

Abstract
Introduction
Extragastrointestinal stromal tumors (EGIST) are rare mesenchymal tumor lesions located outside the gastrointestinal tract. A rare compressing tumor with difficult diagnosis is reported.
Presentation of the Case
A male patient, 63 years old, was admitted in the emergency room complaining of stretching and continuous abdominal pain for one day. He took Hyoscine, with partial improvement of symptoms, but got worse due to hyporexia, and the abdominal pain persisted. The patient also reported early satiety and ten-pound weight loss over the last month.
Discussion
EGIST could be assessed by CT-guided biopsy, leading to diagnosis and proper treatment with surgical resection or Imatinib.
Conclusion
This case report highlights the importance of considering EGIST an important differential diagnosis of compressing upper abdominal tumors.
1. Introduction
Gastrointestinal stromal tumors (GIST) are rare lesions in the mesenchymal neoplasm, accounting for less than 1% of the primary neoplasias of the digestive tract. They may affect any segment of the gastrointestinal tract but can occur in other locations in only 10% of the cases, and, in these situations, they are called EGIST [1]. The diagnosis is hard and may be made through CT-guided puncture and immunohistochemical analysis of the biopsy.
There are three histological types: spindle (70%), epithelial (20%), and mixed-cell. In 95%, there is somatic mutation of CD117 (c-kit), and its discovery in the immunohistochemical characteristic defines the GIST [2]. Staging could be done with abdominal and pelvis tomography, MRI, or PET-CT [3].
A case of massive EGIST is reported to show a rare differential diagnosis of an upper abdominal tumor, emphasizing the proper treatment due to correct diagnosis.
2. Presentation of the Case
A male patient, 63 years old, was admitted in the emergency room complaining of stretching and continuous abdominal pain for one day. He took Hyoscine, with partial improvement of symptoms, but got worse due to hyporexia, and the abdominal pain persisted for a few hours after medication. The patient also reported early satiety and ten-pound weight loss over the last month.
He is a smoker for nearly fifty years. He has no other comorbidities, previous surgeries, nor family history. In the physical examination, the patient showed flat abdomen, pain on superficial palpation of the epigastrium, no rebound tenderness, and palpable mass approximately 12 cm wide in the left abdominal quadrant.
The laboratory assessment was normal. An acute abdominal radiography (Figure 1) was taken, showing elevated left hemidiaphragm. The abdominal tomography (Figure 2) showed a wide hypodense mass with necrosis and heterogeneous absorption. The mass was posterior to the stomach and adjacent to the spleen and left kidney, without a cleavage plane between the left lobe of the liver and the pancreatic body, also compressing adjacent organs, invading the posterior wall of the stomach. The patient also underwent upper digestive endoscopy, showing bulging and gastric mucosal edema.
Figure 1.
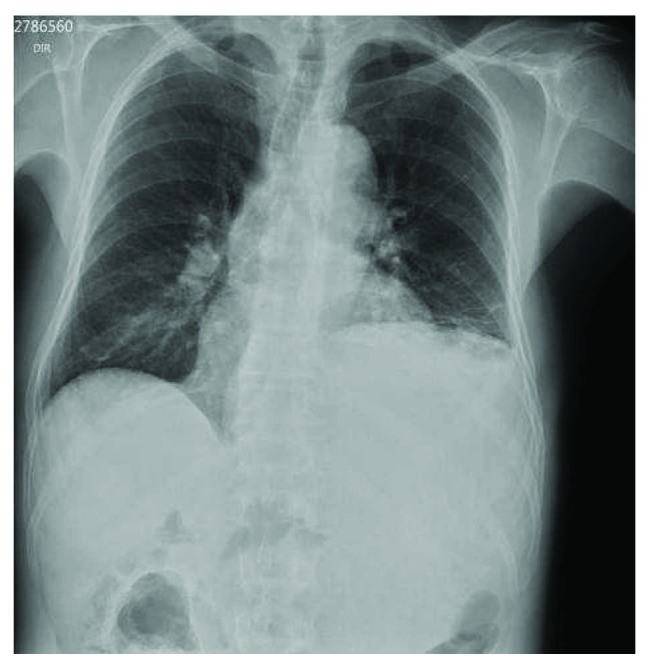
Acute abdominal X-ray showing the chest with elevated left hemidiaphragm.
Figure 2.
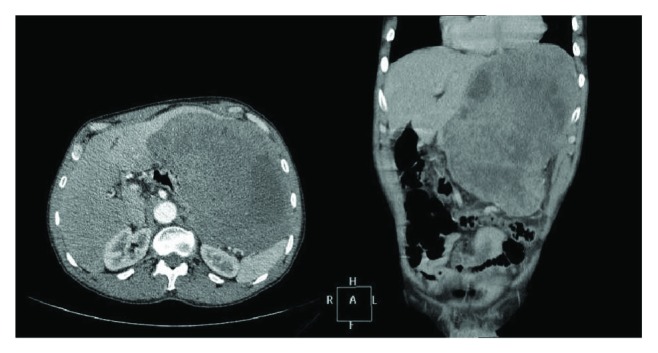
Contrast-enhanced computed tomography showing wide hypodense mass in the left hemiabdomen.
A CT-guided biopsy was taken, resulting in immunohistochemical analysis positive for C-Kit (Figure 3), CD34, and Ki67. These findings led to the correct diagnosis of extragastrointestinal stromal tumor (EGIST). The abdominal tomography was performed in the emergency room, also suggesting this type of tumor. The EGIST was a T4N0M0. As the tumor was greater than 2 cm and nonresectable, surgery was not suggested. The neoadjuvant therapy started with Imatinib, with weekly clinical follow-up.
Figure 3.
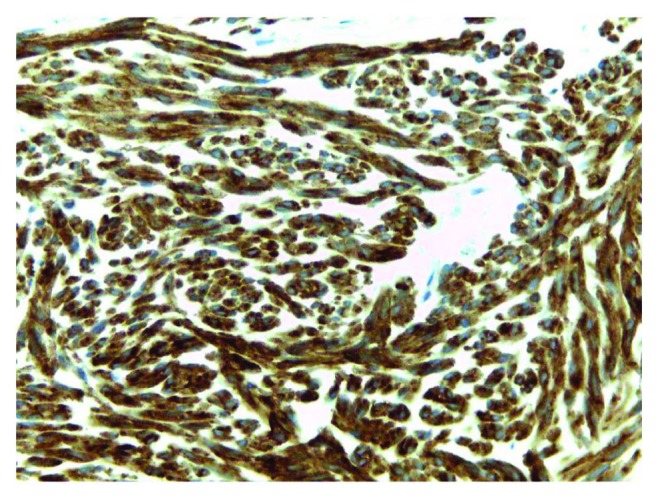
Immunohistochemical analysis positive for CD117 (C-kit) (original magnification 40x).
3. Discussion
The EGIST is a rare diagnosis regarding stromal tumors and can affect other locations in addition to the gastrointestinal tract, such as the omentum, pancreas, rectum, and small intestine. It is an important differential diagnosis of masses in the upper abdomen: leiomyoma, leiomyosarcoma, lipoma, schwannoma, carcinoids, and fibroids. CT-guided puncture or ultrasound may provide biopsy material. The immunohistochemical analysis with CD117 (C-Kit) confirms the diagnosis [4–6]. A recent study showed positive immunohistochemistry in 93.3% for CD117, 70% for CD34, and 10% for S1007. The biopsy result in this case report was positive for CD117, CD34, and Ki67.
Once the diagnosis is established, it is necessary to stage the tumor for better management [7]. The study patient was staged as T4N0M0 and nonresectable. The guidelines suggest that the first-line systemic treatment for advanced GIST cases is neoadjuvant therapy with Imatinib [3, 8, 9]. This treatment may result in 83–89% of patients responding or having the progression of the disease stabilized [8].
4. Conclusion
The EGIST should be noted as an important diagnosis of tumor masses, especially when symptomatic, such as masses in the upper abdomen. The correct diagnosis is very relevant, to the extent that it outlines the choice of clinical or surgical treatment.
Acknowledgments
The authors would like to thank the patient for the authorization and the employees that supported our work at the General Surgery Department.
Abbreviations
- EGIST:
Extragastrointestinal stromal tumors
- GIST:
Gastrointestinal stromal tumors.
Consent
The patient signed the written informed consent, allowing publication of this case report and any images accompanying it. A copy of the written consent is available for review by the Chief Editor of this journal.
Conflicts of Interest
The authors declare no conflicts of interest.
Authors' Contributions
Clara Kimie Miyahira made substantial contributions to the conception and design, or data analysis and interpretation, involved in the preparation of the manuscript; Miguel Bonfitto made contributions to the data analysis and interpretation involved in the preparation of the manuscript or in the critical revision of important intellectual content; Jéssyca Fernanda de Lima Farto made substantial contributions to the design and preparation of the manuscript; Annelise de Figueiredo Calili made contributions in revising medical records and to the final revision of the case report; Nathalia Rabello da Silva Sousa was involved in the preparation of the manuscript and helped to translate the manuscript into the English language; and Ana Paula de Figueiredo Calili made contributions on data interpretation and complementary research. All authors read and approved the final manuscript.
References
- 1.Yi J. H., Park B.-B., Kang J. H., et al. Retrospective analysis of extra-gastrointestinal stromal tumors. 2005;21(6):1845–1850. doi: 10.3748/wjg.v21.i6.1845. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Dorfman D. M., Bui M. M., Tubbs R. R., et al. The CD117 immunohistochemistry tissue microarray survey for quality assurance and interlaboratory comparison - a College of American Pathologists Cell Markers Committee Study. 2006;130(6):779–782. doi: 10.5858/2006-130-779-TCITMS. [DOI] [PubMed] [Google Scholar]
- 3.National Comprehensive Cancer Network. Soft tissue sarcoma, version 2.2016, NCCN clinical practice guidelines in oncology. http://www.jnccn.org/content/14/6/758.full. [DOI] [PubMed]
- 4.Miettinen M., El-Rifai W., Sobin L., Lasota J. Evaluation of malignancy and prognosis of gastrointestinal stromal tumors: a review. 2002;33(5):478–483. doi: 10.1053/hupa.2002.124123. [DOI] [PubMed] [Google Scholar]
- 5.Shinomura Y., Kinoshita K., Tsutsui S., Hirota S. Pathophysiology, diagnosis, and treatment of gastrointestinal stromal tumors. 2005;40(8):775–780. doi: 10.1007/s00535-005-1674-0. [DOI] [PubMed] [Google Scholar]
- 6.Watal P., Brahmbhatt S. G., Thoriya P. J., Bahri N. U. Retroperitoneal extragastrointestinal stromal tumor: radiologic pathologic correlation. 2014;4(1):p. 34. doi: 10.4103/2156-7514.135484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Quezada N., Acevedo F., Marambio A., et al. Complete pathological response to Imatinib mesylate in an extraintestinal gastrointestinal stromal tumor. 2014;5(10):681–685. doi: 10.1016/j.ijscr.2014.05.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Joensuu H., Hohenberger P., Corless C. L. Gastrointestinal stromal tumour. 2013;382(9896):973–983. doi: 10.1016/S0140-6736(13)60106-3. [DOI] [PubMed] [Google Scholar]
- 9.Rubin B. P. Gastrointestinal stromal tumours: an update. 2006;48(1):83–96. doi: 10.1111/j.1365-2559.2005.02291.x. [DOI] [PubMed] [Google Scholar]