

Abstract
Background:
The 7th package of health reform in Iran has been implemented in May 15, 1393, is concerned with the “promotion of natural childbirth.” It has been focusing on reducing cesarean section (CS) and promoting normal vaginal delivery (NVD) as broadly as possible. This study evaluated the changes in the vaginal delivery and cesarean before and after implementation of the 7th package of health reform in public and private hospitals of Isfahan Province in 2014.
Methods:
This was a quasi-experimental research. The population of this study contained all public and private hospitals in Isfahan Province covered by the Health Reform Program. It included 22 public and 6 private hospitals. The data collected from the vice chancellor of treatment in 6 months before and after the implementation of the program have been analyzed. SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA) and independent t-test have been employed for data analysis.
Results:
It was demonstrated that the increasing rate of NVD (P = 0.001) and decreasing rate of CS in public hospitals (P = 0.027) after the implementation of the plan were significant. On the other hand, the increasing rate of CS in private hospitals was significant (P = 0.026).
Conclusions:
Although this scheme has achieved its targets in public hospitals of Isfahan Province, it has not met its objectives in private hospitals. It seems CS operations were shifted from public hospitals to private ones, which is conflict with the objectives of the health reform plan.
Keywords: Cesarean section, health reform, Iran, Isfahan, normal vaginal delivery
Introduction
Childbirth is a natural process which begins with some regulatory systematic changes and ends with the delivery of the child. In some cases due to medical reasons including malposition, malpresentation, umbilical cord prolapse, and severe preeclampsia, it is impossible to deliver the child through vaginal operation, so cesarean section (CS) is done.[1,2,3] CS is a surgical incision for delivering a child by cutting through the wall of the mother's abdomen and uterus. Due to this fact that this method of delivery is invasive, it can only be used in some determinately certain cases.[4] In general, it cannot be regarded as a preferred mode of delivery, since like any other surgical operations, it carries significant consequences and risks for both mother and her child.[5]
According to the conducted research, CS carries numerous consequences including fever and infection, bleeding, aspiration, atelectasis, uterine inertia, tummy adhesion, increasing risk of hysterectomy, increasing probability need to blood transfusion, cardiopulmonary disorders, thromboembolism, biliary diseases for the mother, the possibility of damage to the bladder and ureter, placenta previa, and psychological effects.[6,7,8] Moreover, the mortality risk of mothers and infants involved in cesarean delivery is higher than that of natural delivery.[9,10,11,12,13] One more complication of CS is respiratory problems in newborns.[14]
In addition to these consequences due to the effects of surgery, proper nutrition through breastfeeding might be probably disturbed.[15]
Despite numerous consequences and complications of cesarean deliveries as well as international organizations' confirmation on restriction of CS, the rate of cesarean delivery in developed and developing nations is significantly high.[5]
In a study that was conducted by Shariat in 2002, the overall rates of CS over 20 years have increased from 5% to 25%.[16]
This increasing CS rate is also occurring in Iran. According to the studies, the percentage of CS in different cities of Iran is: Tehran 44%,[17] Hamedan 50.2%,[18] Damghan 51.7%,[19] Gilan 64.3%,[20] Gorgan 49.8%,[21] and Shiraz 66.4%.[22]
The increasing rate of CS in Iran has caused a concern for health-care system to decline cesarean delivery and promote natural vaginal delivery. This study was aimed to “promote normal delivery promotion instructions” to assess the impact on the rate of cesarean and normal delivery in public and private hospitals in Isfahan Province was conducted in 2014.
Methods
This is a quasi-experimental research before and after implementation of the 7th package of health reform in public and private hospitals of Isfahan Province in 2014. Its population consists of public and private hospitals. Although public hospitals are concerned with “natural childbirth promotion instruction,” private hospitals have also been selected to make a better assessment about the effects of the mentioned instruction. With regard to restrictions in population study, census method was used. All the hospitals affiliated to Isfahan University of Medical Sciences and private hospitals were included in this study. It included 22 public and 6 private hospitals. Public hospitals with English letters A to V specified and private hospitals with Greek letters I to VI shown. After a formal permission from vice chancellor with number of 394,594, refer to vice chancellor of treatment of Isfahan University of Medical Sciences and Statistics related to normal delivery and cesarean in targeted hospitals can be derived. SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA) and independent t-test were used for data analysis.
Results
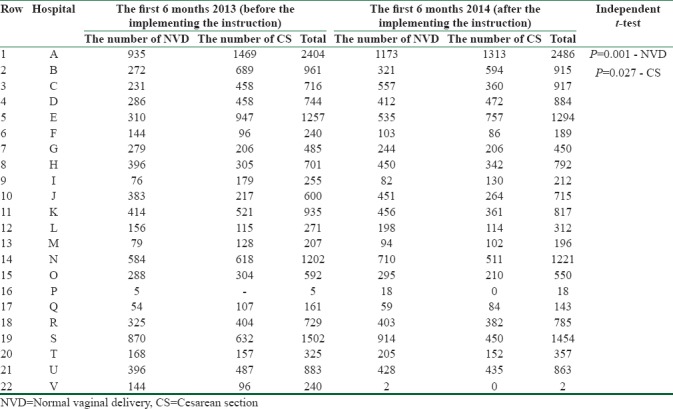
Overall 22 public hospitals investigated in this study. The highest and lowest numbers of vaginal delivery in 6 months before the implementation of the health-care reform plan in A hospital were 935 cases and in P hospital 5 cases and in the same 6 months after the implementation of the health-care reform plan the numbers of vaginal delivery after 6 months in A hospital was 1173 cases and in V hospital was 2 cases. The highest and lowest numbers of cesarean deliveries in 6 months before implementing the instruction in A hospital were 1469 cases and in P hospital no cesarean deliveries were reported. Alternatively, the numbers of cesarean deliveries after 6 months in A hospital were 1313 cases and in V and P hospitals no cesarean deliveries were reported. The paired t-test demonstrated that the fluctuations in the rates of cesarean and vaginal deliveries were significant [Table 1].
Table 1.
The numbers of vaginal and cesarean deliveries in 6 months before and after implementing the instruction in public hospitals of Isfahan Province
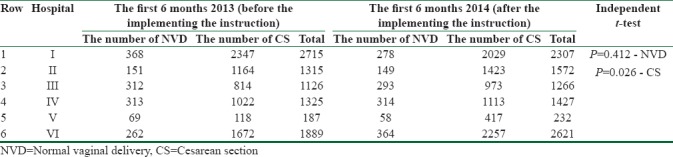
In private hospitals studied, the highest and lowest numbers of vaginal delivery in 6 months before implementing the “natural childbirth promotion instruction” in I hospital were 368 cases and in V hospital 69 cases. Alternatively, the numbers of cesarean delivery after 6 months in VI hospital were the highest number of 2257 and lowest number of 174 in V hospital. The paired t-test proved that the rate of cesarean delivery after implementing the plan was significant [Table 2].
Table 2.
The numbers of vaginal and cesarean deliveries in 6 months before and after implementing the instruction in private hospitals of Isfahan Province
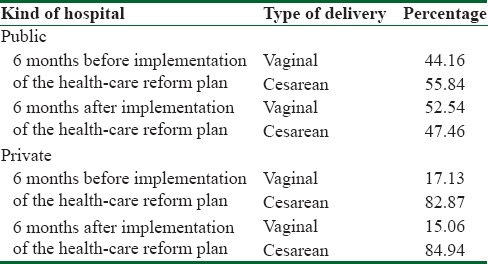
In addition, the ratio of vaginal delivery in public hospitals after implementation of the 7th package of health reform increased compared to the previous of the 7th package of health reform. This is the opposite in private hospitals [Table 3].
Table 3.
The percentage of vaginal and cesarean deliveries in 6 months before and after implementing the instruction in public and private hospitals of Isfahan Province
Discussion
The high rate of cesarean delivery in Iran convinced health-care system to decrease the high rate of CS. The findings of the present study have indicated that the natural childbirth promotion instruction has positively influenced this issue in public hospitals 6 months after implementing the plan. Moreover, according to Table 2, it has significantly increased the rate of normal vaginal delivery (P = 0.001). Apparently, it can be regarded as an encouraging point. Another encouraging point is that according to statistics, the plan has caused a significant reduction in rate of cesarean delivery in public hospitals (P = 0.027).
Studies in foreign countries in promoting natural childbirth are based more on hospital programs, and governments or health systems do not play a role. In other words, hospitals themselves attempted to plan to decrease the rate of cesarean delivery, so health-care system would not interfere directly in this process. Hence, no study was found to prove the direct interference of health-care system in each scheme. A case in point is the one conducted by Northwestern Memorial Hospital. This hospital embarked on a 5-year project to decline CS rate by instructing pregnant women, measuring CS rate, and evaluating the performance of medical staff. The results of this study led to falling in CS rate in nulliparous women from 27.3% to 18.2%.[23] Another study was conducted in one of the teaching hospitals of Florida. This hospital embarked on a 4-year project based on instructing pregnant women and specialists. Eventually, it could decrease cesarean delivery from 28 to 11 out of 100 cases.[24] The results of Robinson study proved that if there is a regular audit cycle for performed CSs, the fear of legitimate consequences prevents the specialists to deliver the child through cesarean without indication. Therefore, it might decrease cesarean delivery rate.[25] As it was noted, the above-mentioned instruction has so far been effective on the rate of cesarean and vaginal deliveries in the first 6 months of its implementation. The vaginal delivery rate in public hospitals has raised, and cesarean delivery rate has fallen. On the other hand, cesarean delivery rate in private hospitals has increased. Obviously, in accordance to studies carried out in other countries, it is concluded that they fruitfully have controlled cesarean rate by focusing on series of instructional actions. These specific actions have not been noticed in the 7th package of health reform in Iran. These practices include instructing pregnant women, instructing medical staff, establishing preventable regulations, and so forth. According to the results of this study, the refusal of performing cesarean and leading pregnant women to private sections might be considered as a cause in falling cesarean delivery rate in public hospitals which cannot be considered as a favorable outcome. Preferentially, to enhance the effects of the above-mentioned instruction, some arrangements have to be taken in account. To illustrate, educating society, establishing regular plans, and employing mass media are some instances which would be helpful to achieve satisfactory results in the long run.
Conclusion
Finally, it can be conclude that promoting vaginal delivery and reducing the rate of cesarean require comprehensive measures in different dimensions including instruction, raising awareness, enlightening, and establishing regulations. Hence, in this way, the rate of vaginal delivery might be effectively increased (P = 0.001). The results of this study revealed that the above-mentioned instruction has so far been efficient to increase vaginal delivery in public hospitals of Isfahan Province. Nonetheless, the increased cesarean rate has been significantly noticed in private hospitals which must be taken into consideration. To carry out a more appropriate evaluation and make a better judgment about this instruction, more comprehensive studies have to be conducted under certain circumstances.
Financial support and sponsorship
This study was supported by Vice Chancellor for Research and Technology, Isfahan, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
This study was supported by Vice Chancellor for Research and Technology, Isfahan, Iran (Grant Number 394594). We would like to thank Dr. Azade Alavi for his administrative support to undertake this project.
References
- 1.Sauls DJ. Effects of labor support on mothers, babies, and birth outcomes. J Obstet Gynecol Neonatal Nurs. 2002;31:733–41. doi: 10.1177/0884217502239209. [DOI] [PubMed] [Google Scholar]
- 2.Lavender T, Hofmeyr GJ, Neilson JP, Kingdon C, Gyte GM. Caesarean section for non-medical reasons at term. Cochrane Libr. 2012;3:434. doi: 10.1002/14651858.CD004660.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and causes of preterm birth. Lancet. 2008;371:75–84. doi: 10.1016/S0140-6736(08)60074-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Karami K, Najafian M, Shahri P, Faizi S, Noorifard Z. Comparison of frequency vaginal and caesarean deliveries. Iran J Public Health. 2009;38:97–102. [Google Scholar]
- 5.Rivlin ME, Martin RW. 4th ed. London: Little Brown and Company; 1999. Manual of clinical problems in obstetrics and gynecology; p. 510. [Google Scholar]
- 6.Khani S, Shabankhani B. Can the caesarean rate be reduced in Mazandaran. J Mazandaran Univ Med Sci. 2004;14:43–51. [Google Scholar]
- 7.Firoozi M, Hadizadeh Talasaz F. The survey of attitude of gynecologists and midwives about vaginal birth after caesarean delivery and barriers from their views. Ofogh Danesh J. 2006;12:26–33. [Google Scholar]
- 8.Karlström A, Lindgren H, Hildingsson I. Maternal and infant outcome after caesarean section without recorded medical indication: Findings from a Swedish case-control study. BJOG. 2013;120:479–86. doi: 10.1111/1471-0528.12129. [DOI] [PubMed] [Google Scholar]
- 9.Kilsztajn S, Carmo MS, Machado LC, Jr, Lopes ES, Lima LZ. Caesarean sections and maternal mortality in Sao Paulo. Eur J Obstet Gynecol Reprod Biol. 2007;132:64–9. doi: 10.1016/j.ejogrb.2006.06.005. [DOI] [PubMed] [Google Scholar]
- 10.Rahimikian F, Mirmohamadaliei M, Mehran A, Aboozari Ghforoodi K, Salmaani Barough N. Effect of education designed based on health belief model on choosing delivery mode. Hayat. 2009;14:25–32. [Google Scholar]
- 11.Landon MB, Hauth JC, Leveno KJ, Spong CY, Leindecker S, Varner MW, et al. Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. N Engl J Med. 2004;351:2581–9. doi: 10.1056/NEJMoa040405. [DOI] [PubMed] [Google Scholar]
- 12.Boskabadi H, Zakerihamidi M, Bagheri F. Outcomes of vaginal delivery and caesarean in Mashhad Ghaem University Hospital. Tehran Univ Med J. 2014;71:807–15. [Google Scholar]
- 13.Pallasmaa N, Ekblad U, Gissler M. Severe maternal morbidity and the mode of delivery. Acta Obstet Gynecol Scand. 2008;87:662–8. doi: 10.1080/00016340802108763. [DOI] [PubMed] [Google Scholar]
- 14.Hansen AK, Wisborg K, Uldbjerg N, Henriksen TB. Risk of respiratory morbidity in term infants delivered by elective caesarean section: Cohort study. BMJ. 2008;336:85–7. doi: 10.1136/bmj.39405.539282.BE. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.DiGirolamo AM, Grummer-Strawn LM, Fein SB. Effect of maternity-care practices on breastfeeding. Pediatrics. 2008;122(Suppl 2):S43–9. doi: 10.1542/peds.2008-1315e. [DOI] [PubMed] [Google Scholar]
- 16.Shariat M. Rate of caesarean and factors related to that in Maternity of Tehran. Payesh J. 2002;3:1. [Google Scholar]
- 17.Mohammadi TS, Kiani AA, Heydari M. The survey on tendencies of primiparous women for selecting the mode of delivery. Journal of Babol University of Medical Sciences. 2009;3:54–9. [Google Scholar]
- 18.Moeini B, Allahverdipour H, Mahjoub H, Bashirian S. Assessing pregnant women's beliefs, behavioral intention and predictive factors for caesarean section in Hamadan. Iranian Journal of Obstetrics, Gyneocology and Infertility. 2011;14:37–44. [Google Scholar]
- 19.Bahonar A, Shaebani A, Aghajani M. Determinants of caesarean and its trend in damghan, Iran. Iran J Epidemiol. 2010;6:33–8. [Google Scholar]
- 20.Moayed MS, Sohrabi Z. The trend analysis of caesarean section\rate in a hospital, Tehran, Iran. Payesh. 2011;10:261–4. [Google Scholar]
- 21.Tabandeh A, Kashani E. The prevalence of caesarean among employed educated women of medical science groups in Gorgan. Journal of Gorgan University of Medical Sciences Summer. 2007;9:67–70. [Google Scholar]
- 22.Mohammad BA, Tabatabaei S, Mohammad SN, Yazdani M. Factors influencing caesarean delivery method in Shiraz hospitals. IJN. 2009;21:37–45. [Google Scholar]
- 23.Socol ML, Garcia PM, Peaceman AM, Dooley SL. Reducing caesarean births at a primarily private university hospital. Am J Obstet Gynecol. 1993;168:1748–58. doi: 10.1016/0002-9378(93)90686-d. [DOI] [PubMed] [Google Scholar]
- 24.Sanchez-Ramos L, Kaunitz AM, Peterson HB, Martinez-Schnell B, Thompson RJ. Reducing caesarean sections at a teaching hospital. Am J Obstet Gynecol. 1990;163:1081–8. doi: 10.1016/0002-9378(90)91132-v. [DOI] [PubMed] [Google Scholar]
- 25.Robson MS, Scudamore IW, Walsh SM. Using the medical audit cycle to reduce caesarean section rates. Am J Obstet Gynecol. 1996;174:199–205. doi: 10.1016/s0002-9378(96)70394-0. [DOI] [PubMed] [Google Scholar]