

Abstract
Although a tibial eminence avulsion fracture is a rare knee injury, it can result in some complications such as nonunion, limited range of motion, and anterior instability of the knee if the displaced fracture is not well reduced. Arthroscopic procedures for this fracture have been commonly performed in recent years. In patients with small fragments, a pullout operation is usually performed, but arthroscopic suture reduction is technically difficult. In addition, anterior instability of the knee may remain even if the fragment is well reduced at the time of the surgical procedure. Generally, surgeons are concerned about anatomic reduction compared with appropriate tensioning during surgery. Therefore, one of the key points to avoid remaining anterior instability of the knee is to obtain and maintain appropriate tensioning. The purpose of this article is to present an easy and safe technique for acquisition of appropriate tensioning using a tensioning device for tibial eminence avulsion fractures. Although it has limitations, this technique can facilitate the reduction of tibial eminence avulsion fractures and appropriate tensioning of the anterior cruciate ligament.
Tibial eminence avulsion fractures are uncommon knee injuries. The causes of these fractures are motor vehicle accidents; sports injuries; and falls that cause hyperextension, hyperflexion, and/or rotation.1, 2, 3 In particular, hyperflexion and rotation comprise the most common injury mechanism and can occur as a skier falls back while landing after a jump. The patient's symptoms are swelling, pain, and limited range of motion. The Lachman or anterior drawer test is positive as with a substantial anterior cruciate ligament (ACL) tear. Radiographs usually show an avulsed fragment, and these fractures are classified into 4 types depending on fracture displacement: type I, undisplaced fracture; type II, partially displaced or hinged fracture; type III, completely displaced fracture4; or type IV, displaced comminuted fracture.1 Both type I and reducible type II fractures are usually treated conservatively with casting. Type II fractures with dislocation of more than 2 mm and type III and type IV fractures are usually treated surgically. Some authors have preferred to use computed tomography (CT) or magnetic resonance imaging as supplemental diagnostic imaging to confirm the diagnosis and to evaluate associated soft-tissue damage.5, 6 Traditionally, open reduction–internal fixation was performed for displaced tibial eminence avulsion fractures. However, with the evolution of arthroscopic techniques, arthroscopic treatment has been more common in recent years. Although a pullout operation is usually performed under arthroscopic visualization, it is technically difficult to reduce the fragment with suture and keep appropriate tensioning during surgery. Therefore, even if the fragment is well reduced at the time of the surgical procedure, anterior instability of the knee may remain. This Technical Note and accompanying video (Video 1) describe a modified arthroscopic suture fixation and tensioning technique to treat a tibial eminence avulsion fracture.
Technique
Preparation
The surgical steps are described in Table 1. For preoperative preparation, CT is performed to evaluate the displaced tibial eminence avulsion fracture (Fig 1, Fig 2, Fig 3).
Table 1.
Tips and Tricks of Procedure Based on Our Experience
| Indications |
| All tibial eminence avulsion fractures |
| Surgical steps |
| Preparation |
| No. 2 FiberWire suture is attached to the Scorpion suture passer. |
| Standard knee arthroscopy is performed with anterolateral and anteromedial portals. |
| Blood clots are removed to confirm the shape of the bone fragment and fracture bed. |
| Reduction with suture |
| The suture is tied to the ACL near the base of its insertion on the fragment. |
| A small incision is made medial to the tibial tubercle. |
| A 2.4-mm Kirschner wire is drilled to the center of the tibial fracture bed with an ACL guide. |
| Suture is pulled out through the tibial tunnel using a suture retriever or needle with loop suture. |
| Anatomic reduction is performed by pulling down the suture. |
| Temporary fixation is performed using an EndoButton at the anterior surface of the tibia. |
| Tensioning and fixation |
| The second suture is passed to the posterior side of the ACL near the base of its insertion on the fragment. |
| Two other tunnels are created on the medial and lateral side of the fracture bed with an ACL guide. |
| The second suture is pulled out through the tunnel using a suture retriever or 18-gauge needle with loop suture. |
| The second suture is tied over the tibial cortex regardless of the knee flexion angle. |
| The Tighting Gun is used for strong tensioning with or without an EndoButton. |
| Examination and final fixation |
| The knee joint undergoes flexion and extension after reduction and temporary fixation. |
| Knee stability is checked with the Lachman test. |
| Final tensioning is performed with the Tighting Gun regardless of the knee flexion angle. |
| The tension of the ACL is confirmed under direct arthroscopic visualization. |
| The first and second sutures are tied over the tibial cortex. |
ACL, anterior cruciate ligament.
Fig 1.

For preoperative preparation, computed tomography is performed to evaluate a displaced tibial eminence avulsion fracture (arrow).
Fig 2.

A computed tomography scan of the right knee in the sagittal plane shows a type III displaced tibial eminence avulsion fracture (arrow).
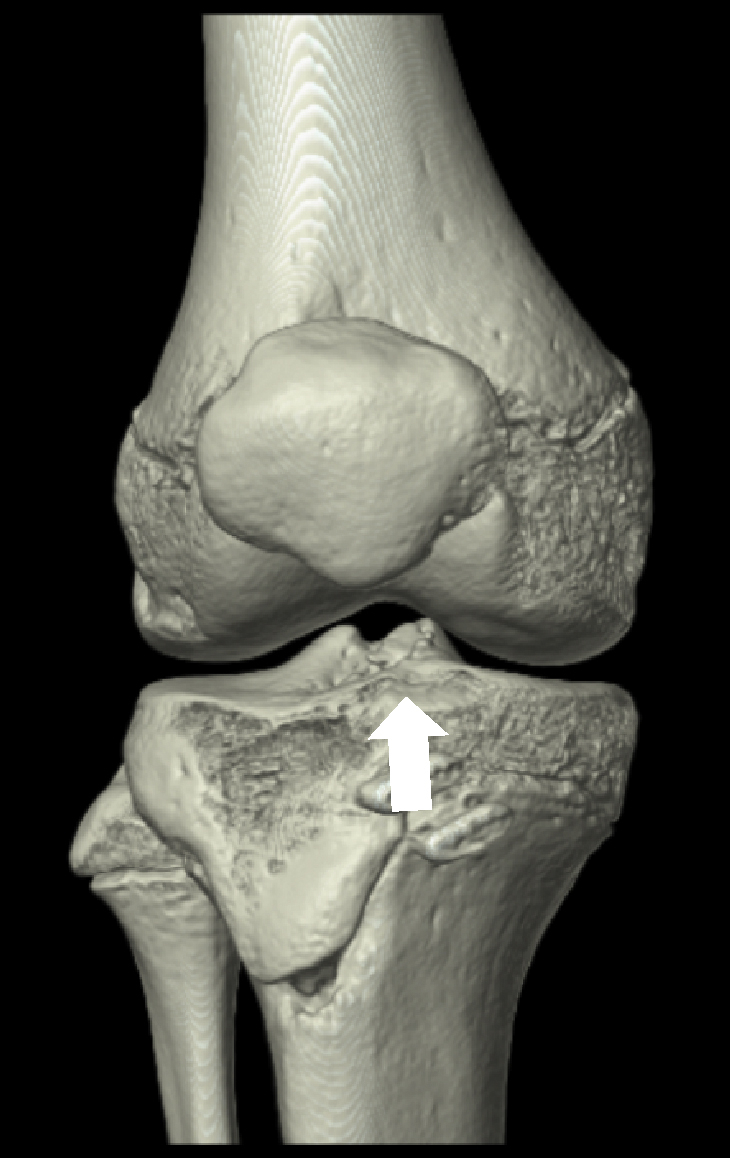
Fig 3.

A 3-dimensional computed tomography scan of the right knee shows a displaced tibial eminence avulsion fracture (arrow).
The patient, under general anesthesia, is placed in the supine position on an operative table with a standard leg holder (Mizuho, Tokyo, Japan) allowing full range of motion. Standard knee arthroscopy is performed with anterolateral and anteromedial portals. Initially, a complete diagnostic arthroscopy is performed. The ACL is probed to ensure that the femoral attachment is intact and there is no intraligamentous tear. A 3.5-mm shaver (Smith & Nephew Endoscopy, Andover, MA) is used to remove the fracture debris and blood clots so that the avulsed bone fragment and fracture site are well visualized (Fig 4). Trial reduction of the avulsed fragment is performed with a probe. After trial reduction, No. 2 FiberWire suture (Arthrex, Naples, FL) is attached to a Scorpion suture passer (Arthrex) (Fig 5).
Fig 4.

The patient, under general anesthesia, is placed in the supine position on an operative table with a standard leg holder (Mizuho) allowing full range of motion. Standard knee arthroscopy is performed with anterolateral and anteromedial portals. Initially, a complete diagnostic arthroscopy is performed. The anterior cruciate ligament is probed to ensure that the femoral attachment is intact and there is no intraligamentous tear. A 3.5-mm shaver (Smith & Nephew Endoscopy) is used to remove the fracture debris and blood clots so that the avulsed bone fragment and fracture site (arrow) are well visualized.
Fig 5.

No. 2 FiberWire suture is attached to the Scorpion suture passer (arrow).
Reduction With Suture
The Scorpion suture passer with attached No. 2 FiberWire suture is used to tie suture to the ACL near the base of its insertion on the fragment. Thereafter, a small incision is made medial to the tibial tubercle. A 2.4-mm Kirschner wire is drilled from medial to the tibial tubercle to the anterior half of the bony fracture bed of the tibia by using an ACL guide. The suture is pulled out through the tibial tunnel with a suture retriever (Smith & Nephew Endoscopy) or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon (Bearmedic, Tokyo, Japan). Anatomic reduction of the avulsed fracture can be obtained by pulling down the FiberWire (Fig 6). This technique was reported by Gamboa et al.7 and is effective especially for type II fractures. Temporary fixation is performed with or without use of an EndoButton (Smith & Nephew Endoscopy) at the anterior surface of the tibia.
Fig 6.

The Scorpion suture passer with attached No. 2 FiberWire suture is used to tie suture to the anterior cruciate ligament near the base of its insertion on the fragment. Thereafter, a small incision is made medial to the tibial tubercle. A 2.4-mm Kirschner wire is drilled from medial to the tibial tubercle to the anterior half of the bony fracture bed of the tibia by using an anterior cruciate ligament guide. The suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon. Anatomic reduction of the avulsed fracture can be obtained by pulling down the FiberWire (arrow).
Tensioning and Fixation
Two other tunnels are created on the medial and lateral side of the fracture bed with a standard ACL guide (Arthrex or Smith & Nephew Endoscopy) using a 2.4-mm Kirschner wire. The Scorpion suture passer with attached No. 2 FiberWire suture is used to stitch the ACL again, and a second suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon (Fig 7). Then, the second suture is tied over the tibial cortex regardless of the knee flexion angle. Thereafter, a tensioning technique (Tighting Gun TGL; Alfresa Pharma, Osaka, Japan) is used for appropriate tensioning with or without an EndoButton (Fig 8).
Fig 7.

Two tunnels are created on the medial and lateral side of the fracture bed with a standard anterior cruciate ligament guide (Arthrex or Smith & Nephew Endoscopy) using a 2.4-mm Kirschner wire. The Scorpion suture passer with attached No. 2 FiberWire suture is used to stitch the anterior cruciate ligament again, and a second suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon (arrow).
Fig 8.

A tensioning technique (Tighting Gun TGL) is used for appropriate tensioning (right knee). After temporary fixation, knee stability is evaluated with the Lachman test. Final tensioning is performed with the Tighting Gun (arrow) regardless of the knee flexion angle again, if necessary. The tension of the anterior cruciate ligament should be confirmed with a probe under direct arthroscopic visualization. Last, the first and second sutures are tied over the tibial cortex.
Examination and Final Fixation
After temporary fixation, knee stability is evaluated with the Lachman test. Final tensioning is performed with the Tighting Gun regardless of the knee flexion angle again, if necessary. The tension of the ACL should be confirmed with a probe under direct arthroscopic visualization. Last, the first and second sutures are tied over the tibial cortex.
Postoperative Management
The knee is immobilized in full extension in a brace for 2 weeks after the operation; then, range-of-motion exercise is started gradually. Partial weight bearing in the brace is allowed as tolerated with crutch support after 2 weeks. Full weight bearing is allowed at postoperative week 4. Isometric quadriceps muscle exercises should be performed throughout the immobilization period to minimize muscle atrophy. Postoperative CT shows that anatomic reduction is obtained (Figs 9 and 10).
Fig 9.

Postoperative computed tomography should be performed to evaluate the reduction of the fragment. A postoperative computed tomography scan of the right knee in the sagittal plane shows anatomic reduction of the fragment (arrow).
Fig 10.
A postoperative 3-dimensional computed tomography scan shows that anatomic reduction (arrow) is obtained.
Discussion
If a tibial eminence avulsion fracture is not well treated, it can result in some complications such as nonunion, limited range of motion, and anterior instability of the knee. Although open reduction–internal fixation had traditionally been performed for displaced fractures, McLennan8 reported the usefulness of arthroscopic reduction in 1982 and emphasized its advantages including less invasiveness and rapid recovery of knee function compared with open surgery. Van Loon and Marti9 used a drill guide for knee ligament reconstruction in arthroscopic fixation for tibial eminence avulsion fractures. Since then, arthroscopic fixation has been more common. Multiple surgical fixation devices such as Kirschner wires, metal screws, steel wires, sutures, and suture anchors have been described for tibial eminence avulsion fractures. Although multiple techniques for arthroscopic reduction and internal fixation have been developed, there is no gold standard.10 Suture fixation and screw fixation are the most commonly described fixation techniques, and both have yielded satisfactory results.11, 12 Liao et al.13 reported that there were no significant differences between nonabsorbable suture fixation and absorbable suture anchor fixation in terms of the clinical efficacy of arthroscopic tibial eminence fracture treatment. In adults with large bony fragments, screw fixation provides robust fixation strength.14, 15 However, in children with small or comminuted fragments, screw fixation is usually not available. Arthroscopic pullout suture techniques should be indicated for small or comminuted fragments,6, 11 although these surgical techniques are often difficult. With our technique, it is easy to obtain and maintain the appropriate tensioning and fixation.
There are some key points in this technique (Table 2). First, the tightening device should be used for gradual tensioning. Second, it is important to avoid over-tensioning the first suture to prevent posterior translation of the fragment. Third, it is not necessary for the surgeon to take care of the knee flexion angle at the time of fixation. Last, the surgeon can confirm the suture movement and ACL tension under direct arthroscopic visualization. The advantages of the technique are that preparation for the procedure is easy, gradual tensioning can be performed while checking the tension of the ACL, the procedure is safe and easy for the patient, and the technique does not take much time.
Table 2.
Key Points, Advantages, and Limitations of Procedure Based on Our Experience
| Key points |
| The tightening device should be used for gradual tensioning. |
| Over-tensioning the first suture should be avoided to prevent posterior translation of the fragment. |
| It is not necessary for the surgeon to take care of the knee flexion angle at the time of fixation. |
| The surgeon should confirm the suture movement and ACL tension under direct arthroscopic visualization. |
| Advantages |
| Preparation for the procedure is easy. |
| Gradual tensioning can be performed while checking the tension of the ACL. |
| The procedure is safe and easy for the patient. |
| The technique does not take much time. |
| Limitations |
| The threshold of suture tension for this procedure is unknown. |
| It is difficult for the surgeon to loosen the tension of the suture after tensioning. |
ACL, anterior cruciate ligament.
Despite having numerous advantages, our technique has several limitations. Specifically, the threshold of suture tension for this procedure is unknown. Therefore, surgeons should take caution to avoid suture rupture during tensioning using the tightening device. It is difficult for surgeons to loosen the tension of the suture after tensioning. Gradual tensioning is thus a key issue to prevent over-tightening or loosening of intraoperative tension. Nevertheless, the described technique can facilitate the reduction of tibial eminence avulsion fractures and acquisition of appropriate tensioning of the ACL.
Acknowledgment
The authors thank Hiroaki Suzuki for editorial assistance in the preparation of the article.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article. Full ICMJE author disclosure forms are available for this article online, as supplementary material.
Supplementary Data
Standard knee arthroscopy is performed with anterolateral and anteromedial portals. Initially, a complete diagnostic arthroscopy is performed (left knee in case 1 and right knee in case 2). The anterior cruciate ligament (ACL) is probed to ensure that the femoral attachment is intact and there is no intraligamentous tear. Trial reduction of the avulsed fragment is performed with a probe. After trial reduction, No. 2 FiberWire suture is attached to a Scorpion suture passer. The Scorpion suture passer with attached No. 2 FiberWire suture is used to tie suture to the ACL near the base of its insertion on the fragment. Thereafter, a small incision is made medial to the tibial tubercle. A 2.4-mm Kirschner wire is drilled from medial to the tibial tubercle to the anterior half of the bony fracture bed of the tibia by using an ACL guide. The suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon. Anatomic reduction of the avulsed fracture can be obtained by pulling down the FiberWire. Temporary fixation is performed with or without use of an EndoButton at the anterior surface of the tibia. Two other tunnels are created on the medial and lateral side of the fracture bed with a standard ACL guide (Arthrex or Smith & Nephew Endoscopy) using a 2.4-mm Kirschner wire. A Scorpion suture passer with attached No. 2 FiberWire suture is used to stitch the ACL again, and a second suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon. Then, the second suture is tied. Thereafter, a tensioning technique (Tighting Gun TGL) is used for appropriate tensioning with or without an EndoButton.
References
- 1.Zaricznyj B. Avulsion fracture of the tibial eminence: Treatment by open reduction and pinning. J Bone Joint Surg Am. 1977;59:1111–1114. [PubMed] [Google Scholar]
- 2.Gronkvist H., Hirsch G., Johansson L. Fracture of the anterior tibial spine in children. J Pediatr Orthop. 1984;4:465–468. doi: 10.1097/01241398-198408000-00015. [DOI] [PubMed] [Google Scholar]
- 3.Kendall N.S., Hsu S.Y., Chan K.M. Fracture of the tibial spine in adults and children. A review of 31 cases. J Bone Joint Surg Br. 1992;74:848–852. doi: 10.1302/0301-620X.74B6.1447245. [DOI] [PubMed] [Google Scholar]
- 4.Meyers M.H., McKeever F.M. Fracture of the intercondylar eminence of the tibia. J Bone Joint Surg Am. 1959;41:209–220. discussion 220-222. [PubMed] [Google Scholar]
- 5.Binnet M.S., Gurkan I., Yilmaz C., Karakas A., Cetin C. Arthroscopic fixation of intercondylar eminence fractures using a 4-portal technique. Arthroscopy. 2001;17:450–460. doi: 10.1053/jars.2001.23573. [DOI] [PubMed] [Google Scholar]
- 6.Hunter R.E., Willis J.A. Arthroscopic fixation of avulsion fractures of the tibial eminence: Technique and outcome. Arthroscopy. 2004;20:113–121. doi: 10.1016/j.arthro.2003.11.028. [DOI] [PubMed] [Google Scholar]
- 7.Gamboa J.T., Durrant B.A., Pathare N.P., Shin E.C., Chen J.L. Arthroscopic reduction of tibial spine avulsion: Suture lever reduction technique. Arthrosc Tech. 2017;6:e121–e126. doi: 10.1016/j.eats.2016.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.McLennan J.G. The role of arthroscopic surgery in the treatment of fractures of the intercondylar eminence of the tibia. J Bone Joint Surg Br. 1982;64:477–480. doi: 10.1302/0301-620X.64B4.6896515. [DOI] [PubMed] [Google Scholar]
- 9.van Loon T., Marti R.K. A fracture of the intercondylar eminence of the tibia treated by arthroscopic fixation. Arthroscopy. 1991;7:385–388. doi: 10.1016/0749-8063(91)90009-m. [DOI] [PubMed] [Google Scholar]
- 10.Sawyer G.A., Anderson B.C., Paller D., Schiller J., Eberson C.P., Hulstyn M. Biomechanical analysis of suture bridge fixation for tibial eminence fractures. Arthroscopy. 2012;28:1533–1539. doi: 10.1016/j.arthro.2012.02.020. [DOI] [PubMed] [Google Scholar]
- 11.Lubowitz J.H., Elson W.S., Guttmann D. Part II: Arthroscopic treatment of tibial plateau fractures: Intercondylar eminence avulsion fractures. Arthroscopy. 2005;21:86–92. doi: 10.1016/j.arthro.2004.09.031. [DOI] [PubMed] [Google Scholar]
- 12.Seon J.K., Park S.J., Lee K.B. A clinical comparison of screw and suture fixation of anterior cruciate ligament tibial avulsion fractures. Am J Sports Med. 2009;37:2334–2339. doi: 10.1177/0363546509341031. [DOI] [PubMed] [Google Scholar]
- 13.Liao W., Li Z., Zhang H., Li J., Wang K., Yang Y. Arthroscopic fixation of tibial eminence fractures: A clinical comparative study of nonabsorbable sutures versus absorbable suture anchors. Arthroscopy. 2016;32:1639–1650. doi: 10.1016/j.arthro.2016.01.032. [DOI] [PubMed] [Google Scholar]
- 14.Pan R.Y., Yang J.J., Chang J.H., Shen H.C., Lin L.C., Lian Y.T. Clinical outcome of arthroscopic fixation of anterior tibial eminence avulsion fractures in skeletally mature patients: A comparison of suture and screw fixation technique. J Trauma Acute Care Surg. 2012;72:E88–E93. doi: 10.1097/TA.0b013e3182319d5a. [DOI] [PubMed] [Google Scholar]
- 15.Wiegand N., Naumov I., Vamhidy L., Not L.G. Arthroscopic treatment of tibial spine fracture in children with a cannulated Herbert screw. Knee. 2014;21:481–485. doi: 10.1016/j.knee.2013.12.004. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Standard knee arthroscopy is performed with anterolateral and anteromedial portals. Initially, a complete diagnostic arthroscopy is performed (left knee in case 1 and right knee in case 2). The anterior cruciate ligament (ACL) is probed to ensure that the femoral attachment is intact and there is no intraligamentous tear. Trial reduction of the avulsed fragment is performed with a probe. After trial reduction, No. 2 FiberWire suture is attached to a Scorpion suture passer. The Scorpion suture passer with attached No. 2 FiberWire suture is used to tie suture to the ACL near the base of its insertion on the fragment. Thereafter, a small incision is made medial to the tibial tubercle. A 2.4-mm Kirschner wire is drilled from medial to the tibial tubercle to the anterior half of the bony fracture bed of the tibia by using an ACL guide. The suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon. Anatomic reduction of the avulsed fracture can be obtained by pulling down the FiberWire. Temporary fixation is performed with or without use of an EndoButton at the anterior surface of the tibia. Two other tunnels are created on the medial and lateral side of the fracture bed with a standard ACL guide (Arthrex or Smith & Nephew Endoscopy) using a 2.4-mm Kirschner wire. A Scorpion suture passer with attached No. 2 FiberWire suture is used to stitch the ACL again, and a second suture is pulled out through the tibial tunnel with a suture retriever or 18-gauge needle with loop suture made of No. 2-0 monofilament nylon. Then, the second suture is tied. Thereafter, a tensioning technique (Tighting Gun TGL) is used for appropriate tensioning with or without an EndoButton.