

Abstract
Background
The incidence of community-acquired pneumonia and lower respiratory tract infection rises considerably in later life. Immunoglobulin M (IgM) antibody levels to pneumococcal capsular polysaccharide are known to decrease with age; however, whether levels of IgM antibody to pneumococcal proteins are subject to the same decline has not yet been investigated.
Methods
This study measured serum levels and binding capacity of IgM antibody specific to the pneumococcal surface protein A (PspA) and an unencapsulated pneumococcal strain in serum isolated from hospital patients aged < 60 and ≥ 60, with and without lower respiratory tract infection. A group of young healthy volunteers was used as a comparator to represent adults at very low risk of pneumococcal pneumonia. IgM serum antibody levels were measured by enzyme-linked immunosorbent assay (ELISA) and flow cytometry was performed to assess IgM binding capacity. Linear regression and one-way analysis of variance (ANOVA) tests were used to analyse the results.
Results
Levels and binding capacity of IgM antibody to PspA and the unencapsulated pneumococcal strain were unchanged with age.
Conclusions
These findings suggest that protein-based pneumococcal vaccines may provide protective immunity in the elderly.
Trial registration
The LRTI trial (LRTI and control groups) was approved by the National Health Service Research Ethics Committee in October 2013 (12/NW/0713). Recruitment opened in January 2013 and was completed in July 2013. Healthy volunteer samples were taken from the EHPC dose-ranging and reproducibility trial, approved by the same Research Ethics Committee in October 2011 (11/NW/0592). Recruitment for this study ran from October 2011 until December 2012. LRTI trial: (NCT01861184), EHPC dose-ranging and reproducibility trial: (ISRCTN85403723).
Keywords: IgM antibodies, Pneumococcus, Vaccines, Immune senescence, Proteins
Background
Community-acquired pneumonia (CAP) has an incidence of 5–11 per 1000 adult population [1, 2], with an associated mortality between 5 and 20%, increasing to 50% in cases admitted to the intensive care unit [3]. The most common cause of CAP is Streptococcus pneumoniae [4]. Eighty per cent of CAP occurs in people ≥60 years [5–7], and this has been attributed to immune senescence, impairment of protective airway reflexes [8], reduced airway mucociliary clearance [9, 10] and alterations in respiratory tract immune function [11, 12]. Polysaccharide-based vaccines are recommended for older adults: the pneumococcal conjugate vaccine (PCV) is now licensed for adults over the age of 50 in the United States (US) and the pneumococcal polysaccharide vaccine (PPV) is recommended to people over 65 years of age in the United Kingdom (UK). However, the true levels of protection conferred by these vaccines in older adults are unclear [13–16]. They also have significant short-comings with regards to limited pneumococcal serotype coverage. Protein-based vaccines are being investigated as alternative immunization strategies, on the basis that they could provide full serotype coverage by targeting conserved proteins. As immunogenicity in vivo will depend on exposure to the host immune system, surface-expressed proteins are obvious potential vaccine candidates.
The protective role of antibody responses to pneumococcal infection is well described. IgM antibodies are the first class of antibodies to be produced in a primary response to microbial challenge. Although they bind with low affinity they exhibit a broad specificity to a variety of antigens [17]. Murine models have demonstrated that the passive transfer of IgM antibodies targeting pneumococcal polysaccharides can improve survival following a lethal pneumococcal challenge, suggesting that IgM antibody may be sufficient to confer protection against pneumococcal disease [18]. The therapeutic potential of an immunoglobulin preparation enriched with IgM for the treatment of severe CAP is under investigation [19]. Levels of antibodies to pneumococcal polysaccharides decline with aging, with IgM levels being more affected than the IgG subclass [20–22]. Levels of IgG to several pneumococcal protein antigens are also reduced in the elderly [22].
Pneumococcal surface protein A (PspA) is a major and well characterized virulence factor of the pneumococcus. Antibodies directed against PspA augment C3 deposition, and immunization with PspA confers protection to a variety of murine infection models [23, 24]. PspA is expressed in the majority of clinically important pneumococcal serotypes [25] and clade 4 in particular exhibits broad cross reactivity [26], allowing for sensitive detection of anti-PspA antibodies.
Despite evidence that IgM antibodies may play a role in anti-pneumococcal defence, and that IgG antibodies to pneumococcal proteins have protective potential, the impact of age on levels of IgM antibodies to pneumococcal proteins in humans has not been investigated. This study seeks to address this knowledge gap by investigating changes in levels and function of IgM antibodies against pneumococcal proteins in relation to aging and lower respiratory tract infection (LRTI) using the PspA clade 4 (PspA4) and an unencapsulated pneumococcal strain. It was hypothesised that as subjects age, levels and binding capacity of IgM antibodies against pneumococcal proteins in serum would be impaired and that patients hospitalized with LRTI would have lower IgM levels and functionality when compared to controls.
Methods
Study subjects
Serum samples used in this study were collected as part of two clinical trials, both of which have already had their primary end-points reported elsewhere: the LRTI trial [27] and the dose-ranging trial [28]. The volunteers can be separated into three cohorts: LRTI, control (both from the LRTI trial) and healthy (taken from the dose-ranging trial).
The LRTI cohort consisted of patients with a diagnosis of LRTI, based on presentation with symptoms of respiratory infection with ≥2 of the following clinical signs: “cough, breathlessness, pleuritic chest pain, fever and increased or new sputum production” [27]. Without additional radiological consolidation, LRTI patients cannot be considered to have CAP, but this broader cohort was chosen because of its clinical relevance in the UK hospitals setting [27].
The control cohort comprised patients admitted to hospital for reasons other than LRTI. They had no respiratory symptoms, and were age- and gender-matched to the LRTI patients.
The healthy cohort was formed of healthy volunteers aged 18–60 with no concurrent co-morbidities.
Sample collection
Nasal washes and serum samples were taken from LRTI and control group volunteers within 3 days of hospital admission. Baseline nasal washes and serum samples were taken from healthy volunteers by appointment.
Nasal washes were processed as described previously [27, 28] and used to determine pneumococcal carriage status and density by classical microbiology and by lytA qPCR. Urine from LRTI and control volunteers was collected to perform the BinaxNOW (Alere International Ltd., Ireland) (urine chromatography) test.
Bacterial strains
An unencapsulated D39 strain with deleted cpsD (D39-D∆) [29] (donated by Professor Jeremy S. Brown, University College, London) was cultured in Todd-Hewitt broth with 0.5% yeast extract (THY) until the mid-log phase. Bacteria was then pelleted, washed in phosphate buffered saline (PBS) and either used for whole cell ELISA (WCE) or resuspended in THY+ 20% glycerol and stored at − 80 °C for later use in an immunoglobulin binding assay.
Enzyme-linked immunosorbent assay (ELISA)
ELISA was used to quantify levels of IgM antibodies in the serum samples as previously described [30]. Briefly, 96-well plates (Nunc, Denmark) were coated with carbonate/bicarbonate buffer containing capture antigens/antibodies. The capture antigens/antibodies included 1 μg/ml recombinant PspA4 (kindly donated by Dr. Eliane Miyaji, Butantan Institute, Sao Paulo, Brazil), the non-encapsulated D39-D∆ pneumococcal strain and anti-human IgM μ chain-specific antibody (I2386, Sigma-Aldrich, St Louis, Missouri, USA).
Plates were washed then blocked with 1% bovine serum albumin(BSA)-PBS before adding serial dilutions of serum samples. Standard curves for calculating total IgM were made using purified total IgM from serum (I8260, Sigma-Aldrich, USA) at a level of 1 mg/ml. WCE and anti-PspA4 values were based on a standard pool serum with an IgM level of 4000 arbitrary units/μl (donated by Prof David Briles, University of Alabama).
IgM was bound to a goat anti-human IgM polyclonal antibody conjugated to biotin (Abcam, Cambridge, UK). The conjugate was quantified by streptavidin-alkaline phosphatase (Bio-Rad Laboratories, Hemel Hempstead, UK) using 4-Nitrophenyl phosphate disodium salt hexahydrate (N9389, Sigma-Aldrich, USA) as the substrate for development. Absorbance at 405 nm wavelength was determined using the Fluostar Omega® (BMG Labtech, Ortenberg, Germany) plate reader. A standard curve was fitted using a 4-parameter fit model.
Flow cytometry
Immunoglobulin deposition on whole live unencapsulated pneumococci was assayed using a modification of a published flow cytometry assay [31]. Briefly, D39-DΔ resuspended in THY + 20% glycerol was grown to mid-log phase in THY media with erythromycin, before two cycles of washing with PBS. Serum from patient groups was pooled and diluted in PBS at ratios of 1:2 and 1:20. Fixed volumes of the bacterial suspension were washed and resuspended in 100 μl of pooled serum before incubation for 30 min at 37 °C. Samples were pelleted, resuspended in IgM-PE-Cy5 (Clone G20–127, BD Biosciences, Franklin Lake, NJ, USA) and incubated for 20 min at 37 °C. Bacteria were washed and the level of IgM binding measured by flow cytometry using a BD LSR II (BD Biosciences, New Jersey, USA). The level of binding was calculated as the percentage of the bacterial population positive for IgM deposition multiplied by the geometric mean fluorescence of the bacterial population positive for IgM.
Statistical analysis
Linear regression analysis was used to correlate levels of antibodies with age. Antibody levels were log transformed to obtain normal distribution then analysed by one-way ANOVA with the Bonferroni correction to compare levels between the three groups. Analyses were performed using GraphPad Prism v5 (GraphPad Inc., California, USA) and significance was set at p < 0.05.
Results
Clinical trials
Overall, 38 hospital inpatients were enrolled in the LRTI trial, equally divided between patients with a diagnosis of LRTI (n = 19) and controls (n = 19). All LRTI patients, and 3 control patients, had been treated with antibiotics before recruitment to this study [27]. However, none of the control patients presented with a symptomatic infection. 10 volunteers were chosen from the dose-ranging study to be included in this analysis as healthy volunteers.
Table 1 outlines cohort characteristics. The mean age for LRTI patients was 64.5 years ±15.8 and 64.6 years ±14.5 for the control group. The mean age of the healthy group was 21.2 years ±2.4. A similar percentage of volunteers were female in all three cohorts: 53% for LRTI and control groups, and 50% for healthy volunteers. Risk factors for pneumococcal infection were recorded for both LRTI and control cohorts. Vaccination with PPV and contact with children was similar between both groups, whereas LRTI patients were more likely to be smokers, use corticosteroids and have COPD and/or asthma (Table 1).
Table 1.
Study population characteristics
| LRTI (n = 19) | Controls (n = 19) | Healthy volunteers (n = 10) | |
|---|---|---|---|
| Age (mean ± SD) (yr) | 64.5 (15.8) 10 (53) |
64.6 (14.5) 10 (53) |
21.2 (2.4) 5 (50) |
| Female gender (n [%]) | |||
| Smoker/ex-smoker (n [%]) | 15 (79) | 10 (53) | 0 (0) |
| PPV (n [%]) | 7 (37) | 8 (42) | 0 (0) |
| Contact with children (n [%]) | 10 (53) | 12 (63) | 0 (0) |
| Corticosteroid use (n [%]) | 16 (84) | 3 (16) | 0 (0) |
| COPD (n [%]) | 8 (42) | 2 (11) | 0 (0) |
| Asthmatic (n [%]) | 5 (26) | 1 (5) | 0 (0) |
COPD, chronic obstructive pulmonary disease; LRTI, lower respiratory tract infection; PPV, pneumococcal polysaccharide vaccine
Evidence was found of recent pneumococcal exposure in 50% (19/38) of the study’s patients, either by detection of pneumococcal nasal carriage or BinaxNOW (urine immunochromatography) test [27]. Of these, 11 belonged to the LRTI cohort. There was no significant difference in IgM antibody levels between pneumococcal carriers and non-carriers, nor was there any correlation between IgM antibody levels and carriage density by qPCR (data not shown).
Effect of age on immunoglobulin M antibody levels in serum
While the total levels of IgM trended to increase with increase of age (r2 = 0.15, p = 0.006) (Fig. 1a), no correlation was observed for levels of specific pneumococcal IgM antibody and age: D39-DΔ (r2 = 0.07, p = 0.05) and PspA4 (r2 = 0.005, p = 0.60) (Figs. 1b and c).
Fig. 1.
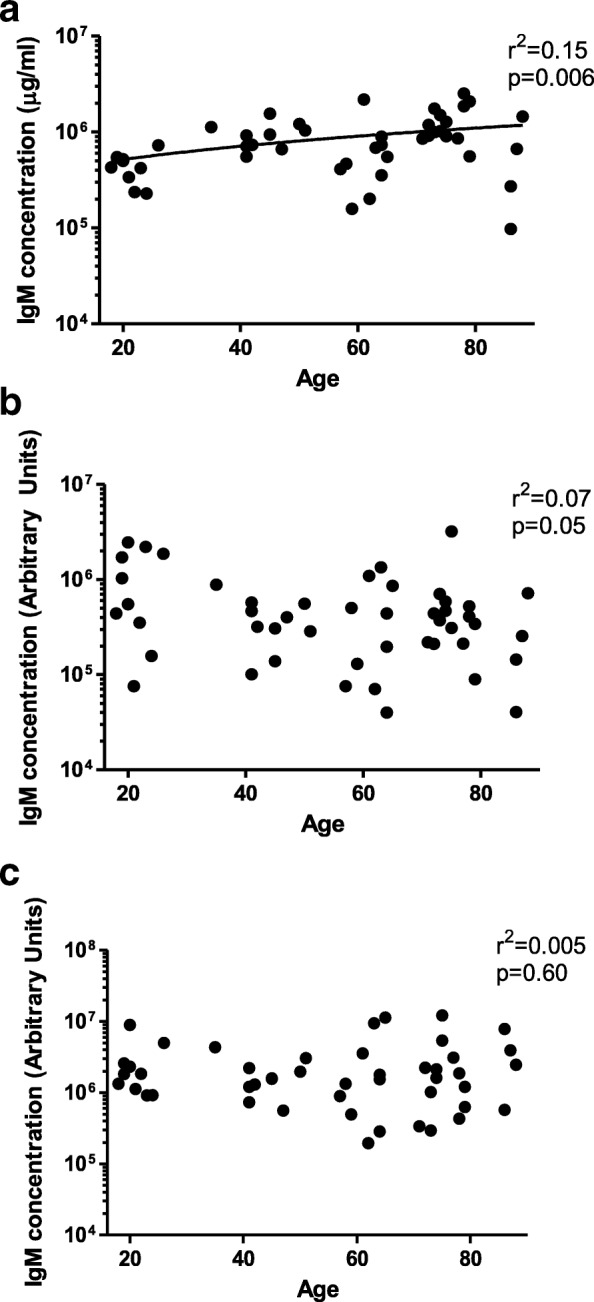
Levels of IgM in relation to age. Levels of (a) total IgM, (b) IgM to the unencapsulated D39-ΔD pneumococcus and to the (c) Pneumococcal Surface Protein A (PspA4) were plotted against volunteer age. Correlations were analysed using linear regression analysis
Effect of lower respiratory tract infection on immunoglobulin M levels
There was no difference in total IgM levels between LRTI and control groups. The LRTI group had higher levels of total IgM when compared to the healthy group (p = 0.01 for ANOVA analysis, p < 0.05 for the difference between LRTI and healthy groups) (Fig. 2a). No significant difference was observed in IgM antibody levels to D39-DΔ (p = 0.64 for ANOVA analysis) or to PspA4 (p = 0.14 for ANOVA analysis) between any of the groups (Figs. 2b and c).
Fig. 2.
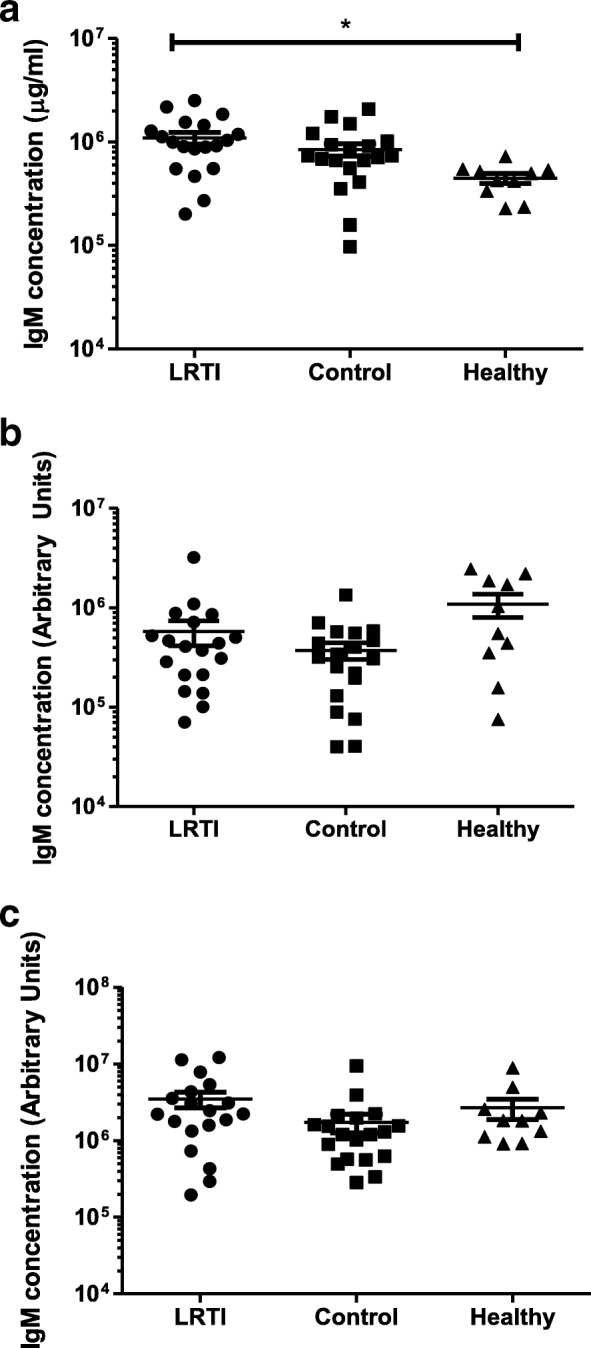
Levels of IgM in relation to LRTI. The level of total IgM was examined for patients with LRTI, hospital Controls and a young cohort of Healthy volunteers. Levels of (a) total IgM, (b) IgM to the unencapsulated D39-ΔD pneumococcus and to the (c) Pneumococcal Surface Protein A (PspA4) are shown. Mean values ± SD are shown. * p < 0.05 using ANOVA with Bonferroni’s correction
Immunoglobulin binding to whole-cell unencapsulated pneumococcus
The immunoglobulin binding assay was performed to assess changes in the binding capacity of IgM with aging and LRTI status. Sera from ≥60 control group showed no decrease in binding compared to younger volunteers from the healthy group (Figs. 3a and b). Contrary to the study’s initial hypothesis, the ≥60 LRTI group exhibited the highest level of IgM binding while the < 60 control group showed the lowest levels of binding.
Fig. 3.

Flow cytometric assessment of IgM binding to pneumococcus surface. Pooled sera from different volunteer groups were added to bacteria. Two experiments using different dilutions (1:2 and 1:20) of sera were performed. a Histogram of surface binding of IgM to intact pneumococcus D39-D∆. b Surface binding of IgM from pooled serum samples expressed as the percentage of the bacterial population positive for IgM deposition multiplied by the geometric mean fluorescence of the bacterial population positive for IgM
Discussion
These results demonstrate that the levels and binding capacity of IgM to pneumococcal proteins are unaltered with aging. Patients with LRTI did not show decreased IgM antibody to D39-DΔ or PspA4 compared to either the control or healthy groups. The study observed higher IgM binding to pneumococcus in a flow cytometry assay for sera from LRTI patients over 60 years.
High levels of total IgM in patients with LRTI cannot be an artefact of current infection, but rather of aging, because control patients without infection presented with similar total IgM levels, but the healthy group had significantly lower total IgM levels. Although only IgM antibodies against pneumococcal polysaccharides and proteins can be expected to confer protection against pneumococcal infection, it is nevertheless interesting to note that total IgM antibody levels are maintained despite immune senescence.
A study of IgM levels in mice found that total IgM levels were increased in older animals [32]. However, the authors found that anti-pneumococcal protein IgM antibody levels (as indicated by antibodies to phosphoryl choline, a pneumococcal cell wall antigen) dropped with age. This discrepancy with the present study’s data could be explained by the different choice of antigen or the limitation of animal models (which are immunologically naïve) to represent human responses (which are frequently re-challenged by in vivo exposure to pneumococcus through nasal carriage) [28]. IgM from older mice (18- or 24-month) was less protective against pneumococcal challenge when compared to younger mice (3-month) [32]. The present study showed, however, that IgM in adults over the age of 60 retains the ability to bind to non-encapsulated S. pneumoniae.
In whole-cell ELISA, in addition to surface protein antigens, cell wall antigens are also present, to which IgM binding may occur; however, whether these antibodies confer meaningful protection has been questioned [33, 34]. It has been suggested that bacterial autolysis during the overnight coating step releases internal antigens which would not in vivo be presented to the immune system [31]. Antibodies to these internal and cell wall antigens could conceivably lead to an overestimation of levels of IgM antibody against surface protein antigens. To address this issue, the study also used a flow cytometric approach to evaluate antibody binding to intact pneumococcus. Whereas cohort and age showed no impact on antibody levels measured by whole cell ELISA, differences were observed in antibody binding as assessed by flow cytometry. This discrepancy could be explained by bacterial rupture.
Limitations of this study include the small number of samples and the unknown etiology of LRTI of these patients. This study cohort also had significant heterogeneity with respect to many factors affecting immunoglobulin levels; for example, vaccination status, co-morbidities, corticosteroid treatment, and history of previous pneumococcal infection [27]. Furthermore, 12 of the LRTI patients received Clarithromycin prior to recruitment. The activities of 14-membered macrolide antibiotics are known to exert immunomodulatory effects [35] and this may have affected IgM responses to S.pneumoniae in this cohort.
Conclusions
In summary, these findings suggest that IgM antibodies against pneumococcal proteins do not decrease with age and this warrants further investigation into IgM antibodies against pneumococcal proteins and its role in immunity through pneumococcal protein vaccination.
Acknowledgements
The authors are grateful to Professor Jeremy S Brown (University College, London, UK), Dr. Eliane N Miyaji (Butantan Institutue, Sao Paulo, Brazil) and Professor David Briles (University of Alabama, Alabama, USA), for their generous contributions of D39-D∆ (JSB), recombinant PspA4 (ENM) and standard serum (DB). They also appreciate the helpful comments and advice provided by Dr. Jamie Rylance, Dr. Hugh Adler and Dr. Jesús Reiné (Liverpool School of Tropical Medicine, Liverpool, UK) upon review of the manuscript.
Funding
This work was financed by The Bill & Melinda Gates Foundation Grand Challenge Exploration programme, Medical Research Council/Sao Paulo Research Foundation bilateral agreement (MRC-FAPESP) and the Wellcome Trust. The researchers work entirely independently from the funders.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CAP
Community Acquired Pneumonia
- D39-D∆
Unencapsulated D39 strain with deleted cpsD
- LRTI
Lower Respiratory Tract Infection
- PBS
Phosphate Buffered Saline
- PCV
Pneumococcal Conjugate Vaccine
- PPV
Pneumococcal Polysaccharide Vaccine
- PspA
Pneumococcal surface protein A
- THY
Todd-Hewitt broth with 0.5% yeast extract
- WCE
Whole Cell ELISA
Authors’ contributions
The LRTI study was designed by AMC, ADHW, and SBG. Samples were collected by ADHW and processed by JFG and AB. The experiments were designed by BAH, DMF and SBG. Laboratory work was carried out by BAH and ELG with the assistance of AB, SHP (flow cytometry), JFG, and EM (ELISAs). Data was analysed and interpreted by BAH, SBG, DMF, EM and ELG. The manuscript was prepared for submission by BAH, ELG, SHP and DMF. The final version of the manuscript was approved by all authors prior to submission.
Ethics approval and consent to participate
The samples used for these experiments were taken from volunteers participating in studies approved by the North West-Liverpool East Research Ethics Committee (12/NW/0713 for LRTI and Control groups; 11/NW/0592 for the Healthy group). All studies were conducted in compliance with the Declaration of Helsinki and informed consent was gained prior to all samples being obtained.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Footnotes
Esther L. German and Bahij Al-Hakim contributed equally to this work.
Contributor Information
Esther L. German, Email: esther.german@lstmed.ac.uk
Bahij Al-Hakim, Email: bahijal-hakim@hotmail.co.uk.
Elena Mitsi, Email: Elena.mitsi@lstmed.ac.uk.
Shaun H. Pennington, Email: Shaun.Pennington@lstmed.ac.uk
Jenna F. Gritzfeld, Email: Jenna.Gritzfeld@phe.gov.uk
Angie D. Hyder-Wright, Email: Angela.Hyder-Wright@lstmed.ac.uk
Antonia Banyard, Email: Antonia.banyard@cruk.manchester.ac.uk.
Stephen B. Gordon, Email: sgordon@mlw.mw
Andrea M. Collins, Email: Andrea.Collins@lstmed.ac.uk
Daniela M. Ferreira, Email: Daniela.Ferreira@lstmed.ac.uk
References
- 1.Brar NK, Niederman MS. Management of community-acquired pneumonia: a review and update. Ther Adv Respir Dis. 2011;5:61–78. doi: 10.1177/1753465810381518. [DOI] [PubMed] [Google Scholar]
- 2.Levy ML, Jeune IL, Woodhead MA, Macfarlane JT, Lim WS. Primary care summary of the British Thoracic Society guidelines for the management of community acquired pneumonia in adults: 2009 update. Prim Care Respir J. 2010;19:21–27. doi: 10.4104/pcrj.2010.00014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Welte T, Köhnlein T. Global and local epidemiology of community-acquired pneumonia: the experience of the CAPNETZ network. Semin Respir Crit Care Med. 2009;30:127–135. doi: 10.1055/s-0029-1202941. [DOI] [PubMed] [Google Scholar]
- 4.van der Poll T, Opal SM. Pathogenesis, treatment, and prevention of pneumococcal pneumonia. Lancet. 2009;374:1543–1556. doi: 10.1016/S0140-6736(09)61114-4. [DOI] [PubMed] [Google Scholar]
- 5.Ewig S, Birkner N, Strauss R, Schaefer E, Pauletzki J, Bischoff H, Schraeder P, Welte T, Hoeffken G. New perspectives on community-acquired pneumonia in 388 406 patients. Results from a nationwide mandatory performance measurement programme in healthcare quality. Thorax. 2009;64:1062–1069. doi: 10.1136/thx.2008.109785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Millett ERC, Quint JK, Smeeth L, Daniel RM, Thomas SL. Incidence of community-acquired lower respiratory tract infections and pneumonia among older adults in the United Kingdom: a population-based study. PLoS One. 2013;8:e75131. doi: 10.1371/journal.pone.0075131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Sliedrecht A, den Elzen WPJ, Verheij TJM, Westendorp RGJ, Gussekloo J. Incidence and predictive factors of lower respiratory tract infections among the very elderly in the general population. The Leiden 85-plus study. Thorax. 2008;63:817–822. doi: 10.1136/thx.2007.093013. [DOI] [PubMed] [Google Scholar]
- 8.Yamaya M, Yanai M, Ohrui T, Arai H, Sasaki H. Interventions to prevent pneumonia among older adults. J Am Geriatr Soc. 2001;49:85–90. doi: 10.1046/j.1532-5415.2001.49015.x. [DOI] [PubMed] [Google Scholar]
- 9.Svartengren M, Falk R, Philipson K. Long-term clearance from small airways decreases with age. Eur Respir J. 2005;26:609–615. doi: 10.1183/09031936.05.00002105. [DOI] [PubMed] [Google Scholar]
- 10.Ho JC, Chan KN, Hu WH, Lam WK, Zheng L, Tipoe GL, Sun J, Leung R, Tsang KW. The effect of aging on nasal mucociliary clearance, beat frequency, and ultrastructure of respiratory cilia. Am J Respir Crit Care Med. 2001;163:983–988. doi: 10.1164/ajrccm.163.4.9909121. [DOI] [PubMed] [Google Scholar]
- 11.Meyer KC. The role of immunity in susceptibility to respiratory infection in the aging lung. Respir Physiol. 2001;128:23–31. doi: 10.1016/S0034-5687(01)00261-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Meyer KC. Aging. Proc Am Thorac Soc. 2005;2:433–439. doi: 10.1513/pats.200508-081JS. [DOI] [PubMed] [Google Scholar]
- 13.Jackson LA, Janoff EN. Pneumococcal vaccination of elderly adults: new paradigms for protection. Clin Infect Dis. 2008;47:1328–1338. doi: 10.1086/592691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bonten MJM, Huijts SM, Bolkenbaas M, Webber C, Patterson S, Gault S, van Werkhoven CH, van Deursen AMM, Sanders EAM, Verheij TJM, Patton M, McDonough A, Moradoghli-Haftvani A, Smith H, Mellelieu T, Pride MW, Crowther G, Schmoele-Thoma B, Scott DA, Jansen KU, Lobatto R, Oosterman B, Visser N, Caspers E, Smorenburg A, Emini EA, Gruber WC, Grobee DE. Polysaccharide conjugate vaccine against pneumococcal pneumonia in adults. N Engl J Med. 2015;372:1114–1125. doi: 10.1056/NEJMoa1408544. [DOI] [PubMed] [Google Scholar]
- 15.Huss A, Scott P, Stuck AE, Trotter C, Egger M. Efficacy of pneumococcal vaccination in adults: a meta-analysis. CMAJ. 2009;180:48–58. doi: 10.1503/cmaj.080734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.José RJ, Brown JS. Adult pneumococcal vaccination: advances, impact and unmet needs. Curr Opin Pulm Med. 2017;23(3):225–230. doi: 10.1097/MCP.0000000000000369. [DOI] [PubMed] [Google Scholar]
- 17.Boes M. Role of natural and immune IgM antibodies in immune responses. Mol Immunol. 2001;37:1141–1149. doi: 10.1016/S0161-5890(01)00025-6. [DOI] [PubMed] [Google Scholar]
- 18.Baxendale HE, Johnson M, Stephens RCM, Yuste J, Klein N, Brown JS, Goldblatt D. Natural human antibodies to pneumococcus have distinctive molecular characteristics and protect against pneumococcal disease. Clin Exp Immunol. 2008;51:51–60. doi: 10.1111/j.1365-2249.2007.03535.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Welte T, Dellinger RP, Ebelt H, Ferrer M, Opal SM, Schliephake DE, Wartenberg-Demand A, Werdan K, Löffler K, Torres A. Concept for a study design in patients with severe community-acquired pneumonia: a randomised controlled trial with a novel IGM-enriched immunoglobulin preparation – the CIGMA study. Respir Med. 2015;109:758–767. doi: 10.1016/j.rmed.2015.03.008. [DOI] [PubMed] [Google Scholar]
- 20.Shi Y, Yamazaki T, Okubo Y, Uehara Y, Sugane K, Agematsu K. Regulation of aged humoral immune defense against pneumococcal bacteria by IgM memory B cell. J Immunol. 2005;175:3262–3267. doi: 10.4049/jimmunol.175.5.3262. [DOI] [PubMed] [Google Scholar]
- 21.Leggat DJ, Thompson RS, Khaskhely NM, Iyer AS, Westerink MAJ. The immune response to pneumococcal polysaccharides 14 and 23F among elderly individuals consists predominantly of switched memory B cells. J Infect Dis. 2013;208(1):101–108. doi: 10.1093/infdis/jit139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Simell B, Lahdenkari M, Reunanen A, Käyhty H, Väkeväinen M. Effects of aging and gender on naturally acquired antibodies to pneumococcal capsular polysaccharides and virulence-associated proteins. Clin Vaccine Immunol. 2008;15:1391–1397. doi: 10.1128/CVI.00110-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ren B, Szalai AJ, Hollingshead SK, Briles DE. Effects of PspA and antibodies to PspA on activation and deposition of complement on the pneumococcal surface. Infect Immun. 2004;72:114–122. doi: 10.1128/IAI.72.1.114-122.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Wu HY, Nahm MH, Guo Y, Russell MW, Briles DE. Intranasal immunization of mice with PspA (pneumococcal surface protein a) can prevent lntranasal carriage, pulmonary infection, and sepsis with Streptococcus pneumoniae. J Infect Dis. 1997;175:839–846. doi: 10.1086/513980. [DOI] [PubMed] [Google Scholar]
- 25.Crain MJ, Waltman Ii WD, Turner JS, Yother J, Talkington DF, McDaniel LS, Gray BM, Briles DE. Pneumococcal surface protein a (PspA) is serologically highly variable and is expressed by all clinically important capsular serotypes of Streptococcus pneumoniae. Infect Immun. 1990;58:3293–3299. doi: 10.1128/iai.58.10.3293-3299.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Darrieux M, Moreno AT, Ferreira DM, Pimenta FC, De Andrade ALSS, Lopes APY, Leite LCC, Miyaji EN. Recognition of pneumococcal isolates by antisera raised against PspA fragments from different clades. J Med Microbiol. 2008;57:273–278. doi: 10.1099/jmm.0.47661-0. [DOI] [PubMed] [Google Scholar]
- 27.Collins AM, Johnstone CMK, Gritzfeld JF, Banyard A, Hancock CA, Wright AD, Macfarlane L, Ferreira DM, Gordon SB. Pneumococcal colonization rates in patients admitted to a United Kingdom hospital with lower respiratory tract infection: a prospective case-control study. J Clin Microbiol. 2016;54:944–949. doi: 10.1128/JCM.02008-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ferreira DM, Neill DR, Bangert M, Gritzfeld JF, Green N, Wright AK, Pennington SH, Bricio-Moreno L, Moreno AT, Miyaji EN, Wright AD, Collins AM, Goldblatt D, Kadioglu A, Gordon SB. Controlled human infection and rechallenge with Streptococcus pneumoniae reveals the protective efficacy of carriage in healthy adults. Am J Respir Crit Care Med. 2013;187(8):855–864. doi: 10.1164/rccm.201212-2277OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Morona JK, Miller DC, Morona R, Paton JC. The effect that mutations in the conserved capsular polysaccharide biosynthesis genes cpsA, cpsB, and cpsD have on virulence of Streptococcus pneumoniae. JID. 2004;189:1905–1913. doi: 10.1086/383352. [DOI] [PubMed] [Google Scholar]
- 30.Vadesilho CFM, Ferreira DM, Moreno AT, Chavez-Olortegui C, Machado de Avila RA, Oliveira MLS, Ho PL, Miyaji EN. Characterization of the antibody response elicited by immunization with pneumococcal surface protein a (PspA) as recombinant protein or DNA vaccine and analysis of protection against an intranasal lethal challenge with Streptococcus pneumoniae. Mic Path. 2012;53:243–249. doi: 10.1016/j.micpath.2012.08.007. [DOI] [PubMed] [Google Scholar]
- 31.Cohen JM, Wilson R, Shah P, Baxendale HE, Brown JS. Lack of cross-protection against invasive pneumonia caused by heterologous strains following murine Streptococcus pneumoniae nasopharyngeal colonisation despite whole cell ELISAs showing significant cross-reactive IgG. Vaccine. 2013;31(19):2328–2332. doi: 10.1016/j.vaccine.2013.03.013. [DOI] [PubMed] [Google Scholar]
- 32.Holodick NE, Vizconde T, Hopkins TJ, Rothstein TL. Age-related decline in natural IgM function: diversification and selection of the B-1a cell pool with age. J Immunol. 2016;196(10):4348–4357. doi: 10.4049/jimmunol.1600073. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Musher DM, Watson DA, Baughn RE. Does naturally acquired IgG antibody to cell wall polysaccharide protect human subjects against pneumococcal infection? J Infect Dis. 1990;161:736–740. doi: 10.1093/infdis/161.4.736. [DOI] [PubMed] [Google Scholar]
- 34.Nielsen SV, Skov Sorensen UB, henrichsen J. Antibodies against pneumococcal C-polysaccharide are not protective. Microb Pathog. 1993;14:299–305. doi: 10.1006/mpat.1993.1029. [DOI] [PubMed] [Google Scholar]
- 35.Kanoh S, Rubin BK. Mechanisms of action and clinical application of macrolides as immunomodulatory medications. Clin Microbiol Rev. 2010;23(3):590–615. doi: 10.1128/CMR.00078-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.