

To the Editor
We report on a rare case of trisomy 17 identified by amniocentesis at 16 weeks of gestation in a fetus from a 23-year-old white woman (gravida 3 para 1 ab 1) with a history of an elevated maternal serum alpha fetoprotein level reported on two occasions. Amniocentesis was performed subsequently. The amniocentesis results showed a 47,XX,+17 karyotype (in 26 cells from 26 colonies from three primary cultures). Several ultrasound studies, including level 3 ultrasonography, were performed, but no fetal abnormalities or growth retardation was noted. The amount of amniotic fluid was normal. Several options were discussed with the parents, including fetal blood sampling and a repeat amniocentesis. The family elected to have a repeat amniocentesis, which was performed at approximately 19 weeks of gestation. The second amniocentesis showed a 46,XX karyotype in six cells from six colonies, and a 47,XX,+17 karyotype in 15 cells from 15 colonies. Additional ultrasound studies were undertaken. No fetal abnormalities were noted, and fetal size was consistent with estimated gestational age. The pregnancy was unremarkable for bleeding, illnesses, use of medications, alcohol or smoking, hyperthermia, and chemical or X-ray exposure. The pregnancy was continued and the baby was born by a normal spontaneous vaginal delivery at approximately 40 weeks of gestation. She weighed 2,948 g (20th centile) and was 50.8 cm long (60th centile) at birth. No minor anomalies were noted at delivery, and no neonatal problems were recorded. A cord blood specimen was collected for chromosome studies, and the 30 metaphases analyzed showed a normal (46,XX) female chromosome complement. The baby was breast-fed for the first 3 weeks and then changed to formula feedings without difficulty. She was hospitalized for 2 days at age 5 months, and again at 6 months, because of pneumonia. She was treated with antibiotics and has had no health problems since. She sat at age 5 months, crawled at 7 months, walked at 12 months, and had her first tooth at 5 months. At age 6 months the baby weighed 7.26 kg (30th centile) and was 64.1 cm long (30th centile). Her head circumference was 43 cm (50th centile). She is now 1 year old and has a 10-word vocabulary, stands independently, and can walk with assistance. She is on no medications.
The family history was unremarkable for genetic disorders; the patient has a healthy 4-year-old brother.
Polymerase chain reaction (PCR) was undertaken using D17S786 (range, 135–157 bp; heterozygosity index of 0.77) and D17S796 (range, 144–174 bp; heterozygosity index of 0.80) [Weissenbach et ah, 1992] DNA primers obtained from Research Genetics (Huntsville, AL), following the protocols reported by Weber and May [1989] and Mutirangura et al. [1993], Genomic DNA was isolated from amniocentesis specimens from the first and second procedures, from placental tissue obtained at the time of delivery, and from the cord blood sample. Peripheral blood specimens were also obtained from the parents for genetic analyses. PCR analysis with D17S786 showed heterozygosity with separate alleles produced (data not shown) for the mother (alleles 1 and 2), father (alleles 2 and 3), and infant (alleles 1 and 2) from DNA isolated from blood samples. Two alleles were also seen in the DNA isolated from the two separate amniocentesis specimens and from placental tissue from the patient; therefore, there was no evidence of a third allele in these tissue sources. PCR analysis with D17S796 showed heterozygosity with separate alleles produced for the mother (alleles 1 and 3), father (alleles 2 and 4), and infant (alleles 3 and 4) from DNA isolated from blood samples, indicating biparental (normal) inheritance of the chromosome 17s and not uniparental disomy in the infant (Fig. 1).
Fig. 1.
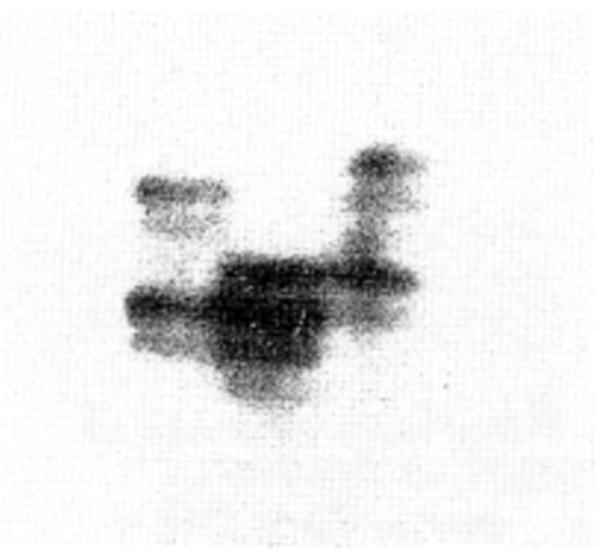
PCR amplification with radiolabeled primers from D1VS796 locus from genomic DNA isolated from peripheral blood from the newborn with trisomy 17 mosaicism identified by amniocentesis (middle lane), her mother (right lane), and her father (left lane). Each parent was heterozygous for different alleles. Biparental (normal) inheritance of D17S796 was seen in the newborn, with no evidence of disomy for chromosome 17.
In summary, we describe a rare case of trisomy 17 or trisomy 17 mosaicism in a fetus who was born healthy and without anomalies. Our patient is now 1 year old and has normal physical and psychomotor development. Trisomy 17 mosaicism was reported previously by Djalali et al. [1991] in amniotic fluid cells but not confirmed in the newborn infant. Lymphocytes from their healthy newborn male showed a normal male karyotype. The authors concluded that the trisomie cell lines were restricted, most probably to the extra fetal tissue, as is apparently true in our female infant. A second case of trisomy 17 mosaicism was reported by Bullerdick and Bartnitzke [1982] and the newborn had severe malformations, but no information was available regarding specific malformations.
Acknowledgments
We thank Verna Wyatt for expert preparation of the manuscript. We thank Lora Hedges for technical assistance, and acknowledge the support of NICHD grant 30329-02 (to M.G.B.).
Contributor Information
Merlin G. Butler, Departments of Pediatrics, Pathology, and Orthopedics, Vanderbilt University, Nashville, Tennessee
Richard L. Neu, Integrated Genetics, Santa Fe, New Mexico
Kay Mitchell, Women’s Health Center, Lebanon, Tennessee.
References
- Bullerdick J, Bartnitzke S. 46,XY/47,XY,+17 mosaicism in a newborn with severe malformations. Hum Genet. 1982;60:296. [Google Scholar]
- Djalali M, Barbi G, Grab D. Mosaic trisomy 17 in amniotic fluid cells not confirmed in the newborn. Prenat Diagn. 1991;11:399–402. doi: 10.1002/pd.1970110610. [DOI] [PubMed] [Google Scholar]
- Mutirangura A, Greenberg F, Butler MG, Malcolm S, Nicholls RD, Chakravarti A, Ledbetter DH. Multiplex PCR of three dinucleotide repeats in the Prader-Willi/Angelman critical region (15q11q13): Molecular diagnosis and mechanism of parental disomy. Hum Mol Genet. 1993;2:143–151. doi: 10.1093/hmg/2.2.143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weber JL, May PE. Abundant class of human DNA polymorphisms which can be typed using the polymerase chain reaction. Am J Hum Genet. 1989;44:388–396. [PMC free article] [PubMed] [Google Scholar]
- Weissenbach J, Gyopay G, Dib C, Vignal A, Morrisette J, Millasseau P, Vaysseix G, Lathrop M. A second generation linkage map of the human genome. Nature. 1992;359:794–801. doi: 10.1038/359794a0. [DOI] [PubMed] [Google Scholar]