

Abstract
Background
New licensing regulations require Louisiana early care and education centers (ECEs) to limit children’s screen-time and increase physical activity. A community-academic partnership involving academic, community, government, and ECE stakeholders launched two initiatives: 1) an evaluation of the implementation of licensing regulations at the local level and 2) a state-wide effort to develop technical assistance for ECE directors.
Objectives
To describe the methods and lessons learned and to establish recommendations based on this ongoing participatory action research.
Methods
A case study approach was used to identify the lessons learned and recommendations thus far, based on partners’ perspectives and ECE directors’ participation.
Lessons Learned
Recommendations include to share power and funding among stakeholders, to engage directors as partners to overcome recruitment challenges, and to start with the end in mind to ensure meaningful community engagement.
Conclusion
This participatory action approach is leading to innovative, feasible strategies to increase children’s physical activity.
Childhood obesity contributes to a higher risk of adult obesity, premature mortality, and comorbidities including diabetes, heart disease, and asthma.1 Low levels of physical activity and high levels of sedentary activity contribute to obesity during the preschool years,2–3 as well as to high blood pressure, behavioral problems, irregular sleep, and feelings of sadness and boredom.4–5 Due to increased device availability,6 screens (e.g. televisions, tablets, smartphones) are highly prevalent in children’s lives. Despite recommendations by the American Academy of Pediatrics for limiting use to 1 hour/day,7 preschoolers are estimated to spend 1.5 to 7.0 hours/day in screen-time.8,9 Furthermore, the recommended 2 hours/day of physical activity is obtained by less than 10% of preschoolers nationwide.10,11
Early care and education centers (ECEs) present an opportunity to add physical activity and reduce sedentary behavior in children, since over 80% of children spend some time in childcare settings by the age of 3 years.12 However, physical activity is highly variable within and across these settings.13 Many centers schedule little physical activity time14 yet expose children to an average of 1.3 hours/day of screen-time.4 African American children and children with obesity are most likely to have both low levels of physical activity and high levels of screen-time,15 indicating certain populations have a particular need for targeted improvements in health behaviors. In Louisiana, a state where 34% of the population is African American,16 obesity affects 13.2% of its preschoolers,17 a substantially higher prevalence than the rest of the country (8.9%).18 Therefore, interventions to improve health behaviors in ECE settings in this state are particularly warranted.
Impetus for Change: New Licensing Regulations
In 2015 the Louisiana Department of Education released the Louisiana Early Learning Center Licensing Regulations requiring ECEs to create: 1) an electronic devices policy allowing no more than 2 hours/day of electronic device activities for children ages two and over and prohibiting electronic device activity for children under two and 2) a written policy with procedures for providing at least 1 hour/day of physical activity including teacher-led and free play for all children (Table 1).
Table 1.
Louisiana Department of Education licensing regulations on electronic devices and physical activity in early learning centers.
|
The enactment of these new regulations has brought together stakeholders with a shared mission: to establish and disseminate strategies to reduce children’s screen-time and increase physical activity in ECE settings. Because prior successful ECE-based interventions engaged ECE directors in assessment and implementation efforts,19 this partnership includes ECE directors as critical stakeholders to identify barriers to implementing regulations and to develop and test strategies to overcome these barriers. The stakeholders represent academic, community, and public health professionals, who together with ECE directors identified a series of research questions: Will centers implement these new regulations as intended? Do these new regulations actually benefit the intended audience, i.e. reduce children’s screen-time and increase physical activity in ECE settings? Do ECE directors need support to implement these new regulations, and what technical assistance strategies can be developed and disseminated to support their efforts?
To address these research questions, this community-academic partnership is embarking on two initiatives. The first initiative is to evaluate the implementation of the licensing regulations in ECEs at a local level in one municipality (Baton Rouge, Louisiana). With the use of objective assessments and classroom observations, the team is determining if centers are truly following the regulations and if the new policies/practices are achieving the desired effect of improving children’s behavior. The second initiative of the partnership is a state-wide effort to develop technical assistance strategies to help ECE directors to implement the screen-time and physical activity regulations in their centers.
This community-academic partnership is bringing together a new collaboration of Louisiana stakeholders to better understand the needs of the state’s ECE directors and tailor technical assistance strategies to achieve the overall goal of increasing children’s physical activity while reducing screen-time. The purpose of this manuscript is to describe the methods of this ongoing participatory action research and to provide recommendations based on lessons learned. Results specific to the initiatives will be reported elsewhere.
Methods of Building a Participatory Action Research Strategy
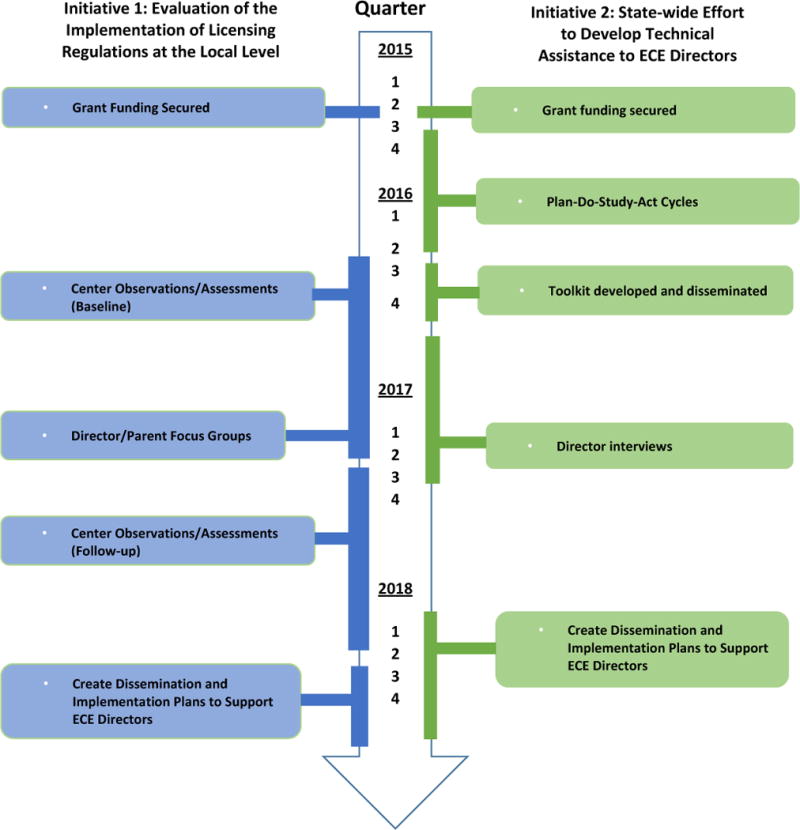
The evolution and methods of the partnership are detailed below, beginning with a description of the partnership, followed by the examination of the implementation of regulations at a local level then the development of technical assistance strategies state-wide. A timeline of the partnership’s activities is provided in Table 2, and the roles of each partner are detailed in Table 3.
Table 2.
Timeline of activities in the community-academic partnership.
|
Note. ECE = early care and education.
Table 3.
Key partners and their roles in the community-academic partnership.
| Partner | Role |
|---|---|
| Community | |
| Mayor’s Healthy City Initiative of Baton Rouge |
• Initiative 1: Community Principal Investigator
|
| Louisiana Department of Health |
• Initiative 2: Governmental agency lead
|
| Louisiana Department of Education |
• Initiative 2: Governmental agency partner
|
| Early Care and Education (ECE) Directors |
• Initiative 1: Practitioner partner
|
• Initiative 2: Practitioner partner
| |
| Academic | |
| Pennington Biomedical Research Center |
• Initiative 1: Academic Principal Investigator
|
• Initiative 2: Evaluation partner
| |
| Louisiana State University School of Kinesiology |
• Initiative 1: Research partner
|
| Tulane University |
• Initiative 2: Evaluation partner
|
Note. ECE = early care and education, PDSA = Plan Do Study Act quality improvement strategy.
Partnership
The partnership first began in response to a funding call for community-based health policy research projects. Academic researchers at Pennington Biomedical Research Center, an academic institute within Louisiana State University, convened with the Mayor’s Healthy City Initiative (MHCI) of Baton Rouge and successfully received grant funding to examine implementation of the screen-time and physical activity policies in ECEs before and after the new state regulations are enacted. As part of a national effort organized by the U.S. Conference of Mayors, the MHCI was launched in 2008 when the Mayor-President of Baton Rouge focused on childhood obesity as the chair of the Youth, Education, and Families Institute with the National League of Cities. The MHCI then expanded its focus to obesity, HIV and sexually transmitted infections, behavioral health, and the overuse of emergency rooms. The MHCI is a 501(c)(3) non-profit organization that includes three advisory boards that meet monthly and represent over 80 hospitals, non-profit organizations, and government agencies. The MHCI director and the Pennington Biomedical academic investigator are Co-Principal Investigators for the first initiative, which is a prospective cohort study to evaluate the implementation of licensing regulations at the local level; the two partners share leadership for the project and responsibility for meeting benchmarks.
Shortly after securing this initial grant, a team from the Louisiana Department of Health approached Pennington Biomedical to join the partnership to develop and implement technical assistance strategies to help ECE directors to implement the new regulations. Funding from the Association of State Public Health Nutritionists (ASPHN) provides support for these statewide stakeholders to join the partnership, including representatives of the childcare community from the Louisiana Department of Health (the Early Childhood Education and School Health Leader, the WellSpot Designation Program Coordinator, and a Centers for Disease Control and Prevention Public Health Advisor) and the Chief of Staff in Division of Early Education in the Louisiana Department of Education who oversees licensing regulations in ECEs, as well as additional academic research partners with expertise in early childhood development and policy implementation.
Initiative 1: Evaluation of the Implementation of Licensing Regulations at the Local Level
To examine the implementation of the new state regulations, a prospective cohort study is underway by the joint efforts of the Mayor’s Healthy City Initiative of Baton Rouge (MHCI) and Pennington Biomedical Research Center. Together, the team secured external funding and is now empirically testing the implementation of the new state regulations by examining ECE policies and practices and children’s behavior in the city of Baton Rouge.
Approach
A prospective observational cohort design is being used to examine the physical activity and screen-time environment of licensed ECEs in Baton Rouge, and the children’s physical activity and screen-time, before and after the enactment of new state regulations. Based on data from Dowda et al.,14 ten ECEs were randomly selected and enrolled to ensure a well-powered study. Screen-time and physical activity practices are being measured in the 10 enrolled centers using the Environment and Policy Assessment and Observation (EPAO) tool.19–20 A survey is being administered to each ECE director to capture structured physical activity programs, free play, and screen-time policies. Children’s physical activity is objectively measured by an accelerometer, and screen-time is assessed using direct observation20 and parent-report.21 Additional funding has been secured to assess children’s fundamental motor skills to examine relationships with screen-time and to identify intervention targets to promote children’s physical activity. Assessments are being conducted twice at each center, one year apart, to capture potential changes after the policies are implemented.
The final goal of the local initiative is to create dissemination and implementation plans to support ECEs and parents in reducing children’s screen-time and increasing physical activity. MHCI led four focus groups with 20 parents and 8 ECE directors to identify thoughts and concerns about the amount of physical activity and technology in children’s lives and its impact on children’s health behaviors. Results are forthcoming and will be shared with academic, community, and governmental stakeholders via conference presentations and publications.
Initiative 2: State-wide Effort to Develop Technical Assistance to ECE Directors
Concurrently with the local initiative, the partnership includes a state-wide initiative to develop and test technical assistance strategies to help ECE directors implement the new regulations. One of the first actions of this initiative was led by the Obesity Prevention Program Manager of the Bureau of Family Health in the Louisiana Department of Health to assemble a successful grant application to ASPHN, which had acquired federal funding to support select states in its Pediatric Obesity Mini Collaborative Improvement and Innovation Network Project (CoIIN). A CoIIN is a virtually connected team of people who have a collective vision and work together with national experts to share best practices and lessons learned and to track progress towards benchmarks.22 The pediatric obesity miniCoIIN supports the Expert Committee Recommendations on the prevention of child and adolescent overweight and obesity, which includes adopting policies and practices in ECE settings that support healthy weight behaviors.23 As part of the miniCoIIN, ASPHN sponsors annual workshops to support team planning, interaction with other state teams, and technical guidance from national experts. Further, ASPHN provides annual funding for each team’s project and bimonthly virtual webinars to focus on specific topics related to childhood obesity prevention.
The funding application was built on extensive experience of the Louisiana Department of Health Office of Public Health, which since 2010 has funded and implemented the Nutrition and Physical Activity Self-Assessment of Child Care Centers (NAP SACC) program in over 250 ECEs statewide. A prior community-academic partnership in Louisiana demonstrated that centers participating in NAP SACC significantly increased children’s physical activity levels compared to control centers.24 The ASPHN funding seeks to build on the state’s prior success by focusing on ways to help ECE directors comply with the state’s new licensing regulations.
Approach
To start this initiative, the Louisiana miniCoIIN team attended a workshop hosted by ASPHN and learned how to enact Plan-Do-Study-Act (PDSA) cycles, a quality improvement tool for rapid implementation and evaluation of small-scale changes.25 “Plan” involves planning a small test or observation, “Do” consists of collecting information to test the plan, “Study” is interpreting the data, and “Act” allows a refinement and advancement to the next plan. The team then invited six ECE directors from across the state to participate as partners in the project; these directors provided input on the PDSA cycles and received technical assistance and a $500 stipend towards developing and implementing their electronic devices policy.
The first PDSA cycle involved reviewing or writing an electronic devices policy with each ECE director over a 2-month period, via phone calls and face-to-face meetings. Already existing policies were strengthened to align with the new state regulations and then used as examples for the remaining ECE centers. During these conversations, it became clear that some centers prohibited screens entirely, whereas others used screens only for educational purposes. The phrase “Smart Screen” was chosen to describe centers that limit screen-time exposure to educational purposes and “Screen Free” describes centers that prohibit screen-time.
Because the directors voiced concerns of children’s exposure to screen-time at home, the following PDSA cycles focused on creating flyers, newsletter content, and a workshop for parents to describe the center’s policy on screen-time and ways parents can reduce their children’s screen-time at home. ECE directors reviewed the materials and provided suggestions on several iterations to reduce the literacy level. Finally, a lesson plan was developed with input from the ECE directors to teach children about active time and screen-time. The ECE centers’ involvement culminated in a “Screen Free Week” in May 2016 involving local press coverage of the centers’ efforts to reduce screen-time.
Products from the PDSA cycles were compiled to create the “Louisiana Screen Time Regulations Toolkit for Early Childhood Education Centers,” which is disseminated in print and online for free download26 and was presented at two state-wide conferences. The toolkit consists of three parts: 1) an introduction to the importance of limiting children’s screen-time and a copy of the electronic devices and physical activity licensing regulations; 2) guidelines to create a screen free or smart screen facility including a self-assessment adapted from the NAP SACC program27 and examples of policies from the six Louisiana ECE partners, and 3) tools and resources for the centers.
After releasing the toolkit, the team conducted key informant interviews with ECE directors to better understand how the state’s screen-time policies are implemented, monitored, enforced and evaluated. Together, the academic and public health team created an interview script adapted from a prior interview of elementary school key informants.28 Twelve ECE centers were randomly selected state-wide, and directors were interviewed. Results are forthcoming and will guide future strategies to provide ECE directors with resources and technical support to implement and evaluate their electronic devices policies. The team was re-funded by ASPHN and is now focusing on initiatives to support ECE directors and parents, including a project to use playground stenciling to promote physical activity at ECE centers, with the assistance of a pediatric kinesiologist at Louisiana State University and a physical education consultant.
Recommendations based on Lessons Learned
Recommendation 1: Share Power among Stakeholders
The key to success has been power sharing among the academic-community partners. For instance, at the MHCI boards’ request, the research study in the first initiative incorporated a question about the directors’ and parents’ awareness of the “5-2-1-0” health message (which recommends 5 fruits and vegetables, 2 or fewer hours of screen-time, 1 hour of physical activity, and 0 sugar sweetened beverages per day)29 that is promoted by the MHCI. For the second initiative, the ECE directors provide input on which PDSA cycles are successful and request additional technical assistance strategies to test, such as the parent workshop. The academic researchers create survey questions to help the team determine which PDSA cycles are successful, and the public health professionals use their training and experiences to create and modify content to be acceptable by ECE directors. These examples build on prior work that illustrated the importance of involving ECE practitioners in an iterative, ongoing partnership when designing and implementing health-related changes in preschools.30
Recommendation 2: Allocate Funding among Stakeholders
The new state regulations created a window of opportunity to successfully garner multiple external funding streams, which then allowed funding to be allocated to research and quality improvement activities. Monies are specifically designated at the local level to support a policy intern to conduct the focus groups and serve as a liaison with the MHCI advisory boards. The intern has benefited from training in focus group administration from the research staff. Monies are also allocated at a local level to ECE directors and parents to participate in the focus groups, and school supplies are being purchased for the 10 ECE centers participating in the research study. For the state-wide technical assistance initiative, monies are allocated for the ECE directors to participate in the PDSA cycles and interviews and for the creation of the toolkit.
Recommendation 3: Engage ECE Directors as Partners
The chief barrier for the partnership is recruiting childcare center directors to participate in the activities. For the prospective cohort study in the first initiative, the team approached over 150 licensed ECE centers in the Baton Rouge area to identify 10 centers to enroll in the prospective cohort study. The community investigator assisted in enrolling centers by asking community leaders to encourage ECE directors to participate. Over $400 worth of school supplies are being provided as incentives to the director to compensate for the time commitment needed to complete a survey and allow research staff on-site for multiple days at two timepoints for data collection and classroom observation. For the second initiative, there was funding for six ECE centers to participate in PDSA cycles and only six applied. Five centers completed all PDSA cycles, but one center ended contact and quit the project before the end, forfeiting their stipend. Regarding the interviews, 82 centers were contacted by email to find 12 directors to agree to participate. These ECE directors received $25 worth of school supplies to compensate for their time.
One strategy to better engage ECE directors is to provide them with more decision-making power. As previously observed in teachers’ experiences in participatory research,31 education practitioners need to be involved in decision-making for a successful academic-community partnership. In the current partnership, ECE directors are asked to provide input on the identification, development, and testing of technical assistance strategies as well as to identify barriers and facilitators for implementing the state regulations. Still, directors may have concerns regarding their policies and practices being evaluated by state agencies. Many prior ECE-based interventions, including those outside of Louisiana, failed to be fully implemented without the buy-in of ECE directors.32 An important exception is the NAP SACC program which requires directors to conduct a self-assessment and design a tailored action plan for implementation.19,27 This program has shown effectiveness in improving children’s nutrition,27 likely due to its dependence on each ECE director to self-assess, design a plan, and execute that plan within the center. While ECE directors are instrumental to the present partnership, they could be given more responsibility by steering the priorities, activities, and dissemination plans, and having authority over budgetary decisions. To overcome the potential distrust or concern by ECE directors, directors should be fully engaged as decision-makers, which may ultimately strengthen their commitment and the likelihood of sustained impact.
Recommendation 4: Start with the End in Mind to Ensure Meaningful Community Engagement
This partnership has been developed with the end in mind: to establish and disseminate strategies to reduce children’s screen-time and increase physical activity in ECEs. The final phase of the partnership is to present information to community stakeholders, including at ECE professional workshops and conferences and to the MHCI advisory boards, and use these data to solicit input for technical assistance strategies for ECEs. Continued support of the state agencies to provide technical assistance and the MHCI to bridge communication with ECE directors will enable dissemination and implementation of strategies to achieve community health goals after each of the grants has ended. Although community stakeholders identify childhood obesity prevention as a top priority, most parents fail to recognize obesity in preschool children,33 and many mistakenly think obesity is not a health problem at this age. The team seeks a shift in the climate in the state to recognize that preschool is a critical opportunity to improve health behaviors and to put children on a trajectory towards life-long healthy living.
Conclusion
A community academic partnership in Louisiana is working toward the goal of reducing children’s screen-time and increasing physical activity in ECEs. Partners are from a number of community and academic settings and are engaged in multiple activities including obtaining funding, collecting data, interpreting findings, and developing technical assistance strategies to support ECE directors in implementing policy changes in their centers. Unlike prior collaboratives on child health policy that began with stakeholder-driven research in order to create recommendations for new policies,34 this partnership began with a new state policy already in place and used this policy as an impetus to develop technical resources to assist ECE directors in implementing the new regulations. For these community-academic partnerships to be effective, it is important to share power and funding among stakeholders, to engage the ECE directors (or other relevant community members) as partners to overcome recruitment challenges, and to start with the end in mind to ensure meaningful community engagement. Dissemination of findings through community briefings is the final step. Changing policies in childcare settings can prompt participatory action research which may ultimately improve children’s health behaviors to reduce childhood obesity.
Acknowledgments
We are grateful for the contributions of Kate Holmes, Lisa Brochard, Jamila Freightman, Tim Nguyen, Johannah Frelier, Patti Boyd, and the ECE directors, parents, children, and community stakeholders who participated in our project. The prospective cohort study project was supported by Award Number U54MD008602 for the Gulf States Collaborative Center for Health Policy Research (Gulf States-HPC) from the National Institute on Minority Health and Health Disparities of the National Institutes of Health with ancillary funding from the LSU Biomedical Collaborative Research Program. The miniCoIIN quality improvement project was supported by the Association of State Public Health Nutritionists. AES is supported in part by 1 U54 GM104940 from the National Institute of General Medical Sciences of the National Institutes of Health, which funds the Louisiana Clinical and Translational Science Center. CKM is supported in part by the NORC Center Grant P30DK072476 entitled “Nutrition and Metabolic Health Through the Lifespan” sponsored by NIDDK. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
References
- 1.Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes. 2011;35(7):891–8. doi: 10.1038/ijo.2010.222. [DOI] [PubMed] [Google Scholar]
- 2.Ekelund U, Luan J, Sherar LB, Esliger DW, Griew P, Cooper A. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. JAMA. 2012;307(7):704–12. doi: 10.1001/jama.2012.156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tremblay M, LeBlanc A, Kho M, Saunders T, Larouche R, Colley R, et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011;8(1):98. doi: 10.1186/1479-5868-8-98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vanderloo LM. Screen-viewing among preschoolers in childcare: a systematic review. BMC Pediatr. 2014;14:205. doi: 10.1186/1471-2431-14-205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.U.S. Department of Agriculture, U.S. Department of Health and Human Services. 2010 Retrieved from https://health.gov/dietaryguidelines/2010/
- 6.Strasburger VC, Hogan MJ, Mulligan DA, Ameenuddin N, Christakis D, Cross C, et al. Children, adolescents, and the media. Pediatrics. 2013;132(5):958–61. doi: 10.1542/peds.2013-2656. [DOI] [PubMed] [Google Scholar]
- 7.American Academy of Pediatrics Council on Communications and Media. Media and young minds. Pediatrics. 2016;138(5):e20162591. doi: 10.1542/peds.2016-2591. [DOI] [PubMed] [Google Scholar]
- 8.Rideout VJ, Foehr UG, Roberts DF. Generation M2: Media in the lives of 8- to 18-year-olds. 2010 Retrieved from http://files.eric.ed.gov/fulltext/ED527859.pdf.
- 9.Heelan KA, Eisenmann JC. Physical activity, media time, and body composition in young children. J Phys Act Health. 2006;3(2):200. doi: 10.1123/jpah.3.2.200. [DOI] [PubMed] [Google Scholar]
- 10.SHAPE America – Society of Health and Physical Educators. Active Start: a Statement of Physical Activity Guidelines for children from Birth to Age 5. 2nd. Reston, VA: National Association for Sport and Physical Education; 2009. [Google Scholar]
- 11.Beets MW, Bornstein D, Dowda M, Pate RR. Compliance with national guidelines for physical activity in U.S. preschoolers: measurement and interpretation. Pediatrics. 2011;127(4):658–64. doi: 10.1542/peds.2010-2021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Tandon PS, Zhou C, Lozano P, Christakis DA. Preschoolers’ total daily screen time at home and by type of child care. J Pediatr. 2011;158(2):297–300. doi: 10.1016/j.jpeds.2010.08.005. [DOI] [PubMed] [Google Scholar]
- 13.Pate RR, Pfeiffer KA, Trost SG, Ziegler P, Dowda M. Physical activity among children attending preschools. Pediatrics. 2004;114(5):1258–63. doi: 10.1542/peds.2003-1088-L. [DOI] [PubMed] [Google Scholar]
- 14.Dowda M, Pate RR, Trost SG, Almeida MJC, Sirard JR. Influences of preschool policies and practices on children’s physical activity. J Community Health. 2004;29(3):183–96. doi: 10.1023/b:johe.0000022025.77294.af. [DOI] [PubMed] [Google Scholar]
- 15.Anderson SE, Economos CD, Must A. Active play and screen time in US children aged 4 to 11 years in relation to sociodemographic and weight status characteristics: a nationally representative cross-sectional analysis. BMC Public Health. 2008;8(1):366. doi: 10.1186/1471-2458-8-366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.U.S. Census Bureau. American FactFinder, 2015. 2015 Retrieved from http://factfindercensusgov.
- 17.Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion. Nutrition, physical activity, and obesity- data, trend and maps [online] 2017 Retrieved from https://www.cdc.gov/nccdphp/dnpao/data-trends-maps/index.html.
- 18.Ogden CL, Carroll MD, Lawman HG, Fryar D, Kruszon-Moran D, Kit BK, et al. Trends in obesity prevalence among children and adolescents in the United States, 1988-1994 through 2013-2014. JAMA. 2016;315(21):2292–9. doi: 10.1001/jama.2016.6361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Ward DME, McWilliams C, Vaughn A, Erinosho T, Mazzuca S, Hanson P, et al. Go NAP SACC: Nutrition and Physical Activity Self-Assessment for Child Care. 2nd. Center for Health Promotion and Disease Prevention and Department of Nutrition; University of North Carolina at Chapel Hill: 2014. [Google Scholar]
- 20.Bower JK, Hales DP, Tate DF, Rubin DA, Benjamin SE, Ward DS. The childcare environment and children’s physical activity. Am J Prev Med. 2008;34(1):23–9. doi: 10.1016/j.amepre.2007.09.022. [DOI] [PubMed] [Google Scholar]
- 21.Jago R, Thompson J, Sebire S, et al. Cross-sectional associations between the screen-time of parents and young children: differences by parent and child gender and day of the week. Int J Behav Nutr Phys Act. 2014;11:54. doi: 10.1186/1479-5868-11-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gloor PA. Swarm creativity: Competitive advantage through collaborative innovation networks. New York: Oxford University Press; 2006. [Google Scholar]
- 23.Barlow S. Committee atE: Expert Committee Recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics. 2007;120 doi: 10.1542/peds.2007-2329C. [DOI] [PubMed] [Google Scholar]
- 24.Bonis M, Loftin M, Ward D, Tseng TS, Clesi A, Sothern M. Improving physical activity in daycare interventions. Child Obes. 2014;10(4):334–41. doi: 10.1089/chi.2014.0040. [DOI] [PubMed] [Google Scholar]
- 25.Speroff T, O’Connor GT. Study designs for PDSA quality improvement research. Qual Manag Health Care. 2004;13(1):17–32. doi: 10.1097/00019514-200401000-00002. [DOI] [PubMed] [Google Scholar]
- 26.Lewis L, Brochard L, Fowler W, Freightmanh J, Gustat J, Holmes K, et al. Louisiana screen time regulations toolkit for early childhood education centers. 2016 Retrieved from http://wellaheadla.com/Programs/Early-Childhood-Health.
- 27.Ward DS, Benjamin SE, Ammerman AS, Ball SC, Neelon B, Bangdiwala SI. Nutrition and physical activity in child care: Results from an environmental intervention. Am J Prev Med. 2008;35(4):352–356. doi: 10.1016/j.amepre.2008.06.030. [DOI] [PubMed] [Google Scholar]
- 28.Cradock AL, Barrett JL, Carnoske C, Chriqui J, Evenson K, Gustat J, et al. Roles and strategies of state organizations related to school-based physical education and physical activity policies. J Public Health Manag Pract. 2013;19:S34–S40. doi: 10.1097/PHH.0b013e3182840da2. [DOI] [PubMed] [Google Scholar]
- 29.Rogers VW, Hart PH, Motyka E, Rines EN, Vine J, Deatrick DA. Impact of Let’s Go! 5-2-1-0: a community-based, multisetting childhood obesity prevention program. J Pediatr Psychol. 2013;38(9):1010–20. doi: 10.1093/jpepsy/jst057. [DOI] [PubMed] [Google Scholar]
- 30.Izumi BT, Peden AM, Hallman JA, Barberis D, Stott B, Nimz S, Ries WR, Capello A. A community-based participatory research approach to developing the Harvest for Healthy Kids curriculum. Progress in Community Health Partnerships: Research, Education, and Action. 2013;7(4):379–384. doi: 10.1353/cpr.2013.0047. [DOI] [PubMed] [Google Scholar]
- 31.Ferreira R, Ebersohn L, Mbongwe BB. Power-sharing partnerships: Teachers’ experiences of participatory methodology. Progress in Community Health Partnerships: Research, Education, and Action. 2015;9(1):1–2. doi: 10.1353/cpr.2015.0015. [DOI] [PubMed] [Google Scholar]
- 32.Wolfenden L, Jones J, Finch M, Wyse RJ, Yoong SL, Steele EJ, Williams AJ, Wiggers J, Small T, Seward K, et al. Strategies to improve the implementation of healthy eating, physical activity and obesity prevention policies, practices or programmes within childcare services. Cochrane database of systematic reviews (Online) 2015;2015 doi: 10.1002/14651858.CD011779.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Lundahl A, Kidwell KM, Nelson TD. Parental underestimates of child weight: a meta-analysis. Pediatrics. 2014;133(3):e689–e703. doi: 10.1542/peds.2013-2690. [DOI] [PubMed] [Google Scholar]
- 34.Maternal and Child Health Care Leadership Collaborative Pennsylvania Allegheny County. Keyser DJ, Pincus HA. From community-based pilot testing to region-wide systems change: Lessons from a local quality improvement collaborative. Progress in Community Health Partnerships: Research, Education, and Action. 2010;4(2):105–114. doi: 10.1353/cpr.0.0119. [DOI] [PubMed] [Google Scholar]