, Jung RE, Deyhle H, Hämmerle CH. In vitro assessment of artifacts induced by titanium dental implants in cone beam computed tomography. Clin Oral Implants Res 2013; 24: 378–83. doi: https://doi.org/10.1111/clr.12048 [DOI] [PubMed] [Google Scholar]
- 16.Costa FF, Gaia BF, Umetsubo OS, Pinheiro LR, Tortamano IP, Cavalcanti MG. Use of large-volume cone-beam computed tomography in identification and localization of horizontal root fracture in the presence and absence of intracanalmetallic post. J Endod 2012; 38: 856–9. doi: https://doi.org/10.1016/j.joen.2012.03.011 [DOI] [PubMed] [Google Scholar]
- 17.Costa FF, Gaia BF, Umetsubo OS, Cavalcanti MG. Detection of horizontal root fracture with small-volume cone-beam computed tomography in the presence and absence of intracanalmetallic post. J Endod 2011; 37: 1456–9. doi: https://doi.org/10.1016/j.joen.2011.05.040 [DOI] [PubMed] [Google Scholar]
- 18.de Rezende Barbosa GL, Sousa Melo SL, Alencar PN, Nascimento MC, Almeida SM. Performance of an artefact reduction algorithm in the diagnosis of in vitro vertical root fracture in four different root filling conditions on CBCT images. Int Endod J 2016; 49: 500–8. doi: https://doi.org/10.1111/iej.12477 [DOI] [PubMed] [Google Scholar]
- 19.Moudi E, Haghanifar S, Madani Z, Alhavaz A, Bijani A, Bagheri M. Assessment of vertical root fracture using cone-beam computed tomography. Imaging Sci Dent 2014; 44: 37–41. doi: https://doi.org/10.5624/isd.2014.44.1.37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Patel S, Brady E, Wilson R, Brown J, Mannocci F. The detection of vertical root fractures in root filled teeth with periapical radiographs and CBCT scans. Int Endod J 2013; 46: 1140–52. doi: https://doi.org/10.1111/iej.12109 [DOI] [PubMed] [Google Scholar]
- 21.Gimenez T, Piovesan C, Braga MM, Raggio DP, Deery C, Ricketts DN, et al. Visual Inspection for Caries detection: a Systematic review and Meta-analysis. J Dent Res 2015; 94: 895–904. doi: https://doi.org/10.1177/0022034515586763 [DOI] [PubMed] [Google Scholar]
- 22.Long H, Zhou Y, Ye N, Liao L, Jian F, Wang Y, et al. Diagnostic accuracy of CBCT for tooth fractures: a meta-analysis. J Dent 2014; 42: 240–8. doi: https://doi.org/10.1016/j.jdent.2013.11.024 [DOI] [PubMed] [Google Scholar]
- 23.Chang E, Lam E, Shah P, Azarpazhooh A. Cone-beam computed tomography for detecting vertical root fractures in endodontically treated teeth: a systematic review. J Endod 2016; 42: 177–85. doi: https://doi.org/10.1016/j.joen.2015.10.005 [DOI] [PubMed] [Google Scholar]
- 24.Corbella S, Del Fabbro M, Tamse A, Rosen E, Tsesis I, Taschieri S. Cone beam computed tomography for the diagnosis of vertical root fractures: a systematic review of the literature and meta-analysis. Oral Surg Oral Med Oral Pathol Oral Radiol 2014; 118: 593–602. doi: https://doi.org/10.1016/j.oooo.2014.07.014 [DOI] [PubMed] [Google Scholar]
- 25.Sackett DL, Haynes RB. The architecture of diagnostic research. BMJ 2002; 324: 539–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 2009; 6: e1000100. doi: https://doi.org/10.1371/journal.pmed.1000100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Giro G, Chambrone L, Goldstein A, Rodrigues JA, Zenóbio E, Feres M, et al. Impact of osteoporosis in dental implants: A systematic review. World J Orthop 2015; 6: 311. doi: https://doi.org/10.5312/wjo.v6.i2.311 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Whiting PF, Rutjes AW, Westwood ME, Mallett S, Deeks JJ, Reitsma JB, et al. QUADAS-2 Group QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med 2011; 155: 529. doi: https://doi.org/10.7326/0003-4819-155-8-201110180-00009 [DOI] [PubMed] [Google Scholar]
- 29.Zamora J, Abraira V, Muriel A, Khan K, Coomarasamy A. Meta-DiSc: a software for meta-analysis of test accuracy data. BMC Med Res Methodol 2006; 6: 31. doi: https://doi.org/10.1186/1471-2288-6-31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Metska ME, Aartman IH, Wesselink PR, Özok AR. Detection of vertical root fractures in vivo in endodontically treated teeth by cone-beam computed tomography scans. J Endod 2012; 38: 1344–7. doi: https://doi.org/10.1016/j.joen.2012.05.003 [DOI] [PubMed] [Google Scholar]
- 31.Edlund M, Nair MK, Nair UP. Detection of vertical root fractures by using cone-beam computed tomography: a clinical study. J Endod 2011; 37: 768–72. doi: https://doi.org/10.1016/j.joen.2011.02.034 [DOI] [PubMed] [Google Scholar]
- 32.Wang P, Yan XB, Lui DG, Zhang WL, Zhang Y, Ma XC. Detection of dental root fractures by using cone-beam computed tomography. Dentomaxillofac Radiol 2011; 40: 290–8. doi: https://doi.org/10.1259/dmfr/84907460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ludlow JB, Timothy R, Walker C, Hunter R, Benavides E, Samuelson DB, et al. Effective dose of dental CBCT-a Meta analysis of published data and additional data for nine CBCT units. Dentomaxillofac Radiol 2015; 44: 20140197. doi: https://doi.org/10.1259/dmfr.20140197 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Scarfe WC, Farman AG. What is cone-beam CT and how does it work? Dent Clin North Am 2008; 52: 707–30. doi: https://doi.org/10.1016/j.cden.2008.05.005 [DOI] [PubMed] [Google Scholar]
- 35.Kamburoglu K, Onder B, Murat S, Avsever H, Yüksel S, Paksoy CS. Radiographic detection of artificially created horizontal root fracture using different cone beam CT units with small fields of view. Dentomaxillofac Radiol 2013; 42: 20120261. doi: https://doi.org/10.1259/dmfr.20120261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Bezerra ISQ, Neves FS, Vasconcelos TV, Ambrosano GMB, Freitas DQ. Influence of the artefact reduction algorithm of Picasso Trio CBCT system on the diagnosis of vertical root fractures in teeth with metal posts. Dentomaxillofac Radiol 2015; 44: 20140428. doi: https://doi.org/10.1259/dmfr.20140428 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bechara B, Alex McMahan C, Moore WS, Noujeim M, Teixeira FB, Geha H. Cone beam CT scans with and without artefact reduction in root fracture detection of endodontically treated teeth. Dentomaxillofac Radiol 2013; 42: 20120245. doi: https://doi.org/10.1259/dmfr.20120245 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Jones D, Mannocci F, Andiappan M, Brown J, Patel S. The effect of alteration of the exposure parameters of a cone-beam computed tomographic scan on the diagnosis of simulated horizontal root fractures. J Endod 2015; 41: 520–5. doi: https://doi.org/10.1016/j.joen.2014.11.022 [DOI] [PubMed] [Google Scholar]
- 39.Junqueira RB, Verner FS, Campos CN, Devito KL, do Carmo AM. Detection of vertical root fractures in the presence of intracanalmetallic post: a comparison between periapical radiography and cone-beam computed tomography. J Endod 2013; 39: 1620–4. doi: https://doi.org/10.1016/j.joen.2013.08.031 [DOI] [PubMed] [Google Scholar]
- 40.Özer SY, Yiğit Özer S. Detection of vertical root fractures by using cone beam computed tomography with variable voxel sizes in an in vitro model. J Endod 2011; 37: 75–9. doi: https://doi.org/10.1016/j.joen.2010.04.021 [DOI] [PubMed] [Google Scholar]
- 41.Jakobson SJ, Westphalen VP, Silva Neto UX, Fariniuk LF, Schroeder AG, Carneiro E. The influence of metallic posts in the detection of vertical root fractures using different imaging examinations. Dentomaxillofac Radiol 2014; 43: 20130287. doi: https://doi.org/10.1259/dmfr.20130287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Taramsari M, Kajan ZD, Bashirzadeh P, Salamat F. Comparison of high-resolution and standard zoom imaging modes in cone beam computed tomography for detection of longitudinal root fracture: an in vitro study. Imaging Sci Dent 2013; 43: 171–7. doi: https://doi.org/10.5624/isd.2013.43.3.171 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ferreira RI, Bahrami G, Isidor F, Wenzel A, Haiter-Neto F, Groppo FC. Detection of vertical root fractures by cone-beam computerized tomography in endodontically treated teeth with fiber-resin and titanium posts: an in vitro study. Oral Surg Oral Med Oral Pathol Oral Radiol 2013; 115: e49–e57. doi: https://doi.org/10.1016/j.oooo.2012.06.012 [DOI] [PubMed] [Google Scholar]
- 44.Melo SL, Bortoluzzi EA, Abreu M, Corrêa LR, Corrêa M. Diagnostic ability of a cone-beam computed tomography scan to assess longitudinal root fractures in prosthetically treated teeth. J Endod 2010; 36: 1879–82. doi: https://doi.org/10.1016/j.joen.2010.08.025 [DOI] [PubMed] [Google Scholar]
- 45.Bechara B, McMahan CA, Noujeim M, Faddoul T, Moore WS, Teixeira FB, et al. Comparison of cone beam CT scans with enhanced photostimulated phosphor plate images in the detection of root fracture of endodontically treated teeth. Dentomaxillofac Radiol 2013; 42: 20120404. doi: https://doi.org/10.1259/dmfr.20120404 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Kajan ZD, Taromsari M. Value of cone beam CT in detection of dental root fractures. Dentomaxillofac Radiol 2012; 41: 3–10. doi: https://doi.org/10.1259/dmfr/25194588 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Mohammadpour M, Bakhshalian N, Shahab S, Sadeghi S, Ataee M, Sarikhani S. Effect of titanium and stainless steel posts in detection of vertical root fractures using NewTom VG cone beam computed tomography system. Imaging Sci Dent 2014; 44: 89–94. doi: https://doi.org/10.5624/isd.2014.44.2.89 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Takeshita WM, Iwaki LC, da Silva MC, Sabio S, Albino PR. Comparison of periapical radiography with cone beam computed tomography in the diagnosis of vertical root fractures in teeth with metallic post. J Conserv Dent 2014; 17: 225–9. doi: https://doi.org/10.4103/0972-0707.131781 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ezzodini Ardakani F, Razavi SH, Tabrizizadeh M. Diagnostic value of cone-beam computed tomography and periapical radiography in detection of vertical root fracture. Iran Endod J 2015; 10: 122–6. [PMC free article] [PubMed] [Google Scholar]
- 50.Chavda R, Mannocci F, Andiappan M, Patel S. Comparing the in vivo diagnostic accuracy of digital periapical radiography with cone-beam computed tomography for the detection of vertical root fracture. J Endod 2014; 40: 1524–9. doi: https://doi.org/10.1016/j.joen.2014.05.011 [DOI] [PubMed] [Google Scholar]
- 51.Neves FS, Freitas DQ, Campos PS, Ekestubbe A, Lofthag-Hansen S. Evaluation of cone-beam computed tomography in the diagnosis of vertical root fractures: the influence of imaging modes and root canal materials. J Endod 2014; 40: 1530–6. doi: https://doi.org/10.1016/j.joen.2014.06.012 [DOI] [PubMed] [Google Scholar]
- 52.Fisekcioglu E, Dolekoglu S, Ilguy M, Ersan N, Ilguy D. In vitro detection of dental root fractures with cone beam computed tomography (CBCT). Iran J Radiol 2014; 11: e11485. doi: https://doi.org/10.5812/iranjradiol.11485 [DOI] [PMC free article] [PubMed] [Google Scholar]