

Abstract
Purpose:
To gauge the differences in ophthalmology residency training, academic, clinical and surgical, in the last three decades of the 20th century and the first decade of the 21st century.
Methods:
A survey was conducted by the Academic and Research Committee of the All India Ophthalmological Society, in 2014–2016, using a prevalidated questionnaire, which was circulated to ophthalmologists to gauge the practicality of the teaching protocols of clinical and surgical skills during postgraduate residency program.
Results:
Of the 1005 respondents, 320 ophthalmologists who completed residency between 1967 and 2002 (20th century trained) and 531 who completed a residency in 2003–2012 (21st century trained) fulfilled the inclusion criteria. The average age was 49.2 years (standard deviation [SD] 4) and 32.6 years (SD 4), respectively. Twenty-first century trained ophthalmologists rated their training significantly better than the 20th century trained ophthalmologists for slit lamp examination (P = 0.001), indirect ophthalmoscopy, gonioscopy, automated perimetry, optical coherence tomography, and fundus photography (all having P < 0.001), while the 20th century trained rated their teaching of refraction, synoptophore, diplopia charting better (all P < 0.001). The range of grading was 0–10 in all categories. The median number of surgeries performed independently by 20th century and 21st century trained (during their training period) were: intracapsular cataract extraction (ICCE) 10, 0; extracapsular cataract extraction (ECCE) 43, 18; small incision cataract surgery (SICS) 5, 55; phacoemulsification (Phaco) 0, 1; pterygium excision 20, 15; dacryocystectomy 11, 4; dacryocystorhinostomy 11, 2; chalazion 35, 30; trabeculectomies 5, 0; strabismus correction 0, 0; vitrectomy 0, 0; keratoplasty 0, 0; eyelid surgery 6, 2; and ocular emergencies 18, 20.
Conclusion:
Teaching of many clinical skills had improved over decades. Cataract surgery training has shifted from ICCE and ECCE to SICS and Phaco, but other surgeries were still taught sparingly. There was an enormous variation across the country in residency training which needs immediate attention.
Keywords: India, ophthalmology residency, postgraduate medical education, residency training
Residency training of postgraduate medical students is the base for all medical specialty training. Ophthalmology, a surgical specialty, is no exception to this. The goal of a postgraduate educational program in ophthalmology is training for practice. The practice involves being competent to diagnose, treat, and manage the most common conditions encountered in clinical practice effectively and with minimal error.
Conventionally, this has meant acquisition of knowledge and skills for decision-making and operative skills. In addition, the dissertation has been a part of the postgraduate courses to develop the residents’ research skills. Other competencies identified more recently as being an important part of the postgraduate curriculum includes professionalism and ethics, communication, leadership, social accountability, and an understanding of systems-based practice.
Curriculum is dynamic and is expected to change in keeping with the scientific advancements of the particular specialty. While regulatory bodies and universities continue to update their curricula regularly (the “declared curriculum”),[1,2] the “taught curriculum” predominates in the residency program. Although congruence between declared and taught is the ideal, there is a variance in adherence.
In the past decades, ophthalmology practice has changed tremendously. Intracapsular cataract extraction (ICCE) surgery, the surgery of choice for cataract extraction till the 1970s has given way to phacoemulsification (Phaco) and small incision cataract surgery (SICS). Glaucoma management and treatment of retinal disorders have undergone a sea change.
However, there are few studies documenting if and how the residency training has changed or progressed with time. The Academic and Research Committee of the All India Ophthalmological Society had commissioned a survey to understand the functionality of ophthalmological residency training. There have been numerous studies from India, China, Canada, and Unites States of America regarding the efficacy of residency training, but none comparing it across time.[3,4,5,6,7,8,9,10,11,12,13] This manuscript presents the feedback of residency training of those who were trained in the last decades of the 20th century and compares it with the feedback on training imparted in the first decade of the 21st century. Clinical skills learnt, surgical training and demographic factors were compared between both the groups.
This study endeavors to capture the change over time in the trend related to the choice of ophthalmology as a specialty, the nature of educational experience during the residency and ways in which the graduates advance their careers and continue to develop professional skills. The research question that the study seeks to answer is: What is the changing trend of ophthalmology residency programs from the last decades of the 20th century to the first decade of the 21st century.
Methods
This was a cross-sectional study to explore the changes in teaching practice in ophthalmology residency programs in India, using a prevalidated questionnaire. The survey was prevalidated by having it vetted by six researchers and educationists and then doing a pilot study on a sample of 15 ophthalmologists. The All India Ophthalmological Society (AIOS) through its Academic and Research Committee commissioned a survey of residency training. The study population was ophthalmologists who were trained in India.
The “change” was studied between two cohorts that graduated at different points in time: Group A (20th century trained) who started training between 1967 and 2001 and graduated before 2002 and Group B (21st century trained) that enrolled between 2003 and 2012 and graduated before 2014. The respondents were asked to grade clinical skills and surgeries learnt and performed during their residency. They had the choice of anonymity but were also asked certain demographic information and details of their academic program and research project during residency training. The details are in Appendix 1 (294.8KB, pdf) .
Questionnaire used in the study
Although the survey aimed at getting feedback from 21st century trained ophthalmologists, it was kept open for all ophthalmologists. The survey was circulated among all members of the AIOS, irrespective of their seniority and was open to all ophthalmologists (both members and nonmembers). There were repeated reminders through E-mails, text messages, and later phone calls to participate in the study. Heads of institutions of excellence retired, and serving Professors were requested to send the survey link to their past students. Telephone, E-mail, and text message reminders were sent to potential respondents on 11 occasions between October 2014 and February 2016. Incomplete responses were not considered.
The collected data were organized into four categories – (1) demographic data, (2) training place characteristics, (3) curricular aspects, and (4) career advancement following the training.
The aim was to understand the differences in the training methods and outputs over the past decades. Respondents had to fill their demographic details, the institution where their residency was completed, clinical examination skills learnt and surgeries observed, assisted, operated under supervision and independently during the residency training. A section dealt with the dissertation done by the residents and whether it was presented and/or published. The immediate future plans and need for further training by the respondents was a part of the questionnaire.
The data were entered into Excel Worksheets and Statistical Package for Social Sciences (SSPS version 16), IBM Corporation, Armonk, New York, USA was used for data analysis. Mean, standard deviation (SD), and median of the responses was considered.
Results
A total of 320 ophthalmologists who did their residency in the last decades of the 20th century completed the questionnaire, 75 (23.4%) were females. Their average age was 49.2 years (SD 8.7, range 37–84), median 47 years. They had completed their residency between 1967 and 2002. One hundred and twenty-eight (39.9%) were from metro cities, 93 (29%) from large towns, 70 (21.8%) from district headquarters while 18 (56%) from smaller towns or villages. Twenty-three (7.2%) were MD, 107 (33.3%) were master of surgery in ophthalmology, 58 (18.1%) were diplomate of the national board in ophthalmology while 81 (25.2%) were diploma in ophthalmology. Only 15 (4.7%) came from a family of ophthalmologists. Ninety-eight (30.5%) chose ophthalmology as they believed it had good career prospects. Twenty-one (6.5%) chose ophthalmology for financial gains and 67 (20.9%) chose ophthalmology for improvement of knowledge. Eighteen (5.6%) worked in a government hospital, 28 (8.7%) in a nongovernment organization hospital, 49 (15.3%) in a teaching institution, 66 (20.6%) in private practice, and 15 (4.7%) in group practice. The rest did not give details about the type or nature of their practice. The data of 21st century trained ophthalmologists have been published in this journal earlier.[14,15]
Table 1 shows how the 20th century trained ophthalmologists rated their clinical skills and education while undergoing residency training. Refraction, slit lamp examination, and direct ophthalmoscopy were taught well. However, exposure to equipment oriented skills such as perimetry, fundus photography, fluorescein angiography, optical coherence tomography (OCT), and B-scan and A-scan ultrasonography was not taught to their satisfaction. Contact lens evaluation was taught to 109 (52.6%) of the survey respondents.
Table 1.
Teaching of clinical skills as rated by 20th century trained ophthalmologists
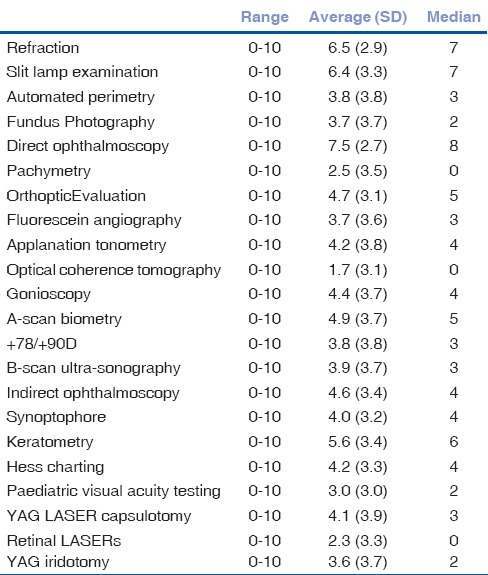
Table 2 demonstrates the surgical experience gained by the 20th century trained during their residency training. ICCE surgery was second to conventional extracapsular cataract extraction (ECCE) surgery as the most common surgery performed in the residency. Except for ECCE, there was a large difference in the mean and median for ICCE, SICS, and Phaco. There was a substantial variation across residency training programs for surgeries observed, assisted, performed under supervision, and surgeries performed independently. The standard deviation was more, as some programs gave insufficient surgical exposure to residents. Pterygium excision, sac surgeries, and ocular emergencies were more regularly a part of programs.
Table 2.
Surgeries observed, assisted, performed under supervision and independently by 20th century trained ophthalmologists during their residency training
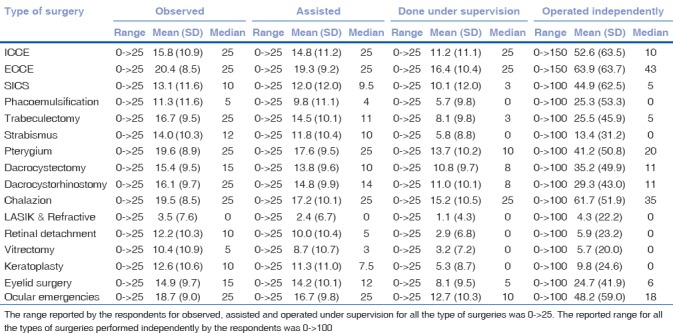
Table 3 compares the demographics between 20th century trained and 21st century trained ophthalmologists in this study. [Table 4] compares the clinical skills learnt during residency training between 20th and 21st century trained ophthalmologists. Ophthalmologists trained in 21st century were better exposed to automated perimetry, fundus photography, fluorescein angiography, OCT, +90/+78 D fundus evaluation, A- and B-scan ultrasonography, indirect ophthalmoscopy, and applanation tonometry. However, exposure to pediatric visual acuity testing and orthoptic evaluation was areas that were desired by the respondents. Clinical skills such as refraction, diplopia charting, and synoptophore use were perceived to be taught less by 21st century trained ophthalmologists compared to their 20th century trained counterparts. While Nd: YAG laser capsulotomy and retinal laser exposure have increased, the same did not feature for YAG iridotomies. While (52.6%) 20th century trained reported being taught contact lenses during residency training, only 152/531 (28.6%) 21st century trained ophthalmologists reported the same.
Table 3.
Comparing demographics between 20th and 21st century trained ophthalmologists in this study
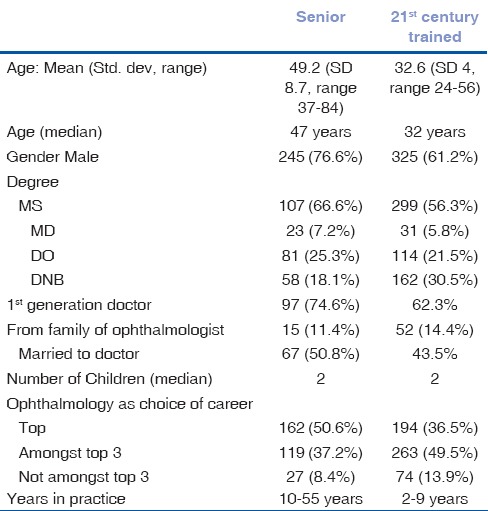
Table 4.
Comparing the clinical skills taught during residency between 20th and 21st century trained ophthalmologists
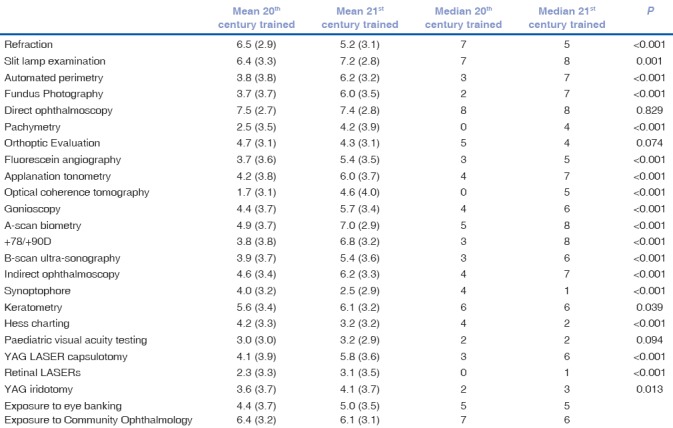
Table 5 compares the surgical training across generations of ophthalmologists. ICCE had become uncustomary, and manual SICS and Phaco were the most common cataract surgeries taught. However, there was a considerable variation in the country across programs (range 0–>25 or 0–>100 in all surgeries); and this has not changed substantially over the decades in the population studied.
Table 5.
Comparing surgical skills taught during residency between 20th and 21st century trained ophthalmologists, by comparing the number of surgeries performed independently during the residency
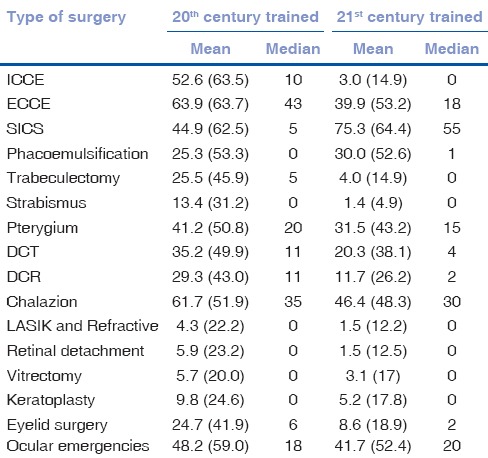
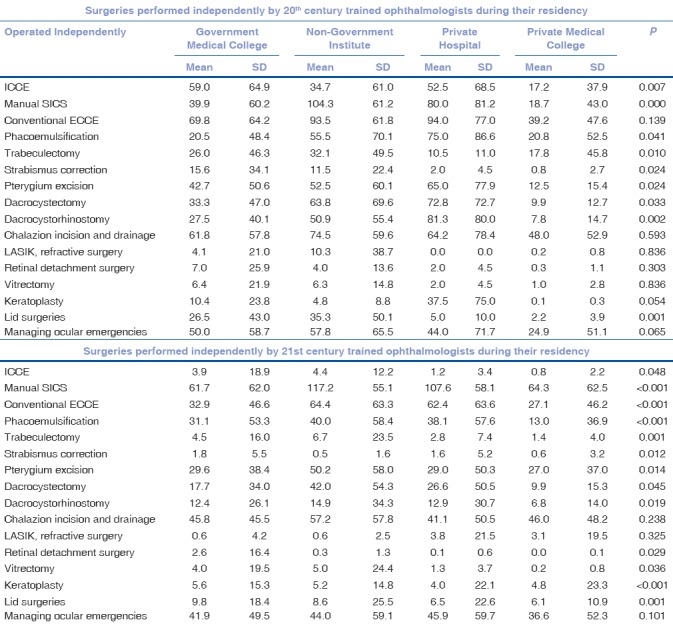
Table 6 compares the academic and research inputs given to residents in the two groups. Seminars and case presentations have remained the most popular mode of teaching postgraduate ophthalmology students. Wet laboratories, rare in the last century, have become more popular in the 21st century. [Table 7] and [Table 8] compare the clinical skills and surgical experience gained by the residents in the 20th and 21st century trained groups across the different teaching institutes.
Table 6.
Comparing the rating of academic schedule and types of teaching activities
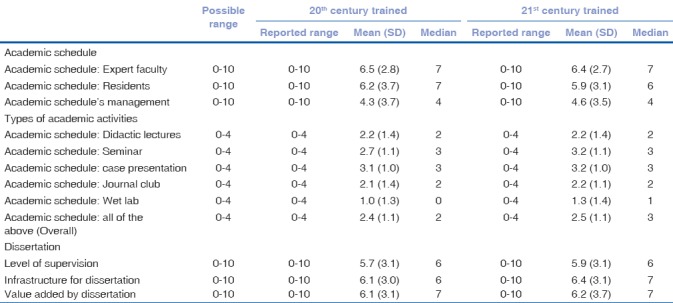
Table 7.
Comparing the clinical skills taught to 20th and 21st century trained ophthalmologists depending on the type of institution in which residency raining was completed. The possible range for each response was 0.10
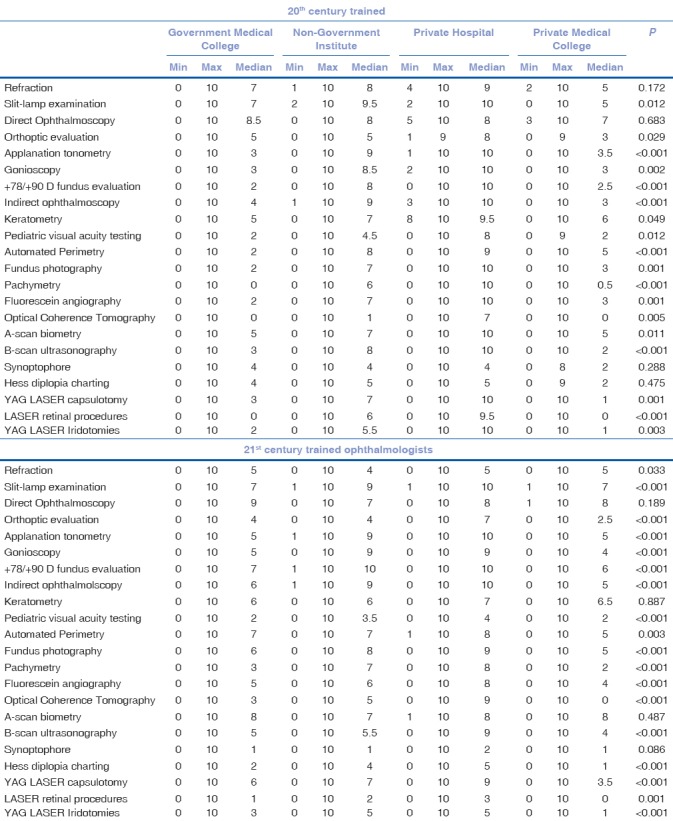
Table 8.
Comparison of surgical training imparted depending on the type of institute where residency was done
Discussion
The type of ophthalmic surgeries have changed over the decades, and the clinical skills have improved. However, there was a wide variation among residency programs, and the range of responses was graded from 0 to 10. Some aspects have had desirable changes. Demographically more women have entered ophthalmology. There were more second generation medical professionals and many of them chose ophthalmology as a career. Ophthalmology still remained a sought-after career option for medical graduates.
In the 21st century trained, many more come from a family of ophthalmologists as compared to the cohort trained in the last century. Medical graduates still remained the choice for spouse for both groups.
Almost all the clinical skills, teaching and exposure to investigations had improved over the past decade. The 20th century trained cohort reported only refraction, diplopia charting, and synoptophore being taught better than the 21st century trained cohort. Orthoptic evaluation, pediatric visual acuity testing and diplopia charting are skills imperative for general ophthalmologists, and this is a requirement which needs to be addressed in the teaching curriculum, even in the present day.
However, a wide range (actual reported range 0–10 for all clinical skills, investigations, and surgeries) had remained the same with both groups. Thus, while the median residency program has improved, uniformity in basic quality in residency training needs to be pursued energetically.
Cataract is still the most common cause of avoidable blindness.[16,17,18] Exposure to cataract surgery was adequate but not uniform. ICCE had become a surgery of the past and manual SICS was the most common cataract surgery taught presently. Glaucoma surgeries in residency training programs showed a decline, even though it is a significant cause of blindness.[19] Better pharmacological agents and their easier availability may be a reason for the overall decrease in glaucoma surgeries.[20,21] However, learning the correct technique of filtration glaucoma surgery is essential in a residency program.[22] Pterygium excisions, sac surgeries, and eyelid surgeries had declined in number in residency training. Less outdoor work, use of protective spectacles and by and large, lesser number of patients being referred to the teaching hospitals could be possible causes. The median for strabismus surgeries, retinal detachment surgery, vitrectomy, and keratoplasty was zero for both groups. Both independent surgeries and surgeries performed under supervision were less. Strabismus, corneal, and retinal diseases are significant contributors to ocular morbidity and visual impairment.[23]
Eye bank training had improved to an extent. The Medical Council of India has made it mandatory for each medical college to have an eye bank.
Diabetic retinopathy is increasing as a cause of blindness and visual impairment.[24,25] The resident's exposure to various modalities to manage this disease (OCT, fundus photography, lasers) has improved over time; but the exposure was uneven across the different programs in the country.
The “declared curricula” earlier and now were guidelines about the topics and subject matter to be covered.[1,2] They were not explicit about the details of the clinical, surgical, and research skills that a resident should master during the training unlike the competency standards set in the United States of America.[13] The system leaves a lot to the residents’ initiative. They are expected to learn by observing and following their teachers as it was in the ancient 'Gurukul' times.[26]
Mid-term assessments were rare. Exit examinations are mainly theoretical and practical examinations are based on case presentations. A robust methodology to judge the surgical skills of a passing-out resident is needed. Practical and theoretical teaching of refractive errors, the most common cause of visual impairment is of paramount importance. The residency curriculum should stress on comprehensive ophthalmology.
The teaching of certain diagnostic techniques has gained importance in the past decade, but teaching of basic ophthalmic clinical skills has not shown a consistent growth. The emphasis of surgical training is mainly on cataract surgery. Some tried and tested academic techniques such as journal clubs and wet laboratories need to be popularised.
The study is limited to the respondents’ responses. There may be a selection bias since respondents with extreme views (both positive and negative) about their residency training may have been more inclined to participate. The possibility of recall bias is relevant to the study. The other limitation of this study was the absence of evaluation of other pertinent skills, for example, professionalism and ethics, communication, leadership, and social accountability. However, since the entire process was voluntary (and anonymous if needed), we have for the first time a picture across decades about how residency training was being imparted.
The lack of standardization indicates the role of a strong regulatory authority for the implementation of the curriculum. The curriculum should be such that it focuses on the infrastructure, human resources and the actuality of the residents’ learning. In addition, the curriculum should be “need-based;” it should establish standards, follow them. There should be a method to monitor these standards.
The role of residents as teachers and researchers needs to be emphasized during residency since senior residents make excellent teachers.[27] These are part of competency-based residency curricula elsewhere.[13]
Conclusion
Indian ophthalmology is considered as one of the world leaders in blindness prevention and control.[28,29] It is held as a model for delivering quality eye care with low-cost innovations.[30,31] Ophthalmology is still a sought-after medical sub-specialty attracting the best of talents for postgraduation. Residency training programs have evolved considerably in the past decades, but a significant variation still exists in the Indian subcontinent, which needs to be bridged at the earliest, through a uniform and robust residency program.
Financial support and sponsorship
The study was commissioned by All India Ophthalmological Society, Academic and Research Committee (2014–2017).
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to Ramamurthy Dandapani, Debashish Bhattacharya, Barun Kumar Nayak, Karl Golnik, Santhan Gopal, Yogesh Shah, Ajit Babu Majjhi, Rishi Pukhraj, Virendra Agarwal, Ashis Bhattacharya, Namrata Sharma, Lingam Gopal, Pradeep Sharma, P Namperumalsamy, Meenakshi Yadav Dhar, G Chandrashekhar, Amod Gupta, Samar Kumar Basak, O K Radhakrishnan, Anil N Kulkarni, Tara Prasad Das.
References
- 1.Maharashtra University of Health Sciences, syllabus for postgraduate degree in ophthalmology. [Last accessed on 2016 Oct 15]. http://www.muhs.ac.in/ showpdf.aspx?src1=http://intranet.muhs.ac.in/syllabus.aspx .
- 2.Medical Council of India. [Last accessed on 2016 Oct 15]. www.mciindia.org/post-graduate .
- 3.Thomas R, Dogra M. An evaluation of medical college departments of ophthalmology in India and change following provision of modern instrumentation and training. Ind J Ophthalmol. 2008;56:9–16. doi: 10.4103/0301-4738.37589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Grover AK. Postgraduate ophthalmic education in India: Are we on the right track? Ind J Ophthalmol. 2008;56:3–4. doi: 10.4103/0301-4738.37581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Murthy GV, Gupta SK, Bachani D, Sanga L, John N, Tewari HK. Status of specialty training in ophthalmology in India. Ind J Ophthalmol. 2005;53:135–42. doi: 10.4103/0301-4738.16182. [DOI] [PubMed] [Google Scholar]
- 6.Gogate P, Deshpande M, Dharmadhikari S. Which is the best method to learn ophthalmology. Resident doctors’ perspective of ophthalmology training? Ind J Ophthalmol. 2008;56:409–12. doi: 10.4103/0301-4738.42419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ajay K, Krishnaprasad R. Feedback of final year ophthalmology postgraduates about their residency ophthalmology training in South India. Ind J Ophthalmol. 2014;62:814–7. doi: 10.4103/0301-4738.138628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ajay K, Krishnaprasad R, Divya DS. Ophthalmic surgical training in Karnataka and Southern India: Present status and future interests from a survey of final-year residents. Ind J Ophthalmol. 2015;63:306–11. doi: 10.4103/0301-4738.158067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Young AL, Jhanji V, Liang Y, Congdon N, Chow S, Wang F, et al. A survey of perceived training differences between ophthalmology residents in Hong Kong and China. BMC Med Edu. 2015;15:158. doi: 10.1186/s12909-015-0440-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Le K, Bursztyn L, Rootman D, Harissi-Dagher M. National survey of Canadian ophthalmology residency education. Can J Ophthalmol. 2016;51:219–25. doi: 10.1016/j.jcjo.2016.04.017. [DOI] [PubMed] [Google Scholar]
- 11.Binenbaum G, Volpe NJ. Ophthalmology resident surgical competency: A national survey. Ophthalmology. 2006;113:1237–44. doi: 10.1016/j.ophtha.2006.03.026. [DOI] [PubMed] [Google Scholar]
- 12.McDonnell PJ, Kirwan TJ, Brinton GS, Golnik KC, Melendez RF, Parke DW, 2nd, et al. Perceptions of recent ophthalmology residency graduates regarding preparation for practice. Ophthalmology. 2007;114:387–91. doi: 10.1016/j.ophtha.2006.10.027. [DOI] [PubMed] [Google Scholar]
- 13.Golnik KC, Lee AG, Wilson MC. A national program director survey of the shift to competency-based education in ophthalmology. Ophthalmol. 2008;115:1426–30. doi: 10.1016/j.ophtha.2008.01.017. [DOI] [PubMed] [Google Scholar]
- 14.Gogate PM, Biswas P, Natarajan S, Ramamurthy D, Bhattacharya D, Golnik K. Residency Evaluation and Adherence Design Study: Young ophthalmologists’ perception of their residency programs; Clinical & Surgical skills. Ind J Ophthalmol. 2017;65(In press) doi: 10.4103/ijo.IJO_643_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gogate PM, Biswas P, Natarajan S, Nayak BK, Gopal S, Shah Y, Basak SK. Residency Evaluation and Adherence Design Study: Young ophthalmologists’ perception of their residency programs II: Academics &Research dissertation. Ind J Ophthalmol. 2017;65:12–8. doi: 10.4103/ijo.IJO_668_16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Venkataswamy G. Cataract in the Indian subcontinent. Ophthalmic Surg. 1987;18:464–6. [PubMed] [Google Scholar]
- 17.Minnassian DC, Mehra V. 3.8 million blinded by cataract each year: projections from the first epidemiological study of incidence of cataract blindness in India. Br J Ophthalmol. 1990;74:341–3. doi: 10.1136/bjo.74.6.341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Neena J, Rachel J, Praveen V, Murthy GV. Rapid assessment of avoidable blindness in India. PLoS ONE. 2008;3:e2867. doi: 10.1371/journal.pone.0002867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vijaya L, George R, Asokan R, Velumuri L, Ramesh SV. Prevalence and causes of low vision and blindness is an urban population: The Chennai Glaucoma study. Ind J Ophthalmol. 2014;62:477–81. doi: 10.4103/0301-4738.111186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Nayak BK, Maskati QB, Parikh R. the unique problem of glaucoma: under diagnosis and over treatment. Ind J Ophthalmol. 2011;59:51–2. doi: 10.4103/0301-4738.73677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dietlein TS, Hermann MM, Jordan JF. The medical and surgical treatment of glaucoma. Dtsch Arztebl Int. 2009;106:597–605. doi: 10.3238/arztebl.2009.0597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gogate PM, Deshpande R, Chelerkar V, Deshpande S, Deshpande M. Is glaucoma a disease of ignorance and poverty. A case control study for late presentation of glaucoma in India. Ind J Ophthalmol. 2011;59:29–35. doi: 10.4103/0301-4738.73720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pineda R. Corneal transplantation with developing world: Lessons learnt & meeting the challenge. Cornea. 2015;34:535–40. doi: 10.1097/ICO.0000000000000567. [DOI] [PubMed] [Google Scholar]
- 24.Patil SA, Gogate P, Vora S, Ainapure S, Hingane RN, Kulkarni AN, Shammanna BR. Prevalence and causes of blindness and cataract surgical services in Sindhudurg district on west coast of India. Ind J Ophthalmol. 2014;62:240–5. doi: 10.4103/0301-4738.128633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Raman R, Gella L, Srinivas S, Sharma T. Diabetic retinopathy: An epidemic at home and around the world. Ind J Ophthalmol. 2016;64:69–75. doi: 10.4103/0301-4738.178150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mendis L, Adkoli BV, Adhikari RK, Muzaherul Haq M, Qureshi AF. Postgraduate medical education in South Asia. Br Med J. 2004;328:779–81. doi: 10.1136/bmj.328.7443.779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ryg PA, Hafler JP, Forster SH. The Efficacy of Residents as Teachers in an Ophthalmology Module. J Surg Edu. 2016;73:323–8. doi: 10.1016/j.jsurg.2015.10.014. [DOI] [PubMed] [Google Scholar]
- 28.Rao GN, Khanna RC, Athota SM, Rajshekar V, Ravi P. K Integrated model of primary and secondary eye care for underserved rural areas: The L V Prasad Eye Institute experience. Ind J Ophthalmol. 2012;60:396–400. doi: 10.4103/0301-4738.100533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Le HG, Ehrlich JR, Venkatesh R, Srinivasan A, Kolli A, Haripriya A. A sustainable model for delivering high quality, efficient cataract surgery in southern India. Health Aff (Millwood) 2016;35:1783–90. doi: 10.1377/hlthaff.2016.0562. [DOI] [PubMed] [Google Scholar]
- 30.Gogate P, Deshpande M, Nirmalan P. Why do phacoemulsification?. Manual small incision cataract surgery is almost as effective and more economical. Ophthalmol. 2007;114:965–8. doi: 10.1016/j.ophtha.2006.08.057. [DOI] [PubMed] [Google Scholar]
- 31.Venkataswamy G. Can cataract surgery be marketed like hamburgers in developing countries? Arch Ophthalmol. 1993;111:580. doi: 10.1001/archopht.1993.01090050014002. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Questionnaire used in the study