

Abstract
Objective
To characterize recommendations given to pregnant women by Colorado cannabis dispensaries regarding use of cannabis products for nausea during the first trimester of pregnancy.
Methods
This was a statewide cross-sectional study in which advice about cannabis product use was requested using a mystery caller approach. The caller stated she was 8 weeks pregnant and experiencing morning sickness. Dispensaries were randomly selected from the Colorado Department of Revenue Enforcement Division website. The primary outcome was the proportion of marijuana dispensaries that recommended a cannabis product for use during pregnancy. We hypothesized that 50% of dispensaries would recommend use. A sample size of 400 was targeted to yield a two-sided 95%CI width of 10%. Secondary outcomes included proportion endorsing cannabis use as safe during pregnancy, specific product recommendations, and encouraging discussion with a health care provider. Recommendations were compared by licensure type (medical, retail or both) and location (rural vs urban).
Results
Of the 400 dispensaries contacted, 37% were licensed for medical sale (n=148), 28% for retail (n=111), and 35% for both (n=141). The majority, 69% (277/400), recommended treatment of morning sickness with cannabis products (95%CI 64-74%). Frequency of recommendations differed by license type (medical 83.1%, retail 60.4%, both 61.7%, p<0.001). Recommendations for use were similar for dispensary location (urban 71% vs non-urban 63%, p=0.18. The majority (65%) based their recommendation for use in pregnancy on personal opinion and 36% stated cannabis use is safe in pregnancy. Ultimately, 81.5% of dispensaries recommended discussion with a health care provider; however, only 31.8% made this recommendation without prompting.
Conclusion
Nearly 70% of Colorado cannabis dispensaries contacted recommended cannabis products to treat nausea in the first trimester. Few dispensaries encouraged discussion with a health care provider without prompting. As cannabis legalization expands, policy and education efforts should involve dispensaries.
Introduction
Marijuana use in pregnancy may have adverse effects on the fetus, including fetal growth restriction and long-term neurological consequences.1,2 The American College of Obstetricians and Gynecologists (ACOG) states “obstetrician–gynecologists should be discouraged from prescribing or suggesting the use of marijuana for medicinal purposes during preconception, pregnancy, and lactation.”2
Expanding legalization may increase use among pregnant women, and may be accompanied by increased perception of safety without data to assure safety.3 A cross-sectional study of women who are clients of the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) in the state of Colorado found that 48% of women who reported current marijuana use also reported marijuana use during their prior pregnancy “to help with nausea or vomiting”.4
Pregnant women who are interested in using marijuana may refrain from seeking safety information from health care providers due to fear of legal repercussions, and instead seek advice from cannabis retailers. The primary objective of this study was to estimate the proportion of cannabis dispensaries that recommended cannabis products to a caller posing as pregnant and experiencing nausea in the first trimester of pregnancy. Secondary objectives were to characterize recommendations given to pregnant women by Colorado cannabis dispensaries regarding use of cannabis products. It was hypothesized that 50% of dispensaries would recommend a cannabis product and that recommendations would differ by dispensary type (medical, retail, or both) and geographic location (urban versus rural).
Materials and Methods
This cross-sectional study of cannabis dispensaries in Colorado used a mystery caller approach. The study was approved by the Colorado Multiple Institutional Review Board (number 17-0637).. Minor deception (eg posing as a pregnant caller) was deemed necessary to obtain an accurate assessment of how cannabis dispensaries advise pregnant women. Recommendations, advice, and comments included in this study are limited to the individual dispensary employee who responded to the questions and may or may not reflect the policies or recommendations of the actual dispensary. However, the term “dispensary” is used to reflect the individual employee who answered the phone. All registered dispensaries in Colorado will be informed of the results when published.
The target population consisted of all cannabis dispensaries in Colorado. The sampling frame was a list of licensed dispensaries on the Colorado Department of Revenue Enforcement Division website (accessed December 1, 2016).5 There were 982 licenses among 724 individual dispensaries with three mutually exclusive license types: 270 (37%) medical only, 258 (36%) both (medical and retail), and 196 (27%) retail only. In Colorado, medical dispensaries are licensed pursuant to the medical code to operate a business and sell medical marijuana to registered patients and to primary care givers.6 Retail dispensaries are entities licensed to purchase retail marijuana and retail marijuana concentrate from a retail marijuana cultivation facility or manufacturing facility and to transfer these products to consumers.”7 A dispensary can operate as both a medical and retail dispensary if they obtain both licenses and also confirm that there will be no sales of medical marijuana to individuals under the age of 21 years at the combined use location.7
Sampling occurred proportionally by dispensary type. As some municipalities allow only certain license types, sampling was further stratified by municipality within license type. For medical dispensaries, municipal regions were Colorado Springs (50%), Denver (23%), and elsewhere (27%); for both medical-and-retail license types, regions were municipal Denver (58%) and elsewhere; and for retail-only licenses, municipal regions were Denver and Aurora (24%) and elsewhere (76%). Within each strata, dispensaries were selected randomly without replacement using SAS SURVEYSELECT with a frequency to proportionately represent each strata in a full sample. To replace unavailable dispensaries in order to achieve the targeted sample size, alternative dispensaries were selected randomly without replacement within the appropriate strata among previously unselected dispensaries again using SAS SURVEYSELECT.
The Colorado Department of Revenue Enforcement Division website provided the following information in a publically available Microsoft Excel spreadsheet: license name, business name, license number, address, city, and zip code. Phone numbers were obtained through an online search of the dispensary name and then cross checked against the corresponding address in the registry.
Two investigators (BD and CM) contacted selected dispensaries using a phone script to inquire about cannabis use for nausea in pregnancy (Box 1). The phone script was developed by the investigators and piloted with 15 dispensaries in Alaska, Oregon, and Washington. Each caller stated they were eight weeks pregnant, feeling really nauseated, and asked, “Are there any products that are recommended for morning sickness?” The remainder of the conversation utilized the telephone script to obtain responses (Box 1).
Box 1. Phone Script.
“Hi, I’m eight weeks pregnant and feeling really nauseated. Are there any products that are recommended for morning sickness?”
Prompts in response to no recommendation:
What if I have a medical card? (If asked why you have a card, state it’s for chronic pain from a car accident)
Why not?
Prompts in response to recommendation:
- What product?
- Why?
How often should I use it?
- Is it safe to take during pregnancy?
- If only maternal risks are addressed, ask: Is it also safe for my baby?
- If only fetal risks are addressed, ask: Is it also safe for me?
Before closing call
Should I talk to my doctor about this (if no recommendation previously made to discuss with health care provider)?
If any cannabis products were recommended at any point during the phone call, the response of the dispensary was considered as affirmative for cannabis recommendation. If the dispensary employee noted that it was against policy to make a recommendation or claimed to not be able to make a recommendation, but then went on to recommend cannabis, this was also recorded as an affirmative response. If the dispensary employee asked the caller to come in to the business in person for advice, the response was recorded as “no recommendation made”.
If cannabis products were not initially recommended, the caller asked whether a recommendation could be made if she had a medical marijuana card. The caller stated she had a medical marijuana card for chronic pain after a car accident. In addition, dispensaries were asked whether the caller should discuss cannabis use with a health care provider. Dispensaries were documented as recommending this prior to being prompted, after being prompted, or not recommending even after prompting. To qualify for a medical marijuana card in the state of Colorado, an adult has to be a Colorado resident 18 years or older, and have a qualifying medical condition (cancer, glaucoma, HIV/AIDS, cachexia, persistent muscle spasms, seizures, severe nausea, severe pain, post-traumatic stress disorder) as determined by a licensed Colorado physician.
Recommendation for use was categorized as personal opinion, referenced research, referenced dispensary policy, deferred to health care provider, or did not specify. Recommendations were classified as personal opinion if the dispensary employee stated “in my opinion” or used anecdotes.
For analysis, dispensaries were categorized as urban and rural according to guidelines published by the Colorado Rural Health Center, and utilized by the Colorado Department of Public Health and Environment.8 This resource classifies all zip codes in Colorado as urban, rural, or frontier. Given the small number of dispensaries in the frontier area, frontier and rural dispensaries were grouped together as rural for analysis.
All calls were digitally recorded, which is legally permissible in Colorado. Answers to each branching point were documented on a paper data sheet to avoid interruptions and for future reference if the digital audio recording was unavailable. The audio recordings and paper data sheets were then used to add responses to Research Electronic Data Capture (REDCap).9 To avoid dispensary identification, study identification numbers for each dispensary were used. The paper data sheets were shredded and the audio recordings deleted at the conclusion of data analysis.
Three attempts were made to contact each dispensary within listed business hours. If all three attempts were unsuccessful, the dispensary was recorded as “unavailable”. The dispensary was also considered “unavailable” if no phone number was identified for the location, or if the location never opened or had yet to open. Unavailable dispensaries were replaced with another randomly selected dispensary within the same stratum as noted above. The caller did not request any identifying information about the dispensary employee.
The primary outcome was the proportion of cannabis dispensaries that recommended cannabis use to a pregnant caller reporting nausea in the first trimester. Secondary outcomes included mention of maternal or fetal risks, stated benefits of cannabis use during pregnancy, specific product recommendations including dosing and frequency of use, warning of possible legal consequences, further discussion with a health care provider, length of phone call, rationale for product recommended, and reported source of information on which recommendations were based.
It was hypothesized that 50% of dispensaries would recommend cannabis use to a pregnant caller (the primary outcome). A sample size of 400 was targeted to yield a two-sided 95% CI with width of 10%. The proportions of the primary and secondary endpoints were summarized as percentage and exact 95% confidence interval overall, by three-category dispensary type, and two-category population density (urban versus rural). Method of delivery (i.e. inhalation, topical, edible) was compared across type of product recommended. Differences in endpoints by dispensary type and population density were tested using an exact Pearson chi-square test. Skewed continuous variables (i.e. call duration) were summarized with geometric mean and 95% confidence intervals. Representative quotations from retailers about the nature of the advice were selected to add context to reported quantitative data.
Results
Calls were completed in June and July 2017. Investigators contacted 465 dispensaries. Valid calls were achieved in 76% of calls to retail dispensaries, 75% of medical dispensaries and 89% of both license-type dispensaries (P=0.001). This resulted in 400 valid calls and achieved the target sample size (n=400) of responses (Figure 1). The average length of phone call was 2.4 minutes (95% CI 2.3 – 2.6 minutes). Of the 400 dispensaries included, 37% were licensed as medical (n=148), 35% were licensed as both medical and retail (n=141), and 28% as retail only (n=111). Additionally, 80.0% were urban and 20.0% were rural.
Figure 1.
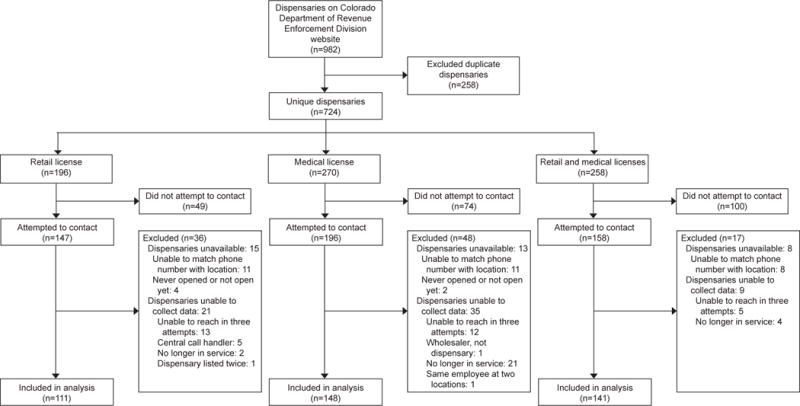
Study population flow diagram.
The majority, 69% (277/400), recommended cannabis products for “morning sickness” (95%CI 64-74%). Frequency of recommendation differed by license type (medical 83.1%, retail 60.4%, both 61.7%, p<0.001), with medical dispensaries recommending most frequently. Recommendations for use were similar by population density (urban 71% vs rural 63%, p=0.18). Of the 277 dispensaries that recommended a product, 65% based their recommendation for use in pregnancy on personal opinion, 30% did not specify a reason, and 36% stated cannabis use is safe in pregnancy (Table 1). Recommendations based on personal opinion differed by dispensary type, with medical dispensaries most frequently basing their recommendation on personal opinion (medical 85%, retail 57%, both 45%, p<0.001). Some dispensary employees (9%, 36/400), initially stated they could not recommend any products, but then proceeded to give a recommendation, which occurred similarly by dispensary type (8.8% medical, 7.2% retail, 10.6% both, p=0.65). Recommendations for use and basis for recommendations did not differ based on population density (Table 2).
Table 1.
Cannabis use guidance among medical, retail, and both dispensaries who recommended products for nausea in pregnancy
| Response from dispensary to “pregnant” caller | Overall | Medical License | Retail License | Medical and Retail License | P value* |
|---|---|---|---|---|---|
| Primary Outcome | n=400 | n=148 | n=111 | n=141 | |
| Recommended cannabis† | 69(64–74) | 83(76–89) | 60(51–70) | 62(53–70) | <0.001 |
| Secondary Outcomes | n=277 | n=123 | n=67 | n=87 | |
| Report of recommendation for use based on: | |||||
| Personal opinion | 65(59–71) | 85(77–90) | 57(44–69) | 45(34–56) | <0.001 |
| Referenced research | 6(3–9) | 7(3–14) | 3(0–10) | 6(2–13) | 0.46 |
| Referenced dispensary policy | 1(0–3) | 1(0–5) | 0(0–5) | 1(0–6) | >0.99 |
| Deferred to health care provider | 3(1–6) | 2(0–6) | 0(0–5) | 7(3–15) | 0.014 |
| Did not specify | 30(24–35) | 9(5–16) | 40(28–53) | 50(39–61) | <0.001 |
| Reported safety of cannabis use: | |||||
| Stated cannabis use safe | 36(30–42) | 41(32–50) | 28(18–41) | 34(25–45) | 0.24 |
| Potential for fetal harm | 5(3–8) | 4(1–9) | 1(0–8) | 8(3–16) | 0.15 |
| Potential for both fetal and maternal harm | 2(1–4) | 2(0–6) | 4(1–13) | 0(0–4) | 0.11 |
| Unsure or depends on certain criteria | 53(47–59) | 53(44–62) | 55(43–67) | 53(42–64) | 0.95 |
| Deferred to health care provider | 15(11–20) | 15(9–22) | 15(7–26) | 15(8–24) | >0.99 |
All data presented as percent (exact 95% CI). Responses are not mutually-exclusive.
P values for 3×2 comparisons using a Pearson exact chi-square.
Provides denominator for percentages in remainder of rows.
Table 2.
Cannabis use guidance among urban and rural dispensaries who recommended products for nausea in pregnancy
| Response from dispensary to “pregnant” caller | Urban | Rural | P value* |
|---|---|---|---|
| Primary Outcome | n=320 | n=80 | |
| Recommended cannabis† | 71(66-76) | 63(51-73) | 0.18 |
| Secondary Outcomes | n=227 | n=50 | |
| Report of recommendation for use based on: | |||
| Personal opinion | 67(61-73) | 56(41-70) | 0.14 |
| Referenced research | 5(2-9) | 10(3-22) | 0.18 |
| Referenced dispensary policy | 1(0-3) | 0(0-7) | >.99 |
| Deferred to health care provider | 3(1-6) | 4(0-14) | 0.64 |
| Did not specify | 28(22-35) | 36(23-51) | 0.31 |
| Reported safety of cannabis use: | |||
| Stated cannabis use safe | 35(29-42) | 38(25-53) | 0.75 |
| Potential for fetal harm | 5(2-9) | 4(0-14) | >.99 |
| Potential for both fetal and maternal harm | 1(0-4) | 4(0-14) | 0.22 |
| Unsure or depends on certain criteria | 54(47-60) | 52(37-66) | 0.88 |
| Deferred to health care provider | 16(12-22) | 8(2-19) | 0.19 |
All data presented as percent (exact 95% CI). Responses are not mutually-exclusive.
P values for 2×2 comparisons using a Pearson exact chi-square.
Provides denominator for percentages in remainder of rows.
Overall, 35.7% (n= 99) endorsed safety of cannabis products during pregnancy. The proportion of dispensaries that endorsed safety did not differ by dispensary type (medical 40.7%, retail 28.4%, and both 34.5%, p=0.24). Only 4.7% reported a risk of fetal harm and 1.8% reported a risk of both maternal and fetal harm. The proportion endorsing risk did not differ by dispensary type (Table 1) or by population density (Table 2). One dispensary employee stated, “After 8 weeks everything should be good with consuming like alcohol and weed and stuff, but I would wait an extra week.”
Of the 277 dispensaries that recommended cannabis use, 99% (n=275) recommended a specific cannabis type. All products were recommended at similar rates by dispensary type; 26% recommended use of cannabidiol (CBD) only products, 17% tetrahydrocannabinol (THC) only products, and the remaining (56%) recommended products with both CBD and THC (p=0.40).
Not all dispensaries recommended a specific method of delivery (i.e. inhalation, edible) and some recommended more than one method. Of the 277 that recommended marijuana, 90% (248/277) recommended a method of use, the most frequently recommended methods were edibles (50.5%), inhalation (37.9%), and tinctures (32.1%), followed by topical, including salve, spray, and lotion (18.1%), pills (16.6%), drinks (11.6%), and concentrate (5.8%).
Among all dispensaries, in response to whether the caller should discuss cannabis use with a health care provider, 13.5% of dispensaries stated they were unsure or equivocal; this differed by dispensary type (medical 16.9%, retail 16.2%, and both 7.8%, p=0.046). Overall, 81.5% of dispensaries recommended discussion of cannabis use with a health care provider (medical 79.7%, retail 80.2%, and both 84.4%, p=0.55). However, only 31.8% of all dispensaries made the recommendation to talk to a health care provider (medical 33.8%, retail 24.3%, and both 35.5%, p=0.02) without prompting, with retail only dispensaries being least likely to make this recommendation. One dispensary employee stated, “Highly, highly recommend talking to your doctor. Always tell your doctor everything you’re putting in your body.”
While the majority of dispensaries encouraged discussion with a health care provider, approximately one fourth (24.6%) of dispensaries recommended the caller obtain more information by doing on-line research, and this was not significantly different by dispensary type (medical 23.3%, retail 32.4%, and both 19.9%, p=0.06). Rural dispensaries were more likely to recommend use of the Internet to research cannabis use in pregnancy (urban 22.9% versus rural 31.7%, p=0.11). No other comparisons by urban versus rural yielded significant differences (data not shown). Callers were warned of possible drug testing during pregnancy (14.1%); this differed by license type (medical 22.1%, retail 7.2%, and both 11.4%, p=0.002) with medical dispensaries most frequently endorsing this warning.
Of the 123 dispensaries that did not initially recommend using a cannabis product, only one dispensary (0.8%) proceeded to give a recommendation when the caller disclosed she had a medical marijuana card (p>0.99). In all other cases, there was still no recommendation made when the caller disclosed she had a medical marijuana card.
Box 2 includes additional representative quotes from dispensary employees in response to the open-ended standardized phone script questions. The response may not necessarily be directly associated with the specific question due to the open-ended nature of the questions.
Box 2. Representative quotes from cannabis dispensary employees in response to phone script questions*.
“I’m calling because I’m eight weeks pregnant and nauseated. Are there any products that are recommended for morning sickness?
|
Why is the product recommended or not recommended?
|
Recommendations on frequency
|
Responses regarding speaking with a health care provider
|
Is cannabis safe to take during pregnancy?
|
The response may not be directly associated with the direct question due to the open-ended nature of the question.
Discussion
The majority of cannabis dispensaries in Colorado recommended cannabis products for morning sickness and their recommendation for use was based predominantly on personal opinion. Medical dispensaries were more likely than retail or both license type dispensaries to recommend cannabis products. The type of cannabis product most frequently endorsed was combined THC and CBD and the most frequently recommended method of use was edibles. Although 80% of dispensary respondents ultimately recommended discussion with a health care provider, the majority needed prompting before making this recommendation.
Given the concern for potential adverse effects on the fetus with maternal cannabis use, ACOG recommends against the use of cannabis products in women who are pregnant. 1,2 Public health efforts in Colorado, the first state to legalize marijuana for recreational use, have similarly focused on discouraging cannabis use during pregnancy and lactation.10 According to the Code of Colorado Regulations, all cannabis products in the state of Colorado are required to have the following statement on every container: “There may be additional health risks associated with the consumption of this product for women who are pregnant, breastfeeding, or planning on becoming pregnant.”6,7 Despite this warning, Colorado and other states that have legalized marijuana, have refrained from prohibiting marijuana use during pregnancy.11–13 There are currently no regulations about recommendations or advice that cannabis dispensaries can provide to customers in Colorado.6,7
Our findings are consistent with other studies in that the majority of advice given by cannabis dispensary employees appears to be based on personal opinion. A study by Haug et al found that only 20% of cannabis dispensary employees received formal medical or scientific training.14 Further, 71% of these employees reported giving recommendations about cannabis products based on personal experience. In another study, in which 56% of dispensary employees had received formal training; only 47% thought that medical decision-making was important when recommending cannabis products. Also, most preferred a patient-centered philosophy (77%) versus that of a dispensary staff-centered philosophy (23%).15
The majority of the limitations of this study were related to appropriate identification of operating dispensaries. The Colorado Marijuana Enforcement Division has an accurate list of all state licenses that have been issued, but this list does not necessarily correspond to stores that are currently open. Therefore, some dispensaries did not have a valid phone number, which may have resulted in selection bias. In addition, all dispensaries routing calls to a “call center” were excluded. Despite this, it is possible that there were “chains” of marijuana dispensaries with similar policies but unique addresses and phone numbers that could have influenced our results. However, the mystery caller design reflects “real world” situations and allows for description of the advice pregnant women receive when calling operating, licensed dispensaries. Finally, our sample size was calculated for our primary outcome and may have been inadequate for some of the secondary outcomes; therefore, non-significant results should not be interpreted as equivalent.
We recognize that recommendations from cannabis dispensary employees may vary depending upon who took the call at a given time and may not be representative of all employees at the dispensary. It is possible that some dispensaries have a policy in place for cannabis use in pregnancy that individual employees did not follow based on personal views. Although the phone script was piloted in dispensaries outside of Colorado, no dispensaries outside of Colorado were included and, thus, these findings may not be generalizable to other states with legalized cannabis. Also, the level of education and medical background of the dispensary representative was unknown.
This study has several strengths. The random selection of cannabis dispensaries was stratified to ensure distribution across the state and across different license types, and selection was from the list of all licensed dispensaries, which strengthens generalizability of results to all dispensaries in Colorado. Further, this study was conducted in Colorado, which was one of the first states to legalize cannabis products. Thus, it is likely that some dispensary respondents have prior experience with pregnant customers requesting advice about cannabis use.
This study prompts many questions about laws and regulations pertaining to cannabis dispensaries. As cannabis legalization becomes more common, women should be cautioned that advice from dispensary employees might not necessarily be informed by medical evidence. Future studies should focus on the effects of maternal cannabis use on maternal and neonatal outcomes, in hopes of being able to provide guidelines to care for pregnant women. Public health initiatives should consider collaborating with dispensary owners and other valuable stakeholders in conversations about standards for advice provided to pregnant women.
Acknowledgments
Dr. Metz is supported by the National Institute on Child Health and Human Development under award number 5K12HD001271-18. This project was also supported by Colorado Clinical and Translational Sciences Institute (CCTSI) with the Development and Informatics Service Center under award number UL1 RR025780. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Financial Disclosure
Dr. Borgelt received grant funding from the Colorado Department of Public Health and Environment (CDPHE) for a study evaluating the use of cannabidiol for the treatment of refractory pediatric epilepsy. Additionally she has served on seven different working groups for the Colorado Department of Revenue and CDPHE regarding use of cannabis and patient safety.
Footnotes
Presented as a poster at the Society for Maternal-Fetal Medicine 38th Annual Meeting, Dallas, TX, February 1, 2018.
The other authors did not report any potential conflicts of interest.
Each author has indicated that he or she has met the journal’s requirements for authorship.
References
- 1.National Academies of Sciences, Engineering, and Medicine. The health effects of cannabis and cannabinoids: The current state of evidence and recommendations for research. Washington, DC: The National Academies Press; 2017. [PubMed] [Google Scholar]
- 2.Marijuana use during pregnancy and lactation Committee Opinion No. 722. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2017;130:e205–9. doi: 10.1097/AOG.0000000000002354. [DOI] [PubMed] [Google Scholar]
- 3.Jarlenski M, Koma JW, Zank J, Bodnar LM, Bogen DL, Chang JC. Trends in perception of risk of regular marijuana use among US pregnant and nonpregnant reproductive-aged women. American Journal of Obstetrics and Gynecology. 2017;217(6):705–707. doi: 10.1016/j.ajog.2017.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Retail Marijuana Public Health Advisory Committee. Changes in Marijuana Use Patterns, Systematic Literature Review, and Possible Marijuana-Related Health Effects. Colorado Department of Public Health and Environment; 2016. Monitoring Health Concerns Related to Marijuana in Colorado: 2016. https://drive.google.com/file/d/0B0tmPQ67k3NVQlFnY3VzZGVmdFk/view. [Google Scholar]
- 5.Enforcement Division. MED Licensed Facilities. Colorado Department of Revenue; 1016. https://www.colorado.gov/pacific/enforcement/med-licensed-facilities. Accessed December 1, 2016.
- 6.Marijuana Enforcement Division. Medical Marijuana Rules: 1 CCR 212-1. Code of Colorado Regulations: Secretary of State, State of Colorado. 2017 https://www.colorado.gov/pacific/sites/default/files/1_CCR212-1_Medical.pdf. Accessed October 1, 2017.
- 7.Marijuana Enforcement Division. Retail Marijuana Rules: 1 CCR 212-2. Code of Colorado Regulations: Secretary of State, State of Colorado. 2017 https://www.colorado.gov/pacific/sites/default/files/Complete_Retail_Marijuana_Rules_as_of_April_14_2017.pdf. Accessed October 1, 2017.
- 8.Map Resources. Colorado Rural Health Center; http://coruralhealth.org/resources/maps-resource. Accessed 2017. [Google Scholar]
- 9.Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of biomedical informatics. 2009;42:377–81. doi: 10.1016/j.jbi.2008.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.How Marijuana Affects Pregnant & Breastfeeding Women. Colorado Department of Public Health and Environment; https://goodtoknowcolorado.com/health-effects/pregnant-and-breastfeeding-mothers. Accessed October 1, 2017. [Google Scholar]
- 11.Colorado Department of Public Health and Environment. Marijuana Pregnancy and Breastfeeding Guidance. 2017 https://www.colorado.gov/pacific/sites/default/files/MJ_RMEP_Pregnancy-Breastfeeding-Clinical-Guidelines.pdf. Accessed October 1, 2017.
- 12.U.S. Department of Health and Human Services. FDA and Marijuana. U.S. Food and Drug Administration; 2017. https://www.fda.gov/newsevents/publichealthfocus/ucm421163.htm. Accessed October 1, 2017. [Google Scholar]
- 13.Qualifying medical conditions Medical Marijuana Registry. Colorado Department of Public Health and Environment; 2017. https://www.colorado.gov/pacific/cdphe/qualifying-medical-conditions-medical-marijuana-registry. Accessed October 1, 2017. [Google Scholar]
- 14.Haug NA, Kieschnick D, Sottile JE, Babson KA, Vandrey R, Bonn-Miller MO. Training and Practices of Cannabis Dispensary Staff. Cannabis and Cannabinoid Research. 2016;1(1):244–251. doi: 10.1089/can.2016.0024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Peiper NC, Gourdet C, Meinhofer A, Reiman A, Reggente N. Medical Decision-Making Processes and Online Behaviors Among Cannabis Dispensary Staff. Substance Abuse: Research and Treatment. 2017;11 doi: 10.1177/1178221817725515. 1178221817725515. [DOI] [PMC free article] [PubMed] [Google Scholar]