

Abstract
AF and heart failure with reduced ejection fraction (HFrEF) frequently coexist. Catheter ablation is an increasingly utilised treatment strategy for patients with AF and can be safely performed and is effective in achieving sinus rhythm for patients with HFrEF. Successful ablation may result in improved LV function, clinical heart failure status, quality of life and possibly even mortality. This review summarises the literature analysing efficacy, safety and outcomes of AF ablation for patients with HFrEF.
Keywords: Atrial fibrillation, cardiomyopathy, catheter ablation, heart failure, outcomes
As the population ages, the incidence of both AF and heart failure (HF) will continue to increase. By the year 2030, there will be an estimated >12 million patients with AF and >8 million patients with HF.[1,2] A significant proportion of patients with HF have reduced (<50 %) left ventricular ejection fraction (heart failure with reduced ejection fraction, HFrEF) and the coexistance of AF in patients with AF and HFrEF has been associated with worse outcomes. Patients with HFrEF are predisposed to developing AF since neurohormonal changes and increased LV filling pressures can lead to LA dilation and fibrosis, facilitating AF progression. The development of AF in patients with severe HF is associated with a multitude of negative endpoints compared with patients without AF, including lower functional class, worse peak oxygen consumption, decreased cardiac output and worse mitral and tricuspid regurgitation.[3]
New-onset AF in patients with HF has also been associated with increased mortality and HF hospitalisations.[4] Determining whether AF is a major driver of HF versus simply a marker of worsening HF is important to identify which patients are likely to derive the most benefit from a rhythm control strategy. After adjusting for concomitant risk factors and comorbid conditions, the majority of randomised controlled trials have found that AF is not an independent predictor of mortality in patients with HF. The presence of AF in patients with HFrEF can potentially worsen HF symptoms in several ways. First, the loss of atrial kick during AF can result in decreased LV filling and, therefore, cardiac output. Second, the irregularity of the ventricular response during AF is associated with reduction in cardiac output, a phenomenon that appears to be independent of heart rate.[5] Prolonged periods of uncontrolled tachycardia with rapid AF have been well known to result in tachycardia-induced cardiomyopathy, and left ventricular ejection fraction (LVEF) may recover in some patients with adequate rate control.[6] Finally, atrial structural changes may occur in the setting of persistent AF, in some cases leading to mitral annular dilation and resultant “atrial functional mitral regurgitation”, which can be reversible with restoration of sinus rhythm.[7,8]
Medical Therapy for AF in Heart Failure with Reduced Ejection Fraction Patients
Guidelines recommmend the use of beta-blockers, angiotensinconverting enzyme inhibitors, angiotensin II recepter blockers, aldosterone antagonists and, more recently, angiotensin receptor–neprilysin inhibitors as medical therapy for patients with symptomatic HFrEF, and these medications are associated with improved mortality.[9] Patients with AF and HFrEF have a significantly higher risk of stroke or systemic embolism, as well as overall mortality compared with patients with both AF and HF with preserved ejection fraction (HFpEF) or without HF.[10] As such, the presence of HF merits one point with the CHADS2 and CHA2DS2-VASc risk scores and thus oral anticoagulation is usually recommended for stroke prophylaxis, as per guidelines.[11]
Beta-blockers
Beta-blockers have long been considered the cornerstone of HF therapy in patients with reduced LVEF. However, the beneficial effect of these medications in patients with HFrEF appears to be mitigated by the coexistance of AF.[12] Studies have suggested that the survival benefit with beta-blockers in HFrEF is limited only to those patients who are in sinus rhythm.[13,14] Large meta-analyses assessing thousands of patients from clinical trials comparing beta-blockers and placebo in patients with HFrEF and sinus rhythm with AF have shown that beta-blockers significantly reduce both all-cause mortality and cardiovascular hospitalisations in patients in sinus rhythm but not AF, despite similar degrees of ventricular rate reduction in both groups.[14,15]
Anti-arrhythmic Drugs
Due to potential for pro-arrhythmia, the choice of anti-arrhythmic drugs for AF is limited to amiodarone and dofetilide in patients with HFrEF, as per the 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society guidelines.[11] Dronedarone is contraindicated in patients with New York Heart Association (NYHA) class III–IV HF or severe LV dysfunction (LVEF <40 %) as its use has been associated with increased early mortality due to HF worsening.[16] Vaughan–Williams classification class Ic agents have negative inotropic effects and should thus be avoided in patients with HFrEF.[11] Sotalol should also be avoided in patients with HFrEF due to increased likelihood of torsades de pointes, particularly in patients with concomitant renal failure.11 Dofetilide was studied in the Danish Investigations of Arrhythmia and Mortality on Dofetilide in Congestive Heart Failure (DIAMOND-CHF) trial, which randomised 1,518 patients with HF and LV dysfunction to dofetilide versus placebo. The study showed that dofetilide was more effective in converting AF to sinus rhythm and maintaining sinus rhythm compared with placebo and dofetilide reduced the risk of HF hospitalisation (RR 0.75, 95 % CI [0.63–0.89]).[17] Although there was no overall difference in mortality compared with placebo among all patients, a post hoc analysis suggested significant reduction in mortality among patients with normal baseline QTc treated with dofetilide compared with patients randomised to placebo.[18] Amiodarone is the most effective anti-arrhythmic drug (AAD) to maintain sinus rhythm, but is also associated with several side effects with long-term use including multiple organ toxicities that may as a result actually increase likelihood of non-cardiac mortality, as was suggested by the Sudden Cardiac Death in Heart Failure Trial (SCDHeFT), which included patients with NYHA class III HF.[19,20] The Atrial Fibrillation and Congestive Heart Failure (AF-CHF) trial randomised 1,376 patients to rate control versus rhythm control (>80 % with amiodarone) and showed that rhythm control was associated with an increased rate of hospitalisation and no mortality benefit.[21]
Catheter Ablation for AF in Heart Failure with Reduced Ejection Fraction
Maintainence of sinus rhythm has been associated with improved mortality and decreased all-cause and heart failure hospitalisations in patients with AF and HFrEF.[22] However, the optimal strategy for rhythm control remains controversial. Since the efficacy of AADs remains suboptimal in patients with HFrEF, catheter ablation has become an increasingly utilised treatment strategy. The decision of whether to perform catheter ablation in patients with HFrEF should be individualised, weighing the potential long-term benefits of successful ablation against the risks of intra-procedural complications. Importantly, certain individual patient characteristics such as larger left atrial volume may predict AF recurrence after ablation.[23] There is a growing body of literature supporting AF ablation for patients with HFrEF, with a large number of retrospective observational studies and several randomised controlled trials in addition to many meta-analyses. Based on these data, the 2017 Heart Rhythm Society/European Heart Rhythm Association/European Cardiac Arrhythmia Society/Asia Pacific Heart Rhythm Society/Latin American Society of Cardiac Stimulation and Electrophysiology expert consensus statement on AF ablation recommends that it is reasonable to use similar indications for AF ablation in selected patients with HF as for patients without HF (class IIa, level of evidence B-R).[24] The optimal ablation strategy for patients with HFrEF remains controversial. Achievement of electrical pulmonary vein isolation (PVI) (Figure 1) should be performed for all AF ablations (class I, level of evidence A) and may be adequate especially in patients with paroxysmal AF. However, especially among patients with non-paroxysmal forms of AF, the benefit additional ablation with lesions sets such as empirical linear ablation, posterior wall isolation and targeting of non-pulmonary vein triggers, complex fractionated atrial electrograms or rotors remains unclear. Prior prospective studies (in non-HFrEF patients) have not shown benefit of additional empirical linear ablation or targeting of complex fractionated atrial electrograms on top of PVI alone in patients with non-paroxysmal AF.[25,26]
Figure 1: Ablation Lesion Set for Circumferential Pulmonary Vein Isolation.
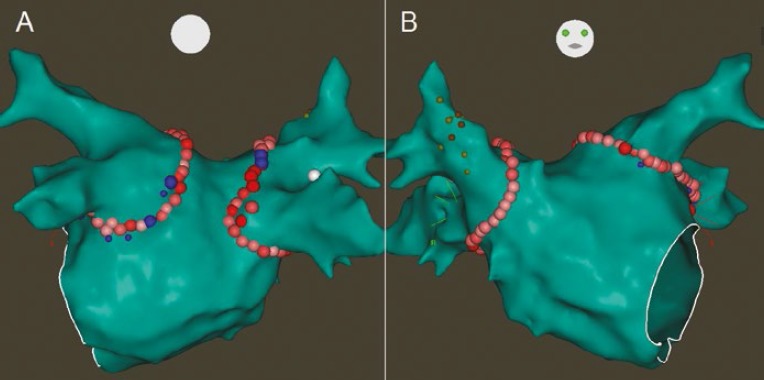
Posterior (A) and anterior (B) projections of the left atrium on the 3-dimensional electroanatomical map showing circular ablation lesions delivered around both sets of pulmonary veins (pink, red and blue circles). The smaller yellow and orange circles in (B) are sites where pacing resulted in diaphragmatic stimulation, delineating the course of the right phrenic nerve.
Observational Studies of AF Ablation in Heart Failure with Reduced Ejection Fraction
There have been numerous retrospective observational studies examining outcomes of catheter ablation for AF in patients with HFrEF.[27–47] Although most these studies are single-centre experiences with relatively small (<100 patients) sample sizes, ablation has been shown to be relatively safe in patients with HFrEF and successful ablation has in general been associated with improved LVEF, improved quality of life and functional capacity.[27] Table 1 summarises the findings of these observational studies.
Table 1: Summary of Observational Studies of AF Ablation in Patients with Heart Failure with Reduced Ejection Fraction (HFrEF).
| Study | Sample size (ablation group) | Comparison arm | Mean LVEF (%) | Follow-up (months) | Single procedure success (%) | Multiple procedure success (%) | Improvement in LVEF (%) | Other comments |
|---|---|---|---|---|---|---|---|---|
| Chen 2004[28] | 377 (94) | Normal LVEF controls | 36 | 14 | 52 | 73 | +5 | Improved QOL |
| Hsu 2004[29] | 116 (58) | Normal LVEF controls | 35 | 12 | 50 | 78 | +22 | Improved QOL, exercise capacity, LV dimensions |
| Tondo 2006[30] | 105 (40) | Normal LVEF controls | 33 | 14 | 55 | 87 | +13 | Improved QOL, exercise capacity |
| Gentlesk 2007[31] | 366 (67) | Normal LVEF controls | 42 | 20 | 55 | 86 | +14 | |
| Efremidis 2008[32] | 13 (13) | – | 36 | 9 | 62 | – | +16 | Improved LV dimensions |
| Nadamanee 2008[33] | 129 (129) | – | 31 | 27 | 58 | 79 | +10 | |
| Lutomsky 2008[34] | 70 (18) | Normal LVEF controls | 41 | 6 | 50 | – | +10 | |
| De Potter 2010[35] | 72 (36) | Normal LVEF controls | 41 | 16 | 50 | 64 | +8 | |
| Choi 2010[36] | 30 (15) | HF treated medically | 37 | 16 | 46 | 73 | +13 | |
| Cha 2011[37] | 368 (111) | Normal LVEF, diastolic dysfunction controls | 35 | 13 | – | 75 | +21 | |
| Anselmino 2013[38] | 196 (196) | – | 40 | 46 | 45 | 62 | +10 | Improved LV dimensions and mitral regurgitation |
| Calvo 2013[39] | 658 (97) | Normal LVEF controls | 40 | 6 | 70 | 83 | +12 | |
| Nedios 2014[40] | 138 (69) | Normal LVEF controls | 31 | 28 | 40 | 65 | +15 | |
| Kosiuk 2014[41] | 73 (73) | – | 37 | 40 | 37 | – | +4 | Reduction in ICD therapies |
| Lobo 2015[42] | 31 (31) | – | 45 | 20 | 51 | 77 | +14 | |
| Bunch 2015[43] | 2403 (267) | Matched HFrEF with AF but ablation; and HFrEF with no AF | 27 | 60 | 39 | – | +16 | Reduction in death and hospitalisation |
| Rillig 2015[44] | 80 (80) | – | 35 | 72 | 35 | 57 | +21 | |
| Kato 2016[45] | 18 (18) | – | 26 | 21 | 11 | 61 | +11 | |
| Yanagisawa 2016[46] | 54 (54) | – | 39 | 6 | 65 | 65 | +10 | Reduction in BNP |
| Ullah 2016[47] | 1273 (171) | Normal LVEF controls | 34 | 43 | 26 | 65 | +12 | Reduction in cardiac death |
BNP = B-type natriuretic peptide; ICD = implantable cardioverter defibrillator; LVEF = left ventricular ejection fraction; QOL = quality of life. Adapted and modified, with permission, from Verma et al.[25]
Prospective Randomised Controlled Trials of AF Ablation in Heart Failure with Reduced Ejection Fraction
Most randomised controlled trials have demonstrated overall benefit with ablation.[48–53] However, there has been one notable exception: a study by MacDonald et al. published in 2011 randomised 41 patients with persistent AF and HFrEF (LVEF <35 %, NYHA class II–IV) to AF ablation versus medical therapy and found no difference in LVEF improvement, N-terminal pro-brain natriuretic peptide level, 6-minute walk distance or quality of life.[54] Importantly, in this study, only 50 % of patients remained in sinus rhythm at 6 months and there was a 15 % complication rate in the ablation group.
Khan et al. randomised 81 patients with HFrEF (LVEF ≤40 % and NYHA class II–III) to AF ablation versus AV nodal ablation and biventricular pacing and showed that at 6 months, those randomised to AF ablation had improved questionnaire scores, longer 6-minute walk distance and higher LVEF.[48]
Jones et al. randomised 52 patients with LVEF ≤35 % and persistent AF to ablation versus rate control.[49] Overall, 88 % of patients in the ablation group were in sinus rhythm at the end of the study (68 % single procedure success). The primary endpoint of peak oxygen consumption was significantly higher in the ablation group. Furthermore, significant improvements in Minnesota score and B-type natriuretic peptide (BNP) level were seen in the ablation group as well as a non-significant trend towards benefit in 6-minute walk distance and LVEF.[49] In the Catheter Ablation versus Medical Treatment of Atrial Fibrillation in Heart Failure (CAMTAF) trial, Hunter et al. randomised 50 patients with persistent AF and LVEF <50 % to ablation versus rate control. At 6 months, those randomised to ablation had 81 % freedom from recurrent AF off AADs and improved LVEF, peak oxygen consumption and Minnesota score compared with the rate control arm.[50] in the Ablation versus Amiodarone for Treatment of Persistent Atrial Fibrillation in Patients with Congestive Heart Failure and an Implanted Device (AATAC) trial, Di Biase et al. randomised 203 patients with persistent AF, dual-chamber or biventricular implantable cardioverter defibrillator (ICD) and HFrEF (LVEF ≤40 % and NYHA class II–III) to ablation versus amiodarone.[51] The primary endpoint was AF recurrence and secondary endpoints were all-cause mortality and unplanned hospitalisations. Despite a wide range of single-procedure success rates between centres (29–61 %), those randomised to ablation were more likely to be in sinus rhythm after single and multiple procedures. Over 2 years of follow-up, the ablation group had lower rates of hospitalisation (31 versus 57 %, p<0.001) and mortality (8 versus 18 %, p=0.037) compared with those randomised to amiodarone.[51] In the Catheter Ablation versus Medical Rate Control in Atrial Fibrillation and Systolic Dysfunction (CAMERAMRI) trial, Prabhu et al. randomised 68 patients with persistent AF and LVEF ≤45 % to ablation versus rate control and found that the ablation group were more likely to have improved LVEF.[52] They also demonstrated that absence of late gadolineium enhancement on pre-procedural MRI predicted greater improvement in LVEF and normalisation of LVEF at 6 months. Catheter Ablation versus Standard Conventional Treatment in Patients with Left Ventricular Dysfunction and Atrial Fibrillation (CASTLE-AF) is the most recent randomised controlled trial, where patients with paroxysmal or persistent AF and HFrEF (<35 %) and ICD (with home monitoring capability) were randomised to either ablation or conventional medical therapy for AF.[55] The primary endpoint was a composite of all-cause mortality and unplanned hospitalisation for worsening HF. Over median follow-up of 37.8 months, those randomised to ablation were significantly less likely to experience the composite primary endpoint (28.5 % versus 44.6; HR 0.62, 95 % CI [0.43–0.87]; p=0.007) than controls. Those in the ablation group were also less likely to meet the secondary endpoints of all-cause mortality (13.4 % versus 25 %; HR 0.53, 95 % CI [0.32–0.86]; p=0.011) or HF hospitalisation (20.7 % versus 35.9 %; HR 0.56, 95 % CI [0.37–0.83]; p=0.004) than controls.
Table 2 summarises the major randomised controlled trials comparing catheter ablation with medical therapy.
Table 2: Summary of Randomised Controlled Trials of Patients with Heart Failure with Reduced Ejection Fraction (HFrEF) treated with AF Ablation.
| Study | Sample size (ablation group) | Comparison arm | Mean LVEF (%) | Follow-up (months) | Single procedure success (%) | Multiple procedure success (%) | Improvement in LVEF (%) | Other comments |
|---|---|---|---|---|---|---|---|---|
| Khan 2008[48] | 81 (41) | AVJ, CRT | 27 | 6 | 68 | 88 | +8 | Improved 6MWD and Minnesota score |
| MacDonald 2011[54] | 41 (22) | Rate control | 36 | 12 | 40 | 50 | +4 | High rate of complications (%) |
| Jones 2013[49] | 52 (26) | Rate control | 22 | 12 | 68 | 88 | +11 | Improved Minnesota score, BNP, peak oxygen consumption |
| Hunter 2014[50] | 366 (67) | Rate control | 42 | 20 | 38 | 81 | +8 | Improved Minnesota score, peak oxygen consumption Di |
| Biase 2016[51] | 203 (102) | Amiodarone | 29 | 24 | – | 70 | +8 | Improved Minnesota score. Lower mortality and hospitalisation rates |
| Prabhu 2017[52] | 66 (33) | Rate control | 32 | 6 | 56 | – | +18 | Absence of LGE predicted LVEF improvement in ablation group |
| CASTLE-AF 2017[53,55] | 363 (179) | Medical therapy (32% on AAD, mostly amiodarone) | 32 | 60 | – | – | +8 | Lower mortality and heart failure hospitalisation |
AVJ = AV junction ablation; BNP = B-type natriuretic peptide; CRT = cardiac resynchronization therapy; LGE = late gadolinium enhancement; LVEF = left ventricular ejection fraction; 6MWD = 6-minute walk distance. Adapted and modified, with permission, from Verma et al.[25]
Meta-analyses of AF Ablation in Heart Failure with Reduced Ejection Fraction
A number of meta-analyses have examined the benefit, efficacy and safety of catheter ablation for patients with HFrEF, all of which have suggested AF ablation to be safe, effective and beneficial in this patient population.[56–59] Anselmino et al. pooled data for 1,838 patients from 26 studies (randomised controlled trials, clinical trials and observational studies) and found that over mean follow-up of 23 months, there was a 4.2 % complication rate and 60 % of patients maintained sinus rhythm over long-term follow-up.[56] AF ablation resulted in significant improvement in LVEF (13 %) and reduction in BNP (620 pg/ml). Wilton et al. included eight studies of 1,851 patients in their meta-analysis comparing efficacy and safety of AF ablation in patients with reduced verses normal left ventricular systolic function.[57] Freedom from recurrent AF after a single procedure was achieved in 28–55 % of patients with HFrEF; although allowing for multiple procedures, this number increased to 64–96 % (mean 1.4 procedures). There was no difference in rates of complications between groups and there was an 11 % improvement in LVEF in patients in the HFrEF group after AF ablation.
Conclusion
Significant interplay exists between AF and HFrEF. Catheter ablation can be safely performed and is effective in maintaining sinus rhythm in patients with HFrEF, although multiple ablations may be necessary to achieve long-term freedom from AF. Successful ablation may result in improved LV function, clinical heart failure status and quality of life, as evidenced by lower BNP levels and improved peak oxygen consumption, Minnesota score and 6-minute walk distance. As such, AF ablation should be considered as an adjunctive treatment strategy for patients with HFrEF.
References
- 1.Colilla S, Crow A, Petkun W et al. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112:1142–7. doi: 10.1016/j.amjcard.2013.05.063. [DOI] [PubMed] [Google Scholar]
- 2.Heidenreich PA, Albert NM, Allen LA et al. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–19. doi: 10.1161/HHF.0b013e318291329a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Pozzoli M, Cioffi G, Traversi E et al. Predictors of primary atrial fibrillation and concomitant clinical and hemodynamic changes in patients with chronic heart failure: a prospective study in 344 patients with baseline sinus rhythm. J Am Coll Cardiol. 1998;32:197–204. doi: 10.1016/S0735-1097(98)00221-6. [DOI] [PubMed] [Google Scholar]
- 4.Chamberlain AM, Redfield MM, Alonso A et al. Atrial fibrillation and mortality in heart failure: a community study. Circ Heart Fail. 2011;4:740–6. doi: 10.1161/CIRCHEARTFAILURE.111.962688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Daoud EG, Weiss R, Bahu M et al. Effect of an irregular ventricular rhythm on cardiac output. Am J Cardiol. 1996;78:1433–6. doi: 10.1016/S0002-9149(97)89297-1. [DOI] [PubMed] [Google Scholar]
- 6.Martin CA, Lambiase PD. Pathophysiology, diagnosis and treatment of tachycardiomyopathy. Heart. 2017;103:1543–52. doi: 10.1136/heartjnl-2016-310391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liang JJ, Silvestry FE. Mechanistic insights into mitral regurgitation due to atrial fibrillation: “Atrial functional mitral regurgitation”. Trends Cardiovasc Med. 2016;26:681–9. doi: 10.1016/j.tcm.2016.04.012. [DOI] [PubMed] [Google Scholar]
- 8.Gertz ZM, Raina A, Saghy L et al. Evidence of atrial functional mitral regurgitation due to atrial fibrillation: reversal with arrhythmia control. J Am Coll Cardiol. 2011;58:1474–81. doi: 10.1016/j.jacc.2011.06.032. [DOI] [PubMed] [Google Scholar]
- 9.Yancy CW, Jessup M, Bozkurt B et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America. J Am Coll Cardiol. 2017;70:776–803. doi: 10.1016/j.jacc.2017.04.025. [DOI] [PubMed] [Google Scholar]
- 10.McMurray JJ, Ezekowitz JA, Lewis BS et al. Left ventricular systolic dysfunction, heart failure, and the risk of stroke and systemic embolism in patients with atrial fibrillation: insights from the ARISTOTLE trial. Circ Heart Fail. 2013;6:451–60. doi: 10.1161/CIRCHEARTFAILURE.112.000143. [DOI] [PubMed] [Google Scholar]
- 11.January CT, Wann LS, Alpert JS et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:2071–104. doi: 10.1161/CIR.0000000000000040. [DOI] [PubMed] [Google Scholar]
- 12.Rienstra M, Damman K, Mulder BA et al. Beta-blockers and outcome in heart failure and atrial fibrillation: a meta-analysis. JACC Heart Fail. 2013;1:21–8. doi: 10.1016/j.jchf.2012.09.002. [DOI] [PubMed] [Google Scholar]
- 13.Cullington D, Goode KM, Zhang J et al. Is heart rate important for patients with heart failure in atrial fibrillation? JACC Heart Fail. 2014;2:213–20. doi: 10.1016/j.jchf.2014.01.005. [DOI] [PubMed] [Google Scholar]
- 14.Kotecha D, Flather MD, Altman DG et al. Heart rate and rhythm and the benefit of beta-blockers in patients with heart failure. J Am Coll Cardiol. 2017;69:2885–96. doi: 10.1016/j.jacc.2017.04.001. [DOI] [PubMed] [Google Scholar]
- 15.Kotecha D, Holmes J, Krum H et al. Efficacy of beta blockers in patients with heart failure plus atrial fibrillation: an individual-patient data meta-analysis. Lancet. 2014;384:2235–43. doi: 10.1016/S0140-6736(14)61373-8.. [DOI] [PubMed] [Google Scholar]
- 16.Kober L, Torp-Pedersen C, McMurray JJ et al. Increased mortality after dronedarone therapy for severe heart failure. N Engl J Med. 2008;358:2678–87. doi: 10.1056/NEJMoa0800456. [DOI] [PubMed] [Google Scholar]
- 17.Torp-Pedersen C, Møller M, Bloch-Thomsen PE et al. Dofetilide in patients with congestive heart failure and left ventricular dysfunction. N Engl J Med. 1999;341:857–65. doi: 10.1056/NEJM199909163411201. [DOI] [PubMed] [Google Scholar]
- 18.Brendorp B, Elming H, Jun L et al. QTc interval as a guide to select those patients with congestive heart failure and reduced left ventricular systolic function who will benefit from antiarrhythmic treatment with dofetilide. Circulation. 2001;103:1422–7. doi: 10.1161/01.CIR.103.10.1422. [DOI] [PubMed] [Google Scholar]
- 19.Freemantle N, Lafuente-Lafuente C, Mitchell S et al. Mixed treatment comparison of dronedarone, amiodarone, sotalol, flecainide, and propafenone, for the management of atrial fibrillation. Europace. 2011;13:329–45. doi: 10.1093/europace/euq450. [DOI] [PubMed] [Google Scholar]
- 20.Packer DL, Prutkin JM, Hellkamp AS et al. Impact of implantable cardioverter-defibrillator, amiodarone, and placebo on the mode of death in stable patients with heart failure: analysis from the sudden cardiac death in heart failure trial. Circulation. 2009;120:2170–6. doi: 10.1161/CIRCULATIONAHA.109.853689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Roy D, Talajic M, Nattel S et al. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358:2667–77. doi: 10.1056/NEJMoa0708789. [DOI] [PubMed] [Google Scholar]
- 22.Pedersen OD, Bagger H, Keller N et al. Efficacy of dofetilide in the treatment of atrial fibrillation-flutter in patients with reduced left ventricular function: a Danish Investigations of Arrhythmia and Mortality ON Dofetilide (DIAMOND) substudy. Circulation. 2001;104:292–296. doi: 10.1161/01.CIR.104.3.292. [DOI] [PubMed] [Google Scholar]
- 23.Njoku A, Kannabhiran M, Arora R et al. Left atrial volume predicts atrial fibrillation recurrence after radiofrequency ablation: a meta-analysis. Europace. 2018;20:33–42. doi: 10.1093/europace/eux013. [DOI] [PubMed] [Google Scholar]
- 24.Calkins H, Hindricks G, Cappato R et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14:e275–e444. doi: 10.1016/j.hrthm.2017.05.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Verma A, Jiang CY, Betts TR et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015;372:1812–22. doi: 10.1056/NEJMoa1408288. [DOI] [PubMed] [Google Scholar]
- 26.Dixit S, Marchlinski FE, Lin D et al. Randomized ablation strategies for the treatment of persistent atrial fibrillation: RASTA study. Circ Arrhythm Electrophysiol. 2012;5:287–94. doi: 10.1161/CIRCEP.111.966226. [DOI] [PubMed] [Google Scholar]
- 27.Verma A, Kalman JM, Callans DJ. Treatment of patients with atrial fibrillation and heart failure with reduced ejection fraction. Circulation. 2017;135:1547–63. doi: 10.1161/CIRCULATIONAHA.116.026054. [DOI] [PubMed] [Google Scholar]
- 28.Chen MS, Marrouche NF, Khaykin Y et al. Pulmonary vein isolation for the treatment of atrial fibrillation in patients with impaired systolic function. J Am Coll Cardiol. 2004;43:1004–9. doi: 10.1016/j.jacc.2003.09.056. [DOI] [PubMed] [Google Scholar]
- 29.Hsu LF, Jais P, Sanders P et al. Catheter ablation for atrial fibrillation in congestive heart failure. N Engl J Med. 2004;351:2373–83. doi: 10.1056/NEJMoa041018. [DOI] [PubMed] [Google Scholar]
- 30.Tondo C, Mantica M, Russo G et al. Pulmonary vein vestibule ablation for the control of atrial fibrillation in patients with impaired left ventricular function. Pacing Clin Electrophysiol. 2006;29:962–70. doi: 10.1111/j.1540-8159.2006.00471.x. [DOI] [PubMed] [Google Scholar]
- 31.Gentlesk PJ, Sauer WH, Gerstenfeld EP et al. Reversal of left ventricular dysfunction following ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 2007;18:9–14. doi: 10.1111/j.1540-8167.2006.00653.x. [DOI] [PubMed] [Google Scholar]
- 32.Efremidis M, Sideris A, Xydonas S et al. Ablation of atrial fibrillation in patients with heart failure: reversal of atrial and ventricular remodelling. Hellenic J Cardiol. 2008;49:19–25. [PubMed] [Google Scholar]
- 33.Nademanee K, Schwab MC, Kosar EM et al. Clinical outcomes of catheter substrate ablation for high-risk patients with atrial fibrillation. J Am Coll Cardiol. 2008;51:843–9. doi: 10.1016/j.jacc.2007.10.044. [DOI] [PubMed] [Google Scholar]
- 34.Lutomsky BA, Rostock T, Koops A et al. Catheter ablation of paroxysmal atrial fibrillation improves cardiac function: a prospective study on the impact of atrial fibrillation ablation on left ventricular function assessed by magnetic resonance imaging. Europace. 2008;10:593–9. doi: 10.1093/europace/eun076. [DOI] [PubMed] [Google Scholar]
- 35.De Potter T, Berruezo A, Mont L et al. Left ventricular systolic dysfunction by itself does not influence outcome of atrial fibrillation ablation. Europace. 2010;12:24–9. doi: 10.1093/europace/eup309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Choi AD, Hematpour K, Kukin M et al. Ablation vs medical therapy in the setting of symptomatic atrial fibrillation and left ventricular dysfunction. Congest Heart Fail. 2010;16:10–4. doi: 10.1111/j.1751-7133.2009.00116.x. [DOI] [PubMed] [Google Scholar]
- 37.Cha YM, Wokhlu A, Asirvatham SJ et al. Success of ablation for atrial fibrillation in isolated left ventricular diastolic dysfunction: a comparison to systolic dysfunction and normal ventricular function. Circ Arrhythm Electrophysiol. 2011;4:724–32. doi: 10.1161/CIRCEP.110.960690. [DOI] [PubMed] [Google Scholar]
- 38.Anselmino M, Grossi S, Scaglione M et al. Long-term results of transcatheter atrial fibrillation ablation in patients with impaired left ventricular systolic function. J Cardiovasc Electrophysiol. 2013;24:24–32. doi: 10.1111/j.1540-8167.2012.02419.x. [DOI] [PubMed] [Google Scholar]
- 39.Calvo N, Bisbal F, Guiu E et al. Impact of atrial fibrillationinduced tachycardiomyopathy in patients undergoing pulmonary vein isolation. Int J Cardiol. 2013;168:4093–7. doi: 10.1016/j.ijcard.2013.07.017. [DOI] [PubMed] [Google Scholar]
- 40.Nedios S, Sommer P, Dagres N et al. Long-term follow-up after atrial fibrillation ablation in patients with impaired left ventricular systolic function: the importance of rhythm and rate control. Heart Rhythm. 2014;11:344–51. doi: 10.1016/j.hrthm.2013.12.031. [DOI] [PubMed] [Google Scholar]
- 41.Kosiuk J, Nedios S, Darma A et al. Impact of single atrial fibrillation catheter ablation on implantable cardioverter defibrillator therapies in patients with ischaemic and nonischaemic cardiomyopathies. Europace. 2014;16:1322–6. doi: 10.1093/europace/euu018. [DOI] [PubMed] [Google Scholar]
- 42.Lobo TJ, Pachon CT, Pachon JC et al. Atrial fibrillation ablation in systolic dysfunction: clinical and echocardiographic outcomes. Arq Bras Cardiol. 2015;104:45–52. doi: 10.5935/abc.20140167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Bunch TJ, May HT, Bair TL et al. Five-year outcomes of catheter ablation in patients with atrial fibrillation and left ventricular systolic dysfunction. J Cardiovasc Electrophysiol. 2015;26:363–70. doi: 10.1111/jce.12602. [DOI] [PubMed] [Google Scholar]
- 44.Rillig A, Makimoto H, Wegner J Six-year clinical outcomes after catheter ablation of atrial fibrillation in patients with impaired left ventricular function. J Cardiovasc Electrophysiol. 2015. [DOI] [PubMed]
- 45.Kato K, Ejima K, Fukushima N et al. Catheter ablation of atrial fibrillation in patients with severely impaired left ventricular systolic function. Heart Vessels. 2016;31:584–92. doi: 10.1007/s00380-015-0635-7. [DOI] [PubMed] [Google Scholar]
- 46.Yanagisawa S, Inden Y, Kato H et al. Decrease in B-type natriuretic peptide levels and successful catheter ablation for atrial fibrillation in patients with heart failure. Pacing Clin Electrophysiol. 2016;39:225–34. doi: 10.1111/pace.12788. [DOI] [PubMed] [Google Scholar]
- 47.Ullah W, Ling LH, Prabhu S et al. Catheter ablation of atrial fibrillation in patients with heart failure: impact of maintaining sinus rhythm on heart failure status and long-term rates of stroke and death. Europace. 2016;18:679–86. doi: 10.1093/europace/euv440. [DOI] [PubMed] [Google Scholar]
- 48.Khan MN, Jais P, Cummings J et al. Pulmonary-vein isolation for atrial fibrillation in patients with heart failure. N Engl J Med. 2008;359:1778–85. doi: 10.1056/NEJMoa0708234. [DOI] [PubMed] [Google Scholar]
- 49.Jones DG, Haldar SK, Hussain W et al. A randomized trial to assess catheter ablation versus rate control in the management of persistent atrial fibrillation in heart failure. J Am Coll Cardiol. 2013;61:1894–903. doi: 10.1016/j.jacc.2013.01.069. [DOI] [PubMed] [Google Scholar]
- 50.Hunter RJ, Berriman TJ, Diab I et al. A randomized controlled trial of catheter ablation versus medical treatment of atrial fibrillation in heart failure (the CAMTAF trial). Circ Arrhythm Electrophysiol. 2014;7:31–8. doi: 10.1161/CIRCEP.113.000806. [DOI] [PubMed] [Google Scholar]
- 51.Di Biase L, Mohanty P, Mohanty S et al. Ablation versus amiodarone for treatment of persistent atrial fibrillation in patients with congestive heart failure and an implanted device: results from the AATAC Multicenter Randomized Trial. Circulation. 2016;133:1637–44. doi: 10.1161/CIRCULATIONAHA.115.019406. [DOI] [PubMed] [Google Scholar]
- 52.Prabhu S, Taylor AJ, Costello BT et al. Catheter ablation versus medical rate control in atrial fibrillation and systolic dysfunction: the CAMERA-MRI Study. J Am Coll Cardiol. 2017;70:1949–61. doi: 10.1016/j.jacc.2017.08.041. [DOI] [PubMed] [Google Scholar]
- 53.Catheter Ablation vs. Standard Conventional Treatment in Patients With LV Dysfunction and AF (CASTLE-AF). https://clinicaltrialsgov/show/NCT00643188 (Accessed 13 January 2018.
- 54.MacDonald MR, Connelly DT, Hawkins NM et al. Radiofrequency ablation for persistent atrial fibrillation in patients with advanced heart failure and severe left ventricular systolic dysfunction: a randomised controlled trial. Heart. 2011;97:740–7. doi: 10.1136/hrt.2010.207340. [DOI] [PubMed] [Google Scholar]
- 55.Marrouche NF, Brachmann J, Andresen D et al. Catheter ablation for atrial fibrillation with heart failure. N Engl J Med. 2018;378:417–27. doi: 10.1056/NEJMoa1707855. [DOI] [PubMed] [Google Scholar]
- 56.Anselmino M, Matta M, D’Ascenzo F et al. Catheter ablation of atrial fibrillation in patients with left ventricular systolic dysfunction: a systematic review and meta-analysis. Circ Arrhythm Electrophysiol. 2014;7:1011–8. doi: 10.1161/CIRCEP.114.001938. [DOI] [PubMed] [Google Scholar]
- 57.Wilton SB, Fundytus A, Ghali WA et al. Meta-analysis of the effectiveness and safety of catheter ablation of atrial fibrillation in patients with versus without left ventricular systolic dysfunction. Am J Cardiol. 2010;106:1284–91. doi: 10.1016/j.amjcard.2010.06.053. [DOI] [PubMed] [Google Scholar]
- 58.Dagres N, Varounis C, Gaspar T et al. Catheter ablation for atrial fibrillation in patients with left ventricular systolic dysfunction. A systematic review and meta-analysis. J Card Fail. 2011;17:964–70. doi: 10.1016/j.cardfail.2011.07.009. [DOI] [PubMed] [Google Scholar]
- 59.Ganesan AN, Nandal S, Luker J et al. Catheter ablation of atrial fibrillation in patients with concomitant left ventricular impairment: a systematic review of efficacy and effect on ejection fraction. Heart Lung Circ. 2015;24:270–80. doi: 10.1016/j.hlc.2014.09.012. [DOI] [PubMed] [Google Scholar]