

Abstract
Acute heart failure (AHF) is a life-threatening condition requiring immediate treatment. The initial therapy should take into account the clinical presentation, pathophysiology at play, precipitating factors and underlying cardiac pathology. Particular attention should be given to polymorbidity and the avoidance of potential iatrogenic harm. Patient preferences and ethical issues should be integrated into the treatment plan at an early stage. The average survival of AHF patients is 2 years and the most vulnerable period is the 3-month time window directly after discharge. Reducing both persistent subclinical congestion and underutilisation of disease-modifying heart failure therapies as well as ensuring optimal transitions of care after hospital discharge are essential in improving outcomes for AHF patients.
Keywords: Acute heart failure, cardiogenic shock, pathophysiology, treatment, precipitating factors, vulnerable phase
Heart failure is a clinical syndrome induced by cardiac abnormalities resulting in reduced cardiac output and/or elevated intra-cardiac enddiastolic pressures and causing symptoms that are often accompanied by typical physical signs.1 Demographic changes, improved treatment of several acute cardiac disorders, such myocardial infarction, arrhythmia and congenital heart disease, and increased long-term survival of patients with reduced left ventricular systolic function have led to a dramatic increase in the number of patients living with heart failure.
Acute heart failure (AHF) is defined as new-onset or worsening of symptoms and signs of heart failure.1 AHF is the most frequent cause of unplanned hospital admission in patients aged 65 years or older and is characterised by significant in-hospital mortality and frequent readmissions.2,3 Outcomes of AHF remain globally poor.4,5 Independent of ejection fraction, the average survival after hospitalisation for AHF is 2 years, with the most vulnerable phase being in the months directly after discharge from hospital. Despite significant achievements in the treatment of chronic heart failure, all trials targeting AHF with short-term in-hospital therapies have had disappointing or at most neutral endpoints. Thus, the optimal strategy for improving longterm outcomes in patients admitted with AHF should be revisited. Optimisation, personalisation and continuation of (A)HF treatment after hospital discharge seem crucial to achieving the best outcomes. This article reviews the principles of optimisation and personalisation of AHF treatment during the hospital stay and early outpatient phase.
Triage and the Initial 7-P Evaluation
Patients presenting with (suspected) AHF should undergo rapid triage to exclude cardiogenic shock, respiratory failure, myocardial infarction and/or arrhythmia and receive the appropriate level of monitoring and specific treatments (e.g. pharmacological/mechanical haemodynamic support, mechanical ventilation and percutaneous revascularisation).1,6,7 Moreover, since AHF is a life-threatening condition, initial treatment should be started as soon as possible, ideally within 30–60 min after hospital admission, as this is associated with better outcomes.6–8 The initial treatment should then be tailored and optimised according to a 7-P evaluation: phenotype, pathophysiology, precipitants, pathology, polymorbidity, potential harm and preferences (Figure 1).9
Figure 1: The 7-P Initial Evaluation of Acute Heart Failure Patients.
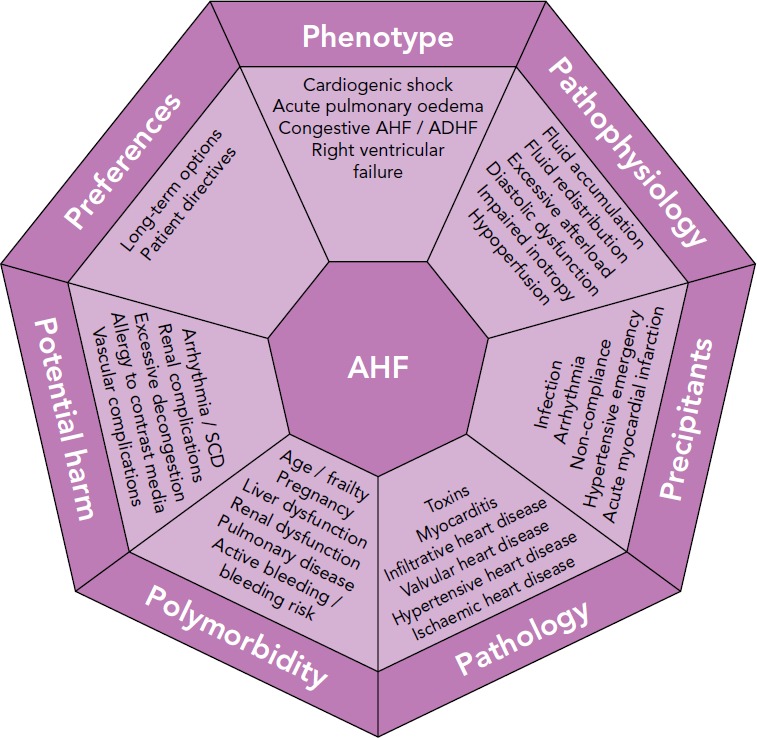
ADHF = acute decompensated heart failure; AHF = acute heart failure; SCD = sudden cardiac death. Adapted from Arrigo et al., 2017.9
Phenotype
The initial evaluation should include the assessment of the clinical phenotype based on symptoms or signs of peripheral hypoperfusion (forward failure) and/or systemic congestion (backward failure). However, given the limited sensitivity and specificity of clinical assessment, additional confirmatory tests may be required, such as biomarkers, echocardiography, lung ultrasound or chest X-ray, to exclude differential diagnoses.
The vast majority of AHF patients are well perfused but congested (warm-wet), while only a minority are hypoperfused (either cold-wet or cold-dry). Hypoperfusion defines cardiogenic shock, the most severe clinical presentation of AHF, which accounts for only about 10 % of AHF cases. However, the treatment of these patients is often more difficult and is associated with 5- to 10-fold higher in-hospital mortality compared to normally perfused cases.4,10 Systemic congestion, in contrast, is widespread and results from the combination of fluid accumulation and redistribution due to a change in vascular compliance, with variable proportions according to the clinical scenario. Fluid accumulation is found predominantly in cases of acute decompensation in chronic heart failure with reduced systolic function, while fluid redistribution mostly occurs in new-onset AHF patients with preserved systolic function and/or systemic inflammation.
Pathophysiology
The second step in the evaluation of AHF patients should focus on understanding the leading pathophysiology at play. AHF can be a consequence of arrhythmia (with and without atrio- or interventricular asynchrony), anatomical defects, incompetent valves, impaired myocardial contractility, pathological myocardial relaxation, hampered ventricular filling and/or excessive cardiac afterload.
As already mentioned, systemic congestion is the central feature of AHF and results from the combination of fluid accumulation and redistribution induced by neurohumoral activation in the presence of cardiac dysfunction.11 Hypoperfusion manifests only in the most severe forms of AHF (cardiogenic shock) in the presence of severely impaired cardiac output.12 In patients without a previous history of symptomatic heart failure (de novo AHF), AHF mostly occurs secondary to a sudden deterioration in cardiac function – due to myocardial infarction, severe myocarditis or acute valve regurgitation, for example – causing fluid redistribution and, in severe forms, peripheral hypoperfusion.3 These patients have no or only minor increases in body weight before hospital admission. Fluid redistribution and loss due to sweating, perspiratio insensibilis or diuretic therapy can cause intravascular hypovolaemia and insufficient preload. Consequent sympathetic activation induces transient vasoconstriction leading to rapid volume displacement from the peripheral and splanchnic venous systems to the pulmonary circulation.13,14 A mismatch in the ventricular– arterial coupling relationship, with increased afterload and decreased venous capacitance (increased preload), is the primary alteration in hypertensive AHF.15,16
More frequently, AHF consists of acute decompensation of chronic heart failure (ADHF) and is caused by progressive fluid accumulation. Indeed, persistent neurohumoral activation impairs renal sodium excretion, resulting in sodium and then fluid accumulation.17 The classical congestive cascade includes subclinical stages characterised by increased cardiac filling and venous pressures (haemodynamic congestion), followed by redistribution of fluids into the lungs and visceral organs (organ congestion) and finally to overt symptoms and signs of volume overload (clinical congestion) (Figure 2).11 Although clinical and organ congestion usually follows haemodynamic congestion, the correlation between hydrostatic pressure and oedema formation is weak. Indeed, chronic sodium accumulation in heart failure impairs the function of the interstitial glycosaminoglycan network, reducing its capacity to buffer additional sodium and maintain low interstitial compliance.18 Consequently, interstitial oedema formation may occur even in the presence of mildly elevated hydrostatic pressures and vascular capacitance may change, causing increased cardiac filling pressures without increments in vascular or total body fluid.
Figure 2: The Typical Cascade of Systemic Congestion.
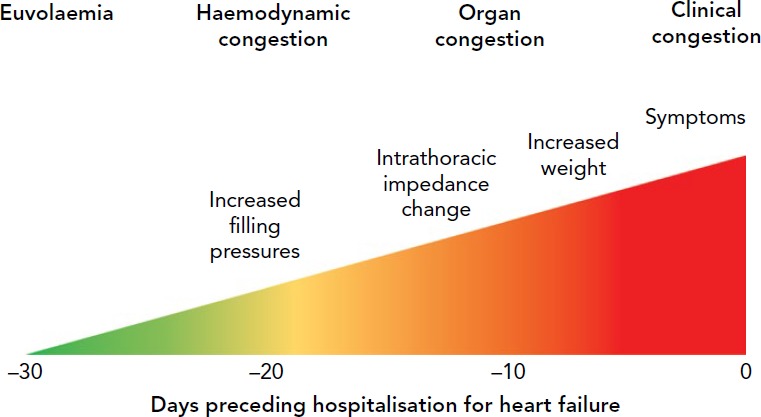
Modified from Adamson, 2009.49 Published with permission from Springer Nature.
Precipitants
During the third step, triggers of AHF should be identified. AHF may be precipitated by several factors that may coexist, such as myocardial ischaemia, arrhythmias, infections, uncontrolled hypertension and non-compliance with medical prescriptions.2,19,20 In patients presenting with cardiogenic shock, myocardial infarction is by far the most common precipitant.10 The aims when identifying precipitants are to detect treatable causes (see below) and provide prognostic information. AHF precipitated by an acute coronary syndrome or infection is associated with poorer outcomes; whereas outcomes tend to be better in AHF precipitated by atrial fibrillation or uncontrolled hypertension.2,20,21
Pathology
The initial treatment of AHF should be started as soon as possible according to the clinical presentation. However, understanding of the underlying cardiac pathology is essential for providing optimal specific therapy and estimating prognosis. For example, giant cell myocarditis requires aggressive immunosuppressive therapy, while severe mitral regurgitation caused by papillary muscle rupture requires cardiac surgery.22 Moreover, end-stage ischaemic heart disease without reversible ischaemia and viability may display significantly lower recovery potential than peripartum cardiomyopathy.23 Infiltrative heart disease may involve other organ systems. Immediate echocardiography is recommended in patients presenting with cardiogenic shock or de novo AHF.1,6
Polymorbidity
AHF is a syndrome causing organ dysfunction, mainly of the lungs and abdominal organs.24–26 Historically, renal and hepatic dysfunctions in heart failure have been considered the consequence of visceral hypoperfusion, but more recent data have shown that venous congestion is the strongest haemodynamic determinant of renal and hepatic dysfunction in AHF.27,28 Assessment of organ dysfunction – in particular severe renal and kidney failure – as well as other conditions causing relative contraindications to diagnostics or treatment – such as allergy, pregnancy or active bleeding – are crucial in deciding on optimal diagnostic modalities and treatments to be delivered. Rapid assessment of frailty is recommended in geriatric patients, since it affects overall outcome.29,30 Metabolic disturbances, such as diabetes or thyroid disease, anaemia and iron deficiency should be assessed and optimised.
Potential Harm
It is crucial to consider the risk of iatrogenic harm associated with diagnostics and treatment in every medical decision made. This is even more important in the treatment of AHF patients – a population of older, critically-ill, polymorbid subjects.31 For example, indiscriminate use of diagnostics (e.g. coronary angiography) and monitoring (e.g. pulmonary artery catheter) may expose patients to severe vascular or radiological complications; excessive use of inotropic agents in the absence of evidence of peripheral hypoperfusion is associated with arrhythmia and excess mortality.32,33
Patient Preferences
The seventh part of the initial evaluation of AHF patients should focus on patient preferences and ethical issues. Discussion with the patient (if feasible) or with relatives about resuscitation directives and treatment options may be time-consuming but is crucial to avoid overtreatment. Importantly, long-term options, such as mechanical assist devices or transplantation, and the wishes of the patient need to be evaluated early rather than late, particularly in AHF patients with the potential for rapid deterioration. In the absence of long-term therapeutic options, palliation and supportive care should be offered to patients. Relatives should be advised of these options if patients are not in a position to consent.34
Treatment at Hospital Admission
Correctly deciding which phenotype/pathophysiology predominates is critical in determining which treatment strategy should be used.35 At hospital admission, AHF patients displaying evidence of congestion should receive decongestive treatment such as vasodilators and/or diuretics.8,36 While diuretics are mainly used in the presence of fluid overload, vasodilators are administered to reduce filling pressures in the presence of fluid redistribution and preserved systolic blood pressure (>110 mmHg; more cautiously between 90 and 110 mmHg). Decongestive therapy should be started as soon as possible and titrated according to clinical response.8 Notably, decongestive therapy should be continued beyond the improvement of symptoms and clinical evidence of organ congestion and maintained until euvolaemia is achieved (Figure 2).
The use of inotropes should be restricted to patients in cardiogenic shock due to impaired myocardial contractility, since their inappropriate use is associated with increased morbidity and mortality.37 In cases of persistent haemodynamic instability despite escalating doses of inotropes, mechanical circulatory support such as veno–arterial extracorporeal life support and percutaneous left-ventricular assist devices should be considered before irreversible organ failure has established.7 In severe pulmonary oedema causing hypoxia, high-flow oxygen therapy, non-invasive or invasive mechanical ventilation are required to ensure oxygenation.
In addition to decongestive therapy, initial management should include specific treatments directed towards decompensation triggers and the underlying cardiac disorders. In particular, early coronary angiography with revascularisation is recommended in AHF precipitated by acute coronary syndrome. Antiarrhythmic treatment and/or electrical cardioversion are recommended in AHF precipitated by arrhythmia. Rapid initiation of antimicrobial therapy is recommended for AHF precipitated by infection/sepsis. Sometimes, percutaneous or surgical treatment of structural heart disease is required to achieve durable stabilisation. Finally, patients should be maintained on oral diseasemodifying heart failure treatment whenever possible.1
After delivery of the initial treatment, continuous reassessment of clinical response and patient allocation in terms of level of care should be ensured. The level of care (discharge home, observation, ward, telemetry or intensive/intermediate care unit) should integrate symptom severity, precipitating factors, haemodynamic and respiratory status, the degree of congestion and biomarkers (i.e. natriuretic peptides, troponin, renal function and serum lactate) and the patient’s general condition. Most patients require hospital admission, about half of them to intensive or intermediate care units. Low-risk patients with good response to initial therapy may be considered for early discharge.
Treatment Before Discharge and the First Outpatient Visit
The optimal time-point for discharging hospitalised AHF patients may be difficult to determine due to the need to balance patient preferences, healthcare resources and the risk of adverse outcomes. Indeed, the risk of death is high during hospitalisation for AHF but is even higher during the immediate post-discharge period, which usually lasts 2–3 months and is known as the vulnerable phase.38 Therefore, optimal transitions of care after hospital discharge may be even more important than the delivery of appropriate treatments during hospitalisation in reducing adverse outcomes in AHF patients.
Since the causes of the vulnerable phase remain controversial, identification of patients at particularly high risk of adverse outcomes after hospital discharge is particularly challenging. A combination of pathophysiological disorders and lack of follow up seems to contribute to the high mortality and readmission rates observed. Several risk scores using multiple clinical variables have been developed, but most of them are complex and lack accuracy. Cardiovascular biomarkers added to clinical parameters may reveal active sub-clinical processes, providing valuable insights into the pathophysiology of the vulnerable phase and increasing prognostic accuracy. In the future, a comprehensive multi-marker strategy reflecting different activated pathways in heart failure (myocardial stress, myocyte injury, neurohumoral activation, inflammation, oxidative stress, matrix remodelling and systemic congestion) may increase the precision of biomarker-guided prognostication.39 Even more importantly, the prognostic information derived from a single or multi-marker strategy may be translated into therapeutic decisions and personalisation of follow up, improving patient outcomes.
Persistent subclinical congestion may contribute to the high rates of death and readmission observed after hospital discharge.40 Indeed, despite a global improvement in symptoms during hospital stay, a relevant proportion of patients still display markedly elevated natriuretic peptides at discharge. This discordance between few symptoms and high natriuretic peptide concentrations suggests persistent haemodynamic congestion. Some studies have reported an association between pre-discharge levels of natriuretic peptides and subsequent risk of death or readmission.41 Based on these data, titration of decongestive therapy based only on symptoms and signs may be insufficient and should include additional parameters, such as biomarkers and/or echocardiography.42,43
Underutilisation of disease-modifying heart failure therapies such as betablockers, renin–angiotensin system (RAS) inhibitors and mineralocorticoid receptor antagonists is prevalent and may further promote adverse events after hospital discharge.5,44 Beta-blocker discontinuation during hospitalisation is associated with detrimental effects on short-term mortality and readmission.45 Very recently, a large propensity scorematched cohort study showed an association between beta-blocker or RAS inhibitor treatment at hospital discharge and a 40–50 % relative risk reduction in 90-day mortality.44 It showed an additional 25–50 % relative risk reduction with combined beta-blocker and RAS inhibitor therapy at hospital discharge compared to either treatment alone.44 The early benefits were present in both reduced and preserved ejection fraction and persisted at 1-year follow up. In the same study, no significant benefit was found with early mineralocorticoid receptor antagonist administration. In beta-blocker-intolerant patients, early administration of ivabradine might be considered to reduce readmissions during the vulnerable phase.46 Current European Society of Cardiology guidelines recommend initiation or continuation of disease-modifying heart failure therapies during hospitalisation in all AHF patients with reduced ejection fraction unless contraindicated.1 Similarly, evaluation of the patient to determine whether a cardiac device (implantable cardiac defibrillator and/or cardiac resynchronisation therapy) is indicated and, if so, planning for its implantation should not be overlooked.
Furthermore, hospital discharge should occur only after precipitating factors of AHF have been adequately treated and resolved. This point includes revascularisation for myocardial infarction, antiarrhythmic therapy for arrhythmias, antimicrobial treatment for infection, antihypertensive therapy for hypertension and patient education for non-compliance with recommendations. Patient education, home-based measurement of body weight and blood pressure, and early contact with healthcare providers have all been proposed to reduce readmission rates; however, these interventions have produced inconsistent results. Early detection of increasing congestion with intrathoracic impedance monitoring and implantable haemodynamic monitoring, e.g. with the CardioMEMS™ HF System (St Jude Medical), have shown promising results in trials but concerns about their cost-effectiveness has prevented their widespread introduction in clinical practice.47,48
Finally, hospital discharge should be planned to allow inclusion of all patients into a comprehensive, post-discharge care programme. If this is not feasible because of limited resources, entry to such a programme should be restricted to those with high-risk feature, such as markedly elevated natriuretic peptides, abnormal systolic blood pressure, persistent hyponatraemia and recurrent readmissions.38 Outpatient visits to a general practitioner and heart failure clinic should be scheduled before hospital discharge to ensure appropriate follow up. In our centres, we usually plan a visit to the general practitioner within 1 week and a visit to the heart failure clinic within 2–3 weeks after discharge.
During early outpatient visits, assessment and optimisation of volume status (including the comparison of natriuretic peptide concentration with pre-discharge values), up-titration of disease-modifying heart failure treatment and evaluation of cardiac device indication should be performed. After bridging the vulnerable phase, optimisation of oral disease-modifying treatments and regular follow-up visits should be continued on an individual basis.
Conclusion
The initial therapy of AHF should be personalised based on clinical phenotype, the pathophysiology at play, precipitants identified and underlying cardiac pathology. Particular attention should be given to polymorbidity, including organ dysfunction, and the avoidance of potential iatrogenic harm. Patient preferences and ethical issues should be integrated into the treatment plan at an early phase. Before hospital discharge, persistent subclinical congestion and underutilisation of disease-modifying heart failure therapies should be addressed and appropriate follow up ensured.
References
- 1.Ponikowski P, Voors AA, Anker SD et al. Authors/Task Force Members. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–200. doi: 10.1093/eurheartj/ehw128;. [DOI] [PubMed] [Google Scholar]
- 2.Arrigo M, Gayat E, Parenica J et al. GREAT Network. Precipitating factors and 90-day outcome of acute heart failure: a report from the intercontinental GREAT registry. Eur J Heart Fail. 2017;19:201–8. doi: 10.1002/ejhf.682;. [DOI] [PubMed] [Google Scholar]
- 3.Rudiger A, Harjola V-P, Müller A et al. Acute heart failure: clinical presentation, one-year mortality and prognostic factors. Eur J Heart Fail. 2005;7:662–70. doi: 10.1016/j.ejheart.2005.01.014;. [DOI] [PubMed] [Google Scholar]
- 4.Follath F, Yilmaz MB, Delgado JF et al. Clinical presentation, management and outcomes in the Acute Heart Failure Global Survey of Standard Treatment (ALARM-HF). Intensive Care Med. 2011;37:619–26. doi: 10.1007/s00134-010-2113-0;. [DOI] [PubMed] [Google Scholar]
- 5.Shah KS, Xu H, Matsouaka RA et al. Heart failure with preserved, borderline, and reduced ejection fraction: 5-year outcomes. J Am Coll Cardiol. 2017;70:2476–86. doi: 10.1016/j.jacc.2017.08.074;. [DOI] [PubMed] [Google Scholar]
- 6.Mebazaa A, Yilmaz MB, Levy P et al. Recommendations on pre-hospital and early hospital management of acute heart failure: a consensus paper from the Heart Failure Association of the European Society of Cardiology, the European Society of Emergency Medicine and the Society of Academic Emergency Medicine ? short version. Eur Heart J. 2015;36:1958–66. doi: 10.1093/eurheartj/ehv066;. [DOI] [PubMed] [Google Scholar]
- 7.Mebazaa A, Tolppanen H, Mueller C et al. Acute heart failure and cardiogenic shock: a multidisciplinary practical guidance. Intensive Care Med. 2016;42:147–63. doi: 10.1007/s00134-015-4041-5;. [DOI] [PubMed] [Google Scholar]
- 8.Matsue Y, Damman K, Voors AA et al. Time-to-furosemide treatment and mortality in patients hospitalized with acute heart failure. J Am Coll Cardiol. 2017;69:3042–51. doi: 10.1016/j.jacc.2017.04.042;. [DOI] [PubMed] [Google Scholar]
- 9.Arrigo M, Rudiger A. Acute heart failure: from pathophysiology to optimal treatment. Cardiovascular Medicine. 2017;20:229–35. [Google Scholar]
- 10.Harjola V-P, Lassus J, Sionis A et al. Clinical picture and risk prediction of short-term mortality in cardiogenic shock. Eur J Heart Fail. 2015;17:501–9. doi: 10.1002/ejhf.260;. [DOI] [PubMed] [Google Scholar]
- 11.Arrigo M, Parissis JT, Akiyama E, Mebazaa A. Understanding acute heart failure: pathophysiology and diagnosis. Eur Heart J Suppl. 2016;18(suppl G):G11–8. doi: 10.1093/eurheartj/suw044. [DOI] [Google Scholar]
- 12.Rudiger A. Understanding cardiogenic shock. Eur J Heart Fail. 2015;17:466–7. doi: 10.1002/ejhf.265;. [DOI] [PubMed] [Google Scholar]
- 13.Cotter G, Metra M, Milo-Cotter O et al. Fluid overload in acute heart failure ? re-distribution and other mechanisms beyond fluid accumulation. Eur J Heart Fail. 2008;10:165–9. doi: 10.1016/j.ejheart.2008.01.007;. [DOI] [PubMed] [Google Scholar]
- 14.Francis GS, Siegel RM, Goldsmith SR et al. Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Activation of the neurohumoral axis. Ann Intern Med. 1985;103:1–6. doi: 10.7326/0003-4819-103-1-1;. [DOI] [PubMed] [Google Scholar]
- 15.Gandhi SK, Powers JC, Nomeir AM et al. The pathogenesis of acute pulmonary edema associated with hypertension. N Engl J Med. 2001;344:17–22. doi: 10.1056/NEJM200101043440103;. [DOI] [PubMed] [Google Scholar]
- 16.Viau DM, Sala-Mercado JA, Spranger MD et al. The pathophysiology of hypertensive acute heart failure. Heart. 2015;101:1861–7. doi: 10.1136/heartjnl-2015-307461;. [DOI] [PubMed] [Google Scholar]
- 17.Mullens W, Verbrugge FH, Nijst P, Tang WHW. Renal sodium avidity in heart failure: from pathophysiology to treatment strategies. Eur Heart J. 2017;38:1872–82. doi: 10.1093/eurheartj/ehx035;. [DOI] [PubMed] [Google Scholar]
- 18.Nijst P, Verbrugge FH, Grieten L et al. The pathophysiological role of interstitial sodium in heart failure. J Am Coll Cardiol. 2015;65:378–88. doi: 10.1016/j.jacc.2014.11.025;. [DOI] [PubMed] [Google Scholar]
- 19.Fonarow GC, Abraham WT, Albert NM et al. Factors identified as precipitating hospital admissions for heart failure and clinical outcomes: findings from OPTIMIZE-HF. Arch Intern Med. 2008;168:847–54. doi: 10.1001/archinte.168.8.847;. [DOI] [PubMed] [Google Scholar]
- 20.Arrigo M, Tolppanen H, Sadoune M et al. GREAT Network. Effect of precipitating factors of acute heart failure on readmission and long-term mortality. ESC Heart Fail. 2016;3:115–21. doi: 10.1002/ehf2.12083;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Rudiger A, Streit M, Businger F et al. The impact of infections on critically ill acute heart failure patients: an observational study. Swiss Med Wkly. 2010;140:w13125. doi: 10.4414/smw.2010.13125. [DOI] [PubMed] [Google Scholar]
- 22.Ekström K, Lehtonen J, Kandolin R et al. Long-term outcome and its predictors in giant cell myocarditis. Eur J Heart Fail. 2016;18:1452–8. doi: 10.1002/ejhf.606;. [DOI] [PubMed] [Google Scholar]
- 23.Bauersachs J, Arrigo M, Hilfiker-Kleiner D et al. Current management of patients with severe acute peripartum cardiomyopathy: practical guidance from the Heart Failure Association of the European Society of Cardiology Study Group on peripartum cardiomyopathy. Eur J Heart Fail. 2016;18:1096–105. doi: 10.1002/ejhf.586;. [DOI] [PubMed] [Google Scholar]
- 24.Ronco C, Haapio M, House AA et al. Cardiorenal syndrome. J Am Coll Cardiol. 2008;52:1527–39. doi: 10.1016/j.jacc.2008.07.051;. [DOI] [PubMed] [Google Scholar]
- 25.Nikolaou M, Parissis J, Yilmaz MB et al. Liver function abnormalities, clinical profile, and outcome in acute decompensated heart failure. Eur Heart J. 2013;34:742–9. doi: 10.1093/eurheartj/ehs332;. [DOI] [PubMed] [Google Scholar]
- 26.Verbrugge FH, Dupont M, Steels P et al. Abdominal contributions to cardiorenal dysfunction in congestive heart failure. J Am Coll Cardiol. 2013;62:485–95. doi: 10.1016/j.jacc.2013.04.070;. [DOI] [PubMed] [Google Scholar]
- 27.Mullens W, Abrahams Z, Francis GS et al. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J Am Coll Cardiol. 2009;53:589–96. doi: 10.1016/j.jacc.2008.05.068;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ishihara S, Gayat E, Sato N et al. Similar hemodynamic decongestion with vasodilators and inotropes: systematic review, meta-analysis, and meta-regression of 35 studies on acute heart failure. Clin Res Cardiol. 2016;105:971–80. doi: 10.1007/s00392-016-1009-6;. [DOI] [PubMed] [Google Scholar]
- 29.Teixeira A, Arrigo M, Tolppanen H et al. Management of acute heart failure in elderly patients. Arch Cardiovasc Dis. 2016;109:422–30. doi: 10.1016/j.acvd.2016.02.002;. [DOI] [PubMed] [Google Scholar]
- 30.Afilalo J, Alexander KP, Mack MJ et al. Frailty assessment in the cardiovascular care of older adults. J Am Coll Cardiol. 2014;63:747–62. doi: 10.1016/j.jacc.2013.09.070;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Singer M, Glynne P. Treating critical illness: the importance of first doing no harm. PLoS Med. 2005;2:e167. doi: 10.1371/journal.pmed.0020167;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Cecconi M, De Backer D, Antonelli M et al. Consensus on circulatory shock and hemodynamic monitoring. Task force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40:1795–815. doi: 10.1007/s00134-014-3525-z;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Arrigo M, Mebazaa A. Understanding the differences among inotropes. Intensive Care Med. 2015;41:912–5. doi: 10.1007/s00134-015-3659-7;. [DOI] [PubMed] [Google Scholar]
- 34.Nieminen MS, Dickstein K, Fonseca C et al. The patient perspective: quality of life in advanced heart failure with frequent hospitalisations. Int J Cardiol. 2015;191:256–64. doi: 10.1016/j.ijcard.2015.04.235;. [DOI] [PubMed] [Google Scholar]
- 35.Verbrugge FH, Grieten L, Mullens W. New insights into combinational drug therapy to manage congestion in heart failure. Curr Heart Fail Rep. 2014;11:1–9. doi: 10.1007/s11897-013-0174-4;. [DOI] [PubMed] [Google Scholar]
- 36.Cotter G, Metzkor E, Kaluski E et al. Randomised trial of highdose isosorbide dinitrate plus low-dose furosemide versus high-dose furosemide plus low-dose isosorbide dinitrate in severe pulmonary oedema. Lancet. 1998;351:389–93. doi: 10.1016/S0140-6736(97)08417-1;. [DOI] [PubMed] [Google Scholar]
- 37.Mebazaa A, Parissis J, Porcher R et al. Short-term survival by treatment among patients hospitalized with acute heart failure: the global ALARM-HF registry using propensity scoring methods. Intensive Care Med. 2011;37:290–301. doi: 10.1007/s00134-010-2073-4;. [DOI] [PubMed] [Google Scholar]
- 38.Greene SJ, Fonarow GC, Vaduganathan M et al. The vulnerable phase after hospitalization for heart failure. Nat Rev Cardiol. 2015;12:220–9. doi: 10.1038/nrcardio.2015.14;. [DOI] [PubMed] [Google Scholar]
- 39.Demissei BG, Cotter G, Prescott MF et al. A multimarker multi-time point-based risk stratification strategy in acute heart failure: results from the RELAX-AHF trial. Eur J Heart Fail. 2017;19:1001–10. doi: 10.1002/ejhf.749;. [DOI] [PubMed] [Google Scholar]
- 40.Ambrosy AP, Pang PS, Khan S et al. EVEREST Trial Investigators. Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: findings from the EVEREST trial. Eur Heart J. 2013;34:835–43. doi: 10.1093/eurheartj/ehs444;. [DOI] [PubMed] [Google Scholar]
- 41.Logeart D, Thabut G, Jourdain P et al. Predischarge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol. 2004;43:635–41. doi: 10.1016/j.jacc.2003.09.044;. [DOI] [PubMed] [Google Scholar]
- 42.Arrigo M, Truong QA, Onat D et al. Soluble CD146 Is a novel marker of systemic congestion in heart failure patients: an experimental mechanistic and transcardiac clinical study. Clin Chem. 2017;63:386–93. doi: 10.1373/clinchem.2016.260471;. [DOI] [PubMed] [Google Scholar]
- 43.Kubena P, Arrigo M, Parenica J et al. GREAT Network. Plasma levels of soluble CD146 reflect the severity of pulmonary congestion better than brain natriuretic peptide in acute coronary syndrome. Ann Lab Med. 2016;36:300–5. doi: 10.3343/alm.2016.36.4.300;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Gayat E, Arrigo M, Littnerova S et al. GREAT Network. Heart failure oral therapies at discharge are associated with better outcome in acute heart failure: a propensity-score matched study. Eur J Heart Fail. 2017;18:613. doi: 10.1002/ejhf.932;. [DOI] [PubMed] [Google Scholar]
- 45.Prins KW, Neill JM, Tyler JO et al. Effects of beta-blocker withdrawal in acute decompensated heart failure: a systematic review and meta-analysis. JACC Heart Fail. 2015;3:647–53. doi: 10.1016/j.jchf.2015.03.008;. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Komajda M, Tavazzi L, Swedberg K et al. SHIFT Investigators. Chronic exposure to ivabradine reduces readmissions in the vulnerable phase after hospitalization for worsening systolic heart failure: a post-hoc analysis of SHIFT. Eur J Heart Fail. 2016;18:1182–9. doi: 10.1002/ejhf.582;. [DOI] [PubMed] [Google Scholar]
- 47.Hindricks G, Taborsky M, Glikson M et al. IN-TIME Study Group. Implant-based multiparameter telemonitoring of patients with heart failure (IN-TIME): a randomised controlled trial. Lancet. 2014;384:583–90. doi: 10.1016/S0140-6736(14)61176-4;. [DOI] [PubMed] [Google Scholar]
- 48.Abraham WT, Adamson PB, Bourge RC et al. CHAMPION Trial Study Group. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet. 2011;377:658–66. doi: 10.1016/S0140-6736(11)60101-3;. [DOI] [PubMed] [Google Scholar]
- 49.Adamson PB. Pathophysiology of the transition from chronic compensated and acute decompensated heart failure: new insights from continuous monitoring devices. Curr Heart Fail Rep. 2009;6:287–92. doi: 10.1007/s11897-009-0039-z;. [DOI] [PubMed] [Google Scholar]