

Abstract
OBJECTIVES:
This study aimed to find the prevalence of Hypodontia and Hyperdontia in different ethnicities in patients from 7 to 14 years old.
MATERIAL AND METHODS:
A group of 520 children were included aged 7 to 14 years, only the children who went to primary schools. Controls were performed by professional people to preserve the criteria of orthodontic abnormalities evaluation. The data were recorded in the individual card specially formulated for this research and all the patients suspected for hypodontia and hyperdontia the orthopantomography for confirmation was made. The data were analysed using descriptive statistical analysis using χ2 test for the significant difference for p ˂ 0.05 and Fisher test for p < 0.05.
RESULTS:
Hypodontia, not counting the patients with missing third molars was found in 18 patients researched or 3.46%. The most commonly missing teeth were the second lower premolars, the second upper premolars, second upper lateral incisors followed by the lower incisors. Hyperdontia not including the third molars was found in 4 cases of the participants or 0.76% from which the most frequent atypical tooth mesiodens and one case of bilateral hypodontia of a lateral upper incisor with typical shape and size. But there were no significant differences when tested between genders and jaws.
CONCLUSION:
The prevalence we found is similar to the prevalence in the region. Our findings indicate that there is a difference between the genders in the prevalence of hypodontia, but without statistical significance, while for hyperdontia we can’t see such a difference between the sexes.
Keywords: Hypodontia, Hyperdontia, ethnics, children
Introduction
Hypodontia and hypodontia are particular dental anomalies, they are known as number dental anomalies. Hypodontia is best defined as agenesis of one or more teeth [1] and considered to be one of the most frequently encountered oral alterations [2] [3] Agenesis of teeth can be classified as hypodontia, oligodontia or anodontia. The term hypodontia is used to describe the agenesis of one or six teeth (excluding third molars), oligodontia shows the absence of more than six teeth and anodontia represents total lack of teeth [4]. Congenital absence of teeth or hypodontia is one of the most common abnormalities in tooth development in human beings. The prevalence of hypodontia varies from 2.63% to 11.2% depending on the race [5] [6] [7].
Many authors have used similar methods of classifying the congenital absence of teeth. In general, they identify three categories of hypodontia, excluding third molars, as follows: mild with 1 or 2 missing teeth, moderate with 3-5 and severe more than 5 missing teeth [8]. Thus, hypodontia can occur either as part of a syndromic or as a non-syndromic patient, familiar form; in the latter, it occurs as an isolated trait, affects variable numbers of teeth and appears either sporadically or as an inherited condition within a family pedigree [9]. Dental anomaly reported in patients with hypodontia is a conical form of lateral incisors, defects in the enamel development and transposition of lateral incisor and canine [10] [11].
For many years the dental anthropologists have researched the evolution of human teeth. All agree that the development in food processing from prehistory until modern times reflects in the morphological changes in human masticator space. By reducing the level of physiological teeth friction, well documented over evolution which today is completed because eating habits are stable, some authors believe in their useful effect related to dental arch; less density fewer impactions in the third molar and large stable occlusion [12] [13].
Clinicians often believe that the teeth agenesis is increasing me the recent decades. But again there is no evidence that this trend is true for the human dentition or it is purely a hypothetical observation, and it can be described under the examination and diagnostics of dental anomalies. The new genetic researchers show new fascinating horizons in this field, aiming at explaining the mystery of agenesis of the tooth, dental embryology and fetal development. The family lacks teeth were described in a research done by Arts and Vastardis [3] [4]. These anomalies are autosome dominant mutations of MSX1 gene in chromosome 4p (the short side).
Other studies indicate that hypodontia is different compared to deciduous and permanent teeth, tooth type, by gender and racial group. Early research shows that the prevalence of hypodontia is higher in patients that are relative compared to the general population. It also affects both dentitions [14]. In the deciduous dentition, it varies from 0.5-0.9% while oligodontia is rare with a prevalence of 0.25% [3]. Some authors show a higher prevalence among women hypodontia [15] [16] [17], but there are studies that found no statistically significant difference between genders [18] [19] [20]. In the deciduous dentition the anomaly is rare, and most often it appears in the upper jaw compared to the lower jaw, most often the upper lateral incisors are rarely missing the central and lateral lower incisor. Lack of central incisors, canine and deciduous molar are a rare occurrence and are most often as a symptom of ectoderm dysplasia.
In the permanent dentition, the most commonly missing teeth are the third molars, followed by the second lower premolars, upper lateral incisors [21] [22]. The following differences present the prevalence between racial groups: 1.5-3% for the white race, 6-9.2% for the oriental race and 7.7% for the African-Americans [3]. Other dental anomalies have been reported in patients with hypodontia such as defects in developing [23] and transposition of lateral with canine [9].
In the literature, there are few data for hyperdontia compared to the hypodontia in every aspect of these phenomena.
Hyperdontia is defined as an increase in the number of teeth in dental arches in the deciduous or permanent dentition. Morphological appearance of hypodontia teeth varies from those similar with the normal teeth (supplementary) to the teeth with a form that is not normal (atypical).
Although presented in both dentitions it is most often found in the permanent dentition, where the frequency ranges 0.2-0.9%. In the deciduous dentition, the hypertonic teeth are in the upper jaw with the most frequent involvement of lateral incisor. In the permanent teeth, the frequency ranges from 0.1-3.6% in the population, from the typical tooth most often the second lateral upper incisor, the third premolar and the fourth molar. Hyperdontia of the permanent canine of the upper jaw are characteristics of the orofacial digital syndrome, while the hyperdontia of the lower canine is a characteristic for dysostosis cleidocranial.
From the atypical hyperdontic teeth which in general are found in the permanent dentition, most often appear as atypical tooth localised in between or in the location of central upper incisors-mesiodens.
This study aimed to find the prevalence of Hypodontia and Hyperdontia in different ethnicities in patients from 7 to 14 years old.
Material and Methods
Subjects
In our research 520 children were included aged 7 to 14 years. We included children from town those who went to primary schools with classes in Macedonian, Albanian and Turkish language, with a total number of 364 children or 70.68% from the total number of children examined in the town of Gostivar. In rural areas, we involved primary schools from the village Cigllana and schools in the village Vrapcishte with classes in Macedonian, Albanian and Turkish language, with a total number of 156 pupils from rural areas or 29.32% of the total number of children involved. Controls were performed by professional people to preserve the criteria of orthodontic abnormalities evaluation. Detection of orthodontic anomalies was performed by the same criteria in the assessment of the existence of hypodontia or hyperdontia in all children examined. It should also be noted that all the data were recorded in the individual card specially formulated for this research, which was done by the same examiners, all to avoid possible errors that may appear during the gathering, sorting, statistical processing and interpretation of results.
Data Collection
In all those cases where the data of the anamnesis has shown that there was no extraction of the appropriate tooth, those patients were separated for further research regarding verifying whether it was an extraction performed as told by the parent’s anamnesis, and in all the patients the orthopantomography were made. Only then the patients were registered as hypodontia or hyperdontia. The exams was conducted in classes, where the patients were seated and examined with dental mirrors, and dental probes and OJ and OB measurement was performed with Korkhause kit, for each pupil we took 5 pictures with a digital camera of which 2 extra oral in profile and frontal plane and 3 intraoral the left side, right and front in occlusion for verification and the complete documentation. In our study, the third molars were not included from the fact that their mineralisation and visibility in the OPT recordings is delayed even after 12-13 years of age.
Data Analysis
The data obtained from systematic orthodontic controls after they were organised and systemized in the database, they were analysed using descriptive statistical analysis using χ2 test for the significant difference for p ˂ 0.05 and Fisher test for p < 0.05.
Ethics
All the protocols and data used in this research were approved by the Ethical Board.
Results
Hypodontia, not counting the patients with missing third molars was found in 18 patients researched or 3.46% as shown in the table below. This lack of the number of the teeth was more common in the female children 65.7%, while the male children with 34.3% in the upper jaw, compared to the lower jaw were the presence was 63.5% versus 36.5% (F vs M). The most commonly missing teeth were the second lower premolars, the second upper premolars, second upper lateral incisors followed by the lower incisors.
In table 2 it is noted that from the total number of anomalies, in the missing number of teeth there has been a difference between men and women, in the upper jaw (34.3: 65.7%) and the lower jaw (36.5: 63.5%). Using the Fisher’s test we found no statistical significance for p ˂ 0.05.
Table 2.
Hypodontia according to the gender
| N | N | M/Max | F/Max | M/Mand | F/Mand |
|---|---|---|---|---|---|
| 520 | 18 | 6 | 12 | 7 | 11 |
| % | 100% | 34.30% | 65.70% | 36.50% | 63.50% |
Fisher Test, p = 0.74.
Table 1.
Hypodontia percentage
| Hypodontia | Row total | |
| Count | No | 502 |
| Percentage | 96.54% | |
| Count | Yes | 18 |
| Percentage | 3.46% | |
| Count | all Groups | 520 |
Pearsons Chi-square 1.99 df=1, p=16.
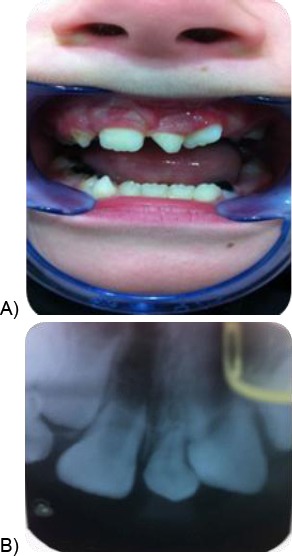
A patient with hypodontia is shown in Fig. 1 also a radiographic picture in the 2nd one where we can see all the missing teeth. While in the Fig. 2 is a patient with missing central incisor and his radiography.
Figure 1.
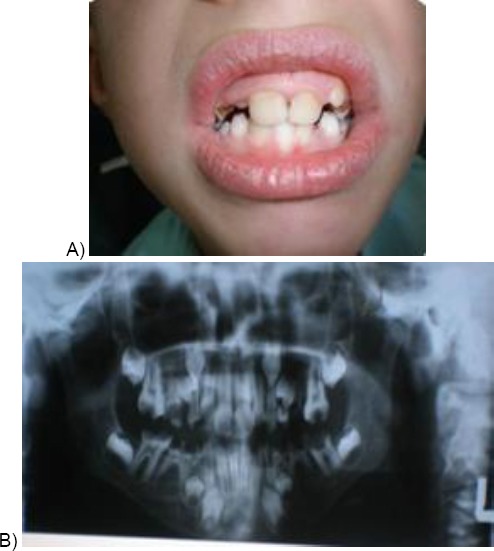
A) A case with hypodontia; B) A case with hypodontia of second upper and lower premolars
Figure 2.

A case with hypodontia of the lower central left incisor
Hyperdontia not including the third molars was found in 4 cases of the participants or 0.76% from which the most frequent atypical tooth mesiodens and one case of bilateral hypodontia of a lateral upper incisor with typical shape and size.
From the total of 520 examined, four examined (0.76%) had hyperdontia. In 516 cases (99.24%) there were no hyperdontia diagnosed which are shown in Table 3.
Table 3.
Hyperdontia percentage
| Hyperdontia | Row total | |
|---|---|---|
| Count | No | 516 |
| Percentage | 99.24% | |
| Count | Yes | 4 |
| Percentage | 0.76% | |
| Count | all Groups | 520 |
Pearsons Chi-square 0.16, df = 1, p = 0.69
In the statistical test we found χ2 = 0.16 and p > 0.05 (p = 0.69), so there was no significant difference. Table 4 shows that from the total number of anomalies, in the hyperdontic we found no difference between the genders and jaws regarding statistical validity for p < 0.05.
Table 4.
Hyperdontia according to the gender
| N | N | M/Max | F/Max | M/Mand | F/Mand |
|---|---|---|---|---|---|
| 520 | 4 | 2 | 1 | 1 | 0 |
| % | 100% | 66.7% | 33.3% | 100% | 0 |
Fisher Test, p = 1.
In Fig. 3A we see a patient with hyperdontic teeth, atypical tooth called mesiodens and in Fig. 3B his radiography. While in Fig. 4 is a patient with hyperdontia of 2 upper lateral incisors.
Figure 3.
A case with mesiodens
Figure 4.

A case with hyperdontia of two upper lateral incisors
Discussion
These results are best compared with the results shown in the bottom table (Table 5) in which we see the prevalence of hypodontia and hyperdontia from different researchers.
Table 5.
Authors and hypodontia and hyperdontia percentage
| Authors | Place | Years | No. investigated | Years | Hypodontia % | Common missing tooth | Hyper-don’t % |
|---|---|---|---|---|---|---|---|
| Davis | China | 1987 | 1093 | 12 | 6.9 | mandibular incisors | 2.7 |
| Nik-Hussein | Malasia | 1989 | 5.15 | 2.8 | 12,22 | x | |
| Renkerova et al. | Cekoslovakia | 1989 | 4405 | 7.12 | 4 | X | x |
| Lo Muzio et al. | Italia | 1989 | 1529 | 7.14 | 5.2 | second premolar | x |
| Ignelzi et al. | USA | 1989 | 849 | 3.9 | 7.8 | X | 2.4 |
| Jangida Moris | Japan | 1990 | 4009 | 2.29 | 7.8 | second premolar | 3 |
| Dechkunakorn et al. | Tailand | 1990 | 1160 | 6.15 | 8.6 | 12,22 | x |
| Legovid et al. | Yugslavia | 1990 | 2401 | 6.18 | 6.3 | X | 1.4 |
| Amini et al. | Iran | 1999 | 3374 | x | x | X | 0.7 |
| Locht | Danmark | 1980 | 704 | 9.1 | 7.7 | X | 1.7 |
| O’Dowling | Ireland | 1990 | 3056 | X | 11.3 | X | X |
| Al-emran | Saudi Arabia | 1990 | 500 | 13.5-14.5 | 4 | 35,45 | X |
| Lynham | Australia | 1990 | 662 | 16.26 | 6.3 | 15,25 | X |
| Aaskeim Ogard | Norvegia | 1993 | 1953 | 9 | 6.5 | 35,45 | X |
| Sterzik et al. | Germany | 1994 | 3238 | X | 8.1 | X | X |
In the Table 5 we can see obvious differences between authors Davis, Nik Hussein, Renkerova and Lo Muzio, where the frequency of hypodontia ranges from 2.8-6.9%, depending on the authors and countries where surveys are conducted and also a different age groups with differences from over 5 years to 12 years [24] [25] [26] [27].
We also see that depending on the type of hypodontia teeth there is a discrepancy between the majority of the authors divided into 3 respectively 2 large groups. According to one group [25] [28] hypodontia is more common in the upper lateral incisive, while according to another group [29] [30] [31] which are also similar to our findings that show that the most missing teeth are the second lower premolars after those the upper premolars represented with 6.5% respectively 6.3%.
Hyperdontia was found in a much lower percentage 0.76% but not in all the researches done, but in the most researches, the results are similar or same. Even our results for hyperdontia are similar to different authors [32].
When it comes to hyperdontia between different authors, there is a harmony according to their results the majority of them state that the first upper lateral incisive are the most common hyperdontic (from the typical teeth), respectively mesiodens from those with atypical form.
The data from the present study and their comparison with other studies [33] [34] [35] [36] [37] [38] shows that the prevalence of Hyperdontia and Hyperdontia is found in different frequencies in many countries of the world and even within the same country among different ethnic or regional groups.
According to a study by Ghabanchi et al. in Iran, missing of wisdom teeth accounted for 7% prevalence, this was generally lower than those from other population groups [33]. The prevalence of hypodontia according to Deniz et al. in Turkish population was 5% [34] and in a study by Hunstadbraten et al. in the Norwegian population the prevalence was 10.1%. [35] The frequency of hypodontia among the Swedish subjects in the Josefsson et al. study was 5.5 percent [36].
The prevalence of the hyperdoncia was 2.4% [33] according to Ghabanchi. In Onyeaso’s study in Nigeria showed a higher prevalence of hyperdontia with 14% [37]. A study from Schmuckli et al. shows a prevalence of 1.5% of hyperdontia in Swiss population [38].
Regarding the way that the creation of disorders of teeth number anomaly almost all authors put the genetic factors as the first in line. Other genetic defects and the influence of ambient factors play an important role in the distinctiveness of expressiveness of phenotype in the anomaly. Researchers show that hypodontia differs about milk and permanent teeth, tooth type, gender and racial groups. In milk dentition, the prevalence of hypodontia varies from 0.05-0.9%, whereas oligodontia is rare with a prevalence of 0.25% [3]. Some authors show the prevalence of hypodontia is higher in females [16] [17], but there are studies where no significant difference was found between genders [18] [19] [20]. In milk dentition, it is a rare anomaly, and often it appears in the upper jaw about the lower jaw, and it is often the upper lateral incisive missing and less the lateral and central lower incisors. In the permanent dentition excluding the third molars, the main tooth missing was the lower second premolars or the second upper incisor [21] [22]. Other differences were found in the prevalence between racial groups 1.5-3% for the white race, 6 to 9.2% for orientalists and 7.7% for African American [3].
When it comes to the anomaly of supper number of teeth, morphological appearance of hypodontia teeth is different. It is present in the deciduous and permanent dentition, but it is most frequent in the permanent dentition with a frequency varying from 0.2 to 1.9%. In the deciduous teeth, hypodontia is more frequent in the upper jaw, where the most common tooth is the lateral deciduous incisor. Hypodontia is a common anomaly in different populations. The highest prevalence is found in the Irish population, O’Dowlling, McNamara 1900 investigated 3056 patients where they found 11.3% of cases with hypodontia [39].
In our research female represent e high prevalence of hypodontia, these data are similar compared to other research [40]. Hyperdontia also has different prevalence in different populations, and that a lower prevalence in the Iranian population. Amini et al. in 1999 they examined 3374 participants where the hyperdontia prevalence was 0.7%, while the highest was found in Chinese children Devis 1987 in 1093 patients examined found 2.7% cases with hyperdontia and it most often affected the lower jaw incisors [41] [42].
Our research has shown a higher frequency in the absence of teeth of the second lower premolars, the second upper premolars, second upper incisor followed by the second lower incisor. In different researchers, we found different missing teeth, not including the third molars, but there is compliance between the authors. The most frequent missing dental follicles in a research done in children in Iran [43] were the lower second premolars, in a research in Chinese children the most frequent was the lower incisors missing, in Japanese, Italian, Austrian and Norwegian children the most frequent missing teeth were the upper and lower second premolars [27].
In our research, although we see differences between the sexes, there was no significant difference when we compared the means, although many authors show a difference in the prevalence of hypodontia in between the gender [44].
In conclusion, our findings for the prevalence of hypodontia are in average values within 3.46% compared with data from the literature. It is found, and it is evident that the prevalence of hypodontia compared to hyperdontia indicates a significant difference and is much higher (3.46%: 0.76%). Our findings indicate that there is a difference between the genders in the prevalence of hypodontia, but without statistical significance, while for hyperdontia we can’t see such a difference between the sexes. From the total number of teeth, the most often hypodontia tooth was the second lower premolar, upper second premolar and after it the lateral upper incisor. The most hyperdontic tooth was found to be the upper lateral incisor from the typical type while from the atypical type mesiodens.
A more comprehensive study should be made including more regions to investigate these anomalies, in different families especially those in special vulnerable areas so we can achieve the connectivity of those with the etiological factor so that the anomaly can be foreseen and diagnostic and treatment can be done in time.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Jorgenson RJ. Clincinas view of hypdontia J. Am Dent Assoc. 1980;101:283–286. doi: 10.14219/jada.archive.1980.0186. https://doi.org/10.14219/jada.archive.1980.0186. [DOI] [PubMed] [Google Scholar]
- 2.Wei SHY. Pediatric dentistry total patient care lex and Febiger Philadelphia. 1988:362–365. [Google Scholar]
- 3.Vastardis H. The genetics of human tooth agenesis:new discoveries for understanding dental anomalies. American Journal of Orthodontics Dentofacial Orthopedics. 2000;117(6):650–6. https://doi.org/10.1016/S0889-5406(00)70173-9. [PubMed] [Google Scholar]
- 4.Arte S. Phenotipic and Genotipic features of familial hypodontia Thesis University of Helsinki. 2001 [Google Scholar]
- 5.Sisman Y, Uysal T, Gelgor JE. Hypodontia does the prevalence snd distribution pattern differ in Orthodontic patients. Eur J Dent. 2007;1(3):167–173. PMid:19212561 PMCid:PMC2638243. [PMC free article] [PubMed] [Google Scholar]
- 6.Polder BJ, Vant Hof MA, Van der Linden FP, Kuijpers-Jagtman AM. A meta analysis of prevalence of dental agenesis of permanent teeth. Community Dent Oral Epidemiol. 2004;32(3):217–226. doi: 10.1111/j.1600-0528.2004.00158.x. https://doi.org/10.1111/j.1600-0528.2004.00158.x PMid:15151692. [DOI] [PubMed] [Google Scholar]
- 7.Chuny CJ, Han JH, Kim KH. The pattern and prevalence of hypodontia in Koreans. Oral Dis. 2008;(7):620–625. doi: 10.1111/j.1601-0825.2007.01434.x. https://doi.org/10.1111/j.1601-0825.2007.01434.x PMid:18248591. [DOI] [PubMed] [Google Scholar]
- 8.Brook AH, Elcock C, Al-Sharood MH, McKeown HF, Khalaf K, Smith RN. Further studies of a model for the etiology of anomalies of tooth number and size in humans. Connective tissue research. 2002;43(2-3):289–95. doi: 10.1080/03008200290000718. https://doi.org/10.1080/03008200290000718 PMid:12489172. [DOI] [PubMed] [Google Scholar]
- 9.Pemberton TJ, Das PI, Patel PI. Hypodontia genetics and future perspectives. Brasilian Journal of oral sciences. 2005;4:95–706. [Google Scholar]
- 10.Peck S, Peck L, Kataja M. Mandibular lateral incisor –canine transposition concomitant dental anomalies, and genetic control. Angle Orthodontist. 1998;68:455–466. doi: 10.1043/0003-3219(1998)068<0455:MLICTC>2.3.CO;2. PMid:9770104. [DOI] [PubMed] [Google Scholar]
- 11.Shapira Y, Kuftinec MM. Maxillary tooth transposition characteristics features and accompanying dental anomalies. Amer J of Orthodontics and dentofacial orthopedics. 2001;119:127–134. doi: 10.1067/mod.2001.111223. https://doi.org/10.1067/mod.2001.111223 PMid:11174558. [DOI] [PubMed] [Google Scholar]
- 12.Sengupta A, Whittaker DK, Barber G, Rogers J, Musgrave JH. The effects of dental wear on third molar eruption and on the curve of Spee in human rchaeological dentitions. Arch Oral Biol. 1999;44:925–934. doi: 10.1016/s0003-9969(99)00095-3. https://doi.org/10.1016/S0003-9969(99)00095-3. [DOI] [PubMed] [Google Scholar]
- 13.Begg RP. 1954. Stone age man's dentition:with reference to anatomically correct occlusion, the etiology of malocclusion, and a technique for its treatment. Am J Orthod. 1954;40:298–312. 373-383; 462-475; 517-531. https://doi.org/10.1016/0002-9416(54)90092-5. [Google Scholar]
- 14.Chosack A, Eidelman E, Cohen T. Hypodontia a polygene trait, a family study among Israelijews. J Dent Res. 1975;54:16–19. doi: 10.1177/00220345750540011101. https://doi.org/10.1177/00220345750540011101 PMid:1053755. [DOI] [PubMed] [Google Scholar]
- 15.Ahmad W, Brancolini V, ul Faiyaz MF, Lam H, ul Haque S, Haider M, et al. A locus for autosomal recessive hypodontia with associated dental anomalies maps to chromosome 16q 12.1. Am J Human Genet. 1998;62:987–991. doi: 10.1086/301799. https://doi.org/10.1086/301799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Magnusson TE. Prevalence of hypodontia and malformations of permanent teeth in Iceland. Community Dentistry and Oral Epidemiology. 1977;5:173–178. doi: 10.1111/j.1600-0528.1977.tb01635.x. https://doi.org/10.1111/j.1600-0528.1977.tb01635.x PMid:268264. [DOI] [PubMed] [Google Scholar]
- 17.Bäckman B, Wahlin YB. Variations in number and morphology of permanent teeth in 7-year-old Swedish children. International Journal of Paediatric Dentistry. 2001;11:11–17. doi: 10.1046/j.1365-263x.2001.00205.x. https://doi.org/10.1046/j.1365-263x.2001.00205.x PMid:11309867. [DOI] [PubMed] [Google Scholar]
- 18.Grahnen H. Hypodontia in the permanent dentition. Odontologisk Revg supplement. 1956;7:1–100. [Google Scholar]
- 19.Haavikko K. Hypodontia of permanent teeth. An orthopantomographic study. Suom Hammaslääk Toim. 1971;67:219–225. PMid:5289906. [PubMed] [Google Scholar]
- 20.Rolling S. Hypodontia of permanent teeth in Danish schoolchildren. Scand J Dent Res. 1980;88:365–369. doi: 10.1111/j.1600-0722.1980.tb01240.x. https://doi.org/10.1111/j.1600-0722.1980.tb01240.x. [DOI] [PubMed] [Google Scholar]
- 21.Lavelle CLB, Ashton EH, Flinn RM. Cusp pattern, tooth size and third molar agenesis in the human mandibular dentition. Archives of Oral Biology. 1970;15:227–237. doi: 10.1016/0003-9969(70)90081-6. https://doi.org/10.1016/0003-9969(70)90081-6. [DOI] [PubMed] [Google Scholar]
- 22.Müller TP, Hill IN, Peterson AC, Blayney JR. A survey of congenitally missing permanent teeth. American Journal of Orthodontics. 1970;81:101–107. doi: 10.14219/jada.archive.1970.0151. https://doi.org/10.14219/jada.archive.1970.0151. [DOI] [PubMed] [Google Scholar]
- 23.Symons Al, Stritzel F, Stamation J. Anomalies associated with hypodontia of the permanent lateral incisor and second premolar. Journal of clinical pediatrics dentistry. 1993;17:109–111. [PubMed] [Google Scholar]
- 24.Davis PJ. Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dentistry and Oral Epidemiology. 1987;15:218–220. doi: 10.1111/j.1600-0528.1987.tb00524.x. https://doi.org/10.1111/j.1600-0528.1987.tb00524.x PMid:3476247. [DOI] [PubMed] [Google Scholar]
- 25.Nik-Hussein NN. Hypodontia in the permanent dentition:a study of its prevalence in Malaysian children. Aust Orthod J. 1989;11(2):93–95. PMid:2639661. [PubMed] [Google Scholar]
- 26.Renkerova M, Badura S, Manikova H, Jambor J. A contribution to anomalous number of teeth in children in the Zilina District. Parakt Zubn Lek. 1989;37(1):12–8. PMid:2628961. [PubMed] [Google Scholar]
- 27.Lo Muzio L, Mignogna L, Bucci L, Sorrentino L. Statistical study of the incidence of agenesis in a sample of 1529 subjects. Minerva stomatologica. 1989;38:1039–43. [PubMed] [Google Scholar]
- 28.Dechkunakorn S, Chaiwat J, Sawaengkit P. Congenital absence and loss of teeth in an orthodontic patient group. J Dent Assoc Thai. 1990;40:165–76. PMid:2074329. [PubMed] [Google Scholar]
- 29.Al-Emran S, Wisth PJ, Böe OE. Prevalence of malocclusion and need for orthodontic treatment in Saudi Arabia. Community Dentistry and Oral Epidemiology 1990. 1990;18:253–255. doi: 10.1111/j.1600-0528.1990.tb00070.x. https://doi.org/10.1111/j.1600-0528.1990.tb00070.x PMid:2249408. [DOI] [PubMed] [Google Scholar]
- 30.Aasheim B, Øgaard B. Hypodontia in 9-year-old Norwegians related to need of orthodontic treatment. Scandinavian Journal of Dental Research. 1993;101:257–260. doi: 10.1111/j.1600-0722.1993.tb01115.x. https://doi.org/10.1111/j.1600-0722.1993.tb01115.x. [DOI] [PubMed] [Google Scholar]
- 31.Lynham A. Panoramic radiographic survey of hypodontia in Australian Defence Force recruits. Aust Dent J. 1990;35(1):19–22. doi: 10.1111/j.1834-7819.1990.tb03021.x. https://doi.org/10.1111/j.1834-7819.1990.tb03021.x PMid:2322168. [DOI] [PubMed] [Google Scholar]
- 32.Locht S. Panoramic radiographic examination of 704 Danish children aged 9–10 years. Community Dent Oral Epidemiol. 1980;8:375–380. doi: 10.1111/j.1600-0528.1980.tb01311.x. https://doi.org/10.1111/j.1600-0528.1980.tb01311.x PMid:6937285. [DOI] [PubMed] [Google Scholar]
- 33.Ghabanchi J, Haghnegahdar AA, Khodadazadeh Sh, Haghnegahdar S. A radiographic and clinical survey of dental anomalies in patient referring to Shiraz dental school. Shiraz Univ Dent J. 2010;10:26–31. [Google Scholar]
- 34.Uzuner D, Celik MM, Toy E, Turkdonmez CO. Assessment of hypodontia in the Turkish patients referring to the orthodontic clinic:A retrospective study. European Journal of Dentistry. 2013;7(Suppl 1):S9–S14. doi: 10.4103/1305-7456.119057. https://doi.org/10.4103/1305-7456.119057 PMid:24966736 PMCid:PMC4054087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Hunstadbraten K. Hypodontia in the permanent dentition. ASDC J Dent Child. 1973;40:115–7. PMid:4569097. [PubMed] [Google Scholar]
- 36.Onyeaso CO, Oneyeaso AO. Occlusal/dental anomalies found in a random sample of Nigerian schoolchildren. Oral Health Prev Dent. 2006;4:181–186. PMid:16961026. [PubMed] [Google Scholar]
- 37.Salcido-García JF, Ledesma-Montes C, Hernández-Flores F, Pérez D, Garcés-Ortíz M. Frequency of supernumerary teeth in Mexican population. Med Oral Patol Oral Cir Bucal. 2004;9:407–9. PMid:15580117. [PubMed] [Google Scholar]
- 38.Schmuckli R, Lipowsky C, Peltomäki T. Prevalence and morphology of supernumerary teeth in the population of a Swiss community. Short communication. Schweiz Monatsschr Zahnmed. 2010;120:987–93. PMid:21243544. [PubMed] [Google Scholar]
- 39.O'Dowling IB, McNamara TG. Congenital absence of permanent teeth among Irish school-children. J Ir Dent Assoc. 1990;36(4):136–8. PMid:2098447. [PubMed] [Google Scholar]
- 40.Gommes RR, da Fonseca JA, Paula LM, Faber J, Acevedo AG. Prevalenceof hypodontia in orthodontic patients in Brasilia, Brasil. Eur Jour. Orthod. 2010;32:3012–306. doi: 10.1093/ejo/cjp107. [DOI] [PubMed] [Google Scholar]
- 41.Davis PJ. Hypodontia and hyperdontia of permanent teeth in Hong Kong schoolchildren. Community Dentistry and Oral Epidemiology 1987. 1987;15:218–220. doi: 10.1111/j.1600-0528.1987.tb00524.x. https://doi.org/10.1111/j.1600-0528.1987.tb00524.x PMid:3476247. [DOI] [PubMed] [Google Scholar]
- 42.Amini F, Rakhshan V, Jamalzadeh S. Prevalence and Pattern of Accessory Teeth (Hyperdontia) in Permanent Dentition of Iranian Orthodontic Patients. Iranian Journal of Public Health. 2013;42(11):1259–1265. PMid:26171338 PMCid:PMC4499067. [PMC free article] [PubMed] [Google Scholar]
- 43.Vahid-Dastjerdi E, Borzabadi-Farahani A, Mahdian M, Amini N. Non-syndromic hypodontia in an Iranian orthodontic population. Journal of oral science. 2010;52(3):455–61. doi: 10.2334/josnusd.52.455. https://doi.org/10.2334/josnusd.52.455 PMid:20881340. [DOI] [PubMed] [Google Scholar]
- 44.Endo T, Ozoe R, Kubota M, Akiyama M, Shimooka S. A survey of Hypodontia in Japanese Orthodontic patients. American Journal of Orthodontics and Dentofacial Orthopedics. 2006;129(1):29–35. doi: 10.1016/j.ajodo.2004.09.024. https://doi.org/10.1016/j.ajodo.2004.09.024 PMid:16443475. [DOI] [PubMed] [Google Scholar]