

Abstract
The relationship between both interstitial and blood glucose remains a debated topic, on which there is still no consensus. The experimental evidence suggests that blood and interstitial fluid glucose levels are correlated by a kinetic equilibrium, which as a consequence has a time and magnitude gradient in glucose concentration between blood and interstitium. Furthermore, this equilibrium can be perturbed by several physiological effects (such as foreign body response, wound-healing effect, etc.), with a consequent reduction of interstitial fluid glucose versus blood glucose correlation. In the present study, the impact of operating in the interstitium on continuous glucose monitoring systems (CGMs) will be discussed in depth, both for the application of CGMs in the management of diabetes and in other critical areas, such as tight glycaemic control in critically ill patients.
Keywords: Continuous glucose monitoring, lag time delay, interstitial fluid, interstitium, subcutaneous
Continuous glucose monitoring (CGM) technology has become a fundamental tool in all those therapeutic applications where the measurement of the concentration and the rate of change of intracorporeal glucose are required, such as in the management of diabetes,1 in the development of closed-loop systems (‘artificial pancreas’)2,3 and tight glycaemic control in critically ill patients.4–6
If compared with the blood plasma glucose concentration (BG) measurements performed by means of either standard laboratory methods (SLB), point of care systems (POCTs) or self-monitoring of blood glucose systems (SMBGs), the main competitive advantage of CGMs lies in the capability of providing both absolute values and trends of glucose concentration. This enhances the capability to detect rapid hypo- and hyperglycaemia events (usually missed by discontinuous BG measurements), and allows the possibility of evaluating glycaemic variability parameters, which are promising markers for the prevention of diabetic complications and poor outcomes in critically ill patients.7–9 However, there are still some concerns regarding the accuracy and reliability of the actual subcutaneous CGM systems for the application in the most critical areas, such as closed-loop system development10 and tight glycaemic control in critically ill patients.11
The first and still most important field of CGM application is the management of diabetes. CGMs are utilised both in real-time (RT-CGM) for personal use as adjunctive device to SMBGs in the guidance and optimisation of the insulin delivery (particularly for those subjects under intensive insulin treatment and continuous subcutaneous insulin infusion),12–17 and as a blind/retrospective professional glycaemic Holter for diabetes diagnosis, therapy adjustment18–22 and control of gestational diabetes during pregnancy.23,24
Several studies demonstrated that the use of CGMs in the management of type 1 and 2 people with diabetes can decrease the occurrence of hypo/hyperglycaemia events,25–31 lower glycaemic variability,28 improve metabolic control and glycated haemoglobin (HbA1c) values1,16,17,28–33 both treatment safety and quality of life of people with diabetes.34–36
In the last decade several generations of CGMs for diabetes management were launched on the market, mainly from Medtronic, Dexcom, Abbot, and A. Menarini Diagnostics. In most cases these devices were subcutaneous, minimally invasive, amperometric/enzymatic biosensor-based systems37–39 and consequently provided an indirect evaluation of the plasma blood glucose level by means of a glucose concentration measurement in the extracellular interstitial fluid (IF). When using these devices, the sensor (needle-shaped electrode) or the sampling probe (in the case of microdialysis-based systems) needs to be inserted through the skin inside the subcutaneous fatty tissue in order to come into contact with the IF.34
Despite being in the early stages of the CGM development, a number of IF sampling and measurement methods have been considered (optical methods,40–44 capillary ultrafiltration,45 iontophoresis,46–52 hypodermic needles,53,54 ultrasound,46,55 open-flow microperfusion56 and impedance/electromagnetic spectroscopies).57,58 CMGs that showed the highest accuracy and reliability performances are those based on one of two types of technology.59 (1) transcutaneous (or needle-type) systems, where the amperometric biosensor is situated on the tip of a thin needle directly implanted in the subcutaneous tissue60,61 or (2) microdialysis-based systems, in which the glucose is harvested from the IF, by means of a constant flow of saline buffer, which passes through a subcutaneously implanted microdialysis probe, and leads to a biosensor flowcell placed downstream.62 All of these systems have been designed to operate in the subcutis, rather than in the blood, due to its easy and safe accessibility, and for the possibility of frequent sensor replacement.63,64 Given that the aim of CGMs is to guide the insulin delivery and therapy adjustments, which are all based on the plasma glucose concentration, the subcutaneous CGMs (SUB-CGMs) are calibrated using plasma glucose values (capillary or venous), and thus their accuracy evaluation is performed in comparison to BG values as references.65
Although the glucose concentration in the IF (IFG) demonstrated to have an high correlation with the corresponding plasma glucose value, it is nevertheless known that the IFG differs from BG both in time, generally presenting changes in delay in regard to the BG (physiological lag time), and in their absolute value of glucose concentration. In terms of the use of SUB-CGMs in diabetes management, if, on the one hand, the difference between BG and IFG is considered acceptable when the CGM data are used (and calibrated) retrospectively, on the other hand, this raises concerns about the impact of a significant physiological lag time in the capability of CGMs to support in RT the person with diabetes in his or her clinical decisions (such as if to inject insulin or not, or insulin bolus dose).66,67 Moreover, in the most critical areas of potential application of CGMs (closed-loop systems, tight glycaemic control), the glucose measurement/sampling in the IF is actually considered a tremendous limit to the possibility of achieving a truly RT monitoring, and with no risk of uncorrelated response against blood compartment due to physiological condition of the patient.68,69 For these reasons, in order to achieve tight glycaemic control in critically ill patients, an increasing number of companies shifted the selected sampling site from the subcutaneous tissue to the blood compartment by developing intravascular CGMs.59,70–77
Finally, improving the comprehension of BG versus IFG relationship and of its impact on the SUB-CGMs is a crucial step for their further optimisation, improved accuracy evaluation and for the understanding of their objective application limits.
Experimental Evidence
Due to the increasing interest in CGM technology, the physiological relationship between IF and plasma in glucose concentration has been a widely debated topic in the recent years, and thus it has been investigated through a relevant number of studies, a summary of which is reported in Table 1. These evaluations were performed especially in terms of time lag between the changes in BG and in IFG, reporting values ranging from –16 to 25 minute.78,79 Due to the lack of a well- recognised standard method for the IFG sampling and measurement, a significant boost to these studies was given by the microdialysis technique,80–82 and thereafter by the availability of CGMs.
Table 1: Summary of Interstitial Glucose versus Blood Glucose Average Lag Time, Estimated Values and Related Study Information.
| First Author/Year of Publication/Reference | Estimated Lag Time (Minutes) | Study Population | Interstitial Fluid Sampling Method | Measuring Principle or CGM System (If Any) |
|---|---|---|---|---|
| Shichiri M, 1986169 | 5 | People with diabetes (n=5) | Transcutaneous sensor | Enzymatic biosensor |
| Matthews D, 1988170 | 0 | Anaesthesised rats (n=11), healthy subjects (n=10) | Transcutaneous sensor | Enzymatic biosensor |
| Aalders AL, 1991171 | Rise = 4 | People with diabetes (n=10), healthy subjects (n=6) | Microdialysis | Enzymatic biosensor |
| Fall = 8 | ||||
| Meyeroff C, 1992172 | 0–18 | People with type 2 diabetes (n=7), healthy subjects (n=13) | Microdialysis | Enzymatic biosensor |
| Sternberg F, 199690 | 2–12 | IT people with diabetes (n=40) | Microdialysis | Enzymatic biosensor |
| Thomé-Duret V, 199678 | -16 | Anaesthesised rats | Transcutaneous sensor | Enzymatic biosensor |
| Schmidtke DW, 199879 | 9–25 | Anaesthesised rats | Transcutaneous sensor | Enzymatic biosensor |
| Tamada JA, 199948 | 18±10 | People with type 1 and 2 diabetes (n=92) | Reverse iontophoresis | GlucoWatch (Cygnus) |
| Smith A, 1999173 | 2–4 | Healthy subjects (n=4) | Microporation | Fluorescein detection |
| Rebrin K, 200064 | 5–12 | Anaesthetised dogs | Transcutaneous sensor | MiniMed CGMS (Medtronic) |
| Gross T, 2000174 | 10 | People with type 1 or 2 diabetes (n=135) | Transcutaneous sensor | MiniMed CGMS (Medtronic) |
| Aussedat B, 200091 | 5–10 | Anaesthesised rats | Transcutaneous sensor | Enzymatic biosensor |
| Feldman B, 2003146 | 5 | People with type 1 diabetes (n=30) | Transcutaneous sensor | FreeStyle Navigator (Abbott) |
| Boyne MS, 200366 | 4–10 | People with type 1 diabetes (n=14) | Transcutaneous sensor | MiniMed CGMS (Medtronic) |
| Kulcu E, 200383 | 5 | IT people with type 1 or 2 diabetes (n=51) | Reverse iontophoresis | GlucoWatch (Cygnus) |
| Varalli M, 2003175 | 2 | People with diabetes, healthy subjects | Transcutaneous sensor | Glucoday (A. Menarini Diagnostics) |
| Steil GM, 200587 | 3–8 | Insulin-induced hypoglycaemia in healthy subjects (n=10) | Transcutaneous sensor | MiniMed CGMS (Medtronic) |
| Weinstein RL, 2007176 | 13 | People with type 1 diabetes (n=58) | Transcutaneous sensor | FreeStyle Navigator (Abbott) |
| Wentholt IM, 2007177 | 6 | People with type 1 diabetes (n=13) | Microdialysis | Glucoday (A.Menarini Diagnostics) |
| Groenendaal W, 2008145 | 1–3 (dermis) | Insulin-induced hypoglycaemia in healthy subject (n=10) | Transcutaneous sensor | MiniMed CGMS (Medtronic) |
| 5–10 (adipose tissue) | ||||
| Kamath A, 2009178 | 6±1 | IT people with diabetes (n=117) | Transcutaneous sensor | SEVEN (Dexcom) |
| Bailey T, 2009179 | 8 | IT people with type 1 or 2 diabetes (n=51) | Transcutaneous sensor | seven plus (Dexcom) |
| Garg SK, 2009180 | 5±3 (Dexcom) | People with type 1 diabetes (n=14) | Transcutaneous sensor | SEVEN (Dexcom), FreeStyle Navigator (Abbott) |
| 10±3 (Abbott) | ||||
| Kovatchev BP, 2009164 | 13 | People with type 1 diabetes (n=28) | Transcutaneous sensor | Freestyle Navigator (Abbott) |
| Mazze RS, 200967 | 0–20 (Dexcom) | IT people with type 1 or 2 diabetes (n=24) | Transcutaneous sensor | Minimed Guardian RT (Medtronic), STS (Dexcom) |
| 17–32 (Medtronic) | ||||
| Valgimigli f, 2010181 | 11 | People with type 1 and 2 diabetes (n=12) | Microdialysis | GlucoMen Day (A. Menarini Diagnostics) |
| McGarraugh G, 2011182 | 10 | People with type 1 diabetes (n=47) | Transcutaneous sensor | FreeStyle Navigator (Abbott) |
| Ward wk, 2011183 | Rise = 9 | People with type 1 diabetes (n=7) | Transcutaneous sensor | seven plus (Dexcom) |
| Fall = 2 | ||||
| Keenan DB, 2012184 | 8–12 | People with type 1 and 2 diabetes (n=97) | Transcutaneous sensor | Enlite Sensor (Medtronic) |
CGM = continuous glucose monitor; IT = insulin treated.
The outcomes of all the studies reported in Table 1 lead to the assumption that IFG and BG are related by a ‘time gradient’, consisting in the delay (or lag time) between BG and IFG changes, and a ‘magnitude gradient’, corresponding to the difference between IF and plasma in the glucose concentration excursion amplitude and absolute value during the steady-states.83–85 Furthermore, several physiological conditions, related to both the foreign body response (FBR) to the sensor implantation68 and to the investigated subjects themselves,5,64,69 were identified to significantly affect the correlation between IFG and BG.
Time Gradient
With the time gradient it is intended the delay, or lag time, observed between the variation of the BG value (usually referring to the venous plasma) and the corresponding change in IFG. The term ‘lag time’ usually refers only to the physiological lag, and thus only to those physiological processes regulating the glucose exchange between blood and interstitium. However, in several studies, this also included the instrumental lag, specific to the device used for the IFG sampling and measurement. The instrumental lag time also comprises a sampling lag, corresponding to the time needed for glucose transport from the IF to the biosensor and a computational lag, related to all the calculation algorithms applied to the recorded raw CGM signal before the measurement result is returned by the device (e.g. moving average over a period, noise filters, etc.)
The main and ongoing concerns related to the lag time are if it is either positive or negative, and thus if the IFG follows or precedes the BG, and if its value is constant or variable.86 In the large majority of studies it was observed that the IFG delayed with respect to the BG, independently of whether the BG is rising, falling or reaching nadirs/peaks, with a lag time value that ranged between 5 and 25 minutes,66,87 thus confirming a kinetic equilibrium based on a ‘two-compartment’ model of glucose diffusion from blood to IF.64 Furthermore, the lag time presented both high inter-67,68,83 and intra-subject variability (depending on the rising or falling phase of BG,88 from the applied insulin or glucose infusion rate,89 etc.)
In other studies,78,79,90 the IFG was found to anticipate the BG decrease during insulin-induced hypoglycaemia. This was explained by increased glucose uptake from the IF by the surrounding cells, which lead IFG to drop prior to BG, as described by the ‘push–pull’ model.91
Magnitude Gradient
Magnitude gradient generically means the difference in absolute glucose concentration between plasma and IF. This is related both to the glucose concentration value in the two compartments during the steady-states, and to the magnitude of the respective glucose concentration excursions.64,83,92
Studies reported conflicting results about this topic. In some studies,87,93–95 involving mainly healthy subjects, the magnitude of the IFG and BG excursions and their values in their respective steady-states were found to be similar. However, a large group of studies agrees that both the glycaemic excursions and steady-state values of IFG and BG can show significant differences,64,84,85,96 even maintaining a high correlation. Kulcu et al.83 reported a relevant difference in the glucose excursion magnitude between IFG and BG at high glycaemic values during rapid rises of BG. Caplin et al.84 observed that, following to falling phases of BG, the glucose concentration in the interstitium throughout steady-states was lower than that of plasma for prolonged periods of time in people with diabetes,69 confirming what was previously observed in animal studies.91,97
Physiological Conditions Affecting Blood Glucose and Interstitial Fluid Glucose Correlation
The kinetic equilibrium between BG and IFG, which allows an explanation of both the time and magnitude gradients, can be perturbed by the characteristics of the subcutaneous tissue, which represents a non-standard matrix in continuous change, depending on the physiological conditions of the subject.64,91,98,99
Considering the case of minimally invasive CGMs, the insertion of a probe/sensor in the subcutaneous tissue causes a trauma at the implantation site, because of the disruption of the tissue structure, thus leading to a FBR.39,100,101 Despite the development of increasingly miniaturised probes/sensors, composed of materials with higher degrees of biocompatibility,68,102 several local tissue reactions are likely to occur at the implantation site:
• Biofouling: aspecific protein adsorption on the foreign body surface (collagen and other proteins are secreted into the IF space due to transforming grow factor β1 and connective tissue growth factor),103–105 with a consequent obstruction to the glucose diffusion across the IF–probe interface.66,106–109
• Wound-healing effect: the wound-healing cascade104,110 can increase the vascularisation around the implanted probe, modifying the inter-compartment glucose equilibrium between plasma and IF.102 The formation of well-vascularised granulation tissue near to the implantation site is likely to enhance glucose diffusion at the sensor–tissue interface111,112 compared with avascular fibrous encapsulation.113
• Localised accumulation of inflammatory cells, macrophages, monocytes, mast cells and the release of cytokines and chemokines;104,110 can lead to increased oxygen and glucose consumption near to the implantation site.102,114,115
• Fibrous encapsulation at sensor–tissue interface can alter the diffusional equilibrium.63,115–121
• Proteolytic enzymes and free radicals,118,122,123 and local drops of pH due to foreign body digestion attempts,124 can damage to the sensor/probe surface.
• Cycles of bleeding and coagulation at the implantation site can tremendously interfere the sensor–probe functionality.90,125–128
Generally the main effect of these local reactions is transitory and limited to the few hours after the probe implantation, until a new physiological equilibrium at the tissue/probe interface is reached.129 However, the occurrence of pressures, collisions or mechanical shocks on the implantation area can reactivate the local reactions and thus alter the equilibrium at the sensor–tissue interface, leading to another transitory period of lowered IFG versus BG correlation,130–132 or even to a definitive failure of the CGM sensor. Furthermore, these phenomena are considered as possible causes of the sensors drift in signal, usually observed in the most of the enzyme-based subcutaneous CGMs, and which can make them progressively less sensitive and accurate over time.63,66,110,119,133
In addition to local reactions, other physiological conditions can further impact on the IFG versus BG correlation, such as those related to critically ill patients (oedema, shock, hypotension, etc.),5,64 to post-surgical situations,134–136 drug administration,112 altered blood perfusion in the sensor area,69 bodily thermoregulation137,138 and physical exercise.139,140
Referring to studies results reported in Table 1, such a high variability of outcomes indicates that both time and magnitude gradients are extremely case dependent, and that their presence/absence, variability and absolute values are related to the specific experimental conditions in which each study was performed.92 IF sampling method used (microdialysis, transdermal, iontophoresis, etc.); IF sampling site (epidermis, dermis, adipose tissue); IFG measuring method (CGMs or SLB); tested population (animals/humans, healthy or type 1/type 2 people with diabetes); glycaemic control protocol (oral glucose tolerance test [OGGT], insulin/glucose clamp, insulin-induced hypoglycaemia, etc.); appropriate subtraction of the instrumental time lag (of the CGM device or of the sampling/measurement method used); effect of noise reduction and other compensation/elaboration algorithms, which can increase the instrumental lag that is then erroneously perceived as physiological lag time;86,141,142 CGM system calibration method.
Models Describing Interstitium/Blood Glucose Equilibrium
Although a total consensus was not yet achieved on the BG/IFG relationship, a number of mathematical models for the BG versus IFG equilibrium description have been proposed. These models are based on the assumption of a free diffusion of glucose molecule between blood and interstitium, and in its uptake from the IF by the surrounding cells.64,91,143,144
Rebrin and Steil64 proposed a ‘two-compartments’ model, which described IF and blood as two independent compartments (or pools), separated by a diffusional barrier through which the glucose is free to diffuse based on its concentration gradient86,144 (see Figure 1). Moreover, the glucose is cleared from the IF by the surrounding cells, depending from IFG. This model provides an effective mathematical description of two important phenomena experimentally observed in several studies: the IFG follows the BG with a certain lag time; during the steady-states the glucose concentration in the two compartments can be significantly different. The only concern about this model is the assumption that both the diffusion across the IF/blood barrier and the clearance from the IF are related to BG and IFG values by constants (K12 , K21 and K02 in the equation of Figure 1), while several evidences suggest that the dependence of these diffusion processes by BG and IFG is variable over the time.
Figure 1: Two-compartment Model Proposed by Rebrin and Steil64.
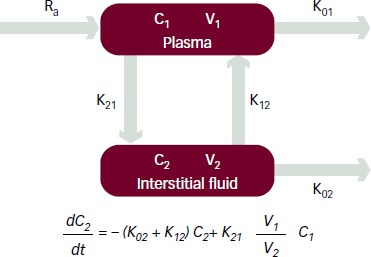
Theoretical relation between the glucose concentration in plasma (C1) and in interstitial fluid (C2), based on diffusion (K12 , K21) and clearance (K02) parameters.
Another widely recognised model, based on the ‘push–pull’ effect, was proposed by Aussedat et al.91 This approach hypothesised that during the rising of BG the lag time between BG and IF is caused by the glucose diffusion (push) from blood to IF, while during the falling period of BG the IFG decreases in advance with respect of BG, due to the insulin-induced uptake (pull) of glucose by the surrounding cells. This model allows explanation how in some particular conditions (e.g. insulin-induced hypoglycaemia) the drop of IFG can anticipate that of BG.78,79
The previous approaches were further refined by Groenendaal et al.,145 reporting a model where a specific equilibrium between IFG and BG was described for each skin layer (epidermis, dermis, adipose tissue).
Impact of Interstitium/Blood Differences on Continuous Glucose Monitoring Systems
The fact that SUB-CGMs provide an indirect BG evaluation by means of an IFG measurement entails a significant impact on the accuracy of these systems. These effects can be generically categorised into three types: pre-analysis effects, affecting the system prior of data collection (such as on calibration); intra-analysis effects, occurring during the measuring phase; and post-analysis effects, related to the CGMs accuracy evaluation.
Pre-analysis Effects – Errors during the Calibration Phase
The calibration of a system that operates in a certain matrix, the IF, using measurement values collected in another matrix (venous/capillary blood) means that those differences existing between these matrixes will reduce the calibration quality, and thus the accuracy of the system.69 This is in addition to the inherent error related to the calibration values itself, which can be significantly high if collected by means of SMBGs146 (up to 20 % versus SLB).147
In order to minimise the error related to the BG versus IFG time gradient, all the manufacturers of CGMs require the system calibration to be performed using euglycaemic BG measurements collected during steady-states of the glycaemic value, where the resulting effect of the physiological lag time is negligible.146,148,149
Most of the CGMs are equipped with control algorithms capable of evaluating both the acceptability of the selected calibration values, based on the manufacturer’s criteria,150,151 and the stability of the corresponding CGM signal,97 prior that the calibration is definitively applied.
In order to overcome the BG versus IFG magnitude gradient, several two-point calibration methods have been developed.141,152 These methods are based on the use of two independent BG calibration points, collected in distinct moments and required to be significantly different in the absolute glucose value (>30 mg/dl), for the estimation and calibration of the IFG excursion magnitude to those of the BG, for the sensor background current correction,63,111 and also for reducing the impact of BG measurement system uncertainty.152 Obviously these calibration methods are well applicable in the case of a retrospective analysis of the CGM data, while they are less effective and more error prone when applied in RT.
The physiological conditions affecting BG versus IFG correlation (see above), generally do not allow any calibration in the first period after probe implantation (run-in time) to be performed, and require a frequent system calibration in the first monitoring hours.
All the pre-analysis effects of the lag time can be mitigated in the retrospective calibration of the CGMs, where the availability of several BG references can allow the calibration versus both the time and magnitude gradient between BG and IFG to be optimised, by means of an algorithm-driven calibration points selection, and two-point or linear regression methods.153,154 For example, King et al.152 demonstrated that a retrospective recalibration of the RT-calibrated CGM data allowed a relevant reduction of the mean absolute deviation during the steady euglycaemic state (from 20.9 down to 10.6 mg/dl). Similar results were showed by Facchinetti et al.,155 where the mean absolute percentage error was reduced from 10.4 to 6.9 %. In the case of the RT calibration of CGMs the application of retrospective-wise selection of the calibration points is not applicable, and thus the impact on the calibration due to operate in the subcutaneous tissue cannot be significantly mitigated.
Intra-analysis Effects – Lag Time and Loss of Interstitial Fluid Glucose/Blood Glucose Correlation during the Monitoring Session
The lag time between BG and IFG is the most recognised source of error in the CGMs. Rather than the presence of a delay, the real problem stems from delay variability. In several cases67,68,83,88,89 the lag time was observed to be variable not only between different subjects, but also within the glycaemic profile of the same subject (e.g. depending from rising and falling phase of BG). Again, this problem is significantly mitigated when the CGM data are retrospectively used, since in this case the lag time (physiological and instrumental) can be evaluated and compensated prior to proceeding with the accuracy evaluation. Obviously, the higher the value and variability of the delay the lower will be the effectiveness of its evaluation and correction. On the contrary, the presence of the time lag, either constant or variable, cannot be eliminated in the RT CGMs application where glucose measurement will follow the BG value with a delay corresponding to the sum of physiological and instrumental lag, usually resulting in a value between 10 and 20 minutes. In this case an excessively high or inconsistent lag time could significantly decrease the effectiveness of the CGM device in controlling insulin delivery.66 Another source of CGM inaccuracy during the monitoring session is related to the occurrence of those physiological conditions that can lower the BG and IFG correlation (see above).
The first strategy adopted for mitigating these kinds of CGM errors is the development of more and more biocompatible and miniaturised sensors,68,156 in order to minimise the FBR and therefore the possibility of having local reactions after implantation.
A more-recent approach consists of redundant sensing, which is based on the use of multiple sensors contemporaneously, and in the combination of all the CGM signals collected in parallel.157 The aim of this method is to detect individual aberrant (outlier) sensor values by means of the responses of the other sensors. Consequently, the crucial step in this approach is the processing method applied for combining the multiple data acquired.158 The redundant sensing can also be ‘orthogonal’, that is, using sensors with different measuring principles, and thus are subjected to different interferences.159–161
On one hand this is a very promising way to increase the reliability of subcutaneous CGMs by correcting for gross errors, inconsistent data and all those evident system failures that are not expected to occur in all the implanted sensors. On the other hand, the capability of these approaches in enhancing the accuracy of CGMs has still to be demonstrated, especially against those physiological conditions affecting the BG versus IFG correlation.
Despite the current developments regarding biocompatibility, miniaturisation and redundant sensing, the CGM errors related to the loss of correlation between IF and blood cannot be avoided162 either in the retrospective or in the RT CGM application, and can be detected only by the direct comparison with frequent BG reference measurements.
Post-analysis Effects – Errors in the Accuracy Evaluation
Following the Performance Metrics for Continuous Interstitial Glucose Monitoring; Approved Guideline (POCT05-A),65 the assessment of the CGMs’ accuracy is actually performed using BG values as references. Consequently, each decrease in the IFG versus BG correlation is erroneously perceived as a CGM measurement error, and thus results in an apparent accuracy deterioration.163 In order to take into account the contribution of the lag time, the guideline suggests that an evaluation, and possibly compensation, of the lag time prior to proceeding with the accuracy assessment. The suggested method is the Kovatchev’s Poincarè Plot,164 which consists of the calculation of Pearson’s correlation coefficient R between CGM and BG reference data pairs, by applying increasing delays to the CGM signal. The applied delay corresponding to the highest R value is considered as the average lag time. The correction is then applied by shifting back in time the CGM data subtracting a delay equal to the calculated average lag time. Despite the fact this method is based on the assumption that the lag time is represented by a constant value (while the evidences suggest it to be variable), and that the correlation parameter used (R) is not ideal for the evaluation of data coming from different subjects with different glucose excursions,165 it offers a good compromise between calculation simplicity and correction for the lag time error. Other lag time evaluation and correction methods, which account for a variable delay on the base of diffusional models, demonstrated the potentiality to further minimise the lag-time effect on the accuracy evaluation, but leading also to an increased calculation complexity.152,163
Another valuable improvement to CGMs’ accuracy assessment was introduced by the Continuous Glucose Error Grid Analysis (CG-EGA),166 which adapted Clarke’s Error Grid Analysis,167 intended for SMBGs, to the particular case of CGMs. The CG-EGA applies different point-accuracy acceptance criteria dependently from the rate of change of BG, and thus allows progressively higher tolerances in case of rapid glucose excursions. Although this method was not designed to directly correct for the lag time, considering that the lag time contribution to the CGMs errors is higher when rapid glucose fluctuations occur, the effect of the lag time is indirectly mitigated anyway.
Conclusion
The relationship between interstitial and blood glucose is still a debated topic, on which a clear consensus has not yet been achieved. The experimental evidence suggest that BG and IFG are correlated by a kinetic equilibrium, which has as consequences a time and magnitude gradient in glucose concentration between blood and interstitium.83 Furthermore, this equilibrium can be perturbed by several physiological effects (such as FBR, wound-healing effect, etc.), with a consequent reduction of IFG versus BG correlation.39,100,101
Regardless, the CGMs errors due to operate in the interstitium are considered acceptable in diabetes management. This is particularly valid when CGM data are retrospectively used, while in the RT application of CGMs the presence of a lag time still raises some concerns on their effectiveness in controlling insulin delivery.66,67 Moreover, regarding the application in the most critical areas, such as tight glycaemic control on critically ill patients, the effects related to measuring in the subcutaneous tissue, instead of blood, are actually considered as a significant limit to SUB-CGMs utilisation, and thus suggest a shift in the development of CGMs, moving to CGM devices which operate directly in the intravascular compartment.59,70–77,168
References
- 1.Benhamou PY, Catargi B, Delenne B. et al. Real-time continuous glucose monitoring (CGM) integrated into the treatment of type 1 diabetes: Consensus of experts from SFD, EVADIAC and SFE. Diabetes Metab. 2012;38:S67–83. doi: 10.1016/S1262-3636(12)71538-0. [DOI] [PubMed] [Google Scholar]
- 2.Hovorka R, Nodale M, Haidar A, Wilinska ME. Assessing performance of closed-loop insulin delivery systems by continuous glucose monitoring: drawbacks and way forward. Diabetes Technol Ther. 2013;15:4–12. doi: 10.1089/dia.2012.0185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Klonoff DC. The artificial pancreas: how sweet engineering will solve bitter problems. J Diabetes Sci Technol. 2007;1:72–81. doi: 10.1177/193229680700100112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Van den Berghe G, Wouters F, Verwaest C. et al. Intensive insulin therapy in critically ill patients. N Engl J Med. 2001;345:1359–67. doi: 10.1056/NEJMoa011300. [DOI] [PubMed] [Google Scholar]
- 5.De Block C, Manuel-y-Keenoy B, Van Gaal L, Rogiers P. Intensive insulin therapy in the intensive care unit. Assessment by continuous glucose monitoring. Diabetes Care. 2006;29:1750–6. doi: 10.2337/dc05-2353. [DOI] [PubMed] [Google Scholar]
- 6.Holzinger U, Warszawska J, Kitzberger R. et al. Real-time continuous glucose monitoring in critically ill patients. Diabetes Care. 2010;33:467–72. doi: 10.2337/dc09-1352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Siegelaar SE, Holleman F, Hoekstra JBL, DeVries JH. Glucose variability; does it matter? Endocr Rev. 2010;31:171–82. doi: 10.1210/er.2009-0021. [DOI] [PubMed] [Google Scholar]
- 8.Penckofer S, Quinn L, Byrn M. et al. Does glycemic variability impact mood and quality of life? Diabetes Technol Ther. 2012;14:303–10. doi: 10.1089/dia.2011.0191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Klonoff DC. Technology to treat hyperglycemia in trauma. J Diabetes Sci Technol. 2007;1:151–2. doi: 10.1177/193229680700100201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Damiano RE, El-Khatib FH, Zheng H. et al. A comparative effectiveness analysis of three continuous glucose monitors. Diabetes Care. 2013;36:251–9. doi: 10.2337/dc12-0070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ligtenberg JJM, de Plaa ME, Zijlstra JG. Continuous subcutaneous glucose monitoring: good enough to use in glucose regulation protocols? Critic Care. 2011;15:403. doi: 10.1186/cc9374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Battelino T, Conget Olsen B I. et al. The use and efficacy of continuous glucose monitoring in type 1 diabetes treated with insulin pump therapy: a randomised controlled trial. Diabetologia. 2012;55:3155–62. doi: 10.1007/s00125-012-2708-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rubin RR, Peyrot M. STAR 3 Study Group, health-related quality of life and treatment satisfaction in the sensor-augmented pump therapy for A1C Reduction 3 (STAR 3) trial. Diabetes Technol Ther. 2012;14:143–51. doi: 10.1089/dia.2011.0162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.O’Connell MA, Donath S, O’Neal DN. et al. Glycaemic impact of patient-led use of sensor-guided pump therapy in type 1 diabetes: a randomised controlled trial. Diabetologia. 2009;52:1250–7. doi: 10.1007/s00125-009-1365-0. [DOI] [PubMed] [Google Scholar]
- 15.Raccah D, Sulmont V, Reznik Y. et al. Incremental value of continuous glucose monitoring when starting pump therapy in patients with poorly controlled type 1 diabetes: the RealTrend study. Diabetes Care. 2009;32:2245–50. doi: 10.2337/dc09-0750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hermanides J, Nørgaard K, Bruttomesso D. et al. Sensor-augmented pump therapy lowers HbA1c in suboptimally controlled Type 1 diabetes; a randomized controlled trial. Diabet Med. 2011;28:1158–67. doi: 10.1111/j.1464-5491.2011.03256.x. [DOI] [PubMed] [Google Scholar]
- 17.Bergenstal RM, Tamborlane WV, Ahmann A. et al. Effectiveness of sensor-augmented insulin-pump therapy in type 1 diabetes. N Engl J Med. 2010;363:311–20. doi: 10.1056/NEJMoa1002853. [DOI] [PubMed] [Google Scholar]
- 18.Cosson E, Hamo-Tchatchouang E, Dufaitre-Patouraux L. et al. Multicentre, randomised, controlled study of the impact of continuous sub-cutaneous glucose monitoring (GlucoDay®) on glycaemic control in type 1 and type 2 diabetes patients. Diabetes Metab. 2009;35:312–8. doi: 10.1016/j.diabet.2009.02.006. [DOI] [PubMed] [Google Scholar]
- 19.Ludvigsson J, Hanas R. Continuous subcutaneous glucose monitoring improved metabolic control in pediatric patients with type 1 diabetes: a controlled crossover study. Pediatrics. 2003;111:933–8. doi: 10.1542/peds.111.5.933. [DOI] [PubMed] [Google Scholar]
- 20.Tanenberg R, Bode B, Lane W. et al. Use of the continuous glucose monitoring system to guide therapy in patients with insulin-treated diabetes: a randomized controlled trial. Mayo Clin Proc. 2004;79:1521–6. doi: 10.4065/79.12.1521. [DOI] [PubMed] [Google Scholar]
- 21.Bode BW, Gross TM, Thornton KR, Mastrototaro JJ. Continuous glucose monitoring used to adjust diabetes therapy improves glycosylated hemoglobin: a pilot study. Diabetes Res Clin Pract. 1999;46:183–90. doi: 10.1016/s0168-8227(99)00113-8. [DOI] [PubMed] [Google Scholar]
- 22.Lagarde WH, Barrows FP, Davenport ML. et al. Continuous subcutaneous glucose monitoring in children with type 1 diabetes mellitus: a single?blind, randomized, controlled trial. Pediatr Diabetes. 2006;7:159–64. doi: 10.1111/j.1399-543X.2006.00162.x. [DOI] [PubMed] [Google Scholar]
- 23.Dalfrà MG, Sartore G, Di Cianni G. et al. Glucose variability in diabetic pregnancy. Diabetes Technol Ther. 2011;13:853–9. doi: 10.1089/dia.2010.0145. [DOI] [PubMed] [Google Scholar]
- 24.Voormolen DN, DeVries JH, Franx A. et al. Effectiveness of continuous glucose monitoring during diabetic pregnancy (GlucoMOMS trial); a randomised controlled trial. BMC Pregnancy Childbirth. 2012;12:164. doi: 10.1186/1471-2393-12-164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ryan M, Savarese V, Hipszer B. et al. Continuous Glucose Monitor Shows Potential for Early Hypoglycemia Detection in Hospitalized Patients. Diabetes Technol Ther. 2009;11:745–7. doi: 10.1089/dia.2009.0071. [DOI] [PubMed] [Google Scholar]
- 26.Deiss D, Bolinder J, Riveline JP. et al. Improved glycemic control in poorly controlled patients with type 1 diabetes using real-time continuous glucose monitoring. Diabetes Care. 2006;29:2730–2. doi: 10.2337/dc06-1134. [DOI] [PubMed] [Google Scholar]
- 27.Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Beck RW, Hirsch IB, Laffel L. et al. The Effect of continuous glucose monitoring in well-controlled Type 1 diabetes. Diabetes Care. 2009;32:1378–83. doi: 10.2337/dc09-0108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Battelino T, Phillip M, Bratina N. et al. Effect of continuous glucose monitoring on hypoglycemia in type 1 diabetes. Diabetes Care. 2011;34:795–800. doi: 10.2337/dc10-1989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Battelino T, Conget Olsen B I. et al. The use and efficacy of continuous glucose monitoring in type 1 diabetes treated with insulin pump therapy: a randomised controlled trial. Diabetologia. 2012:3155–62. doi: 10.1007/s00125-012-2708-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schaepelynck-Belicar P, Vague P, Simonin G, Lassmann-Vague V. Improved metabolic control in diabetic adolescents using the Continuous Glucose Monitoring System (CGMS) Diabetes Metab. 2003;29:608–12. doi: 10.1016/s1262-3636(07)70076-9. [DOI] [PubMed] [Google Scholar]
- 31.Garg SK, Schwartz S, Edelman SV. Improved glucose excursions using an implantable real-time continuous glucose monitoring sensor in adults with type 1 diabetes. Diabetes Care. 2004;27:734–8. doi: 10.2337/diacare.27.3.734. [DOI] [PubMed] [Google Scholar]
- 32.Chase HP, Roberts MD, Wightman C. et al. Use of GlucoWatch Biographer in children with type 1 diabetes. Pediatrics. 2003;111:933–8. doi: 10.1542/peds.111.4.790. [DOI] [PubMed] [Google Scholar]
- 33.Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group. Tamborlane WV, Beck RW, Bode BW. et al. Continuous glucose monitoring and intensive treatment of type 1 diabetes. N Engl J Med. 2008;359:1464–76. doi: 10.1056/NEJMoa0805017. [DOI] [PubMed] [Google Scholar]
- 34.Liebl A, Henrichs HR, Heinemann L. et al. Continuous glucose monitoring working group of the working group diabetes technology of the German Diabetes Association, continuous glucose monitoring: evidence and consensus statement for clinical use. J Diabetes Sci Technol. 2013;7:500–19. doi: 10.1177/193229681300700227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Diabetes Research in Children Network (DirecNet) Study Group Youth and parent satisfaction with clinical use of the GlucoWatch G2 Biographer in the management of pediatric type 1 diabetes. Diabetes Care. 2005;28:1929–35. doi: 10.2337/diacare.28.8.1929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group, Validation of measures of satisfaction with and impact of continuous and conventional glucose monitoring. Diabetes Technol Ther. 2010;12:679–84. doi: 10.1089/dia.2010.0015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rebrin K, Steil GM, Van Antwerp WP, Mastrototaro JJ. Subcutaneous glucose predicts plasma glucose independent of insulin. Implications for continuous monitoring. Am J Physiol. 1999;277:E561–71. doi: 10.1152/ajpendo.1999.277.3.E561. [DOI] [PubMed] [Google Scholar]
- 38.Mauras N, Fox L, Englert K, Beck RW. Continuous glucose monitoring in type 1 diabetes. Endocrine. 2013;43:41–50. doi: 10.1007/s12020-012-9765-1. [DOI] [PubMed] [Google Scholar]
- 39.Vaddiraju S, Burgess DJ, Tomazos I. et al. Technologies for continuous glucose monitoring: current problems and future promises. J Diabetes Sci Technol. 2010;4:1540–62. doi: 10.1177/193229681000400632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Heinemann L, Schmelzeisen-Redeker G. Non-invasive continuous glucose monitoring in type 1 diabetic patients with optical glucose sensors. Diabetologia. 1998;41:848–54. doi: 10.1007/s001250050998. [DOI] [PubMed] [Google Scholar]
- 41.Pickup JC, Hussain F, Evans ND. et al. Fluorescence-based glucose sensors. Biosens Bioelectron. 2005;20:2555–65. doi: 10.1016/j.bios.2004.10.002. [DOI] [PubMed] [Google Scholar]
- 42.Pickup J, McCartney L, Rolinski O, Birch D. In vivo glucose sensing for diabetes management: Progress towards non-invasive monitoring. Br Med J. 1999;319:1289–93. doi: 10.1136/bmj.319.7220.1289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Heo YJ, Shibata H, Okitsu T. et al. Long-term in vivo glucose monitoring using fluorescent hydrogel fibers. Proc Natl Acad Sci U S A. 2011;108:13399–403. doi: 10.1073/pnas.1104954108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Moschou EA, Sharma BV, Deo SK, Daunert S. Fluorescence glucose detection: advances toward the ideal in vivo biosensor. J Fluoresc. 2004;14:535–47. doi: 10.1023/b:jofl.0000039341.64999.83. [DOI] [PubMed] [Google Scholar]
- 45.Linhares MC, Kissinger PT. Capillary ultrafiltration: in vivo sampling probes for small molecules. Anal Chem. 1992;64:2831–5. doi: 10.1021/ac00046a029. [DOI] [PubMed] [Google Scholar]
- 46.Chuang H, Taylor E, Davison TW. Clinical evaluation of a continuous minimally invasive glucose flux sensor placed over ultrasonically permeated skin. Diabetes Technol Ther. 2004;6:21–30. doi: 10.1089/152091504322783378. [DOI] [PubMed] [Google Scholar]
- 47.Garg SK, Potts RO, Ackerman NR. et al. Correlation of fingerstick blood glucose measurements with GlucoWatch biographer glucose results in young subjects with type 1 diabetes. Diabetes Care. 1999;22:1708–14. doi: 10.2337/diacare.22.10.1708. [DOI] [PubMed] [Google Scholar]
- 48.Tamada JA, Garg S, Jovanovic L. et al. Noninvasive Glucose Monitoring: Comprehensive Clinical Results. JAMA. 1999;282:1839–44. doi: 10.1001/jama.282.19.1839. [DOI] [PubMed] [Google Scholar]
- 49.Glikfeld P, Hinz RS, Guy RH. Noninvasive sampling of biological fluids by iontophoresis. Pharm Res. 1989;32:632–41. doi: 10.1023/a:1015957816254. [DOI] [PubMed] [Google Scholar]
- 50.Potts RO, Tamada JA, Tierney MJ. Glucose monitoring by reverse iontophoresis. Diabetes Metab Res Rev. 2002;18:S49–53. doi: 10.1002/dmrr.210. [DOI] [PubMed] [Google Scholar]
- 51.Rao G, Glikfeld P, Guy RH. Reverse iontophoresis: development of a noninvasive approach for glucose monitoring. Pharm Res. 1993;10:1751–5. doi: 10.1023/a:1018926215306. [DOI] [PubMed] [Google Scholar]
- 52.Tamada J, Bohannon N, Potts R. Measurement of glucose in diabetic subjects using noninvasive transdermal extraction. Nat Med. 1995;1:1198–201. doi: 10.1038/nm1195-1198. [DOI] [PubMed] [Google Scholar]
- 53.Bantle J, Thomas W. Glucose measurement in patients with diabetes mellitus with dermal interstitial fluid. J Lab Clin Med. 1997;130:436–41. doi: 10.1016/s0022-2143(97)90044-5. [DOI] [PubMed] [Google Scholar]
- 54.Service FJ, O’Brien PC, Wise SD. et al. Dermal interstitial glucose as an indicator of ambient glycemia. Diabetes Care. 1997;20:1426–9. doi: 10.2337/diacare.20.9.1426. [DOI] [PubMed] [Google Scholar]
- 55.Kost J, Mitragotri S, Gabbay R. et al. Non-invasive blood glucose measurement using ultrasound. Nat Med. 2000;6:347–50. doi: 10.1038/73213. [DOI] [PubMed] [Google Scholar]
- 56.Schaupp L, Ellmerer M, Brunner GA. et al. Direct access to interstitial fluid in adipose tissue in humans by use of open-flow microperfusion. Am J Physiol. 1999;276:E401–8. doi: 10.1152/ajpendo.1999.276.2.E401. [DOI] [PubMed] [Google Scholar]
- 57.Pfützner A, Caduff A, Larbig M, Schrepfer T, Forst T. Impact of posture and fixation technique on impedance spectroscopy used for continuous and noninvasive glucose monitoring. Diabetes Technol Ther. 2004;6:435–41. doi: 10.1089/1520915041705839. [DOI] [PubMed] [Google Scholar]
- 58.Caduff A, Dewarrat F, Talary M. et al. Non-invasive glucose monitoring in patients with diabetes: A novel system based on impedance spectroscopy. Biosens Bioelectron. 2006;22:598–604. doi: 10.1016/j.bios.2006.01.031. [DOI] [PubMed] [Google Scholar]
- 59.Rice MJ, Coursin DB. Continuous measurement of glucose: facts and challenges. Anesthesiology. 2012;116:199–204. doi: 10.1097/ALN.0b013e318236abf6. [DOI] [PubMed] [Google Scholar]
- 60.Wentholt IM, Vollebregt MA, Hart AA. et al. Comparison of a needle-type and a microdialysis continuous glucose monitor in type 1 diabetic patients. Diabetes Care. 2005;28:2871–6. doi: 10.2337/diacare.28.12.2871. [DOI] [PubMed] [Google Scholar]
- 61.Heller A, Feldman B. Electrochemical glucose sensors and their applications in diabetes management. Chem Rev. 2008;108:2482–505. doi: 10.1021/cr068069y. [DOI] [PubMed] [Google Scholar]
- 62.Ricci F, Caprio F, Poscia A. et al. Toward continuous glucose monitoring with planar modified biosensors and microdialysis. Biosens Bioelectron. 2007;22:2032–9. doi: 10.1016/j.bios.2006.08.041. [DOI] [PubMed] [Google Scholar]
- 63.Gerritsen M. Problems associated with subcutaneously implanted glucose sensors. Diabetes Care. 2000;23:143–5. doi: 10.2337/diacare.23.2.143. [DOI] [PubMed] [Google Scholar]
- 64.Rebrin K, Steil GM. Can interstitial glucose assessment replace blood glucose measurements? Diabetes Technol Ther. 2000;2:461–71. doi: 10.1089/15209150050194332. [DOI] [PubMed] [Google Scholar]
- 65. Clinical and Laboratory Standards Institute. Performance metrics for continuous interstitial glucose monitoring; approved guideline. POCT05-A Vol.28 No.33 2008.
- 66.Boyne MS, Silver DM, Kaplan J, Saudek CD. Timing of changes in interstitial and venous blood glucose measured with a continuous subcutaneous glucose sensor. Diabetes. 2003;52:2790–4. doi: 10.2337/diabetes.52.11.2790. [DOI] [PubMed] [Google Scholar]
- 67.Mazze R. Evaluating the accuracy, reliability, and clinical applicability of continuous glucose monitoring (CGM): is CGM ready for real time? Diabetes Technol Ther. 2009;1:11–8. doi: 10.1089/dia.2008.0041. [DOI] [PubMed] [Google Scholar]
- 68.Nichols SP, Koh A, Storm WL, Shin JH, Schoenfisch MH. Biocompatible materials for continuous glucose monitoring devices. Chem Rev. 2013;113:2528–49. doi: 10.1021/cr300387j. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Stout PJ, Racchini JR, Hilgers ME. A novel approach to mitigating the physiological lag between blood and interstitial fluid glucose measurements. Diabetes Technol Ther. 2004;6:635–44. doi: 10.1089/dia.2004.6.635. [DOI] [PubMed] [Google Scholar]
- 70.Schierenbeck F, Öwall A, Franco-Cereceda A, Liska J. Evaluation of a continuous blood glucose monitoring system using a central venous catheter with an integrated microdialysis function. Diabetes Technol Ther. 2013;15:26–31. doi: 10.1089/dia.2012.0169. [DOI] [PubMed] [Google Scholar]
- 71.Bird S, Macken L, Flower O. et al. Continuous arterial and venous glucose monitoring by quenched chemical fluorescence in ICU patients after cardiac surgery. Crit Care. 2013;17:P461. [PubMed] [Google Scholar]
- 72.Blixt C, Rooyackers O, Isaksson O, Wernerman J. Continuous on-line glucose measurement by microdialysis in a central vein. A pilot study. Crit Care. 2013;17:R87. doi: 10.1186/cc12713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Lucarelli F, Scuffi C, Mader JK. et al. Optimising the glucose sampling performance of an intravascular microdialysis-based Continuous Glucose Monitoring device for use in hospital settings. Diabetes Technol Ther. 2013;15:A13. doi: 10.1515/bmt-2013-4142. [DOI] [PubMed] [Google Scholar]
- 74.Mader JK, Feichtner F, Bock G. et al. Microdialysis—A versatile technology to perform metabolic monitoring in diabetes and critically ill patients. Diabetes Res Clin Pract. 2012;97:112–8. doi: 10.1016/j.diabres.2012.02.010. [DOI] [PubMed] [Google Scholar]
- 75.Bochicchio G, Joseph J, Magee M. et al. 219: Multicenter evaluation of a first generation automated blood glucose monitor in the OR/ICU. Crit Care Med. 2011;39:S55. [Google Scholar]
- 76.Jax T, Heise T, Nosek L. et al. Automated near-continuous glucose monitoring measured in plasma using mid-infrared spectroscopy. J Diabetes Sci Technol. 2011;5:345–52. doi: 10.1177/193229681100500222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Skjaervold NK, Solligård E, Hjelme DR, Aadahl P. Continuous measurement of blood glucose: validation of a new intravascular sensor. Anesthesiology. 2011;114:120–5. doi: 10.1097/ALN.0b013e3181ff4187. [DOI] [PubMed] [Google Scholar]
- 78.Thomé-Duret V, Reach G, Gangnerau MN. et al. Use of a subcutaneous glucose sensor to detect decreases in glucose concentration prior to observation in blood. Anal Chem. 1996;68:3822–6. doi: 10.1021/ac960069i. [DOI] [PubMed] [Google Scholar]
- 79.Schmidtke DW, Freeland AC, Heller A, Bonnecaze RT. Measurement and modeling of the transient difference between blood and subcutaneous glucose concentrations in the rat after injection of insulin. Proc Natl Acad Sci U S A. 1998;95:294–9. doi: 10.1073/pnas.95.1.294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Sternberg F, Meyerhoff C, Mennel FJ. et al. Subcutaneous glucose concentration in humans: real estimation and continuous monitoring. Diabetes Care. 1995;18:1266–9. doi: 10.2337/diacare.18.9.1266. [DOI] [PubMed] [Google Scholar]
- 81.Lönnroth P, Jansson PA, Smith U. A microdialysis method allowing characterization of intercellular water space in humans. J Am Physiol. 1987;253:E228–31. doi: 10.1152/ajpendo.1987.253.2.E228. [DOI] [PubMed] [Google Scholar]
- 82.Bolinder J, Hagström-Toft E, Ungerstedt U, Arner P. Self-monitoring of blood glucose in type I diabetic patients: comparison with continuous microdialysis measurements of glucose in subcutaneous adipose tissue during ordinary life conditions. Diabetes Care. 1997;20:64–70. doi: 10.2337/diacare.20.1.64. [DOI] [PubMed] [Google Scholar]
- 83.Kulcu E, Tamada JA, Reach G, Potts RO, Lesho MJ. Physiological differences between interstitial glucose and blood glucose measured in human subjects. Diabetes Care. 2003;26:2405–9. doi: 10.2337/diacare.26.8.2405. [DOI] [PubMed] [Google Scholar]
- 84.Caplin NJ, O’Leary P, Bulsara M. et al. Subcutaneous glucose sensor values closely parallel blood glucose during insulin-induced hypoglycemia. Diabet Med. 2003;20:238–41. doi: 10.1046/j.1464-5491.2003.00837.x. [DOI] [PubMed] [Google Scholar]
- 85.Jensen BM, Bjerring P, Christiansen JS, Orskov H. Glucose content in human skin: relationship with blood glucose levels. Scand J Clin Lab Invest. 1995;55:427–32. doi: 10.3109/00365519509104982. [DOI] [PubMed] [Google Scholar]
- 86.Keenan DB, Mastrototaro JJ, Voskanyan G, Steil GM. Delays in minimally invasive continuous glucose monitoring devices: a review of current technology. J Diabetes Sci Technol. 2009;3:1207–14. doi: 10.1177/193229680900300528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Steil GM, Rebrin K, Hariri F. et al. Interstitial fluid glucose dynamics during insulin-induced hypoglycemia. Diabetologia. 2005;48:1833–40. doi: 10.1007/s00125-005-1852-x. [DOI] [PubMed] [Google Scholar]
- 88.Davey RJ, Low C, Jones TW, Fournier PA. Contribution of an intrinsic lag of continuous glucose monitoring systems to differences in measured and actual glucose concentrations changing at variable rates in vitro. J Diabetes Sci Technol. 2010;4:1393–9. doi: 10.1177/193229681000400614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Jansson PA, Fowelin J, Smith U, Lonnroth P. Characterization by microdialysis of intracellular glucose level in subcutaneous tissue in humans. Am J Physiol. 1988;255:E218–20. doi: 10.1152/ajpendo.1988.255.2.E218. [DOI] [PubMed] [Google Scholar]
- 90.Sternberg F, Meyerhoff C, Mennel F. et al. Does fall in tissue glucose precede fall in blood glucose? Diabetologia. 1996;39:609–12. doi: 10.1007/BF00403309. [DOI] [PubMed] [Google Scholar]
- 91.Aussedat B, Dupire-Angel M, Gifford R. et al. Interstitial glucose concentration and glycemia: implications for continuous subcutaneous glucose monitoring. Am J Physiol Endocrinol Metab. 2000;278:E716–28. doi: 10.1152/ajpendo.2000.278.4.E716. [DOI] [PubMed] [Google Scholar]
- 92.Thennadil SN, Rennert JL, Wenzel BJ. et al. Comparison of glucose concentration in interstitial fluid, and capillary and venous blood during rapid changes in blood glucose levels. Diabetes Technol Ther. 2001;3:357–65. doi: 10.1089/15209150152607132. [DOI] [PubMed] [Google Scholar]
- 93.Petersen LJ, Kristensen JK. Bülow J, Microdialysis of the interstitial water space in human skin in vivo: quantitative measurement of cutaneous glucose concentrations. J Invest Dematol. 1992;99:357–60. doi: 10.1111/1523-1747.ep12616676. [DOI] [PubMed] [Google Scholar]
- 94.Lönnroth P, Jannson PA, Smith U. A microdialysis method allowing characterization of intracellular water space in humans. Am J Physiol. 1987;253:E228–31. doi: 10.1152/ajpendo.1987.253.2.E228. [DOI] [PubMed] [Google Scholar]
- 95.Petersen LJ. Interstitial lactate levels in human skin at rest and during an oral glucose load: a microdialysis study. Clin Physiol. 1999;19:246–50. doi: 10.1046/j.1365-2281.1999.00174.x. [DOI] [PubMed] [Google Scholar]
- 96.Summers LKM, Clark ML, Humphreys SM. et al. The use of microdialysis to monitor rapid changes in glucose concentration. Horm Metab Res. 1999;31:424–8. doi: 10.1055/s-2007-978767. [DOI] [PubMed] [Google Scholar]
- 97.Aussedat B, Thomé-Duret V, Reach G. et al. A user-friendly method for calibrating a subcutaneous glucose sensor-based hypoglycemic alarm. Biosens Bioelectron. 1997;12:1061–71. doi: 10.1016/s0956-5663(97)00083-3. [DOI] [PubMed] [Google Scholar]
- 98.Kerner W, Kiwit M, Linke B. et al. The function of a hydrogen peroxide-detecting electroenzymatic glucose electrode is markedly impaired in human sub-cutaneous tissue and plasma. Biosensor Bioelectron. 1993;8:473–82. doi: 10.1016/0956-5663(93)80032-k. [DOI] [PubMed] [Google Scholar]
- 99.Gerritsen M, Jansen JA, Kros A. et al. Performance of subcutaneously implanted glucose sensors: a review. J Invest Surg. 1998;11:163–74. doi: 10.3109/08941939809098031. [DOI] [PubMed] [Google Scholar]
- 100.Oliver NS, Toumazou C, Cass AE, Johnston DG. Glucose sensors: a review of current and emerging technology. Diabet Med. 2009;26:197–210. doi: 10.1111/j.1464-5491.2008.02642.x. [DOI] [PubMed] [Google Scholar]
- 101.Mou X, Lennartz M, Loegering DJ, Stenken JA. Long-term calibration considerations during subcutaneous microdialysis sampling in mobile rats. Biomaterials. 2010;31:4530–9. doi: 10.1016/j.biomaterials.2010.02.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Gerritsen M, Jansen JA, Kros A. et al. Influence of inflammatory cells and serum on the performance of implantable glucose sensors. J Biomed Mater Res. 2001;54:69–75. doi: 10.1002/1097-4636(200101)54:1<69::aid-jbm8>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 103.Ward WK. A review of the foreign-body response to subcutaneously-implanted devices: role of macrophages and cytokines in biofouling and fibrosis. J Diabetes Sci Technol. 2008;2:768–77. doi: 10.1177/193229680800200504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Anderson JM, Rodriguez A, Chang DT. Foreign body reaction to biomaterials. Semin Immunol. 2008;20:86–100. doi: 10.1016/j.smim.2007.11.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Wilson CJ, Clegg RE, Leavesley DI, Pearcy MJ. Mediation of biomaterial-cell interactions by adsorbed proteins: a review. Tissue Eng. 2005;11:1–18. doi: 10.1089/ten.2005.11.1. [DOI] [PubMed] [Google Scholar]
- 106.Sharkawy AA, Klitzman B, Truskey GA, Reichert WM. Engineering the tissue which encapsulates subcutaneous implants. I. Diffusion properties. J Biomed Mater Res. 1997;37:401–12. doi: 10.1002/(sici)1097-4636(19971205)37:3<401::aid-jbm11>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 107.Sharkawy AA, Klitzman B, Truskey GA, Reichert WM. Engineering the tissue which encapsulates subcutaneous implants. II. Plasma–tissue exchange properties. J Biomed Mater Res. 1998;40:586–97. doi: 10.1002/(sici)1097-4636(19980615)40:4<586::aid-jbm10>3.0.co;2-e. [DOI] [PubMed] [Google Scholar]
- 108.Sharkawy AA, Klitzman B, Truskey GA, Reichert WM. Engineering the tissue which encapsulates subcutaneous implants. III. Effective tissue response times. J Biomed Mater Res. 1998;40:598–605. doi: 10.1002/(sici)1097-4636(19980615)40:4<598::aid-jbm11>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 109.Mang A, Pill J, Gretz N. et al. Biocompatibility of an electrochemical sensor for continuous glucose monitoring in subcutaneous tissue. Diabetes Technol Ther. 2005;7:163–73. doi: 10.1089/dia.2005.7.163. [DOI] [PubMed] [Google Scholar]
- 110.Anderson JM. Biological responses to materials. Annu Rev Mater Res. 2001;31:81–110. [Google Scholar]
- 111.Updike SJ, Shults MC, Rhodes RK. et al. Enzymatic glucose sensors: improved long-term performance in vitro and in vivo. ASAIO J. 1994;40:157–63. [PubMed] [Google Scholar]
- 112.Gilligan BJ, Shults MC, Rhodes RK, Updike SJ. Evaluation of a subcutaneous glucose sensor out to 3 months in a dog model. Diabetes Care. 1994;17:882–7. doi: 10.2337/diacare.17.8.882. [DOI] [PubMed] [Google Scholar]
- 113.Sieminski AL, Gooch KJ. Biomaterial–microvasculature interactions. Biomaterials. 2000;21:2233–41. doi: 10.1016/s0142-9612(00)00149-6. [DOI] [PubMed] [Google Scholar]
- 114.Klueh U, Kaur M, Qiao Y, Kreutzer DL. Critical role of tissue mast cells in controlling long-term glucose sensor function in vivo. Biomaterials. 2010;16:4540–51. doi: 10.1016/j.biomaterials.2010.02.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Koschinsky T, Heinemann L. Sensors for glucose monitoring: technical and clinical aspects. Diabetes Metab Res Rev. 2001;17:113–23. doi: 10.1002/dmrr.188. [DOI] [PubMed] [Google Scholar]
- 116.Rebrin K, Fisher U, Hahn von Dorsche H. et al. Subcutaneous glucose monitoring by means of electrochemical sensors: Fiction or reality? J Biomed Eng. 1992;14:33–40. doi: 10.1016/0141-5425(92)90033-h. [DOI] [PubMed] [Google Scholar]
- 117.Ertefai S, Gough DA. Physiological preparation for studying the response of subcutaneously implanted glucose and oxygen sensors. J Biomed Eng. 1989;11:362–8. doi: 10.1016/0141-5425(89)90097-6. [DOI] [PubMed] [Google Scholar]
- 118.Kyrolaien M, Rigsby P, Eddy S, Vadgma P. Bio-/haemocompatibility: implications and outcomes for sensors. Acta Anaethesiol Scand Suppl. 1995;104:55–60. doi: 10.1111/j.1399-6576.1995.tb04255.x. [DOI] [PubMed] [Google Scholar]
- 119.Cengiz E, Tamborlane WV. A tale of two compartments: Interstitial versus blood glucose monitoring. Diabetes Technol Ther. 2009;11:S11–6. doi: 10.1089/dia.2009.0002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Reach G, Feijen J, Alcock S. BIOMED concerted action chemical sensors for in vivo monitoring. The biocompatibility issue. Biosens Bioelectron. 1994;9:21–8. [Google Scholar]
- 121.Woodward SC. How fibroblasts and giant cells encapsulate implants: considerations in design of glucose sensors. Diabetes Care. 1982;5:278–81. doi: 10.2337/diacare.5.3.278. [DOI] [PubMed] [Google Scholar]
- 122.Clark LC, Spokane RB, Homan MM. et al. Long-term stability of electroenzymatic glucose sensors implanted in mice. ASAIO J. 1988;34:259–65. [PubMed] [Google Scholar]
- 123.Zhao Q, Topham N, Anderson JM. et al. Foreign-body giant cells and polyurethane biostability: In vivo correlation of cell adhesion and surface cracking. J Biomed Mater Res. 1991;25:177–83. doi: 10.1002/jbm.820250205. [DOI] [PubMed] [Google Scholar]
- 124.Luttikhuizen DT, Harmsen MC, Luyn MJV. Cellular and molecular dynamics in the foreign body reaction. Tissue Eng. 2006;12:1955–70. doi: 10.1089/ten.2006.12.1955. [DOI] [PubMed] [Google Scholar]
- 125.Petrofsky JS. The effect of type-2-diabetes-related vascular endothelial dysfunction on skin physiology and activities of daily living. J Diabetes Sci Technol. 2011;5:657–67. doi: 10.1177/193229681100500319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Moussy F, Jakeway S, Harrison DJ, Rajotte RV. In vitro and in vivo performance and lifetime of perfluorinated ionomer-coated glucose sensors after high-temperature curing. Anal Chem. 1994;66:3882–8. doi: 10.1021/ac00094a007. [DOI] [PubMed] [Google Scholar]
- 127.Pfeiffer EF, Meyerhoff C, Bischof F. et al. On line continuous monitoring of subcutaneous tissue glucose is feasible by combining portable glucosensor with microdialysis. Horm Metab Res. 1993;25:121–4. doi: 10.1055/s-2007-1002057. [DOI] [PubMed] [Google Scholar]
- 128.Koudelka M, Rohner-Jeanrenaud F, Terrettaz J. et al. In vivo behaviour of hypodermically implanted microfabricated glucose sensors. Biosens Bioelectron. 1991;6:31–6. doi: 10.1016/0956-5663(91)85005-h. [DOI] [PubMed] [Google Scholar]
- 129.Ratner BD. A paradigm shift: biomaterials that heal. Polym Int. 2007;56:1183–5. [Google Scholar]
- 130.Gilligan BC, Shults M, Rhodes RK. et al. Feasibility of Continuous Long-Term Glucose Monitoring from a Subcutaneous Glucose Sensor in Humans. Diabetes Technol Ther. 2004;6:378–86. doi: 10.1089/152091504774198089. [DOI] [PubMed] [Google Scholar]
- 131.Von Recum AF, Park JB. Permanent percutaneous devices. Crit Rev Bioeng. 1981;5:37–77. [PubMed] [Google Scholar]
- 132.Jansen JA. Paquay YGCJ, van Der Waerden JPCM, Tissue reaction to soft-tissue anchored percutaneous implants in rabbits. J Biomed Mater Res. 1994;28:1047–54. doi: 10.1002/jbm.820280909. [DOI] [PubMed] [Google Scholar]
- 133.Wang C, Yu B, Knudsen B. et al. Synthesis and performance of novel hydrogels coatings for implantable glucose sensors. Biomacromolecules. 2008;9:561–7. doi: 10.1021/bm701102y. [DOI] [PubMed] [Google Scholar]
- 134.Vriesendorp TM, DeVries JH, Holleman F. et al. The use of two continuous glucose sensors during and after surgery. Diabetes Technol Ther. 2005;7:315–22. doi: 10.1089/dia.2005.7.315. [DOI] [PubMed] [Google Scholar]
- 135.Piper HG, Alexander JL, Shukla A. et al. Real-time continuous glucose monitoring in pediatric patients during and after cardiac surgery. Pediatrics. 2006;118:1176–84. doi: 10.1542/peds.2006-0347. [DOI] [PubMed] [Google Scholar]
- 136.Desachy A, Vuagnat AC, Ghazali AD. et al. Accuracy of bedside glucometry in critically ill patients: influence of clinical characteristics and perfusion index. Mayo Clin Proc. 2008;83:400–5. doi: 10.4065/83.4.400. [DOI] [PubMed] [Google Scholar]
- 137.González Alonso J. Human thermoregulation and the cardiovascular system. Exp Physiol. 2012;97:340–6. doi: 10.1113/expphysiol.2011.058701. [DOI] [PubMed] [Google Scholar]
- 138.Myrer JW, Measom G, Durrant E, Fellingham GW. Cold-and hot-pack contrast therapy: subcutaneous and intramuscular temperature change. J Athl Train. 1997;32:238–41. [PMC free article] [PubMed] [Google Scholar]
- 139.Fayolle C, Brun JF, Bringer J. et al. Accuracy of continuous subcutaneous glucose monitoring with the GlucoDay® in type 1 diabetic patients treated by subcutaneous insulin infusion during exercise of low versus high intensity. Diabetes Metab. 2006;32:313–20. doi: 10.1016/s1262-3636(07)70285-9. [DOI] [PubMed] [Google Scholar]
- 140.Iscoe KE, Campbell JE, Jamnik V. et al. Efficacy of continuous real-time blood glucose monitoring during and after prolonged high-intensity cycling exercise: spinning with a continuous glucose monitoring system. Diabetes Technol Ther. 2006;8:627–35. doi: 10.1089/dia.2006.8.627. [DOI] [PubMed] [Google Scholar]
- 141.Bequette BW. Continuous glucose monitoring: real-time algorithms for calibration, filtering, and alarms. J Diabetes Sci Technol. 2010;4:404–18. doi: 10.1177/193229681000400222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Voskanyan G, Keenan DB, Mastrototaro JJ, Steil GM. Putative delays in interstitial fluid (ISF) glucose kinetics can be attributed to the glucose sensing systems used to measure them rather than the delay in ISF glucose itself. J Diabetes Sci Technol. 2007;1:639–44. doi: 10.1177/193229680700100507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 143.Freeland AC, Bonnecaze RT. Inference of blood glucose concentrations from subcutaneous glucose concentrations: applications to glucose biosensors. Ann Biomed Eng. 1999;27:525–37. doi: 10.1114/1.196. [DOI] [PubMed] [Google Scholar]
- 144.Steil GM, Richey J, Kim JK. et al. Extracellular glucose distribution is not altered by insulin: analysis of plasma and interstitial L-glucose kinetics. Am J Physiol. 1996;271:E855–64. doi: 10.1152/ajpendo.1996.271.5.E855. [DOI] [PubMed] [Google Scholar]
- 145.Groenendaal W, Schmidt KA, von Basum G. et al. Modeling glucose and water dynamics in human skin. Diabetes Technol Ther. 2008;10:283–93. doi: 10.1089/dia.2007.0290. [DOI] [PubMed] [Google Scholar]
- 146.Feldman B, Brazg R, Schwartz S, Weinstein R. A continuous glucose sensor based on wired enzyme technology: results from a 3-day trial in patients with type 1 diabetes. Diabetes Technol Ther. 2003;5:769–79. doi: 10.1089/152091503322526978. [DOI] [PubMed] [Google Scholar]
- 147. Clinical and Laboratory Standards Institute, EN ISO 15197:2003 In vitro diagnostic test systems: Requirements for blood glucose monitoring systems for self-testing in managing diabetes mellitus.
- 148.Zueger T, Diem P, Mougiakakou S, Stettler C. Influence of time-point of calibration on accuracy of continuous glucose monitoring in individuals with type 1 diabetes. Diabetes Technol Ther. 2012;14:583–8. doi: 10.1089/dia.2011.0271. [DOI] [PubMed] [Google Scholar]
- 149.Buckingham BA, Kollman C, Beck R. et al. Evaluation of factors affecting CGMS calibration. Diabetes Technol Ther. 2006;8:318–25. doi: 10.1089/dia.2006.8.318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Feldman BJ, McGarraugh GV. United States Patent US; 2007. Nov 20, Method of calibrating an analyte-measurement device, and associated methods, devices and systems. 7,299,082 B2. [Google Scholar]
- 151.Goode PV, Brauker JH, Kamath AU. United States Patent US; System and methods for processing analyte sensor data. 6,931,327 B2 2005 Aug 16. [Google Scholar]
- 152.King C, Anderson SM, Breton M. et al. Modeling of calibration effectiveness and blood-to-interstitial glucose dynamics as potential counfounders of the accuracy of continuous glucose sensors during hyperinsulinemic clamp. J Diabetes Sci Technol. 2007;1:317–22. doi: 10.1901/jaba.2007.1-317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Shiavi R. 3rd ed. Burlington, MA: Elsevier/Academic Press; 2007. Introduction to applied statistical signal analysis: Guide to biomedical and electrical engineering applications. [Google Scholar]
- 154.Panteleon AE, Rebrin K, Steil GM. The role of the independent variable to glucose sensor calibration. Diabetes Technol Ther. 2003;5:401–10. doi: 10.1089/152091503765691901. [DOI] [PubMed] [Google Scholar]
- 155.Facchinetti A, Sparacino G, Cobelli C. Reconstruction of glucose in plasma from interstitial fluid continuous glucose monitoring data: role of sensor calibration. J Diabetes Sci Technol. 2007;1:617–23. doi: 10.1177/193229680700100504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Helton KL, Ratner BD, Wisniewski NA. Biomechanics of the sensor–tissue interface—effects of motion, pressure and design on sensor performance and the foreign body response—part I: theoretical framework. J Diabetes Sci Technol. 2011;5:632–46. doi: 10.1177/193229681100500317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 157.Ward WK, Casey HM, Quinn MJ. et al. A fully implantable subcutaneous glucose sensor array: enhanced accuracy from multiple sensing units and a median-based algorithm. Diabetes Technol Ther. 2003;5:943–52. doi: 10.1089/152091503322640980. [DOI] [PubMed] [Google Scholar]
- 158.Castle JR, Ward WK. Amperometric glucose sensors: sources of error and potential benefit of redundancy. J Diabetes Sci Technol. 2010;4:221–5. doi: 10.1177/193229681000400127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 159.Kosiborod M, Gottlieb R, Sekella J. et al. Performance of the Medtronic Sentrino continuous glucose management system in the cardiac ICU. Crit Care. 2013;17:P462. doi: 10.1136/bmjdrc-2014-000037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160. Medtronic Press Release, December 3, 2012 Avaialble at: http://newsroom.medtronic.com/phoenix.zhtml?c=251324&p=irol-newsArticle&ID=1772458&highlight= (accessed 25 March 2014)
- 161.Saha R, Kristensen JS, Wolfe KT, United States Patent US; Orthogonally Redundant Sensor Systems and Methods. 20130060105 A1 7 March 2013. [Google Scholar]
- 162.Ward WK. A review of the foreign-body response to subcutaneously-implanted devices: the role of macrophages and cytokines in biofouling and fibrosis. J Diabetes Sci Technol. 2008;2:768–77. doi: 10.1177/193229680800200504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 163.Scuffi C, Lucarelli F, Valgimigli F. Minimizing the impact of time lag variability on accuracy evaluation of continuous glucose monitoring systems. J Diabetes Sci Technol. 2012;6:1383–91. doi: 10.1177/193229681200600618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 164.Kovatchev BP, Shields D, Breton M. Graphical and numerical evaluation of continuous glucose sensing time lag. Diabetes Technol Ther. 2009;11:139–43. doi: 10.1089/dia.2008.0044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 165.Molnár GA, Boros AG, Pótó L. et al. The Poincaré plot, but not the correlation R value, is a good marker of temporal variability of CGMS data. Diabetes Technol Ther. 2008;10:506–7. doi: 10.1089/dia.2007.0301. [DOI] [PubMed] [Google Scholar]
- 166.Kovatchev BP, Gonder-Frederick LA, Cox DJ, Clarke WL. Evaluating the accuracy of continuous glucose-monitoring sensors. Diabetes Care. 2004;27:1922–8. doi: 10.2337/diacare.27.8.1922. [DOI] [PubMed] [Google Scholar]
- 167.Clarke WL, Cox D, Gonder-Frederick LA. et al. Evaluating clinical accuracy of systems for self-monitoring of blood glucose. Diabetes Care. 1987;10:622–8. doi: 10.2337/diacare.10.5.622. [DOI] [PubMed] [Google Scholar]
- 168.Lucarelli F, Ricci F, Caprio F. et al. GlucoMenDay Continuous Glucose Monitoring System: a screening for enzymatic and electrochemical interferents. J Diabetes Sci Technol. 2012;6:1172–81. doi: 10.1177/193229681200600522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 169.Shichiri M, Asakawa N, Yamasaki Y. et al. Telemetry glucose monitoring device with needle-type glucose sensor: a useful tool for blood glucose monitoring in diabetic individuals. Diabetes Care. 1986;9:298–301. doi: 10.2337/diacare.9.3.298. [DOI] [PubMed] [Google Scholar]
- 170.Matthews D, Brown E, Beck T. et al. An amperometric needle-type sensor tested in rats and man. Diabet Med. 1988;5:248–52. doi: 10.1111/j.1464-5491.1988.tb00978.x. [DOI] [PubMed] [Google Scholar]
- 171.Aalders A, Schmidt F, Schoonen A. et al. Development of a wearable glucose sensor; studies in healthy volunteers and in diabetic patients. Int J Artif Organs. 1991;14:102–8. [PubMed] [Google Scholar]
- 172.Meyerhoff C, Bischof F, Sternberg F. et al. On line continuous monitoring of subcutaneous tissue glucose in men by combining portable glucosensor with microdialysis. Diabetologia. 1992;35:1087–92. doi: 10.1007/BF02221686. [DOI] [PubMed] [Google Scholar]
- 173.Smith A, Yang D, Delcher H. et al. Fluorescein kinetics in interstitial fluid harvested from diabetic skin during fluoroscein angiography: implications for glucose monitoring. Diabetes Technol Ther. 1999;1:21–7. doi: 10.1089/152091599317530. [DOI] [PubMed] [Google Scholar]
- 174.Gross T, Bode B, Einhorn D. et al. Performance evaluation of the MiniMed Continuous glucose monitoring system during patient home use. Diabetes Technol Ther. 2000;2:49–59. doi: 10.1089/152091500316737. [DOI] [PubMed] [Google Scholar]
- 175.Varalli M, Marelli G, Maran A. et al. A microdialysis technique for continuous subcutaneous glucose monitoring in diabetic patients (part 2) Biosens Bioelectron. 2003;18:899–905. doi: 10.1016/s0956-5663(02)00215-4. [DOI] [PubMed] [Google Scholar]
- 176.Weinstein RL, Schwartz SL, Bragz RL. et al. Accuracy of the 5-day FreeStyle Navigator continuous glucose monitoring system: comparison with frequent laboratory reference measurements. Diabetes Care. 2007;30:1125–30. doi: 10.2337/dc06-1602. [DOI] [PubMed] [Google Scholar]
- 177.Wentholt IM, Hart AA, Hoekstra JB, Devries JH. Relationship beteween interstitial and blood glucose in type 1 diabetes patients: delay and the push-pull phenomenon revisited. Diabetes Technol Ther. 2007;9:169–75. doi: 10.1089/dia.2006.0007. [DOI] [PubMed] [Google Scholar]
- 178.Kamath A, Mahalingam A, Brauker J. Analysis of Time Lags and Other Sources of Error of the DexCom SEVEN Continuous Glucose Monitor. Diabetes Technol Ther. 2009;11:689–95. doi: 10.1089/dia.2009.0060. [DOI] [PubMed] [Google Scholar]
- 179.Bailey T, Zisser H, Chang A. New features and performance of a next-generation SEVEN-Day continuous glucose monitoring system with short lag time. Diabetes Technol Ther. 2009;11:749–55. doi: 10.1089/dia.2009.0075. [DOI] [PubMed] [Google Scholar]
- 180.Garg SK, Smith J, Beatson C. et al. Comparison of accuracy and safety of the SEVEN and the navigator continuous glucose monitoring systems. Diabetes Technol Ther. 2009;11:65–72. doi: 10.1089/dia.2008.0109. [DOI] [PubMed] [Google Scholar]
- 181.Valgimigli F, Lucarelli F, Scuffi C. et al. Evaluating the clinical accuracy of GlucoMenDay: a novel microdialysis-based continuous glucose monitor. J Diabetes Sci Technol. 2010;4:1182–92. doi: 10.1177/193229681000400517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 182.McGarraugh G, Brazg R, Richard W. FreeStyle navigator continuous glucose monitoring system with trustart algorithm, a 1-hour warm-up time. J Diabetes Sci Technol. 2011;5:99–106. doi: 10.1177/193229681100500114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 183.Ward WK, Engle JM, Brenigan D. et al. The effect of rising vs. falling glucose level on amperometric glucose sensor lag and accuracy in Type 1 diabetes. Diabet Med. 2012;29:1067–73. doi: 10.1111/j.1464-5491.2011.03545.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 184.Keenan DB, Mastrototaro JJ, Zisser H. et al. Accuracy of the Enlite 6-day glucose sensor with Guardian and Veo calibration algorithms. Diabetes Technol Ther. 2012;14(225):31. doi: 10.1089/dia.2011.0199. [DOI] [PubMed] [Google Scholar]