

Abstract
Pulmonary embolism (PE) is a common and potentially deadly form of venous thromboembolic disease. It is the third most common cause of cardiovascular death and is associated with multiple inherited and acquired risk factors as well as advanced age. The prognosis from PE depends on the degree of obstruction and hemodynamic effects of PE and understanding the pathophysiology helps in risk-stratifying patients and determining treatment. Though the natural history of thrombus is resolution, a subset of patients have chronic residual thrombus, contributing to the post-PE syndrome.
Keywords: Pulmonary Embolism, venous thromboembolism, risk factors, hemodynamics, natural history, interventional radiology
Objectives: Upon completion of this article, the reader will be able to identify the disease burden of pulmonary embolism, as well as the progression of the disease with and without treatment, and potential for long-term disability.
Accreditation: This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Tufts University School of Medicine (TUSM) and Thieme Medical Publishers, New York. TUSM is accredited by the ACCME to provide continuing medical education for physicians.
Credit: Tufts University School of Medicine designates this journal-based CME activity for a maximum of 1 AMA PRA Category 1 Credit ™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Pulmonary embolism (PE) and deep venous thrombosis (DVT) exist on the spectrum of venous thromboembolic disease (VTE). PE results when thrombus migrates from the venous circulation to the pulmonary vasculature and lodges in the pulmonary arterial system. The clinical presentation of acute PE ranges from asymptomatic and incidentally discovered to massive PE causing immediate death. This review focuses on the epidemiology, risk factors, pathophysiology, and natural history of PE.
Epidemiology
Venous thromboembolism is a major worldwide burden of disease with ∼10 million cases per year and an associated substantial morbidity and mortality. 1 The true incidence of PE is unknown, but in the United States, it is estimated that nearly a third of hospitalized patients are at risk of developing VTE and up to 600,000 cases of VTE are diagnosed per year with 100,000 deaths related to these diseases. 2 3 In the United States, the estimated incidence of diagnosed VTE is 117 per 100,000, but the true incidence is likely to be more as these diseases are frequently undiagnosed or diagnosed only at autopsy. 4 5 6 Based on a review of national inpatient data, the number of admissions for PE increased from nearly 60,000 in 1993 (23 per 100,000) to more than 202,000 in 2012 (65 per 100,000). 7 Despite the increased incidence of PE, there was a decreased incidence of massive PE and hospital mortality over the same time period. Comorbidities associated with PE are also increasing (aging population and medical comorbidities), but the increased incidence in the face of decreased mortality likely reflects increased use of more sensitive CT angiography for diagnosis rather than a true change in prevalence. 7 8 9 10
VTE disproportionately affects the older population and incidence rates of VTE in those older than 70 years are three times higher than those aged 45 to 69 years, which again are three times higher than those aged 20 to 44 years. 11 This age-related increase in incidence in VTE is largely attributed to a disproportionate increase in PE burden. 4 7 The reported incidence of VTE is inconsistent with regard to gender, though several studies suggest higher incidence in males. 4 12
Between 5 and 10% of in-hospital deaths are a direct result of PE. 13 In the United States, PE is responsible for 100,000 deaths per year, though deaths from diagnosed PE have been decreasing. 12 14 Nevertheless, VTE is associated with significant mortality. The case fatality rate of a VTE event is ∼10% at 30 days, which increases to 15% within 3 months, with a further increase up to 20% by 1 year. 11 12 15
Risk Factors
In the mid-19th century, Rudolph Virchow identified the triad of risk factors that contribute to thrombosis—stasis of blood flow, vascular endothelial damage, and hypercoagulability. All VTE risk factors reflect these underlying pathophysiologic processes and generally patients who experience VTE have at least one risk factor. 16 Risk factors can be divided into inherited and acquired factors (see Table 1 ).
Table 1. Risk factors for VTE.
| Inherited risk factors |
| Factor V Leiden Prothrombin gene mutation Antithrombin deficiency Protein C deficiency Protein S deficiency |
| Acquired risk factors |
| Trauma Surgery Malignancy Peripartum state Estrogen therapy Aging Obesity |
Inherited Risk Factors
There are several genetic conditions known to increase the risk of VTE including factor V Leiden, prothrombin gene mutation (G20210-A), antithrombin deficiency, protein C deficiency, and protein S deficiency. Deficiencies in protein C, protein S, and antithrombin are relatively infrequent but potent, and they can confer a 5- to 10-fold increase in venous thrombosis in those affected. 17 18 19 Factor V Leiden is a more common mutation leading to hypercoagulability, and it is associated with a 5-fold increased risk of VTE with heterozygotes and a 10-fold risk with homozygotes. 20 Finally, the prothrombin gene mutation can be detected in 7% of patients with VTE and increases the risk of thrombosis threefold. 21
Acquired Risk Factors
Surgery and trauma are known to increase the risk of VTE. Orthopedic surgery in particular confers a higher risk with half of patients undergoing elective hip or knee replacement developing VTE without prophylaxis. 22 Similarly, patients with traumatic hip fractures are at higher risk for VTE both preoperatively and postoperatively. 23 24 The increased risk is mediated by immobility during and after the surgery as well as by direct venous injury and inflammation during surgery. Pharmacologic thromboprophylaxis is preferred over mechanical thromboprophylaxis and reduces the incidence of DVT and PE in the postoperative period. 25 Active malignancy, associated with the production of procoagulant substances, increases the risk of VTE sevenfold. 26 In a large population study of both solid and hematologic malignancies, nearly 2% of patients were diagnosed with VTE within 2 years of their cancer diagnosis, with the highest rates of VTE seen with metastatic disease and particularly with pancreatic and colon cancer. 27 Additionally, patients with high-grade tumors are at higher risk compared with those with low-grade tumors. 28 The risk of VTE is highest soon after diagnosis or after the initiation of treatment, and importantly, the risk diminishes when cancer is in remission. 27 29
Increased risk of VTE mediated primarily by stasis has been documented in patients with hospitalization, joint fixation, and prolonged travel. Recent hospitalization is noted in more than half of patients with VTE with up to two-thirds of post-hospitalization VTE occurring within the first month following hospitalization and the remainder over the next 3 months. 30 31 Joint immobility due to orthopedic injury in the absence of surgical management also increases the risk of VTE twofold compared with controls over a 72-hour period. 32 Travel is an often cited yet relatively uncommon causal factor for VTE with an estimated incidence of 4.8 cases of PE per million travelers flying over 10,000 km. 33 There is a direct relationship between the frequency of occurrence, the distance, and duration traveled. 34 35
A natural hypercoagulable state exists in pregnancy to decrease the risk of hemorrhage during childbirth. This is mediated by an increase in factors VII, VIII, X, von Willebrand factor, and fibrinogen, along with a decrease in protein S with an acquired activated protein C resistance. 36 37 The rate of VTE increases 4- to 5-fold during pregnancy with a 20-fold increase in 3 months following delivery. 3 38 DVT is four times as common as PE, and PE occurs more often postpartum. 39 40
The risk of VTE while on estrogen containing oral contraceptives increases three- to fourfold. 41 The risk is highest in the first year of use (especially the first 3 months), but it does not increase thereafter and is eliminated with cessation of therapy. 42 A similar increase in risk occurs with postmenopausal hormone replacement therapy. 43
Age-related changes to the balance between anticoagulants and procoagulants mediate an increased propensity for VTE with age. 44 There is an increase in VTE starting in the fourth and fifth decades with a marked increase in those older than 60 years. 4 This is confounded by decreasing mobility and higher rates of malignancy, obesity, and other comorbidities with increasing age. 45
There is a linear relationship between body mass index (BMI) and VTE, and patients with severe obesity (BMI ≥ 35) have a sixfold higher risk of VTE compared with those of normal weight. 46 Interestingly while the incidence of PE is higher in obese patients, the mortality is paradoxically lower than in nonobese patients. 47 It remains unclear whether this is due to increased body fat and an increased activity of the endocannabinoid system exerting a protective effect or due to another mechanism.
Antiphospholipid syndrome is characterized by recurrent venous or arterial thrombosis with DVT and PE being the most frequent manifestation occurring in one-third of patients. 48 The risk of VTE is 5 to 8% higher in patients who carry lupus anticoagulant or anti-β 2 -glycoprotine I antibodies. 49
Atherosclerosis and arterial disease may be related to increased risk of VTE mediated by increased platelet activation and coagulation pathway. Patients with atherosclerosis have an increased risk of VTE, 50 but this relationship is confounded by common comorbidities such as smoking, obesity, diabetes, hyperlipidemia, and hypertension. 51 52
In addition to the risk factors discussed earlier, a prior VTE event increases the risk for a recurrent event. Recurrence rates over a 5-year period can be 25% or higher in patients with unprovoked or idiopathic events. 53
Pathogenesis and Pathophysiology
Pathogenesis
Most PEs originate as thrombi in the deep veins of the lower extremities. The site of thrombosis is most frequently in the calf veins, then femoropopliteal veins, and less frequently in the iliac veins. 54 Thrombosis begins in areas of decreased flow such as valve cusps and bifurcations and then propagates due to local hypercoagulability caused by hypoxia and hemoconcentration. 55 56 A smaller percentage of emboli arises from upper extremity veins and are typically associated with central venous catheters, intracardiac devices such as pacemakers and defibrillators, and malignancy or activity-related venous trauma. 57 Pelvic vein DVTs can also cause pulmonary emboli, but they are generally associated with a predisposing factor such as pelvic infection, pelvic surgery, or pregnancy. Lower extremity central DVTs are most likely to embolize and cause PE (15–32% of the time), whereas upper extremity DVTs cause PE only 6% of the time. 58 59 60 Calf vein DVTs rarely embolize to the lungs, but one-third can extend into the central veins and subsequently have the potential to embolize. 61 62
Emboli detach from their point of origin and travel through the systemic venous system, through the right sided chambers of the heart, and lodge in the pulmonary arterial system. The physiologic and clinical consequences of PE vary ranging from asymptomatic to hemodynamic collapse and death. PE contributes to gas exchange abnormalities and hypoxemia, but it is predominantly the hemodynamic consequences of PE that are responsible for increased morbidity and mortality. An understanding of the pulmonary pathophysiology of PE is important in risk-stratifying patients to determine treatment with anticoagulation alone or consideration for catheter-directed therapies (thrombolytics or mechanical thrombectomy), systemic thrombolytics, or surgical intervention.
Hypoxemia and Gas Exchange
Though a normal partial arterial pressure of oxygen (PaO 2 ) does not exclude PE, hypoxemia is the most common physiologic consequence of acute PE. 63 64 65 The most common mechanisms of hypoxemia are ventilation–perfusion inequalities and shunt. 66 67 68 There is redistribution of cardiac output and blood flow from obstructed regions of the vascular bed to uninvolved areas of the pulmonary vascular bed. This results in areas of low ratios of ventilation to perfusion in some lung gas exchange units and areas of high ratios of ventilation to perfusion in other units. Shunting can be due to intrapulmonary or intracardiac causes. 69 Areas that retain blood flow but no ventilation such as atelectasis due to loss of surfactant or areas of pulmonary hemorrhage or infarct can contribute to shunt. Elevated right atrial pressures in setting of acute PE can open a patent foramen ovale and cause right-to-left intracardiac shunting. Low mixed venous saturation can also contribute to hypoxemia. Massive PE can cause reduced cardiac output leading to a low mixed venous oxygen saturation (SVO2). A low SVO2 coupled with VQ mismatch from the PE can exacerbate hypoxemia. One mechanism relates to areas of high flow (low V/Q units) in non obstructed areas. The abnormally desaturated venous blood will not have enough time to oxygenate as it passes through the alveolar capillaries in these low VQ units. 67 Vascular obstruction leads to increased dead space because lung units continue to be ventilated despite reduced or absent perfusion. Though increased dead space is expected to impair the elimination of carbon dioxide, hypercapnia in acute PE is rare because medullary receptors sense the increase in partial pressure of carbon dioxide and increase minute ventilation. Most patients with PE therefore have a respiratory alkalosis.
Hemodynamics
The cardiac and hemodynamic effects relate to the size and location of emboli and the presence or absence of underlying cardiopulmonary disease (CPD). As opposed to clot burden, acute PEs are categorized according to hemodynamic effect, with a focus on the effects of right ventricular (RV) physiology (see Fig. 1 ). Nonmassive PE patients are those who are normotensive with normal RV function. Massive PE implies hemodynamic instability from RV failure and submassive PE patients may clinically be normotensive but have evidence of RV dysfunction by echocardiography or CT imaging. These categories have risk implications with regard to morbidity and mortality and treatment choices. 70
Fig. 1.
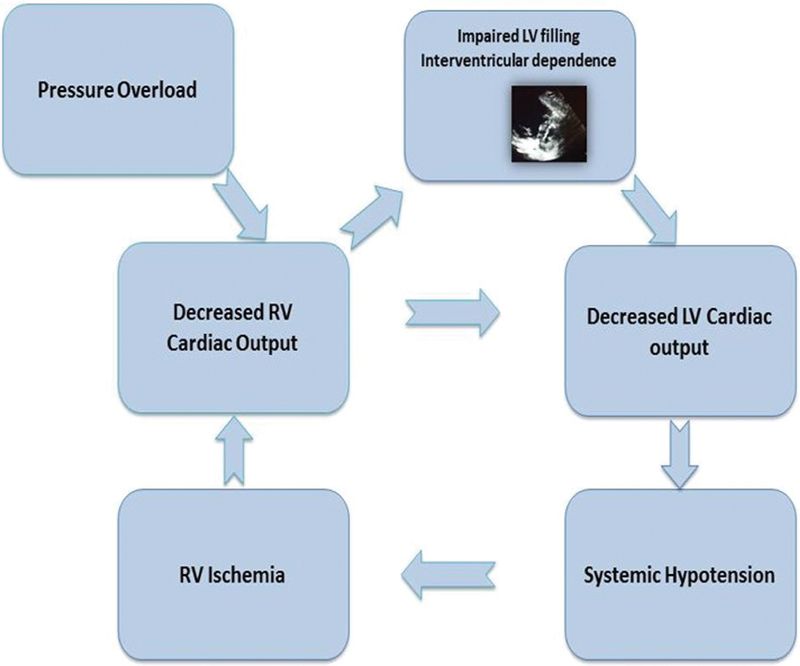
Physiologic consequences of right ventricular (RV) failure on left ventricular (LV) cardiac output. The RV and LV are connected in “series” and in “parallel.” Decreased RV cardiac output leads directly to decreased return to the LV and therefore decreased LV cardiac output (“connected in series”). Furthermore, RV overload and dilatation compresses the interventricular septum which impinges on the LV and further decreases the LV cardiac output (“connected in parallel”).
When thrombus embolizes from the extremities and lodges in the pulmonary arterial vasculature, pulmonary vascular resistance (PVR) increases due to both mechanical obstruction and release of vasoconstrictive substances from platelets (serotonin and thromboxane-A2), plasma (thrombin), and tissue (histamine and endothelin). 71 72 73 The thin walled RV is accustomed to low pressure and cannot easily adapt to this increased afterload, which has effects on both RV and left ventricular (LV) function. 74 If obstruction is mild, PVR and pulmonary artery pressure remain normal by recruiting and distending pulmonary vessels. At moderate levels of obstruction, pulmonary artery pressure and right atrial pressure increase. Initially, RV stroke volume and cardiac output are maintained by an increase in heart rate and contractility. In patients without prior CPD, the maximal mean pulmonary artery pressure that can be generated even with >50% obstruction is ∼40 mm Hg. Obstruction much beyond this will precipitate RV failure. When the degree of obstruction exceeds 50 to 60%, the right heart dilates, RV wall tension increases, coronary perfusion pressure drops, RV ischemia and RV dysfunction develops, and cardiac output falls, leading to hypotension. Furthermore, the dilated RV impinges on the intraventricular septum and via interventricular dependences causes decreased LV diastolic filling and decreased LV cardiac output ( Fig. 1 ). 75 76 77
In patients without prior CPD, the degree of obstruction has a hyperbolic relationship to PVR and the hemodynamic manifestations of PE are related to embolism size. Patients with preexisting CPD have diminished pulmonary vascular reserve and a smaller degree of obstruction can lead to disproportionate increase in pulmonary artery pressure and hemodynamic instability. 76
Natural History
Prognosis from PE depends on the degree of obstruction and hemodynamic effects of PE. Those with massive PE may be at imminent risk of death with an estimated mortality of 25 to 65%, those with submassive PE have a mortality of 3 to 15%, 58 while those with low-risk PE and normal heart function have <1% mortality with anticoagulation. 25 78 79 80 The risk for recurrent VTE is estimated at 20 to 25% after 5 years in unselected cohorts, and higher than 25% in those without a clear provoking cause. 53 81 Recurrence is also increased in those with associated congenital or acquired risk factors. 82 There are potential long-term consequences of PE with regard to functional impairment especially for those with recurrent PE.
The natural history of thrombus is resolution over time. However, 15 to 30% of patients have residual thrombus identified on lung scintigraphy 1 year after the initial event. 83 84 Persistent thrombus can contribute to ongoing increased PVR and RV pressure load and have physiologic consequences leading to functional impairment and decreased quality of life. The “post-PE syndrome” is defined by dyspnea, exercise intolerance, and diminished quality of life in the setting of suboptimal cardiac function, pulmonary artery flow dynamics, or pulmonary gas exchange. 85 The most severe manifestation of post-PE syndrome is chronic thromboembolic pulmonary hypertension (CTEPH), which affects an estimated 1 to 5% of survivors of acute PE. 86 87 Chronic thromboembolic disease (CTED) refers to persistent perfusion defects without pulmonary hypertension, and it is estimated that based on the incidence of acute PE in the United States, 35,000 people will have CTED and 1,250 will have CTEPH. 85 88
Conclusion
The incidence of PE is increasing possibly due to overdiagnosis, and although mortality is falling, PE continues to be a common and a potentially fatal form of VTE. Inherited and acquired risk factors (particularly surgery and malignancy) increase the likelihood of VTE and PE. Though commonly a cause of gas exchange abnormalities, mortality risk is due to the cardiovascular consequences of obstruction with increasing PVR, RV pressure load, and dysfunction. Both the burden of PE and underlying cardiopulmonary status contribute to these hemodynamic consequences. In addition to the immediate morbidity and mortality caused by PE, in recent years the post-PE syndrome of functional limitation in association with ongoing cardiac and gas exchange dysfunction has received more attention and research is ongoing to determine who is at increased risk for these consequences especially in the submassive population with the question of benefits from early intervention to reduce clot burden.
References
- 1.Raskob G E, Angchaisuksiri P, Blanco A N et al. Thrombosis: a major contributor to global disease burden. Semin Thromb Hemost. 2014;40(07):724–735. doi: 10.1055/s-0034-1390325. [DOI] [PubMed] [Google Scholar]
- 2.Anderson F A, Jr, Zayaruzny M, Heit J A, Fidan D, Cohen A T. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol. 2007;82(09):777–782. doi: 10.1002/ajh.20983. [DOI] [PubMed] [Google Scholar]
- 3.Heit J A, Kobbervig C E, James A H, Petterson T M, Bailey K R, Melton L J., III Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med. 2005;143(10):697–706. doi: 10.7326/0003-4819-143-10-200511150-00006. [DOI] [PubMed] [Google Scholar]
- 4.Silverstein M D, Heit J A, Mohr D N, Petterson T M, O'Fallon W M, Melton L J., III Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998;158(06):585–593. doi: 10.1001/archinte.158.6.585. [DOI] [PubMed] [Google Scholar]
- 5.Anderson F A, Jr, Wheeler H B, Goldberg R J et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med. 1991;151(05):933–938. [PubMed] [Google Scholar]
- 6.Goldhaber S Z, Hennekens C H, Evans D A, Newton E C, Godleski J J. Factors associated with correct antemortem diagnosis of major pulmonary embolism. Am J Med. 1982;73(06):822–826. doi: 10.1016/0002-9343(82)90764-1. [DOI] [PubMed] [Google Scholar]
- 7.Smith S B, Geske J B, Kathuria P et al. Analysis of national trends in admissions for pulmonary embolism. Chest. 2016;150(01):35–45. doi: 10.1016/j.chest.2016.02.638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wiener R S, Schwartz L M, Woloshin S. Time trends in pulmonary embolism in the United States: evidence of overdiagnosis. Arch Intern Med. 2011;171(09):831–837. doi: 10.1001/archinternmed.2011.178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sheh S H, Bellin E, Freeman K D, Haramati L B. Pulmonary embolism diagnosis and mortality with pulmonary CT angiography versus ventilation-perfusion scintigraphy: evidence of overdiagnosis with CT? AJR Am J Roentgenol. 2012;198(06):1340–1345. doi: 10.2214/AJR.11.6426. [DOI] [PubMed] [Google Scholar]
- 10.Huang W, Goldberg R J, Anderson F A, Kiefe C I, Spencer F A. Secular trends in occurrence of acute venous thromboembolism: the Worcester VTE study (1985-2009) Am J Med. 2014;127(09):829–3.9E6. doi: 10.1016/j.amjmed.2014.03.041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Naess I A, Christiansen S C, Romundstad P, Cannegieter S C, Rosendaal F R, Hammerstrøm J. Incidence and mortality of venous thrombosis: a population-based study. J Thromb Haemost. 2007;5(04):692–699. doi: 10.1111/j.1538-7836.2007.02450.x. [DOI] [PubMed] [Google Scholar]
- 12.Horlander K T, Mannino D M, Leeper K V. Pulmonary embolism mortality in the United States, 1979-1998: an analysis using multiple-cause mortality data. Arch Intern Med. 2003;163(14):1711–1717. doi: 10.1001/archinte.163.14.1711. [DOI] [PubMed] [Google Scholar]
- 13.Alikhan R, Peters F, Wilmott R, Cohen A T. Fatal pulmonary embolism in hospitalised patients: a necropsy review. J Clin Pathol. 2004;57(12):1254–1257. doi: 10.1136/jcp.2003.013581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lilienfeld D E. Decreasing mortality from pulmonary embolism in the United States, 1979-1996. Int J Epidemiol. 2000;29(03):465–469. [PubMed] [Google Scholar]
- 15.Tagalakis V, Patenaude V, Kahn S R, Suissa S. Incidence of and mortality from venous thromboembolism in a real-world population: the Q-VTE Study Cohort. Am J Med. 2013;126(09):8.32E15–8.32E23. doi: 10.1016/j.amjmed.2013.02.024. [DOI] [PubMed] [Google Scholar]
- 16.Anderson F A, Jr, Wheeler H B. Physician practices in the management of venous thromboembolism: a community-wide survey. J Vasc Surg. 1992;16(05):707–714. doi: 10.1067/mva.1992.41080. [DOI] [PubMed] [Google Scholar]
- 17.Allaart C F, Poort S R, Rosendaal F R, Reitsma P H, Bertina R M, Briët E.Increased risk of venous thrombosis in carriers of hereditary protein C deficiency defect Lancet 1993341(8838):134–138. [DOI] [PubMed] [Google Scholar]
- 18.Demers C, Ginsberg J S, Hirsh J, Henderson P, Blajchman M A. Thrombosis in antithrombin-III-deficient persons. Report of a large kindred and literature review. Ann Intern Med. 1992;116(09):754–761. doi: 10.7326/0003-4819-116-9-754. [DOI] [PubMed] [Google Scholar]
- 19.Heijboer H, Brandjes D P, Büller H R, Sturk A, ten Cate J W. Deficiencies of coagulation-inhibiting and fibrinolytic proteins in outpatients with deep-vein thrombosis. N Engl J Med. 1990;323(22):1512–1516. doi: 10.1056/NEJM199011293232202. [DOI] [PubMed] [Google Scholar]
- 20.Rosendaal F R, Koster T, Vandenbroucke J P, Reitsma P H. High risk of thrombosis in patients homozygous for factor V Leiden (activated protein C resistance) Blood. 1995;85(06):1504–1508. [PubMed] [Google Scholar]
- 21.Poort S R, Rosendaal F R, Reitsma P H, Bertina R M. A common genetic variation in the 3′-untranslated region of the prothrombin gene is associated with elevated plasma prothrombin levels and an increase in venous thrombosis. Blood. 1996;88(10):3698–3703. [PubMed] [Google Scholar]
- 22.Stulberg B N, Insall J N, Williams G W, Ghelman B. Deep-vein thrombosis following total knee replacement. An analysis of six hundred and thirty-eight arthroplasties. J Bone Joint Surg Am. 1984;66(02):194–201. [PubMed] [Google Scholar]
- 23.Shin W C, Woo S H, Lee S-J, Lee J S, Kim C, Suh K T. Preoperative prevalence of and risk factors for venous thromboembolism in patients with a hip fracture: an indirect multidetector CT venography study. J Bone Joint Surg Am. 2016;98(24):2089–2095. doi: 10.2106/JBJS.15.01329. [DOI] [PubMed] [Google Scholar]
- 24.Sevitt S, Gallagher N G.Prevention of venous thrombosis and pulmonary embolism in injured patients. A trial of anticoagulant prophylaxis with phenindione in middle-aged and elderly patients with fractured necks of femur Lancet 19592(7110):981–989. [DOI] [PubMed] [Google Scholar]
- 25.Kearon C, Akl E A, Comerota A Jet al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines Chest 2012141(2, Suppl):e419S–e496S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Blom J W, Doggen C J, Osanto S, Rosendaal F R. Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA. 2005;293(06):715–722. doi: 10.1001/jama.293.6.715. [DOI] [PubMed] [Google Scholar]
- 27.Chew H K, Wun T, Harvey D, Zhou H, White R H. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med. 2006;166(04):458–464. doi: 10.1001/archinte.166.4.458. [DOI] [PubMed] [Google Scholar]
- 28.Ahlbrecht J, Dickmann B, Ay C et al. Tumor grade is associated with venous thromboembolism in patients with cancer: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2012;30(31):3870–3875. doi: 10.1200/JCO.2011.40.1810. [DOI] [PubMed] [Google Scholar]
- 29.Stein P D, Beemath A, Meyers F A, Skaf E, Sanchez J, Olson R E. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006;119(01):60–68. doi: 10.1016/j.amjmed.2005.06.058. [DOI] [PubMed] [Google Scholar]
- 30.Heit J A, O'Fallon W M, Petterson T M et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162(11):1245–1248. doi: 10.1001/archinte.162.11.1245. [DOI] [PubMed] [Google Scholar]
- 31.Spencer F A, Gore J M, Lessard D, Douketis J D, Emery C, Goldberg R J. Patient outcomes after deep vein thrombosis and pulmonary embolism: the Worcester Venous Thromboembolism Study. Arch Intern Med. 2008;168(04):425–430. doi: 10.1001/archinternmed.2007.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Beam D M, Courtney D M, Kabrhel C, Moore C L, Richman P B, Kline J A. Risk of thromboembolism varies, depending on category of immobility in outpatients. Ann Emerg Med. 2009;54(02):147–152. doi: 10.1016/j.annemergmed.2008.10.033. [DOI] [PubMed] [Google Scholar]
- 33.Lapostolle F, Surget V, Borron S W et al. Severe pulmonary embolism associated with air travel. N Engl J Med. 2001;345(11):779–783. doi: 10.1056/NEJMoa010378. [DOI] [PubMed] [Google Scholar]
- 34.Cruickshank J M, Gorlin R, Jennett B.Air travel and thrombotic episodes: the economy class syndrome Lancet 19882(8609):497–498. [DOI] [PubMed] [Google Scholar]
- 35.Chandra D, Parisini E, Mozaffarian D. Meta-analysis: travel and risk for venous thromboembolism. Ann Intern Med. 2009;151(03):180–190. doi: 10.7326/0003-4819-151-3-200908040-00129. [DOI] [PubMed] [Google Scholar]
- 36.Brenner B.Haemostatic changes in pregnancy Thromb Res 2004114(5-6):409–414. [DOI] [PubMed] [Google Scholar]
- 37.Cerneca F, Ricci G, Simeone R, Malisano M, Alberico S, Guaschino S. Coagulation and fibrinolysis changes in normal pregnancy. Increased levels of procoagulants and reduced levels of inhibitors during pregnancy induce a hypercoagulable state, combined with a reactive fibrinolysis. Eur J Obstet Gynecol Reprod Biol. 1997;73(01):31–36. doi: 10.1016/s0301-2115(97)02734-6. [DOI] [PubMed] [Google Scholar]
- 38.James A H. Venous thromboembolism in pregnancy. Arterioscler Thromb Vasc Biol. 2009;29(03):326–331. doi: 10.1161/ATVBAHA.109.184127. [DOI] [PubMed] [Google Scholar]
- 39.James A H, Tapson V F, Goldhaber S Z. Thrombosis during pregnancy and the postpartum period. Am J Obstet Gynecol. 2005;193(01):216–219. doi: 10.1016/j.ajog.2004.11.037. [DOI] [PubMed] [Google Scholar]
- 40.James A H, Jamison M G, Brancazio L R, Myers E R. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. Am J Obstet Gynecol. 2006;194(05):1311–1315. doi: 10.1016/j.ajog.2005.11.008. [DOI] [PubMed] [Google Scholar]
- 41.Petitti D B. Clinical practice. Combination estrogen-progestin oral contraceptives. N Engl J Med. 2003;349(15):1443–1450. doi: 10.1056/NEJMcp030751. [DOI] [PubMed] [Google Scholar]
- 42.Lidegaard Ø, Løkkegaard E, Svendsen A L, Agger C. Hormonal contraception and risk of venous thromboembolism: national follow-up study. BMJ. 2009;339:b2890. doi: 10.1136/bmj.b2890. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Miller J, Chan B K, Nelson H D. Postmenopausal estrogen replacement and risk for venous thromboembolism: a systematic review and meta-analysis for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;136(09):680–690. doi: 10.7326/0003-4819-136-9-200205070-00011. [DOI] [PubMed] [Google Scholar]
- 44.Lowe G D, Rumley A, Woodward M et al. Epidemiology of coagulation factors, inhibitors and activation markers: the Third Glasgow MONICA Survey. I. Illustrative reference ranges by age, sex and hormone use. Br J Haematol. 1997;97(04):775–784. doi: 10.1046/j.1365-2141.1997.1222936.x. [DOI] [PubMed] [Google Scholar]
- 45.Silverstein R L, Bauer K A, Cushman M, Esmon C T, Ershler W B, Tracy R P. Venous thrombosis in the elderly: more questions than answers. Blood. 2007;110(09):3097–3101. doi: 10.1182/blood-2007-06-096545. [DOI] [PubMed] [Google Scholar]
- 46.Goldhaber S Z, Grodstein F, Stampfer M J et al. A prospective study of risk factors for pulmonary embolism in women. JAMA. 1997;277(08):642–645. [PubMed] [Google Scholar]
- 47.Stein P D, Matta F, Goldman J. Obesity and pulmonary embolism: the mounting evidence of risk and the mortality paradox. Thromb Res. 2011;128(06):518–523. doi: 10.1016/j.thromres.2011.10.019. [DOI] [PubMed] [Google Scholar]
- 48.Cervera R, Piette J-C, Font J et al. Antiphospholipid syndrome: clinical and immunologic manifestations and patterns of disease expression in a cohort of 1,000 patients. Arthritis Rheum. 2002;46(04):1019–1027. doi: 10.1002/art.10187. [DOI] [PubMed] [Google Scholar]
- 49.Schved J F, Dupuy-Fons C, Biron C, Quére I, Janbon C. A prospective epidemiological study on the occurrence of antiphospholipid antibody: the Montpellier Antiphospholipid (MAP) Study. Haemostasis. 1994;24(03):175–182. doi: 10.1159/000217099. [DOI] [PubMed] [Google Scholar]
- 50.Prandoni P, Bilora F, Marchiori A et al. An association between atherosclerosis and venous thrombosis. N Engl J Med. 2003;348(15):1435–1441. doi: 10.1056/NEJMoa022157. [DOI] [PubMed] [Google Scholar]
- 51.Ageno W, Becattini C, Brighton T, Selby R, Kamphuisen P W. Cardiovascular risk factors and venous thromboembolism: a meta-analysis. Circulation. 2008;117(01):93–102. doi: 10.1161/CIRCULATIONAHA.107.709204. [DOI] [PubMed] [Google Scholar]
- 52.Glynn R J, Rosner B. Comparison of risk factors for the competing risks of coronary heart disease, stroke, and venous thromboembolism. Am J Epidemiol. 2005;162(10):975–982. doi: 10.1093/aje/kwi309. [DOI] [PubMed] [Google Scholar]
- 53.Hansson P-O, Sörbo J, Eriksson H. Recurrent venous thromboembolism after deep vein thrombosis: incidence and risk factors. Arch Intern Med. 2000;160(06):769–774. doi: 10.1001/archinte.160.6.769. [DOI] [PubMed] [Google Scholar]
- 54.Ouriel K, Green R M, Greenberg R K, Clair D G. The anatomy of deep venous thrombosis of the lower extremity. J Vasc Surg. 2000;31(05):895–900. doi: 10.1067/mva.2000.105956. [DOI] [PubMed] [Google Scholar]
- 55.McLachlin A D, McLachlin J A, Jory T A, Rawling E G. Venous stasis in the lower extremities. Ann Surg. 1960;152(04):678–685. doi: 10.1097/00000658-196010000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Sevitt S. Organization of valve pocket thrombi and the anomalies of double thrombi and valve cusp involvement. Br J Surg. 1974;61(08):641–649. doi: 10.1002/bjs.1800610812. [DOI] [PubMed] [Google Scholar]
- 57.Sajid M S, Ahmed N, Desai M, Baker D, Hamilton G. Upper limb deep vein thrombosis: a literature review to streamline the protocol for management. Acta Haematol. 2007;118(01):10–18. doi: 10.1159/000101700. [DOI] [PubMed] [Google Scholar]
- 58.Kucher N, Tapson V F, Goldhaber S Z; DVT FREE Steering Committee.Risk factors associated with symptomatic pulmonary embolism in a large cohort of deep vein thrombosis patients Thromb Haemost 20059303494–498. [DOI] [PubMed] [Google Scholar]
- 59.Stein P D, Matta F, Musani M H, Diaczok B. Silent pulmonary embolism in patients with deep venous thrombosis: a systematic review. Am J Med. 2010;123(05):426–431. doi: 10.1016/j.amjmed.2009.09.037. [DOI] [PubMed] [Google Scholar]
- 60.Muñoz F J, Mismetti P, Poggio R et al. Clinical outcome of patients with upper-extremity deep vein thrombosis: results from the RIETE Registry. Chest. 2008;133(01):143–148. doi: 10.1378/chest.07-1432. [DOI] [PubMed] [Google Scholar]
- 61.Huisman M V, Büller H R, ten Cate J W. Utility of impedance plethysmography in the diagnosis of recurrent deep-vein thrombosis. Arch Intern Med. 1988;148(03):681–683. [PubMed] [Google Scholar]
- 62.Masuda E M, Kistner R L, Musikasinthorn C, Liquido F, Geling O, He Q. The controversy of managing calf vein thrombosis. J Vasc Surg. 2012;55(02):550–561. doi: 10.1016/j.jvs.2011.05.092. [DOI] [PubMed] [Google Scholar]
- 63.Overton D T, Bocka J J. The alveolar-arterial oxygen gradient in patients with documented pulmonary embolism. Arch Intern Med. 1988;148(07):1617–1619. [PubMed] [Google Scholar]
- 64.Stein P D, Goldhaber S Z, Henry J W. Alveolar-arterial oxygen gradient in the assessment of acute pulmonary embolism. Chest. 1995;107(01):139–143. doi: 10.1378/chest.107.1.139. [DOI] [PubMed] [Google Scholar]
- 65.Santolicandro A, Prediletto R, Fornai E et al. Mechanisms of hypoxemia and hypocapnia in pulmonary embolism. Am J Respir Crit Care Med. 1995;152(01):336–347. doi: 10.1164/ajrccm.152.1.7599843. [DOI] [PubMed] [Google Scholar]
- 66.Huet Y, Lemaire F, Brun-Buisson C et al. Hypoxemia in acute pulmonary embolism. Chest. 1985;88(06):829–836. doi: 10.1378/chest.88.6.829. [DOI] [PubMed] [Google Scholar]
- 67.Manier G, Castaing Y, Guenard H. Determinants of hypoxemia during the acute phase of pulmonary embolism in humans. Am Rev Respir Dis. 1985;132(02):332–338. doi: 10.1164/arrd.1985.132.2.332. [DOI] [PubMed] [Google Scholar]
- 68.D'Angelo E. Lung mechanics and gas exchange in pulmonary embolism. Haematologica. 1997;82(03):371–374. [PubMed] [Google Scholar]
- 69.D'Alonzo G E, Bower J S, DeHart P, Dantzker D R. The mechanisms of abnormal gas exchange in acute massive pulmonary embolism. Am Rev Respir Dis. 1983;128(01):170–172. doi: 10.1164/arrd.1983.128.1.170. [DOI] [PubMed] [Google Scholar]
- 70.Jaff M R, McMurtry M S, Archer S L et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011;123(16):1788–1830. doi: 10.1161/CIR.0b013e318214914f. [DOI] [PubMed] [Google Scholar]
- 71.Elliott C G.Pulmonary physiology during pulmonary embolism Chest 1992101(4, Suppl):163S–171S. [DOI] [PubMed] [Google Scholar]
- 72.Tsang J Y, Lamm W J. Estimation of endothelin-mediated vasoconstriction in acute pulmonary thromboembolism. Pulm Circ. 2012;2(01):67–74. doi: 10.4103/2045-8932.94836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Smulders Y M. Pathophysiology and treatment of haemodynamic instability in acute pulmonary embolism: the pivotal role of pulmonary vasoconstriction. Cardiovasc Res. 2000;48(01):23–33. doi: 10.1016/s0008-6363(00)00168-1. [DOI] [PubMed] [Google Scholar]
- 74.Matthews J C, McLaughlin V. Acute right ventricular failure in the setting of acute pulmonary embolism or chronic pulmonary hypertension: a detailed review of the pathophysiology, diagnosis, and management. Curr Cardiol Rev. 2008;4(01):49–59. doi: 10.2174/157340308783565384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.McIntyre K M, Sasahara A A. Determinants of right ventricular function and hemodynamics after pulmonary embolism. Chest. 1974;65(05):534–543. doi: 10.1378/chest.65.5.534. [DOI] [PubMed] [Google Scholar]
- 76.Wood K E. Major pulmonary embolism: review of a pathophysiologic approach to the golden hour of hemodynamically significant pulmonary embolism. Chest. 2002;121(03):877–905. doi: 10.1378/chest.121.3.877. [DOI] [PubMed] [Google Scholar]
- 77.Lualdi J C, Goldhaber S Z. Right ventricular dysfunction after acute pulmonary embolism: pathophysiologic factors, detection, and therapeutic implications. Am Heart J. 1995;130(06):1276–1282. doi: 10.1016/0002-8703(95)90155-8. [DOI] [PubMed] [Google Scholar]
- 78.Konstantinides S, Torbicki A, Agnelli G et al. 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014;35(43):3033–3069. doi: 10.1093/eurheartj/ehu283. [DOI] [PubMed] [Google Scholar]
- 79.Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W; Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators.Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism N Engl J Med 2002347151143–1150. [DOI] [PubMed] [Google Scholar]
- 80.Meyer G, Vicaut E, Danays T et al. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014;370(15):1402–1411. doi: 10.1056/NEJMoa1302097. [DOI] [PubMed] [Google Scholar]
- 81.Prandoni P, Noventa F, Ghirarduzzi A et al. The risk of recurrent venous thromboembolism after discontinuing anticoagulation in patients with acute proximal deep vein thrombosis or pulmonary embolism. A prospective cohort study in 1,626 patients. Haematologica. 2007;92(02):199–205. doi: 10.3324/haematol.10516. [DOI] [PubMed] [Google Scholar]
- 82.Kyrle P A, Rosendaal F R, Eichinger S.Risk assessment for recurrent venous thrombosis Lancet 2010376(9757):2032–2039. [DOI] [PubMed] [Google Scholar]
- 83.Sanchez O, Helley D, Couchon S et al. Perfusion defects after pulmonary embolism: risk factors and clinical significance. J Thromb Haemost. 2010;8(06):1248–1255. doi: 10.1111/j.1538-7836.2010.03844.x. [DOI] [PubMed] [Google Scholar]
- 84.Cosmi B, Nijkeuter M, Valentino M, Huisman M V, Barozzi L, Palareti G. Residual emboli on lung perfusion scan or multidetector computed tomography after a first episode of acute pulmonary embolism. Intern Emerg Med. 2011;6(06):521–528. doi: 10.1007/s11739-011-0577-8. [DOI] [PubMed] [Google Scholar]
- 85.Sista A K, Klok F A. Late outcomes of pulmonary embolism: the post-PE syndrome. Thromb Res. 2018;164:157–162. doi: 10.1016/j.thromres.2017.06.017. [DOI] [PubMed] [Google Scholar]
- 86.Klok F A, van Kralingen K W, van Dijk A P, Heyning F H, Vliegen H W, Huisman M V. Prospective cardiopulmonary screening program to detect chronic thromboembolic pulmonary hypertension in patients after acute pulmonary embolism. Haematologica. 2010;95(06):970–975. doi: 10.3324/haematol.2009.018960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Pengo V, Lensing A W, Prins M H et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med. 2004;350(22):2257–2264. doi: 10.1056/NEJMoa032274. [DOI] [PubMed] [Google Scholar]
- 88.Delcroix M, Kerr K, Fedullo P. Chronic thromboembolic pulmonary hypertension. Epidemiology and risk factors. Ann Am Thorac Soc. 2016;13 03:S201–S206. doi: 10.1513/AnnalsATS.201509-621AS. [DOI] [PubMed] [Google Scholar]