

Abstract
Introduction
The skin undergoes morphological and physiological changes with the advancing age of an individual. These changes may be caused by intrinsic and extrinsic factors that contribute to cellular ageing and consequent skin ageing. The term photoageing is used to characterise the ageing of the skin caused by solar radiation. Clinically, the skin becomes more flaccid, thicker and hyperpigmented, while there is an early appearance of wrinkles and other skin changes, such as skin cancer. Nowadays, there are numerous treatments for ageing skin, and one of them is with the use of phototherapy, which uses light-emitting diodes (LEDs). The objective of this study will be to evaluate the percentages of reduction in the volume of periocular wrinkles when treated with red and amber LEDs.
Methods and analysis
All of the participants will receive photobiomodulation to treat their periocular wrinkles. They will be using red and amber LEDs, with one colour being used on each hemiface. The facial side to be treated with each colour will be randomised. After an interval of 180 days, the participants will receive a cross-treatment. The primary variable of the study is the volume of periocular wrinkles (crow’s feet), which will be measured by a VisioFace equipment. The secondary variables are elasticity (measured by Cutometer) and hydration (measured by Corneometer). Quality of life and self-assessment of the participants will be measured using the adapted Melasma Quality of Life scale - Brazilian Portuguese adaption (MelasQoL-BP) and Skindex-29 questionnaires. All of the variables will be measured before and after a group of 10 sessions.
Ethics and dissemination
This protocol was approved by the Research Ethics Committee of the Nove de Julho University (acceptance number: 2.550.732). This trial has been registered in the Registro Brasileiro de Ensaios Clínicos (Brazilian Clinical Trials Registry) (REBEC number: RBR-6YFCBM). This study is not recruiting yet.
Trial registration number
RBR6YFCBM; Pre-results.
Keywords: skin aging, wrinkles, phototherapy, photobiomodulation, photodermatology
Strengths and limitations of this study.
Each woman participating in this study will be evaluated before and after the treatment, and the reduction in wrinkles will be measured.
There is no control or placebo group and all of the participants will be treated; in this sense, each participant is in both the treatment group and the control group.
This split-face study will eliminate the individual factors of each participant that affect treatment outcomes.
The VisioFace equipment will standardise the parameters in acquiring photographs, such as light exposure, and it will minimise bias.
The habits of the participants may affect the results, as a consequence of their diet, their use of cosmetics and their exposure to the sun.
Introduction
The skin covers the body and has essential functions in maintaining the homeostasis of an organism, presenting roles such as defence, thermoregulation and sensory awareness. Maintenance of healthy skin and integrity is extremely important.1 Exposure to the sun speeds up the intrinsic ageing of the skin, due to the formation of free radicals and reactive oxygen species, as a result of ultraviolet (UV) radiation.1 Once UVA radiation penetrates deeper into the dermis, the resulting oxidative stress causes damage to the elastin fibres and collagen. In addition, there may occur a decrement in physiological antioxidant reserves and/or in the protective capacity of the skin.2 The changes that are caused by ageing modify the physical properties of the skin, leaving visible signs such as epidermal hyperplasia, irregular pigmentation, telangiectasia, sagging tissues, a reduction of collagen and elastin fibres, as well as a decrement in the natural moisturising factor. These changes result in the appearance of expression lines and creases.3 4
Recent data from the Brazilian Institute of Geography and Statistics (IBGE) have shown that the average life expectancy of the Brazilian population has increased from 66 years in 1991 to 75 years in 2016. This is similar to the increase that has been verified on worldwide population. The challenge faced by science in the last few years has been the development of procedures and technologies that aim to delay the signs of ageing and increase the quality of life of elderly people, by achieving a healthy skin.5 Nowadays, the procedures in use aim to promote a cosmetic benefit and an improvement in the quality of the skin, increasing self-esteem, with a reduction in skin infections. As a result, these procedures can contribute to a longer and healthier life. Among the technologies being used to promote skin repair are dermocosmetics, as well as equipment such as radiofrequency, phototherapy (intense pulsed light, laser and light-emitting diodes (LEDs)) and microneedles.6–9
Phototherapy is a non-invasive procedure that has been used for tissue repair and healing.10 11 The treatment is based on the use of a light-emitting device, and the resulting photons are absorbed by the biological tissues, promoting photochemical, photophysical and photobiological actions. Phototherapy is not ablative, nor does it promote thermal effects, since the devices that are used in phototherapy are low-powered lasers and LEDs; that is, there is no cutaneous damage and no need for any recovery time.12 The LED devices are produced in a wide range of wavelengths, from UV through the visible to infrared spectrum (247–1300 nm). When compared with laser, the LED devices have lower cost and have being used in instruments that can illuminate larger surfaces. Studies have shown that LEDs can be used in therapeutic procedures with excellent results.10 13 14 The use of LEDs in clinical practice has increased significantly, and their main use has been in wound healing, tissue repair and rejuvenation since they do not cause trauma or tissue destruction.15 Some findings have suggested that if suitable parameters are used, the light acts on skin regeneration by modulating cellular activity and collagen expression, with a decrease in matrix metalloproteinases.16 Usually, the wavelengths are chosen by the function that is needed for the purpose of the therapy. The wavelengths in the blue range (400–470 nm) are mainly used in the treatment of acne.17 The wavelengths in the green range (500–570 nm) have shown their ability to induce proliferation of fibroblasts, as well as production and maturation of the collagen fibres.18 19 The infrared range (700–1200 nm) accelerates the healing process of lesions in the skin, increases proliferation of cell differentiation, as well as contributes to an increase in the extracellular matrix.20 21
Many in vitro, in vivo and clinical studies have demonstrated the anti-inflammatory, repair, skin rejuvenation and healing effects that are promoted by red light.11 22 For an amber light, a study that was published by Smith23 in 2005 showed that it is absorbed by keratinocytes, melanocytes, as well as for the cells of Merkel and Langerhans, which are all of extreme importance in the maintenance of the epidermis. Both of these wavelengths are absorbed by cytochrome c oxidase; however, it is considered that the red light penetrates deeper into the skin than the amber light due to the presence of melanin.24–26 Given this background, this work will aim to evaluate the percentages of reduction in the volume of periocular wrinkles when treated with red and amber LEDs.
Methods and analysis
Study design
This will be a controlled, randomised, double-blind, split-face, cross-over and unicentric clinical trial. This protocol has been written based on the guidelines of the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT). The study will be performed in the ambulatory of the Nove de Julho University (UNINOVE), São Paulo, Brazil. Dissemination and registration for participation in the study will be conducted through the UNINOVE website, and the recruited participants will mainly be residents of the city of São Paulo. The participants will be informed about the research, procedures, risks and benefits, and they will sign the informed consent form. Only those participants who have read and have agreed to sign the informed consent form will be included in the study. The study will last for 2 years, with a start date of May 2018. The study is not recruiting yet.
After recruitment, the researcher will check if the patient meets the inclusion/exclusion criteria based on anamnesis and skin evaluation. Anamnesis is an interview performed by the health professional to know patients’ medical and aesthetics treatment history, as well as daily personal and social habits, which may have an influence on treatment outcome. Regarding the daily personal and social habits, anamnesis will include information on sun exposure, smoking and drinking frequency, sleep quality, dietary habits, water intake, professional aesthetics treatment on the face and homecare cosmetics use. Anamnesis was not validated since it is not an instrument to measure patient outcome.27 Skin evaluation, which will be performed by a medical doctor (IdSD), includes skin phototype and degree of severity of the wrinkles. Patients will receive information on the importance of the use of sunscreen on skin health, preventing skin cancer and wrinkles.
Patient and public involvement statement
Patients and/or the public were not involved in the design, recruitment to and conduct of the study.
Inclusion criteria
This study will be conducted in women (40–65 years old) with skin phototypes II, III and IV on the Fitzpatrick Scale, and with signs of ageing III and IV on the Glogau Scale.
Exclusion criteria
This study will exclude the following participants:
With thyroid disorders (hyperthyroidism or hypothyroidism) and who are not undertaking the due treatment, or those who have been taking the medications for less than 1 year.
Who have received a facial filling in the last 12 months.
Who are doing any facial aesthetic procedure.
Who are using retinoic acid or any vitamin A derivative (tretinoin or isotretinoin, topical or oral).
Who are using cosmetics or medications that may increase the photosensitivity of the skin.
Who present any pathology of the skin, such as acne, psoriasis, vitiligo and so forth.
Who present big laterality of skin ageing.
Professional drivers.
Who have undergone bariatric surgery or who are confined to a strict diet.
Who are using any supplement (topic or oral) for the improvement of their skin condition.
Who are pregnant or lactating.
Who are not regular attendees of treatments.
Sample size calculation
A pilot study with 10 patients was performed to generate the data for the sample size calculation. All of the participants of this pilot study signed the informed consent form. The largest and the smallest values of the percentages of reduction in the volume of the wrinkles for each treatment were obtained, as well as for the Standard deviation (SD) of the measurements. The worst-case scenarios were used for this calculation. The smallest and the largest values were 95 and 5, respectively; the highest SD was 29 and the number of treatment groups was 2. These values were used for the calculation of the effect size, as follows:
By using the effect size value as calculated above, t-tests were used to evaluate the differences between the two dependent means (matched pairs); the test power was 80% and the one-tailed test was at 5%; and the sample size calculated by the G*Power software (V.3.1.9.2, Dusseldorf, Germany) was 137.
Randomisation
The equal randomisation will be performed by a researcher (ACRTH) who is not directly involved in the treatment of the participants. It will be generated on Excel 2013 software (Microsoft, USA). The opaque envelopes will be marked and identified by sequential numbers, and each envelope will have a paper containing the information on which particular treatment will be performed on the right hemiface of the participant, in accordance with the draw. These envelopes will be sealed and securely stored in a safe place, with utmost confidentiality, by the same researcher who generated the randomisation. Immediately before the treatments, the researcher responsible for the treatment will receive the envelope, in sequence, and will then perform the indicated procedure.
Interventions
All of the participants will have their faces cleaned with a neutral cleansing soap and receive eye protection, followed by the LED application. The participants will have their eyes protected by goggles, in order to safely allow the illumination of their periocular region. This will also make the study blind, so that they do not know which wavelength is being applied to each hemiface. The application of phototherapy and the measurement of the parameters will be performed by ICSSR. Thus, this protocol will be a double-blind study.
All of the participants will receive photobiomodulation to treat their periocular wrinkles, using red and amber LEDs, with one colour only at each hemiface. The facial side to be treated with each different colour will be randomised. Group A will receive a red LED on the right side of their face and an amber LED on the left side of their face; group B will receive a red LED on the left side of their face and an amber LED on the right side of their face. For both of the groups, the session will last for 10 min (3.8 J/cm² at each wavelength), and the complete treatment will be composed of 10 sessions, 2–3 sessions per week, within 1 month. After a period of 180 days, the cross-over treatment will be performed: the participants in group A will receive the application of an amber LED on their right hemiface and a red LED on their left hemiface, while group B participants will receive a treatment with a red LED on their right hemiface and an amber LED on their left hemiface. As performed in the first part of the study, both of the groups will have 10 min of exposure per session (5.4 J/cm² at each wavelength), with a complete treatment of 10 sessions, performed 2–3 sessions per week, within 1 month. All of the variables will be measured before and after a group of 10 sessions. This procedure will be conducted for each hemiface. This second group of data can inform if the effects of the first treatment would disappear after the washout period and if the clinical response to the second treatment would be different from the first one. The participants may not receive any other facial aesthetic procedure or any supplement (topic or oral) for the improvement of their skin condition during the development of this study.
Variables of the study
The primary outcome of the study is the volume of wrinkles in the periocular region. The secondary outcomes are elasticity/sagging, hydration, melanin/spots, quality of life and self-assessment by the participants.
Volume of wrinkles in the periocular region and the melanin spots
For measurements of the primary variable, VisioFace RD (CK Electronic, Cologne, Germany) equipment will be used. This apparatus has a digital camera with white diode illumination that will record a standardised photograph of each participant’s face. Through a computer program, parameters will be determined that will indicate the volume of wrinkles in the periocular region, which is commonly known as crow’s feet.
Elasticity/Sagging
Other non-invasive measurements of the facial region will also be performed. The viscoelasticity of the skin will be evaluated in the periocular region by Cutometer Dual MPA 580 (CK Electronic) instrumentation. Cutaneous elasticity is an important parameter because it provides indirect information on the quality and quantity of collagen and elastic fibres (structural fibres) that are degraded by the metalloproteinases. It is known that photoaged skin presents disorganised elastin and decreased collagen fibres.28
Hydration
Skin hydration will be evaluated by a Corneometer CM 825 (CK Electronic) probe. This parameter is related to the amount of water in the dermis and epidermis, which allows for suitable skin functions.29
Quality of life and self-assessment by the participants
The participants will respond to the quality of life and self-assessment questionnaires. An interview of around 20 min will be enough to get all of the participants’ answers. In terms of the quality of life, two adapted questionnaires will be applied. First, an adaptation of the questionnaire for the quality of life of participants with dermatological diseases will be used (Skindex-29).30 The second is the adapted version of the Melasma Quality of Life scale - Brazilian Portuguese adaption (MelasQoL-BP) questionnaire.31 Due to these adaptations, the questionnaires will be evaluated in terms of reproducibility and internal consistency. For this, 20 participants, external to the main research, will respond to the questionnaires twice, with an interval of 30 days between answers. Statistical analyses will then be conducted. These particular participants will be duly informed about the research and, if they agree to participate in the study, they will sign the terms of free and informed consent. The rhytidectomy outcome evaluation questionnaire will be performed before and after the phototherapy treatments for the verification of the self-assessment by participants.32
All of the measurements will be performed by LRM, who was previously trained by the CK Electronic’s representative in Brazil. The VisioFace equipment has standardised illumination and face positioning in order to minimise any experimental bias. The questionnaires will be applied by LRM. The data that will be collected from this study will be managed only by the principal investigators (authors of this paper). The data will be saved on the university computer, protected by a password.
The complete study timeline is presented in figure 1.
Figure 1.
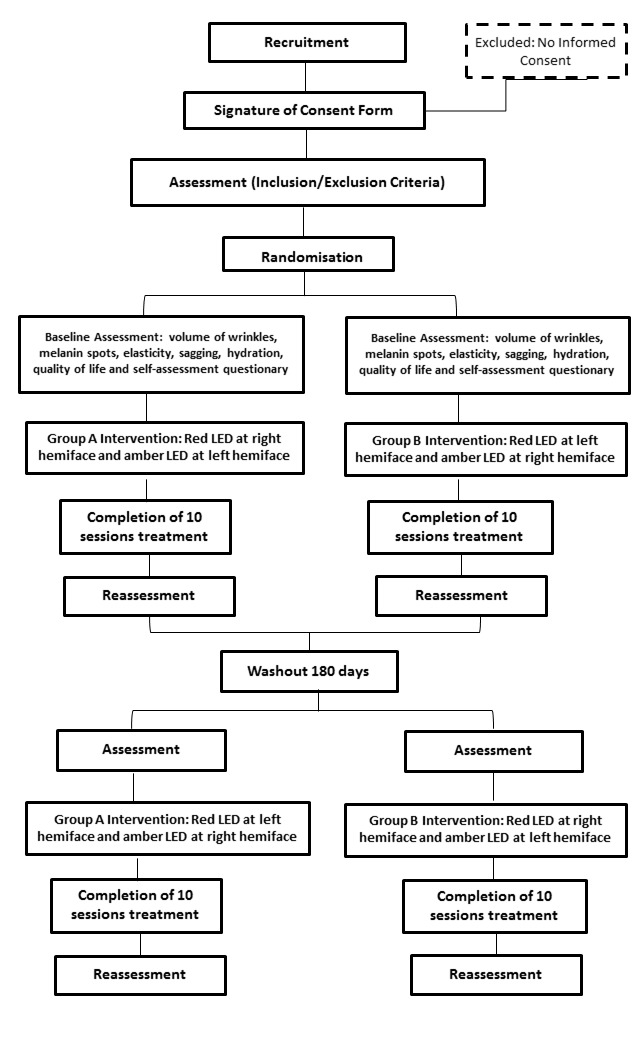
Study timeline. LED, light-emitting diode.
Statistical analyses and data analyses plan
The Shapiro-Wilk test will be used to test for normality of data. If the data are non-parametric, the normalisation will be performed by a math strategy. Student’s t-test for dependent variables will be used for inferential analyses. A p value <0.05 will be considered statistically significant. DdFTdS will perform all the statistical analyses.
Discussion
Photobiomodulation has been extensively studied for wound healing in the medical literature, showing good results.33–35 The effect is related to the increased proliferation of dermal fibroblasts, collagen synthesis, decrease of the inflammatory cells and formation of granulation tissue. The use of both LED and lasers has been considered effective.36 37 Recently, some studies proposed the use of phototherapy in aesthetics protocols for rejuvenation.15 38 However, it is still needed to optimise phototherapy parameters such as energy and the number of sessions.39
Despite the fact that phototherapy has been proposed as an interesting tool to reduce wrinkles, clinical trials evaluating any real effects are sparse.11 40 41 On this subject, this study’s protocol was designed to evaluate the reduction of wrinkles when using red or amber LED devices. This current work has described a study protocol for a unicentric randomised clinical trial based on the comparison of the two interventions. The study has been designed to optimise the obtainment of results and to minimise bias. First, the participants will be their own control, since the measurements are going to be accomplished before and after a series of 10 sessions of interventions. Second, by performing a split-face study, this will eliminate the individual factors of each participant that affect treatment outcomes. Pre-existing systemic pathologies, personal daily care and food intake, together with smoking and drinking habits, may affect the results obtained, and performing both treatments on each patient will make these factors influence the results equally for the two groups. In addition, if the application of phototherapy generates some systemic effects, it will have the same influence on the results of the two treatments. This has been carefully considered, since some studies have shown systemic effects of phototherapy.42 43 Third, it is known that melanin absorbs light in the visible and infrared region of the spectra. Thus, the results of the application of both LED, in red and amber, may be affected by the melanin content of the skin. In this sense, skin types II, III and IV were chosen as inclusion criteria to standardise the melanin content of the participants, excluding skin types with high melanin content (types V and VI) and lower melanin content (type I). Fourth, a double-blind study will reduce errors of bias due to the subconscious influence of the volunteers as well as the researchers on data acquisition. Finally, this randomisation will be performed in an equal way (ie, group A=group B); then in case of a patient’s withdrawal after the first randomisation, new inscriptions and a new randomisation can be generated, thus allowing the researchers to reach the desired number of patients for the study.
The aesthetics of the face may have positive or negative effects on the quality of life of patients, as well as on their self-esteem. Despite being treated as futilities, aesthetic treatments may have strong and important influences on psychological and emotional levels, as well as on the well-being of people. Some studies have already shown improvements in the quality of life and self-assessments by patients after aesthetic treatments.44 45 In this sense, the aforesaid questionnaires will be used to evaluate these aesthetic effects. Since the quality of life and the self-assessment questionnaires that have been validated in Portuguese when related to wrinkles are sparse, we decided to make fairly minor adaptations on some previously validated ones. The adaptation of the quality of life questionnaire for participants with dermatological diseases (Skindex-29)30 has involved the removal of 10 questions related to skin diseases that are not suitable for participants with wrinkles, resulting in a new questionnaire with 19 questions. The adaptation of the quality of life questionnaire for participants with melasma (MelasQoL-BP)31 has included the substitution of the word ‘melasma’ by the word wrinkles. Due to these adaptations, the questionnaires will be evaluated in terms of reproducibility and internal consistency, as has been previously performed on other questionnaires.46
When considering the importance of aesthetics of the face on the life role of a person, the development of efficacious treatments is essential. However, to prove that a treatment presents efficacy, the choice of a quantitative evaluation method is challenging. Most of the trials evaluating facial skin that can be found in the literature are based on subjective measurements (patient satisfaction and photos), since quantitative studies use biopsies.40 41 47 For this research, non-invasive quantification methods will be used aimed at evaluating a group of variables that may be affected or improved by photobiomodulation therapy (volume of wrinkles, elasticity/sagging and hydration). Treatment and evaluation procedures during this study will be performed by beauticians, since the procedures are non-invasive and they are included in beauticians’ professional attributions. In case the participants present any complication, IdSD will evaluate the participant and guide the treatment.
Some studies have pointed to the efficacy of LEDs in tissue repair, cutaneous hydration and increase in the production of the sustentation fibres. However, there are still studies that standardise dosimetry and the parameters of use.48 49 Here, the choice of wavelengths was made from studies that had demonstrated that an application of red light on the skin could trigger cell proliferation, increased collagen fibres and decreased metalloproteinases; these studies had also demonstrated that an amber light can interact with the epidermal cells, triggering mitosis and cell renewal, as well as acting on the protection and the hydration of the epidermis; all of this information is, together with clinical trials, showing an improvement of wrinkles using phototherapy.11 15 22 41 50 There is no consensus in the literature regarding the washout period for phototherapy, which varies from 7 days to 12 weeks.51–54 Due to this, a washout of 180 days for performing the cross-over treatment was chosen to evaluate if there were any residual effects from the first photobiomodulation treatment performed.
The results of this clinical trial may confirm the efficaciousness of phototherapy in reducing periocular wrinkles and show improvements in certain other parameters. Besides, the comparison between the reduction of wrinkles achieved by each wavelength may be a valuable contribution to the aesthetics area and pave the way to developing new treatment protocols with satisfactory results.
Ethics and dissemination
This protocol was approved by the Research Ethics Committee of the Nove de Julho University (acceptance number: 2.550.732). The trial has already been registered in the Registro Brasileiro de Ensaios Clínicos (REBEC number: RBR-6YFCBM) and it grants public access to the full protocol. After publishing the protocol, the data will be collected and the results will be presented at conferences and published in a peer-reviewed journal, selected by interest area and impact factor. At the end of the study, the main results will be disseminated to participants by email. The authorship of the results paper will include the authors of the protocol and others who may contribute to the procedures or analysis of data.
Supplementary Material
Acknowledgments
The authors thank Ieda Cristina Silva Santos Rocha (ICSSR), who performed the treatments, Cosmedical (Mauá, Brazil) which kindly provided the LED device, Lineallux to be used in this research, and Tecnotests (São Paulo, Brazil), the CK Electronic representative in Brazil, which kindly provided the devices for non-invasive analysis of the skin.
Footnotes
Contributors: LRM wrote the protocol and will execute the measurements. LJM adapted the QoL and the self-assessment questionnaires and will perform the reproducibility and internal consistency analysis, and LRM will apply them to the participants. IdSD designed the protocol and will evaluate the participants using the inclusion/exclusion criteria. DdFTdS performed the sample size calculation, proposed the statistics and will analyse the data. ACRTH generated the randomisation and designed the study. CP conceived and designed the treatment protocol. All of the authors have read and approved the final version of the protocol and of the manuscript.
Funding: This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent: Not required.
Ethics approval: This protocol was approved by the Research Ethics Committee of the Nove de Julho University on 22 June 2017 (#2.134.166) and the amendment with 137 patients on 19 March 2018 (#2.550.732).
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Mukherjee S, Date A, Patravale V, et al. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clin Interv Aging 2006;1:327–48. 10.2147/ciia.2006.1.4.327 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Mukherjee PK, Maity N, Nema NK, et al. Bioactive compounds from natural resources against skin aging. Phytomedicine 2011;19:64–73. 10.1016/j.phymed.2011.10.003 [DOI] [PubMed] [Google Scholar]
- 3. Boyd AS, Naylor M, Cameron GS, et al. The effects of chronic sunscreen use on the histologic changes of dermatoheliosis. J Am Acad Dermatol 1995;33:941–6. 10.1016/0190-9622(95)90284-8 [DOI] [PubMed] [Google Scholar]
- 4. Fourtanier A, Moyal D, Seité S. Sunscreens containing the broad-spectrum UVA absorber, Mexoryl SX, prevent the cutaneous detrimental effects of UV exposure: a review of clinical study results. Photodermatol Photoimmunol Photomed 2008;24:164–74. 10.1111/j.1600-0781.2008.00365.x [DOI] [PubMed] [Google Scholar]
- 5. Bennet D, Viswanath B, Kim S, et al. An ultra-sensitive biophysical risk assessment of light effect on skin cells. Oncotarget 2017;8:47861–75. 10.18632/oncotarget.18136 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Sukal SA, Geronemus RG. Thermage: the nonablative radiofrequency for rejuvenation. Clin Dermatol 2008;26:602–7. 10.1016/j.clindermatol.2007.09.007 [DOI] [PubMed] [Google Scholar]
- 7. Tierney EP, Eisen RF, Hanke CW. Fractionated CO2 laser skin rejuvenation. Dermatol Ther 2011;24:41–53. 10.1111/j.1529-8019.2010.01377.x [DOI] [PubMed] [Google Scholar]
- 8. Kaplan H, Kaplan L. Combination of microneedle radiofrequency (RF), fractional RF skin resurfacing and multi-source non-ablative skin tightening for minimal-downtime, full-face skin rejuvenation. J Cosmet Laser Ther 2016;18:438–41. 10.1080/14764172.2016.1228981 [DOI] [PubMed] [Google Scholar]
- 9. Merinville E, Grennan GZ, Gillbro JM, et al. Influence of facial skin ageing characteristics on the perceived age in a Russian female population. Int J Cosmet Sci 2015;37:3–8. 10.1111/ics.12252 [DOI] [PubMed] [Google Scholar]
- 10. Huang YY, Sharma SK, Carroll J, et al. Biphasic dose response in low level light therapy - an update. Dose Response 2011;9:dose-response.1 10.2203/dose-response.11-009.Hamblin [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Calderhead RG, Vasily DB. Low Level Light Therapy with Light-Emitting Diodes for the Aging Face. Clin Plast Surg 2016;43:541–50. 10.1016/j.cps.2016.03.011 [DOI] [PubMed] [Google Scholar]
- 12. Kim SK, You HR, Kim SH, et al. Skin photorejuvenation effects of light-emitting diodes (LEDs): a comparative study of yellow and red LEDs in vitro and in vivo. Clin Exp Dermatol 2016;41:798–805. 10.1111/ced.12902 [DOI] [PubMed] [Google Scholar]
- 13. Minatel DG, Enwemeka CS, França SC, et al. Phototherapy (LEDs 660/890nm) in the treatment of leg ulcers in diabetic patients: case study. An Bras Dermatol 2009;84:279–83. [DOI] [PubMed] [Google Scholar]
- 14. Leal Junior EC, Lopes-Martins RA, Baroni BM, et al. Comparison between single-diode low-level laser therapy (LLLT) and LED multi-diode (cluster) therapy (LEDT) applications before high-intensity exercise. Photomed Laser Surg 2009;27:617–23. 10.1089/pho.2008.2350 [DOI] [PubMed] [Google Scholar]
- 15. Wunsch A, Matuschka K. A controlled trial to determine the efficacy of red and near-infrared light treatment in patient satisfaction, reduction of fine lines, wrinkles, skin roughness, and intradermal collagen density increase. Photomed Laser Surg 2014;32:93–100. 10.1089/pho.2013.3616 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Silveira PCL, Silva LA, Tuon T, et al. Effects of low-level laser therapy on epidermal oxidative response induced by wound healing. Rev Bras Fisioter 2009;13:281–7. [Google Scholar]
- 17. Niedre MJ, Yu CS, Patterson MS, et al. Singlet oxygen luminescence as an in vivo photodynamic therapy dose metric: validation in normal mouse skin with topical amino-levulinic acid. Br J Cancer 2005;92:298–304. 10.1038/sj.bjc.6602331 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Vinck EM, Cagnie BJ, Cornelissen MJ, et al. Green light emitting diode irradiation enhances fibroblast growth impaired by high glucose level. Photomed Laser Surg 2005;23:167–71. 10.1089/pho.2005.23.167 [DOI] [PubMed] [Google Scholar]
- 19. de Vasconcelos Catão MH, Nonaka CF, de Albuquerque RL, et al. Effects of red laser, infrared, photodynamic therapy, and green LED on the healing process of third-degree burns: clinical and histological study in rats. Lasers Med Sci 2015;30:421–8. 10.1007/s10103-014-1687-0 [DOI] [PubMed] [Google Scholar]
- 20. Trelles MA, Allones I, Mayo E. Er:YAG laser ablation of plantar verrucae with red LED therapy-assisted healing. Photomed Laser Surg 2006;24:494–8. 10.1089/pho.2006.24.494 [DOI] [PubMed] [Google Scholar]
- 21. Hawkins D, Abrahamse H. Influence of broad-spectrum and infrared light in combination with laser irradiation on the proliferation of wounded skin fibroblasts. Photomed Laser Surg 2007;25:159–69. 10.1089/pho.2007.2010 [DOI] [PubMed] [Google Scholar]
- 22. Trelles MA, Allones I, Mayo E. Combined visible light and infrared light-emitting diode (LED) therapy enhances wound healing after laser ablative resurfacing of photodamaged facial skin. Medical Laser Application 2006;21:165–75. 10.1016/j.mla.2006.06.001 [DOI] [Google Scholar]
- 23. Smith KC. Laser (and LED) therapy is phototherapy. Photomed Laser Surg 2005;23:78–80. 10.1089/pho.2005.23.78 [DOI] [PubMed] [Google Scholar]
- 24. Karu TI, Afanas’eva NI. [Cytochrome c oxidase as the primary photoacceptor upon laser exposure of cultured cells to visible and near IR-range light]. Dokl Akad Nauk 1995;342:693–5. [PubMed] [Google Scholar]
- 25. Karu TI. Multiple roles of cytochrome c oxidase in mammalian cells under action of red and IR-A radiation. IUBMB Life 2010;62:607–10. 10.1002/iub.359 [DOI] [PubMed] [Google Scholar]
- 26. Kato M, Shinizawa K, Yoshikawa S. Cytochrome oxidase is a possible photoreceptor in mitochondria. Photobiochem Photobiophys 1981;2:263–9. [Google Scholar]
- 27. Lai P. Validating instruments of measure : Is it really necessary? Malays Fam Physician 2013;8:2–4. [PMC free article] [PubMed] [Google Scholar]
- 28. Patriota RC, Rodrigues CJ, Cucé LC. Intense pulsed light in photoaging: a clinical, histopathological and immunohistochemical evaluation. An Bras Dermatol 2011;86:1129–33. [DOI] [PubMed] [Google Scholar]
- 29. Costa A, Pires MC, Fabrício LHZ. Multicenter clinical study to evaluate safety and clinical efficacy of a body moisturizer based on ceramides, omegas, glycerin, Imperata cylindrica, erythritol, and homarine. Surg Cosmet Dermatology 2014;6:32–8. [Google Scholar]
- 30. Paula HR, Haddad A, Weiss MA, et al. Translation, cultural adaptation, and validation of the American Skindex-29 quality of life index. An Bras Dermatol 2014;89:600–7. 10.1590/abd1806-4841.20142453 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Maranzatto CF, Miot HA, Miot LD, et al. Psychometrican analysis and dimensional structure of the Brazilian version of melasma quality of life scale (MELASQoL-BP). An Bras Dermatol 2016;91:422–8. 10.1590/abd1806-4841.20165014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Furlani EAT. Cultural adaptation of rhytidectomy outcome evaluation questionnaire: facial outcome evaluation. Revista Brasileira de Cirurgia Plástica (RBCP) – Brazilian Journal of Plastic Sugery 2015;30:501–5. 10.5935/2177-1235.2015RBCP0186 [DOI] [Google Scholar]
- 33. Machado RS, Viana S, Sbruzzi G. Low-level laser therapy in the treatment of pressure ulcers: systematic review. Lasers Med Sci 2017;32:937–44. 10.1007/s10103-017-2150-9 [DOI] [PubMed] [Google Scholar]
- 34. Romanelli M, Piaggesi A, Scapagnini G, et al. EUREKA study - the evaluation of real-life use of a biophotonic system in chronic wound management: an interim analysis. Drug Des Devel Ther 2017;11:3551–8. 10.2147/DDDT.S142580 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Liu J, Zhang P, Tian J, et al. Ozone therapy for treating foot ulcers in people with diabetes. Cochrane Database Syst Rev 2015:CDO11979 10.1002/14651858.CD008474.pub2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Chaves ME, Araújo AR, Piancastelli AC, et al. Effects of low-power light therapy on wound healing: LASER x LED. An Bras Dermatol 2014;89:616–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Spitler R, Berns MW. Comparison of laser and diode sources for acceleration of in vitro wound healing by low-level light therapy. J Biomed Opt 2014;19:038001 10.1117/1.JBO.19.3.038001 [DOI] [PubMed] [Google Scholar]
- 38. Bhat J, Birch J, Whitehurst C, et al. A single-blinded randomised controlled study to determine the efficacy of Omnilux Revive facial treatment in skin rejuvenation. Lasers Med Sci 2005;20:6–10. 10.1007/s10103-005-0330-5 [DOI] [PubMed] [Google Scholar]
- 39. Jagdeo J, Austin E, Mamalis A, et al. Light-emitting diodes in dermatology: A systematic review of randomized controlled trials. Lasers Surg Med 2018. 10.1002/lsm.22791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Lee SY, Park KH, Choi JW, et al. A prospective, randomized, placebo-controlled, double-blinded, and split-face clinical study on LED phototherapy for skin rejuvenation: clinical, profilometric, histologic, ultrastructural, and biochemical evaluations and comparison of three different treatment settings. J Photochem Photobiol B 2007;88:51–67. 10.1016/j.jphotobiol.2007.04.008 [DOI] [PubMed] [Google Scholar]
- 41. Gold MH, Biron J, Levi L, et al. Safety, efficacy, and usage compliance of home-use device utilizing RF and light energies for treating periorbital wrinkles. J Cosmet Dermatol 2017;16:95–102. 10.1111/jocd.12299 [DOI] [PubMed] [Google Scholar]
- 42. Miranda da Silva C, Peres Leal M, Brochetti RA, et al. Low level laser therapy reduces the development of lung inflammation induced by formaldehyde exposure. PLoS One 2015;10:e0142816–16. 10.1371/journal.pone.0142816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Tomimura S, Silva BP, Sanches IC, et al. Hemodynamic effect of laser therapy in spontaneously hypertensive rats. Arq Bras Cardiol 2014;103:161–4. 10.5935/abc.20140117 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Barone M, Cogliandro A, Di Stefano N, et al. A systematic review of patient-reported outcome measures after rhinoplasty. Eur Arch Otorhinolaryngol 2017;274:1807–11. 10.1007/s00405-016-4359-9 [DOI] [PubMed] [Google Scholar]
- 45. Dauplat J, Kwiatkowski F, Rouanet P, et al. Quality of life after mastectomy with or without immediate breast reconstruction. Br J Surg 2017;104:1197–206. 10.1002/bjs.10537 [DOI] [PubMed] [Google Scholar]
- 46. Chan-Yeung M, Law B, Sheung SY, et al. Internal consistency, reproducibility, responsiveness, and construct validity of the Chinese (HK) version of the asthma quality of life questionnaire. Qual Life Res 2001;10:723–30. 10.1023/A:1013819108662 [DOI] [PubMed] [Google Scholar]
- 47. Berardesca E, Ardigo M, Cameli N, et al. Randomized, double-blinded, vehicle-controlled, split-face study to evaluate the effects of topical application of a Gold Silk Sericin/Niacinamide/Signaline complex on biophysical parameters related to skin ageing. Int J Cosmet Sci 2015;37:606–12. 10.1111/ics.12237 [DOI] [PubMed] [Google Scholar]
- 48. Russell BA, Kellett N, Reilly LR. A study to determine the efficacy of combination LED light therapy (633 nm and 830 nm) in facial skin rejuvenation. J Cosmet Laser Ther 2005;7:196–200. 10.1080/14764170500370059 [DOI] [PubMed] [Google Scholar]
- 49. Baez F, Reilly LR. The use of light-emitting diode therapy in the treatment of photoaged skin. J Cosmet Dermatol 2007;6:189–94. 10.1111/j.1473-2165.2007.00329.x [DOI] [PubMed] [Google Scholar]
- 50. Kim JS, Yoon TJ, Yu KN, et al. Cellular uptake of magnetic nanoparticle is mediated through energy-dependent endocytosis in A549 cells. J Vet Sci 2006;7:321–6. 10.4142/jvs.2006.7.4.321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Jacobsonkram D, Roe JL, Williams JR, et al. Decreased Invitro Lifespan of Fibroblasts Derived from Skin Exposed to Photochemotherapy Invivo. Lancet 1982;2:1399–400. [DOI] [PubMed] [Google Scholar]
- 52. Francisco CO, Beltrame T, Ferraresi C, et al. Evaluation of acute effect of light-emitting diode (LED) phototherapy on muscle deoxygenation and pulmonary oxygen uptake kinetics in patients with diabetes mellitus: study protocol for a randomized controlled trial. Trials 2015;16:572 10.1186/s13063-015-1093-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Ferraresi C, Beltrame T, Fabrizzi F, et al. Muscular pre-conditioning using light-emitting diode therapy (LEDT) for high-intensity exercise: a randomized double-blind placebo-controlled trial with a single elite runner. Physiother Theory Pract 2015;31:354–61. 10.3109/09593985.2014.1003118 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Mateen FJ, Manalo NC, Grundy SJ, et al. Light therapy for multiple sclerosis-associated fatigue: Study protocol for a randomized controlled trial. Medicine 2017;96:e8037 10.1097/MD.0000000000008037 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.