

Sir,
We read Singh and Chowdhary's letter,[1] in which they report the use of ultrasound-guided erector spinae plane block (ESPB) for post-operative analgesia in radical mastectomy.
Forero first described ESPB for thoracic neuropathic pain in a four-case series and cadaveric study.[2] In the first case, the authors successfully applied local anaesthesia (LA) in the interfascial plane between rhomboideus major muscle (RMM) and erector spinae muscle (ESM). This technique failed in the second patient, and subsequent ESPB was performed deep to ESM. In their discussion, the authors clearly state that 'the cadaveric findings and our subsequent clinical experience indicate that the optimal plane for injection in the ESP block is deep to the ESM rather than superficial to it.'[2] All subsequent studies of ESPB have used this technique.[3,4]
In their letter, Singh and Chowdhary[1] state that the LA is applied to the interfascial plane between the RMM and the ESM. However, in Figure 1, the needle tip is between the transverse process and ESM, the mark 'Es' is not above the ESM but is deeper and in the marking area in which the superior costochondral ligament lies.
Figure 1.
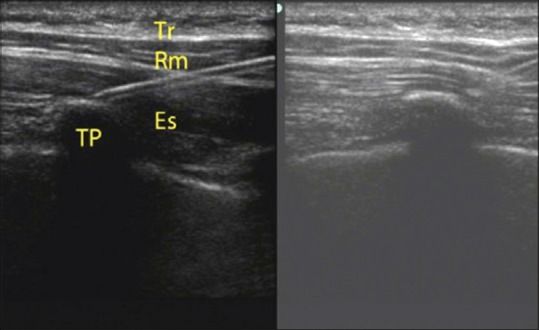
Singh and Chowdhary's letter. Localisation of the space and drug injection. Tr: Trapezius, Rm: Rhomboideus major, Er: Erector spinae, TP: Transverse process
The discrepancy between the text and figure must be corrected, and the technique should be clearly defined. If the authors chose to perform this block between RMM and ESM, they must further elaborate on why this was chosen. We feel that these points must be clarified as ESPB is an increasingly popular regional anaesthetic technique and such reports shape future research in this area.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Singh S, Chowdhary NK. Erector spinae plane block an effective block for post-operative analgesia in modified radical mastectomy. Indian J Anaesth. 2018;62:148–50. doi: 10.4103/ija.IJA_726_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: A novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41:621–7. doi: 10.1097/AAP.0000000000000451. [DOI] [PubMed] [Google Scholar]
- 3.Chin KJ, Adhikary S, Sarwani N, Forero M. The analgesic efficacy of pre-operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia. 2017;72:452–60. doi: 10.1111/anae.13814. [DOI] [PubMed] [Google Scholar]
- 4.Adhikary SD, Pruett A, Forero M, Thiruvenkatarajan V. Erector spinae plane block as an alternative to epidural analgesia for post-operative analgesia following video-assisted thoracoscopic surgery: A case study and a literature review on the spread of local anaesthetic in the erector spinae plane. Indian J Anaesth. 2018;62:75–8. doi: 10.4103/ija.IJA_693_17. [DOI] [PMC free article] [PubMed] [Google Scholar]