

Abstract
Background:
According to the Association of Nephrologist in Indonesia (Pernefri) recommendation, isolation and using special hemodialysis machines are not necessary for hemodialysis (HD) patients who have been infected by hepatitis C virus (HCV), while according to the Ministry of Health Malaysia recommendation, hepatitis C patients should be dialyzed in a separate room or a separate area with a fixed partition and dedicated machines.
Aim:
The aim of this study was to identify the correlation between the recommendation which had been followed by two HD centers in different countries and the impact of that on the hepatitis C infection issue.
Methods:
A cohort prospective and retrospective study was done in this research. The study included HD patients who were followed up for 9 months and who died in the last 5 years. Universal sampling was used to select the patients based on inclusion criteria.
Results:
There was a significant relationship between HCV during the first checkup and HCV during the second checkup during the 9-month follow-up of HD patients in a HD center, Jakarta, Indonesia. The total number of patients who had hepatitis C during the first and second checkups was also different in this HD center.
Conclusion:
Besides providing special HD rooms and machines for HD patients with hepatitis C, minimizing blood transfusion to the patients on HD is also important to reduce the chance for the patients to acquire hepatitis C and to increase the percentage of survival.
Keywords: Hemodialysis, hepatitis C, Indonesia, Malaysia
INTRODUCTION
Hemodialysis (HD) is one of the treatments that is done to replace renal function. Usually, HD centers in all the hospitals will carry out the treatment process appropriate with the guidelines that they used. One of the guidelines famous for HD ward is KDOQI Clinical Practice Guideline Hemodialysis.[1]
Hepatitis C virus (HCV) is transmitted mainly through intravenous infusions.[2] In Asia, HCV infection has become a serious public health problem because it is difficult to identify carriers of HCV and take effective security measures in the HD center, so patients undergoing dialysis are often exposed to HCV.[3]
The European Renal Best Practice (ERBP) workgroup considers isolation of HCV-positive patients who are undergoing HD, although the Kidney Disease Improving Global Outcomes (KDIGO) workgroup concluded that the isolation of HCV-infected patients is not recommended.[4]
According to the Association of Nephrologist in Indonesia (Pernefri) recommendation, isolation and using special HD machines are not necessary for HD patients who have been infected by HCV (Recommendation for controlling hepatitis B virus and HCV infection by PERNEFRI), while the Ministry of Health Malaysia recommend that HD patients who have been infected by HCV should be dialyzed in a separate room or a separate area with a fixed partition and dedicated machines.
MATERIALS AND METHODS
Study location
The research was carried out in the HD ward of Cempaka Putih Islamic Hospital, Jakarta, Indonesia, and General Hospital, Pulau Pinang, Malaysia.
Study participants
The study included diabetic and/or hypertensive patients who underwent HD. Universal sampling was used to select patients based on the inclusion criteria among 178 patients who had been followed up for 9 months and 185 patients who died in the last 5 years in a HD center Jakarta, Indonesia. In a HD center, Penang, universal sampling was used to select among 78 patients who had been followed up for 9 months and 14 patients who died in the last 5 years.
Study design
This was a cohort prospective and retrospective study
-
Inclusion criteria:
- All HD patients who are diabetic and/or hypertensive
- Patients ≥18 years.
-
Exclusion criteria:
- Patients <18 years
- Cancer patients
- Pregnancy patients
- HIV/AIDS patients
- Systemic lupus erythema patients.
Ethical clearance
Ethical clearance was sourced from the Ethical Medical Committee of the Faculty of Medicine in Indonesia and Committee Research Center in Pulau Pinang, Malaysia. The approval letters were given before the start of data collection. Data were collected at Cempaka Putih Islamic Hospital, Jakarta, Indonesia, and General Hospital, Pulau Pinang, Malaysia.
Data collection and handling
The researcher would define the patients by the list of patients in the ward and before collecting data from the medical record, the researcher would explain about the research (background and the purpose of the research) to the patients. Data collection would be started after patients signed the informed consent as an agreement of the research. The data were arranged according to the sociodemographic status, laboratory value checked, and current medication and transferred to clinical research form. The researcher would follow up the patients for 9 months. It can be seen in the research framework [Figure 1].
Figure 1.

Research framework
RESULTS
There was a significant relationship between HCV during the first checkup and HCV during the second checkup among HD patients who had been followed up for 9 months in a HD center, Jakarta, Indonesia, as shown in Tables 1 and 2. The total number of patients who had hepatitis C during the first checkup and in the second checkup was different in this HD center, while in the first checkup, 46 HD patients were found to be reactive in HCV. It increased in the second checkup, while 60 HD patients were determined to be reactive in HCV.
Table 1.
The number of hemodialysis patients who had hepatitis C and the correlation with the clinical outcome among diabetic/hypertensive patients who underwent hemodialysis in a hemodialysis center, Jakarta, Indonesia, and Penang, Malaysia
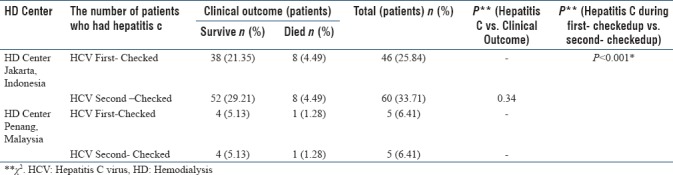
Table 2.
The number of diabetic and/or hypertensive patients who underwent hemodialysis with hepatitis C infection in a hemodialysis center, Jakarta, Indonesia, and Penang, Malaysia

The highest number (58.38 &age) of HD patients who had been infected by hepatitis virus was observed in a HD center Jakarta, Indonesia, for both prospective and retrospective data. The highest number of patients who had hepatitis C infection was the patients who had the month's life since initiating of HD between 13 and 48 months for HD patients who had died in the last 5 years in a HD center, Jakarta, Indonesia, as shown in Table 3.
Table 3.
The number of hemodialysis patients who had hepatitis C infection based on the month's life since initiating hemodialysis among hemodialysis patients who had died in the last 5 years in a hemodialysis center, Jakarta, Indonesia
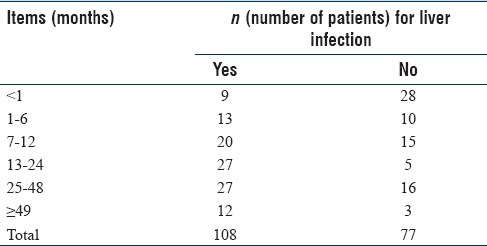
Table 4 shows the relationship between the first follow-up, second follow-up, and third follow-up of SGPT and SGOT for hepatitis C infection among HD patients who had died in the last 5 years in a HD center Jakarta, Indonesia. Significant relationship was found between the first, second, and third follow-up of SGPT for hepatitis C infection but for SGOT, the significant relationship can be seen only between the third follow-up and hepatitis C infection, P < 0.005. Correlation between the first and third follow-up of SGPT and SGOT laboratory value among HD patients who had died in the last 5 years in a HD center, Jakarta, Indonesia, showed a significant relationship (P < 0.001) as shown in Table 5.
Table 4.
Correlation between the first follow-up, second follow-up, and third follow-up of serum glutamic pyruvic transaminase and serum glutamic oxaloacetic transaminase for hepatitis C infection among hemodialysis patients who had died in the last 5 years in a hemodialysis center, Jakarta, Indonesia
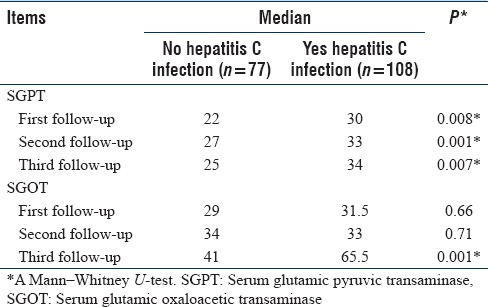
Table 5.
Correlation between the first follow-up and third follow-up of serum glutamic pyruvic transaminase and serum glutamic oxaloacetic transaminase among hemodialysis patients who had died in the last 5 years in a hemodialysis center, Jakarta, Indonesia
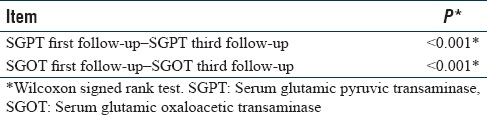
Table 6 shows anemia medication that hemodialyzed patients used in both the HD centers. More than 90% of hemodialyzed patients in Malaysia used erythropoietin (EPO), but only 15.20% of hemodialyzed patients in Indonesia used EPO, and during research based on the investigation in the HD ward., (new Sentence) Most of the patients in Indonesia had experience in below of hemoglobin level (<8 mg/dl). Blood transfusion was the common way to treat the patients having lower value than a normal range of hemoglobin in Indonesia.
Table 6.
Recombinant human erythropoietin used by diabetic/hypertensive patients who underwent hemodialysis (for prospective sample/9-month follow-up) in a hemodialysis center, Jakarta, Indonesia, and in a hemodialysis center, Penang, Malaysia
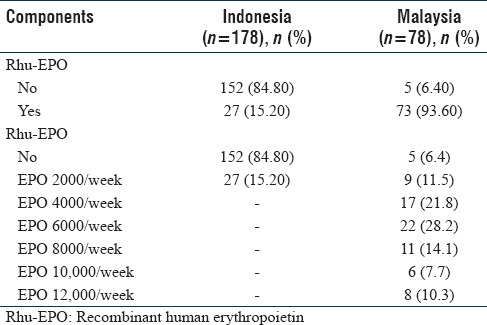
Figure 2 shows HD patients who had hepatitis in a HD center, Jakarta, Indonesia, and Penang, Malaysia. Significant relationship was found among overall comparisons between survival analysis and duration/session of HD among HD patients who had hepatitis in HD center, Jakarta, Indonesia, and Penang, Malaysia. Hepatitis patients who underwent HD in Malaysia had a greater survival rate compared with that of the Indonesian patients.
Figure 2.
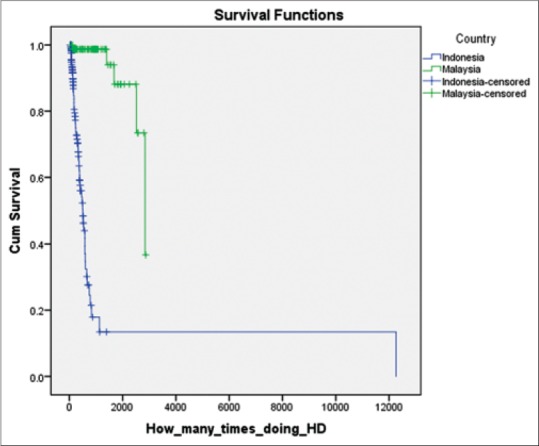
Survival analysis of hepatitis patients based on the duration/session of hemodialysis among hemodialysis patients who had been followed up for 9 months in a hemodialysis center, Jakarta, Indonesia, and in a hemodialysis center, Penang, Malaysia
DISCUSSION
There were two types of data which had been collected from each of the HD centers in Jakarta, Indonesia, and Penang, Malaysia. Retrospective samples were done by taking data of HD patients who had died in the last 5 years and prospective samples were collected by following and evaluating HD patients for 9 months in both countries Table 2. The patients who were included in this study were diabetic and/or hypertensive patients who underwent HD because diabetes and hypertension are the main causes of HD.[5,6]
The 2002 EBPG and the ERBP workgroup considers isolation of positive patients in HD centers with a high HCV patients, although KDIGO workgroup concluded that the isolation of HCV-infected patients is not recommended and the use of dedicated dialysis machines for HCV-infected patients is also not recommended.[7]
From this study, there were no special HD rooms and machines for HD patients who had hepatitis C in a HD center, Jakarta, Indonesia, and thus an increase was observed in the patient's number who had hepatitis C upon second follow up. These patients mixed with the other HD patients who did not have hepatitis C. In this HD center, special HD rooms and machines were only for HD patients who had hepatitis B and HIV infection.
The impact of this mixing was the reduction of the month's life since initiating HD, while the biggest number of patients who had liver infection (hepatitis) had a month's life of 13–48 months since initiating HD. This was in contrast to the clinical pattern in a HD center Penang, Malaysia, in which the patients were located according to the type of infection and this HD center did not mix the HD patients who had hepatitis infection and those who did not have. Also there were special HD rooms and machines for hepatitis B and hepatitis C HD patients.
Some laboratory values that can help to know the progression of the hepatitis infection are alkaline phosphatase, alanine transaminase (ALT), SGPT, and SGOT [8,9]. ALT and aspartate transaminase (AST) are used as the determinants for the liver diseases.[10] Especially, ALT is the most reliable biochemical value to indicate the injury of hepatocytes. The level of ALT shows greater increase than AST in the hepatic cells at the low level damage to hepatocytes.[10]
Blood transfusion was also found to be a factor, which contributed to the high hepatitis incident in a HD center, Indonesia. Blood transfusion was given to hemodialyzed patients who had hemoglobin <8 mg/dl. Knudsen et al. reported a statistically significant difference in the number of blood transfusions between anti-HCV-positive and indeterminate patients compared with anti-HCV-negative patients (30 vs. 13 transfusions, P < 0.005).[11]
For survival of HD patients who had hepatitis, Kalantar et al. study identified the association of hepatitis C and death risk among HD patients.[12] Due to that, the significant relationship between hepatitis C and death risk among HD patients is possible. From Kaplan–Meier analysis, it has been known that survival percentage in a HD center, Penang, Malaysia, is higher than that in Jakarta, Indonesia, as shown in Figure 1.
CONCLUSION
Besides providing special HD rooms and machines for HD patients with hepatitis C, minimizing blood transfusion to the patients on HD is important to reduce the chance for the patients to get hepatitis C and to increase the percentage of survival.
Financial support and sponsorship
The study was not funded or supported by any organization or institution.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We would like to thank to Prof. Dr. Markum and dr. Ihsanil Husna, Sp.PD (Cempaka Putih Islamic Hospital Jakarta) and Dato' Dr Ong Loke Meng (Hospital Pulau Pinang) for all their support in this research. Our gratitude to IPS USM.
REFERENCES
- 1.National Kidney Foundation. Update of the KDOQI ™ Clinical Practice Guideline for Hemodialysis Adequacy. 2015. [DOI] [PubMed]
- 2.Papatheodoridis G, Hatzakis A. Public health issues of hepatitis C virus infection. Best Pract Res Clin Gastroenterol. 2012;26:371–80. doi: 10.1016/j.bpg.2012.09.012. [DOI] [PubMed] [Google Scholar]
- 3.Liu YB, Xie JZ, Zhong CJ, Liu K. Hepatitis C virus infection among hemodialysis patients in Asia: A meta-analysis. Eur Rev Med Pharmacol Sci. 2014;18:3174–82. [PubMed] [Google Scholar]
- 4.Heemann U, Abramowicz D, Spasovski G, Vanholder R. European Renal Best Practice Work Group on Kidney Transplantation. Endorsement of the Kidney Disease Improving Global Outcomes (KDIGO) guidelines on kidney transplantation: A European Renal Best Practice (ERBP) position statement. Nephrol Dial Transplant. 2011;26:2099–106. doi: 10.1093/ndt/gfr169. [DOI] [PubMed] [Google Scholar]
- 5.Ghaderian SB, Hayati F, Shayanpour S, Beladi Mousavi SS. Diabetes and end-stage renal disease; a review article on new concepts. J Renal Inj Prev. 2015;4:28–33. doi: 10.12861/jrip.2015.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lea JP, Nicholas SB. Diabetes mellitus and hypertension: Key risk factors for kidney disease. J Natl Med Assoc. 2002;94:7S–15S. [PMC free article] [PubMed] [Google Scholar]
- 7.Covic A, Abramowicz D, Bruchfeld A, Leroux-Roels G, Samuel D, et al. Endorsement of the Kidney Disease Improving Global Outcomes (KDIGO) guidelines on kidney transplantation: A European Renal Best Practice (ERBP) position statement. Nephrol Dial Transplant. 2009;24:719–27. doi: 10.1093/ndt/gfn608. [DOI] [PubMed] [Google Scholar]
- 8.Marry Anne KK, Alledredge BK. Wolters Kluwer Health. Lipincott: Williams & Walkins; 2013. Koda-Kimble and Young's Applied Therapeutics: The Clinical Use of Drugs. [Google Scholar]
- 9.Kidney Disease Improving Global Outcomes. Clinical practice guideline for anemia in chronic kidney disease KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Int Suppl. 2012;2(4):279–335. [Google Scholar]
- 10.Önlen Y, Savaş L, Özer B, İris NE. The elevation of liver enzymes due to hepatitis B. Eur J Gen Med. 2006;3:197–200. [Google Scholar]
- 11.Knudsen F, Wantzin P, Rasmussen K, Ladefoged SD, Løkkegaard N, Rasmussen LS, et al. Hepatitis C in dialysis patients: Relationship to blood transfusions, dialysis and liver disease. Kidney Int. 1993;43:1353–6. doi: 10.1038/ki.1993.190. [DOI] [PubMed] [Google Scholar]
- 12.Kalantar-Zadeh K, Kilpatrick RD, McAllister CJ, Miller LG, Daar ES, Gjertson DW, et al. Hepatitis C virus and death risk in hemodialysis patients. J Am Soc Nephrol. 2007;18:1584–93. doi: 10.1681/ASN.2006070736. [DOI] [PubMed] [Google Scholar]