

Abstract
Background:
Minimally invasive dentistry (MID) encompasses early caries diagnosis through caries risk assessment (CRA), early detection of incipient carious lesion including primary and secondary prevention based on scientific evidence that remineralization of demineralized enamel and dentin is possible if detected early. Although the dental curriculum focuses on the advantages of MID in tooth preservation, this science is not usually translated into practice.
Aim:
This study aimed to evaluate the knowledge, attitude, and skills of dental practitioners of Puducherry regarding the concepts of MID.
Subjects and Methods:
Data were collected through an online survey questionnaire based on awareness and practice of MID. Statistical evaluation was done on SPSS by Chi-square test.
Results:
A total of 126 dentists responded of which only 55% were trained in MID during their undergraduate and internship period, mainly through lectures (49.6%). Nearly 81% agreed that CRA should be conducted for all patients. Almost 42.7% had heard about International Caries Detection and Assessment System, but only 25.9% used a blunt explorer for caries detection. About 13.7% use magnification (loupes/microscope), but majority (84.7%) use radiographs. More than 70% were unaware of newer methods of caries detection. Statistically significant differences were found (P < 0.05) regarding qualification and experience about the effectiveness of Atraumatic Restorative Treatment and sandwich technique for treatment of caries in permanent teeth and high caries-risk children.
Conclusion:
Although there is knowledge about advantages of MID among dentists of Puducherry, it does not benefit patients, as many practitioners still follow the traditional principles of total caries removal.
Keywords: Caries risk assessment, clinical practice, minimally invasive dentistry, questionnaire, survey, undergraduate teaching
INTRODUCTION
A surgical approach to caries control as the first line of defense does not eliminate the cause of disease but leads to a continuing process of replacement dentistry, wherein the cavity gets larger and the tooth gets weaker.[1] This recognition led to the emergence of minimally invasive dentistry (MID);[2] which is based on the scientific fact that demineralized hydroxyapatite tends to remineralize when provided with a conducive local environment. When demineralizing factors overwhelm the remineralizing factors, carious lesions occur.[3] Furthermore, no restorative material is as good as the enamel-dentin duo; therefore, preserving and conserving the tooth structure is important.
Dawson and Makinson elaborated on this innovative approach for caries “Minimal Treatment” given by Mount and coined the term “Minimal Intervention Dentistry.”[4,5,6]
This medical model of management of carious lesions, MID, includes the following principles:[7,8,9,10]
Identification, where dental caries disease is diagnosed by risk assessment and carious lesions are detected at the earliest stage of demineralization[11]
Primary prevention to prevent the formation of new carious lesions and secondary prevention through remineralization therapy[7]
Control through conservative caries removal in an established lesion, using adhesive restorative materials for small but smart restorations and repair of the restorations rather than replacement.[3,12]
Although this paradigm shift in cariology and restorative dentistry has manifold advantages and is also inbuilt in the curriculum, doubts linger if they are being practiced effectively. Therefore, this study aimed to evaluate the level of knowledge, attitude, and skills toward MID for the management of dental caries among the dental practitioners in Puducherry.
SUBJECTS AND METHODS
Study design
This was an observational, qualitative, questionnaire-based online survey approved by the Institutional Review Board (Ref: IGIDSIRB2016NRP32PGJRCDE) and Institutional Ethical Committee (Ref: IGIDSIEC2016NRP32PGJRCDE). The survey period was from January to March 2017.
Sample size
Calculation was done using Survey Sample Size Calculator (95% confidence interval). Sample size calculated was 160 from among the 200 dental practitioners (including specialists) practicing in Puducherry with estimated 20% dropout.
Participants
A database of dental practitioners in Puducherry was collected from Indian Dental Association, and both undergraduates and postgraduates (inclusive of all specialties and irrespective of their experience) were included. Participants entered the study voluntarily. Study objectives and rationale were given in participant information letter attached to each questionnaire.
Questionnaire
The needs and demands of a specific community can markedly vary between countries, owing to different sociocultural conditions. Although all dentists receive similar training in accordance with dental education programs, their attitudes toward the clinical decision-making process and methods used for diagnosis and treatment of dental caries can exhibit considerable differences. Hence, a shortened version of a previously used questionnaire from the College of Dentistry, University of Iowa, was modified according to the needs of the study, based on the present clinical practices of the dentist population of Puducherry.[13] It was validated through pilot testing on 15 dentists. The questionnaire was then administered using Google Forms; the link for the same was sent to all the practitioners through E-mail. Questions were based on caries diagnosis, caries detection, remineralization therapy, and MID therapy. It focused on the knowledge, attitude, and skills of the practitioners on etiology, prevention, and application of MID principles for caries control, diverse methods used for caries detection, caries risk assessment (CRA), dietary counseling, fluoride exposure, pit and fissure sealants, and ultra-conservative restorative procedures. The questionnaire comprised two sections. The first section assessed the demography of the respondents – gender, age, type of practice, and years of experience in the profession. The second section assessed their knowledge and approach related to MID. Several questions used Likert-type scale response categories to assess the respondents' levels of agreement regarding diagnostic, preventive, and restorative techniques.
Statistical analysis
Data from the Google Forms were analyzed using Statistical Package for the Social Sciences (SPSS), version 17.0 software (IBM SPSS, IBM Corporation 1, Armonk, New York, United States). The sample was set at 95% confidence interval. P ≤ 0.05 was considered statistically significant. Results were expressed as number and percentage of respondents for each question.
RESULTS
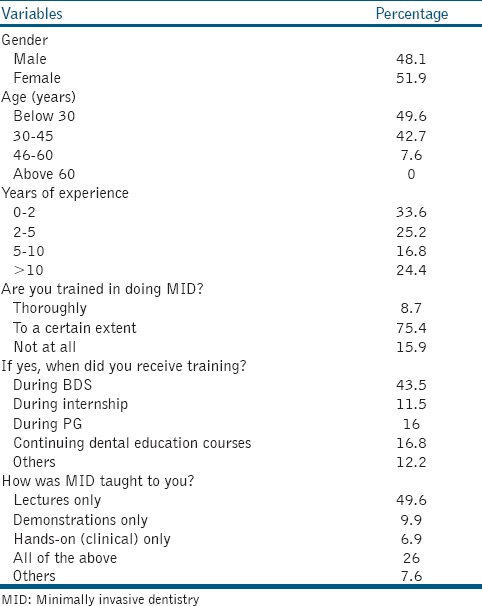
Totally 126 dentists (response rate: 78.8%) from Puducherry responded to the survey among whom 41.2% had been practicing for >5 years with 7.6% aged >45 years. Nearly 39.7% of the practitioners put in 4–8 h of practice per day with 74.8% of them attending >20 patients/day [Table 1].
Table 1.
Sociodemographic and minimally invasive dentistry training characteristics of the sample population
Based on qualification, 97.1% of MDS considered atraumatic restorative treatment (ART) as an effective technique for treatment of caries in permanent teeth compared to 82.4% of the BDS graduates (P < 0.025). Similarly, 68.1% of MDS agreed that ART can be used with high caries-risk children and rampant caries patients compared to 50.8% of BDS (P < 0.006) [Table 2].
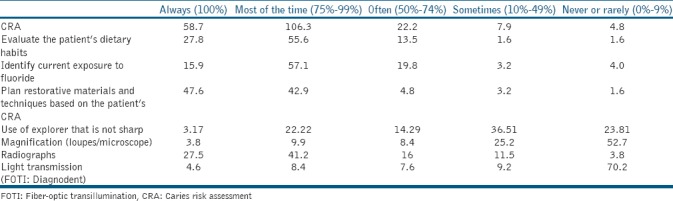
Table 2.
Level of knowledge toward minimally invasive dentistry principles assessed on a 5-point Likert scale (values given in percentage)

Based on experience, 95.9% of practitioners with >5 years' experience compared to 87% with <5 years of experience consider ART as an effective technique for treatment of caries in permanent teeth (P < 0.03). Similarly, 79.5% of practitioners with >5 years' experience compared to 48% with <5 years of experience agreed that ART can be used with high caries-risk children and rampant caries patients (P < 0.003).
Almost 94.6% of the respondents considered sandwich technique as an effective method for treatment of caries in permanent teeth, but only 69.5% agreed for it to be used for both children and adults (P < 0.0001). There was no significant difference in the opinion of an MDS or BDS graduate regarding the effectiveness of sandwich technique for treatment of caries in permanent teeth. Based on experience, 81.6% of practitioners with >5 years' experience compared to 63.6% with <5 years' experience agreed that it is an appropriate technique to be used for both children and adults (P < 0.009).
Nearly 91.3% of respondents considered pit and fissure sealant to be effective for the treatment of caries in permanent teeth, but only 76.4% used it as a routine procedure for high caries-risk children (P < 0.01).
About 72.5% agreed on the effectiveness of tunnel preparation in a proximal lesion instead of a proximal box and 69% on fissurotomy.
More than 90.1% agreed that fluoride is an essential agent in the tooth remineralization process. Fluoride toothpaste (77.9%), in-office fluoride varnish (67.9%), fluoride mouthrinse (66.4%), CPP-ACP (Casein Phosphopeptide and Amorphous Calcium Phosphate) paste (64.1%), and Xylitol chewing gum (45%) were considered effective in the treatment of caries in permanent teeth (P < 0.0001).
Practitioners' awareness about remineralization therapy and various concepts of MID therapy were not significantly related to whether they had undergone MID training.
DISCUSSION
In the present study, age and gender did not seem to affect the knowledge possessed about MID. However, experience within the practice seemed to increase awareness about MID. In a study conducted in Karnataka, 97% of dentists were aware of MID.[14] Similarly, in our study, we observed that 84.7% of the respondents knew MID, showing that there is a paradigm shift toward caries management based on MID. Only 55% of them were educated about MID in their BDS curriculum. Among them, 61.1% had either completed their BDS recently with an experience of <2–5 years or had gained knowledge through advanced continuing dental education programs. Recently completed graduates seem to have understood the efficacy of MID less than experienced practitioners. Although it is evident here that MID is being taught at the undergraduate level, evidence-based, up-to-date teaching programs are needed to best prepare the students for their dental careers.
Nearly 81% of dentists agreed that CRA should be conducted for all patients. CRA forms the cornerstone for successful application of MID in the management of dental caries.[15] Patients with evidence of active dental caries at baseline require a CRA to identify those risk factors that will contribute to the progression of caries. These factors should then be eliminated or moderated to ensure that the disease progression is stabilized before conservative and rehabilitative dental procedures are undertaken [Table 3].
Table 3.
Attitude toward application of minimally invasive dentistry principles and procedures in clinical practice (values given in percentage)
A clear majority (90%) understand that there is a direct relationship between caries and high carbohydrate diet and recommended diet counseling. Federation Dentaire International states that dental caries being an infectious disease the primary focus should be on infection control, plaque control, and reduced carbohydrate intake.[3,16]
Use of a sharp explorer was not related to training in MID. Even though 42.7% were aware of International Caries Detection and Assessment System, only 25.9% used a blunt explorer for caries detection.[17] This suggests that some aspects of the MID approach have not been completely adopted among the dentists. Use of sharp explorers should be discouraged as it removes the possibility of remineralization of the incipient lesions.[18]
Majority among the sample (84.7%) used radiography (Bite Wing Radiograph) for caries detection irrespective of whether they were trained in MID or not.[19] Respondents with MID training are expected to use magnification equipments such as loupes/microscope for caries detection, but the present study shows that only 13.7% do so. Using magnification equipment for detection of incipient lesions should be implemented in the undergraduate training as microscope-assisted precision dentistry is a necessity in MID.[20]
Fluorescence tools having higher magnification guide the dentist toward a more preventive and minimally invasive treatment strategy. Most fluorescent caries detection tools can discriminate between healthy and carious dental tissue, demonstrating various levels of sensitivity and specificity.[21] However, >70% had no knowledge about the newer methods of caries detection such as quantitative laser or light fluorescence, electrical conductive measurement, and fiber-optic transillumination which are less invasive and have good diagnostic value. This can be due to lack of professional reading or adoption of MID or availability or excessive cost.[14]
A statistically significant association was observed between BDS and MDS graduates regarding the effectiveness of ART and sandwich technique.[3,22,23] Compared to the BDS graduates (50.8%), majority of the postgraduates (68.1%) agreed that these methods can be used in high caries-risk children and rampant caries patients. Similarly, 79.5% of the practitioners with >5 years' experience agreed for the same compared to only 48% having <5 years' experience. However, there is widespread use of ART and sandwich technique in permanent teeth than primary teeth. This may be attributed to the widespread use of glass ionomer cement and not MID.
Although 91.3% agreed that pit and fissure sealant is effective in permanent teeth, only 76.4% agreed to its effectiveness in primary teeth. This reveals an inadequate knowledge and attitude toward MID in primary teeth.[22] Sealants occupy a prominent place in MID and are indicated not only for cases of noncavitated occlusal caries lesions, but also for sealing open margins of old restorations [Figure 1].[7]
Figure 1.
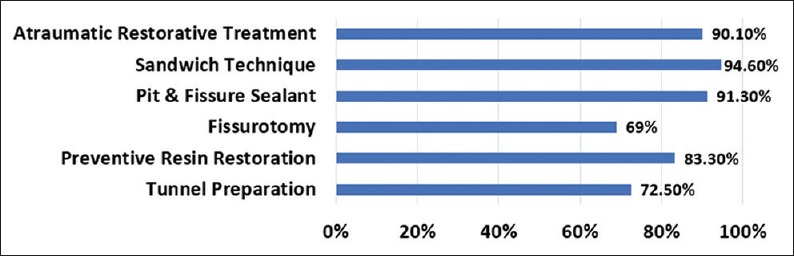
Percentage of respondents' awareness about various minimally invasive dentistry techniques for treatment of caries in permanent teeth
Although >90% were aware that fluoride is an essential agent in tooth remineralization process, only 67%–77% recommend fluoride varnish and fluoridated toothpaste in their practice. Even for the nonfluoride agents such as CPP-ACP paste and Xylitol chewing gum, only 45%–64% agreed to their effectiveness in permanent teeth. There seems to be an adequate agreement on fluorides than nonfluorides. Many studies have confirmed the effectiveness of fluoride in preventing caries, but fluoride also plays a role in remineralization of noncavitated caries.[7] Importance and appropriate prescription of nonfluoride agents must be emphasized during BDS training [Figure 2].
Figure 2.
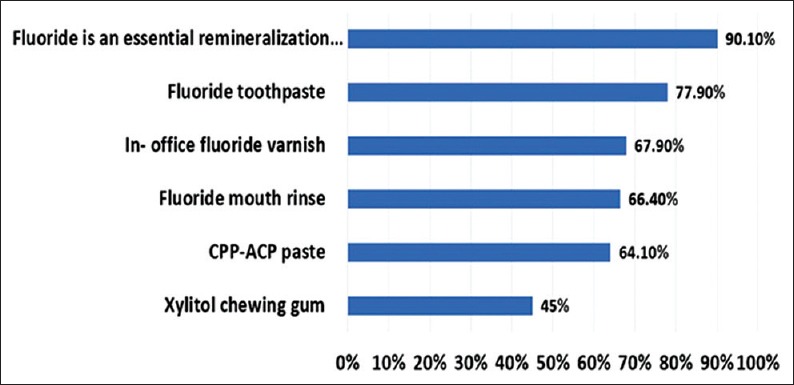
Percentage of respondents' awareness of the effectiveness of fluoride remineralization and its prescription in their daily practice regularly
One of the major limitations of the study is that it involves only dentists of Puducherry which is rather a small sample to formulate an idea about the practice of MID principles. More studies should be done on a nation-wide basis to understand better about the knowledge and attitude of dentists toward MID.
CONCLUSION
This study reveals that knowledge and awareness in MID are adequate, but effective practice is less. Education and practice should move toward a medical model of caries management with due respect to early detection, prevention, and prescription dentistry. There is an urgent need to focus on behavioral, educational, and societal changes of all dental specialties in oral health care to advance clinical evidence into practice starting from undergraduate teaching.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
The authors wish to thank Dr Senthil. M, Professor & Head, Dept. of Public Health Dentistry, Indira Gandhi Institute of Dental Sciences, Pondicherry and Dr Senthil Kumar Subramanian, Assistant Professor, Department of Physiology, Pondicherry Institute of Medical Science, Pondicherry, India for their help with statistics.
REFERENCES
- 1.Mount GJ. Minimal intervention dentistry: Cavity classification preparation. J Minimal Interv Dent. 2009;2:150–62. [Google Scholar]
- 2.Featherstone JD, Doméjean S. Minimal intervention dentistry: Part 1. From 'compulsive' restorative dentistry to rational therapeutic strategies. Br Dent J. 2012;213:441–5. doi: 10.1038/sj.bdj.2012.1007. [DOI] [PubMed] [Google Scholar]
- 3.Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry – A review. FDI commission project 1-97. Int Dent J. 2000;50:1–2. doi: 10.1111/j.1875-595x.2000.tb00540.x. [DOI] [PubMed] [Google Scholar]
- 4.Mount GJ. Minimal treatment of the carious lesion. Int Dent J. 1991;41:55–9. [PubMed] [Google Scholar]
- 5.Dawson AS, Makinson OF. Dental treatment and dental health. Part 1. A review of studies in support of a philosophy of minimum intervention dentistry. Aust Dent J. 1992;37:126–32. doi: 10.1111/j.1834-7819.1992.tb03050.x. [DOI] [PubMed] [Google Scholar]
- 6.Dawson AS, Makinson OF. Dental treatment and dental health. Part 2. An alternative philosophy and some new treatment modalities in operative dentistry. Aust Dent J. 1992;37:205–10. doi: 10.1111/j.1834-7819.1992.tb00744.x. [DOI] [PubMed] [Google Scholar]
- 7.Holmgren C, Gaucher C, Decerle N, Doméjean S. Minimal intervention dentistry II: Part 3. Management of non-cavitated (initial) occlusal caries lesions – Non-invasive approaches through remineralisation and therapeutic sealants. Br Dent J. 2014;216:237–43. doi: 10.1038/sj.bdj.2014.147. [DOI] [PubMed] [Google Scholar]
- 8.Fédération Dentaire Internationale (FDI) General Assembly: September 2016, Poznan, Poland; Policy Statement (revision) Minimal Intervention Dentistry (MID) 2016. pp. 4–5.
- 9.Walsh LJ, Brostek AM. Minimum intervention dentistry principles and objectives. Aust Dent J. 2013;58(Suppl 1):3–16. doi: 10.1111/adj.12045. [DOI] [PubMed] [Google Scholar]
- 10.Frencken JE, Peters MC, Manton DJ, Leal SC, Gordan VV, Eden E, et al. Minimal intervention dentistry for managing dental caries – A review: Report of a FDI task group. Int Dent J. 2012;62:223–43. doi: 10.1111/idj.12007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Guerrieri A, Gaucher C, Bonte E, Lasfargues JJ. Minimal intervention dentistry: Part 4. Detection and diagnosis of initial caries lesions. Br Dent J. 2012;213:551–7. doi: 10.1038/sj.bdj.2012.1087. [DOI] [PubMed] [Google Scholar]
- 12.Ngo H, Opsahl-Vital S. Minimal intervention dentistry II: Part 7. Minimal intervention in cariology: The role of glass-ionomer cements in the preservation of tooth structures against caries. Br Dent J. 2014;216:561–5. doi: 10.1038/sj.bdj.2014.398. [DOI] [PubMed] [Google Scholar]
- 13.Oliveira DC. Master's Thesis. University of Iowa; 2011. Minimally Invasive Dentistry Approach in Dental Public Health. [Google Scholar]
- 14.Sushanth V, Bhate P, Imranulla M, Kalra D, Kumar N, Prashant G. Assessment of knowledge, attitude, and practice regarding preventive options in oral care among dentists in Davangere city, Karnataka: A cross-sectional study. Dent Med Res. 2015;3:20–5. [Google Scholar]
- 15.Hallett KB. The application of caries risk assessment in minimum intervention dentistry. Aust Dent J. 2013;58(Suppl 1):26–34. doi: 10.1111/adj.12047. [DOI] [PubMed] [Google Scholar]
- 16.Fontana M, Gonzalez-Cabezas C. Minimal intervention dentistry: Part 2. Caries risk assessment in adults. Br Dent J. 2012;213:447–51. doi: 10.1038/sj.bdj.2012.1008. [DOI] [PubMed] [Google Scholar]
- 17.Banerjee A. Minimal intervention dentistry: Part 7. Minimally invasive operative caries management: Rationale and techniques. Br Dent J. 2013;214:107–11. doi: 10.1038/sj.bdj.2013.106. [DOI] [PubMed] [Google Scholar]
- 18.Goswami M, Sachdeva P, Paul S, Walia V, Chawla S. Knowledge, attitude and practice regarding caries risk assessment and management in Delhi - National Capital Region: A cross-sectional survey. J Indian Assoc Public Health Dent. 2016;14:188–96. [Google Scholar]
- 19.Vural UK, Gökalp S. Diagnostic methods for dental caries used by private dental practitioners in Ankara. Niger J Clin Pract. 2017;20:382–7. doi: 10.4103/1119-3077.181360. [DOI] [PubMed] [Google Scholar]
- 20.Friedman MJ, Landesman HM. Microscope-assisted precision (MAP) dentistry. A challenge for new knowledge. J Calif Dent Assoc. 1998;26:900–5. [PubMed] [Google Scholar]
- 21.Tassery H, Levallois B, Terrer E, Manton DJ, Otsuki M, Koubi S, et al. Use of new minimum intervention dentistry technologies in caries management. Aust Dent J. 2013;58(Suppl 1):40–59. doi: 10.1111/adj.12049. [DOI] [PubMed] [Google Scholar]
- 22.Shah AH, Sheddi FM, Alharqan MS, Khawja SG, Vohra F, Akram Z, et al. Knowledge and attitude among general dental practitioners towards minimally invasive dentistry in Riyadh and Alkharj. J Clin Diagn Res. 2016;10:ZC90–4. doi: 10.7860/JCDR/2016/20543.8207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Holmgren CJ, Roux D, Doméjean S. Minimal intervention dentistry: Part 5. Atraumatic restorative treatment (ART) – A minimum intervention and minimally invasive approach for the management of dental caries. Br Dent J. 2013;214:11–8. doi: 10.1038/sj.bdj.2012.1175. [DOI] [PubMed] [Google Scholar]