

Abstract
Background
With aging, the ability to generate muscle force decreases, contributing to declines in physical functions such as walking. While most studies assess muscle force by peak torque, the rate of torque development (RTD) reflects a dynamic component of muscle performance that is important for physical function. Using data from the Baltimore Longitudinal Study of Aging, we assessed whether RTD adds significantly to peak torque in associations with lower extremity performance. If so, RTD may help identify weak older adults for screening and intervention.
Methods
We assessed associations of RTD and peak torque with physical performance independent of demographics, BMI, body composition, and each other in 1089 Baltimore Longitudinal Study of Aging participants (49.7% women; aged 26 to 96 years; women, 64.0 ± 13.8 years; men, 68.4 ± 14.4 years). Peak torque was assessed by isometric and 30 deg/s isokinetic knee extension tests. Peak RTD was operationalized as the maximum torque‐time slope among successive 50 ms epochs over the first 3 s of a test of knee extension isometric strength, with the knee joint positioned at 120 deg of flexion. A battery of lower extremity performance tests included gait speed during a 6 m walk at usual and fast pace (6 m usual and fast), time to complete a 400 m walk at fast pace (400 m), distance covered in a 2.5 min walk at normal pace (2.5 min), time to complete 5 and 10 chair stands, and two summary tests of lower extremity performance. Sex‐stratified generalized linear regression models were adjusted for age, race, BMI, appendicular lean mass, and whole body fat mass.
Results
In men, independent of either measure of peak torque and cofactors, RTD was a significant (P < 0.05) predictor of all lower extremity performance tests except the 400 m and 2.5 min walks. In women, independent of peak torque, RTD was only a significant independent correlate of the 6 m fast walk (P < 0.001).
Conclusions
RTD independently contributes to physical functions in men but less in women. The mechanisms underlying the sex difference are unclear and require further study.
Keywords: Aging, Muscle contraction, Muscle strength, Dynamometry, Walking, Physical performance, Sex difference
Introduction
With aging, the ability to generate muscle force decreases in magnitude and speed, leading to problems with walking and balance, and ultimately, to an increased risk of disability.1, 2, 3 Muscle force is frequently assessed as peak torque during isometric, isokinetic, or isotonic muscle contractions; these assessments do not account for speed of contraction. While peak torque is a strong predictor of physical functions,4, 5 the speed of force development may contribute independently to performance, especially in tasks that require rapid force development, such as brisk walking or jumping. One way to account for speed is to assess muscle power, an average measure of force and velocity of movement in tasks conducted at rapid speed. In cross‐sectional studies, leg muscle power is superior to pure measures of strength in predicting mobility performance.2, 6 However, assessing muscle power requires special equipment and many standard tests for measuring power, such as a vertical or long jump may be risky in older adults.7
Assessing the rate of torque development (RTD) represents a valid alternative to muscle power because it captures the maximal rather than average value, incorporating both force and speed of contraction. Much equipment for testing muscle strength records the time course of force development which can be used to assess the rate of doing work. RTD during isometric contraction is widely used in sports research.8, 9, 10 In contrast to muscle power, RTD can be assessed during an isometric contraction (i.e. without external mechanical movement) so is easy and safe to perform in older adults and in a variety of settings.11, 12 Thus, RTD offers potential to inform studies of aging because it captures the speed‐related, dynamic component of muscle performance in a safe and feasible manner.13, 14, 15, 16
Rate of torque development is known to affect lower extremity performance in patients with stroke or cerebral palsy.17, 18, 19 However, these studies have been small and do not address aging in general. Additionally, because it is likely that age, sex, and peak torque contribute to both RTD and lower extremity performance,5, 15, 20, 21 the contribution of RTD to physical performance should be evaluated after adjusting for these potential confounders.
Our aim is to investigate whether, after adjusting for relevant confounders and isometric or isokinetic knee extension peak torque, RTD assessed during a test of knee extensor isometric strength is independently associated with measures of lower extremity performance. Addressing this hypothesis is important to better clarify whether RTD can be useful as a diagnostic tool or as a parameter for tracking the effectiveness of interventions such as those aimed at improving physical function in older persons.
Methods
Participants
The Baltimore Longitudinal Study of Aging (BLSA) is a prospective observational cohort study designed to investigate the aging process and to identify mechanisms underlying the decline of physical and cognitive function that occur with aging in humans.22 Between April 2003 and February 2011, 1089 BLSA participants (49% women; 26–96 years old) performed isometric knee extension strength. The BLSA study began measuring physical performance between January 2006 and July 2007 (see legend in Table 1). During one 3 day visit, participants undergo a variety of tests, including strength and body composition. We used data from the most recent visit with data on isometric knee extension strength. The BLSA protocol was approved by the Institutional Review Board of record at the time of data collection (MedStar Health Research Institute, Baltimore, MD or National Institute of Environmental Health Sciences, NC), and written informed consent was obtained from all participants.
Table 1.
Participant characteristics
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | ± | SD | n | Mean | ± | SD | n | |
| Age (years) | 68.4 | ± | 14.4 | 548 | 64.0 | ± | 13.8 | 541 |
| Race (black, %) | 24.3 | 548 | 34.6 | 541 | ||||
| Body height (cm) | 175.5 | ± | 7.4 | 548 | 162.8 | ± | 6.2 | 541 |
| Body weight (kg) | 84.5 | ± | 14.7 | 548 | 71.0 | ± | 14.6 | 541 |
| Whole body fat mass (kg)a | 25.5 | ± | 9.6 | 520 | 28.8 | ± | 10.6 | 516 |
| ALM (kg)a | 25.1 | ± | 3.9 | 520 | 17.0 | ± | 3.3 | 516 |
| 400 m walk (s) | 258.8 | ± | 60.4 | 315 | 272.4 | ± | 54.9 | 270 |
| 2.5 min walk (m) | 186.1 | ± | 30.1 | 312 | 182.9 | ± | 30.0 | 259 |
| 6 m fast (m/s) | 1.80 | ± | 0.46 | 405 | 1.70 | ± | 0.35 | 385 |
| 6 m usual (m/s) | 1.12 | ± | 0.27 | 409 | 1.14 | ± | 0.25 | 386 |
| HABCPPB (/4 points) | 2.78 | ± | 0.73 | 398 | 2.87 | ± | 0.63 | 382 |
| CS5pace (times/s) | 0.49 | ± | 0.20 | 406 | 0.50 | ± | 0.17 | 388 |
| CS10pace (times/s) | 0.46 | ± | 0.18 | 405 | 0.46 | ± | 0.15 | 385 |
| SPPB (0–12 points) | 11.1 | ± | 1.9 | 395 | 11.3 | ± | 1.6 | 385 |
| Isometric peak torque (Nm)b | 171.1 | ± | 56.9 | 548 | 117.9 | ± | 37.3 | 541 |
| Concentric, isokinetic peak torque at 30 deg/s (Nm) | 148.7 | ± | 55.5 | 460 | 102.2 | ± | 35.2 | 472 |
| Peak RTD (Nm/s)b | 886.1 | ± | 476.2 | 548 | 511.8 | ± | 285.4 | 541 |
ALM, appendicular lean mass; CS5pace, the timed chair stands per second for five stands; CS10pace, the timed chair stands per second for 10 stands; HABCPPB, health ABC physical performance battery; RTD, rate of torque development; SD, standard deviation; SPPB, short physical performance battery; 2.5 min walk, the distance covered by 2.5 min walk at usual pace; 400 m walk, time to complete 400 m walk at fast pace; 6 m fast, gait speed at fast pace in 6 m; 6 m usual, gait speed at usual pace in 6 m.
measured by dual energy X‐ray absorptiometry.
measured by using an isokinetic dynamometer.
Assessment of 400 m walk started from April 2007. The 2.5 min walk started from July 2007. The 6 m gait tests, SPPB, and CS tests started from January 2006. HABCPPB started from January 2006.
Knee extension peak torques and rate of torque development assessments
Participants performed three trials of isometric knee extension at a knee angle of 120 deg with 15 s breaks between trials using a Kin‐Com® isokinetic dynamometer (Kin‐Com model 125E, version 3.2, Chattanooga Group, Chattanooga, TN).23, 24 In the isometric test, participants were asked to extend their knee as hard as possible for 3 s with an instructor's verbal encouragement.25, 26
All signals were sampled at 100 Hz. After exporting the raw data, torque time trajectories were smoothed with a 5‐point moving average (50 ms epochs). The percent change compared with each previous time point was calculated, and the onset of force production was defined as the time point at which the percent change ≥3.0%, and time after force onset was divided into 50 ms epochs (i.e. 0–50, 50–100, 100–150, …, 2950–3000 ms). Then, RTD was calculated as the slope of the torque–time relationship (Δtorque/0.05 s) within each epoch. Finally, peak RTD was defined as the highest value across epochs. We excluded trials that lacked a period of no change in torque >1 Nm for at least 100 ms prior to the force onset. For each trial in which RTD was calculated, isometric peak torque was defined as the peak value during that trial. We selected the trial with the highest peak torque from either leg for both RTD and isometric peak torque.
In addition, participants performed three sets of isokinetic concentric knee extension at 30 deg/s using the Kin‐Com, with 15 s rest periods between trials. Concentric, isokinetic peak torque was defined as the highest value of torque from the same leg as the isometric test.
Lower extremity performance
Lower extremity performance was assessed in several ways. Gait speed was defined as distance divided by time to the tenth of a second. The 6 m walk at usual pace test (6 m usual) was performed before the 6 m walk at fast pace test (6 m fast). Participants stood with their toes just touching the start line, with ‘Ready? Go’, they walked from the tape line at the start to the one at the end of the course. The tests used a stopwatch to capture the time between the first footfall over the start line and the first footfall across or touching the finish line. We also collected data on a 400 m walk at fast pace (400 m, s), distance covered in a 2.5 min walk at normal pace (2.5 min, metre).27, 28 For these two tests, a 20 m walking course was set with two fluorescent orange traffic cones at each end and tape marking each metre between the cones. The examiner used a stopwatch to measure the total time to complete in 400 m walk. In 400 m walk, the examiner stopped timing when the first footfall crossed the finish line. For the 2.5 min walk, the examiner counted the number of laps and metre mark on the floor. Time started at the participants first footfall over the starting line. Standard encouragement was offered after each lap.
For the timed chair stands, participants were asked to stand all the way up and sit all the way down 10 times as quickly as possible while keeping their arms folded across their chests. We used a straight back, flat, level, firm seat 45 cm in height. The times to complete 5 and 10 stands (CS5pace and CS10pace, respectively, times per second) were recorded using a stopwatch. The examiner started timing as soon as saying ‘Go’ and stopped after 10 chair stands were completed. Time to complete five stands was recorded using the split button on the stopwatch. Global lower extremity performance was measured by the Short Physical Performance Battery (SPPB)29 and the Health ABC Physical Performance Battery (HABC PPB) tests.27 SPPB is composed of three standing balance tasks, 6m walking speed at usual pace, and a 5‐time chair stand test. Results are converted to a score ranging from 0 (worst) to 12 (best) points based on predefined cut‐off thresholds in each test. HABC PPB is an extended version of the SPPB aimed at minimizing a ceiling effect by increasing the number of chair stands and including more difficult balance tasks. The score of HABC PPB ranges from 0 (worst) to 4 (best).
Most participants completed the test in about 20 min including instructions and examiner demonstration. Participants could rest between tests as desired.
Body composition
A whole‐body dual‐energy X‐ray absorptiometry (Prodigy Dual Photon X‐ray Absorptiometry unit, General Electric, Milwaukee, WI) with DICOM software ver. 10.51.006 with the array mode was performed to obtain measures of whole body fat mass and appendicular lean mass (ALM) (sum of arm and leg lean mass) as previously described.26
Statistical analysis
Descriptive data are presented as the mean ± standard deviation or percentages. Normality and equal assumptions were verified using the Kolmogorov–Smirnov and Levene tests, respectively. Differences according to sex were assessed with unpaired t‐test for continuous variables and chi‐square tests for categorical variables. Peak RTD was log‐transformed due to skewness. However, untransformed data were used in analyses that explored age‐related differences.
First, we used a non‐parametric strategy to explore the relationship between age and various measures of muscle strength, using locally weighted regression smoothers, LOWESS using the SAS PROC LOESS.4 Second, to test for non‐linearity of the relationship between age and these measures, we fitted quadratic regression models. Third, in only the relationships where the quadratic term significantly increased model fit, we performed piecewise regression with the Marquardt method to test the hypothesis that, on average, decline over time of these strength measures becomes steeper after a certain age. The critical age for slope change was identified using PROC NLIN in SAS, and the 95% confidential interval was calculated by using bootstrap method (resample = 2000).
Sex‐specific generalized linear regression models were used to assess the cross‐ sectional associations of RTD or isometric peak torque with each lower extremity performance. In Model 1, we examined the associations between RTD with each lower extremity performance after adjusting for age, race (blacks vs. other races), and body mass index (BMI, kg/m2). In Model 2, we examined the associations between isometric peak torque and each lower extremity performance after adjusting for the same variables in Model 1. Model 3 included both RTD and isometric peak torque and all potential confounders in Model 1. Model 4 further adjusted for ALM and whole body fat mass and all variables from Model 3.
We also examined the cross‐sectional associations of RTD or isokinetic peak torque with each lower extremity performance by using the same sequence of analyses reported earlier.
Based on the initial exploratory analyses, we assumed that both muscle strength measures and lower extremity performance would decline and be related, predominantly later in life. Thus, we performed sensitivity analyses for the subgroup based on the age breakpoints identified earlier, to determine if the primary findings using the total study population were robust.
Statistical Analysis Software (SAS) version 9.4 for Windows (SAS Institute, Inc., Cary, NC) was used for all data processing and statistical analyses. The level of statistical significance was set as P < 0.05 (two‐sided).
Results
The characteristics of the study population are presented in Table 1. Compared with female participants, male participants were older and had greater strength in all strength measures, as well as better physical performance. The relationship between age and measures of peak RTD, isometric peak torque, or isokinetic peak torque in men and women are depicted in Figures 1 and S2.
Figure 1.
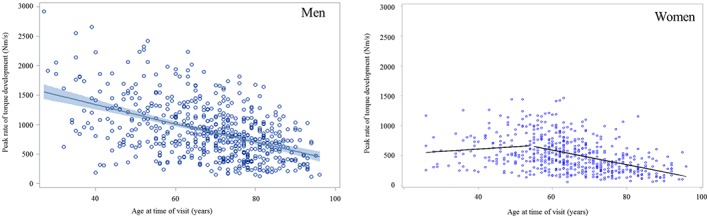
Relationship between age and peak rate of torque development. In men, the solid line is a locally weighted regression smoother with 95% confidence interval. In women, the solid line is a piecewise regression with a breakpoint estimated at 55.1 (48.9–62.1) years old.
In men, peak RTD declined significantly with age (βage = −15.9, P < 0.0001, R 2 = 0.23). The decline was linear, as indicated by the lack of improvement in fit when a quadratic term for age was included in the model (βage2 = 0.05, P = 0.48, R 2 = 0.23). Isometric peak torque also declined with age (βage = −2.3, P < 0.0001, R 2 = 0.33), but the introduction of a quadratic term for age significantly improved the fit of the model (βage2 = −0.02, P = 0.02, R 2 = 0.34), with a steeper decline after the age of 63.0 [95% confidence interval, CI 51.2–74.8] (see Supporting Information, Figure S2a). Isokinetic peak torque also declined with age (βage = −2.1, P < 0.0001, R 2 = 0.31). The relationship was non‐linear (βage2 = −0.03, P = 0.006, R 2 = 0.32), with significantly steeper decline after the age of 63.0 years [95% CI: 51.9–74.0] (see Supporting Information, Figure S3).
In women, peak RTD, isometric peak torque, and isokinetic peak torque declined with age (RTD, βage = −8.0, P < 0.0001, R 2 = 0.15; isometric peak torque, βage = −1.3, P < 0.0001, R 2 = 0.22; isokinetic peak torque, βage = −1.2, P < 0.0001, R 2 = 0.22), and all declines were non‐linear (RTD, βage2 = −0.2, P < 0.0001, R 2 = 0.18; isometric peak torque, βage2 = −0.03, P < 0.001, R 2 = 0.26; isokinetic peak torque, βage2 = −0.03, P < 0.0001, R 2 = 0.26), with accelerated decline after 55.1 years [95% CI: 48.9–62.1] for RTD, 61.9 years [95% CI: 55.0–67.7] for isometric peak torque, and after 61.0 years [95% CI: 54.0–68.0] for isokinetic peak torque (Figure 1 and see Supporting Information, Figures S2b and S3b). Based on these analyses, we created a subgroup of older participants assuming that declines in strength and function accelerate, on average after the age of 60.
Next, we examined relationships between RTD and isometric peak torque with lower extremity performance (Tables 2a and 2b), separately in men and women, using multivariate linear regression models adjusting for age, race, and BMI. When examined separately, isometric peak torque and RTD were significantly associated with all lower extremity performance measures. When RTD and isometric peak torque were included in the same model, results differed by sex (Tables 2a and 2b and Model 3). In men, RTD remained a significant independent predictor of all lower extremity performance measures, except the 400 m (P = 0.21) and the 2.5 min (P = 0.19) walks. After further adjusting for ALM and fat mass, results were substantially unchanged (Model 4). However, in women, when RTD and isometric peak torque were included in the same model, RTD was no longer a significant correlate of most lower extremity performance tests, except the 6 m fast walk (P = 0.01) (Model 3). In the same models, isometric peak torque was a significant independent correlate of performance in the 400 m walk, the 6 m fast walk, and chair stand tests. These findings were substantially unchanged after adjusting for body composition (Model 4).
Table 2a.
The relationship of rate of torque development or isometric knee extension peak torque with physical performance tests in men
| Men | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||||||
| RTDa | ISOM | RTDa | ISOM | RTDa | ISOM | |||||||||||
| β | P value | R 2 | β | P value | R 2 | β | P value | β | P value | R 2 | β | P value | β | P value | R 2 | |
| 400 m walk (s) (n = 311) | −0.17 | 0.001 | 0.44 | −0.23 | <0.0001 | 0.46 | −0.07 | 0.21 | −0.18 | 0.003 | 0.46 | −0.07 | 0.18 | −0.14 | 0.03 | 0.47 |
| 2.5 min walk (m) (n = 308) | 0.15 | 0.01 | 0.26 | 0.17 | 0.01 | 0.26 | 0.09 | 0.19 | 0.11 | 0.14 | 0.26 | 0.09 | 0.19 | 0.07 | 0.35 | 0.27 |
| 6 m fast (m/s) (n = 396) | 0.24 | <0.0001 | 0.40 | 0.29 | <0.0001 | 0.41 | 0.14 | 0.01 | 0.20 | 0.001 | 0.42 | 0.14 | 0.01 | 0.20 | 0.002 | 0.42 |
| 6 m usual (m/s) (n = 399) | 0.22 | <0.0001 | 0.29 | 0.22 | <0.0001 | 0.28 | 0.16 | 0.01 | 0.11 | 0.08 | 0.30 | 0.16 | 0.01 | 0.10 | 0.17 | 0.30 |
| HABCPPB (n = 390) | 0.23 | <0.0001 | 0.39 | 0.23 | <0.0001 | 0.38 | 0.17 | 0.002 | 0.11 | 0.08 | 0.39 | 0.17 | 0.002 | 0.12 | 0.06 | 0.40 |
| CS5pace (times/s) (n = 396) | 0.18 | 0.0002 | 0.23 | 0.19 | 0.001 | 0.22 | 0.13 | 0.04 | 0.10 | 0.14 | 0.23 | 0.12 | 0.04 | 0.15 | 0.03 | 0.30 |
| CS10pace (times/s) (n = 395) | 0.20 | <0.0001 | 0.23 | 0.23 | <0.0001 | 0.23 | 0.13 | 0.04 | 0.14 | 0.04 | 0.24 | 0.12 | 0.04 | 0.19 | 0.01 | 0.30 |
| SPPB (n = 387) | 0.28 | <0.0001 | 0.24 | 0.24 | <0.0001 | 0.21 | 0.23 | 0.0002 | 0.08 | 0.23 | 0.24 | 0.23 | 0.0002 | 0.08 | 0.30 | 0.25 |
CS5pace, chair stands per second for five stands; CS10pace, chair stands per second for 10 stands; HABCPPB, health ABC physical performance battery; ISOM, peak torque (Nm) measured by isometric knee extension strength at 120 deg; RTD, rate of torque development; SPPB, short physical performance battery; 2.5 min walk, the distance covered by 2.5 min walk at usual pace; 400 m walk, time to complete 400 m walk at fast pace; 6 m fast, gait speed at fast pace in 6 m; 6 m usual, gait speed at usual pace in 6 m.
log transformed. All models, P < 0.0001.
Values are standardized regression coefficient from generalized linear regression models. In each physical performance test, Models 1 and 2 were adjusted for age, race, and body mass index. Model 3 was adjusted for variables in Model 1 + ISOM. Model 4 was adjusted for variables in Model 3 + appendicular lean mass and whole body fat free mass.
Table 2b.
The relationship of rate of torque development or isometric knee extension peak torque with physical function tests in women
| Women | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||||||
| RTDa | ISOM | RTDa | ISOM | RTDa | ISOM | |||||||||||
| β | P value | R 2 | β | P value | R 2 | β | P value | β | P value | R 2 | β | P value | β | P value | R 2 | |
| 400 m walk (s) (n = 260) | −0.20 | <0.0001 | 0.51 | −0.30 | <0.0001 | 0.54 | −0.05 | 0.39 | −0.27 | <0.0001 | 0.54 | −0.06 | 0.33 | −0.23 | 0.001 | 0.54 |
| 2.5 min walk (m) (n = 252) | 0.16 | 0.01 | 0.29 | 0.21 | 0.001 | 0.30 | 0.07 | 0.34 | 0.16 | 0.048 | 0.30 | 0.07 | 0.37 | 0.15 | 0.08 | 0.30 |
| 6 m fast (m/s) (n = 375) | 0.22 | <0.0001 | 0.48 | 0.25 | <0.0001 | 0.48 | 0.12 | 0.01 | 0.16 | 0.003 | 0.49 | 0.13 | 0.01 | 0.13 | 0.03 | 0.50 |
| 6 m usual (m/s) (n = 376) | 0.13 | 0.01 | 0.29 | 0.13 | 0.01 | 0.29 | 0.08 | 0.16 | 0.08 | 0.22 | 0.29 | 0.09 | 0.13 | 0.05 | 0.47 | 0.30 |
| HABCPPB (n = 372) | 0.12 | 0.01 | 0.35 | 0.14 | 0.01 | 0.35 | 0.07 | 0.20 | 0.09 | 0.16 | 0.36 | 0.07 | 0.24 | 0.11 | 0.09 | 0.36 |
| Chair stand test (times/s) | ||||||||||||||||
| CS5pace (times/s) (n = 378) | 0.10 | 0.047 | 0.20 | 0.13 | 0.02 | 0.20 | 0.04 | 0.49 | 0.10 | 0.15 | 0.20 | 0.02 | 0.69 | 0.18 | 0.01 | 0.27 |
| CS10pace (times/s) (n = 375) | 0.11 | 0.03 | 0.25 | 0.17 | 0.002 | 0.26 | 0.03 | 0.68 | 0.15 | 0.02 | 0.26 | 0.00 | 0.97 | 0.25 | 0.0003 | 0.33 |
| SPPB (n = 375) | 0.09 | 0.09 | 0.18 | 0.10 | 0.08 | 0.18 | 0.05 | 0.42 | 0.06 | 0.38 | 0.19 | 0.04 | 0.51 | 0.10 | 0.19 | 0.20 |
CS5pace, chair stands per second for five stands; CS10pace, chair stands per second for 10 stands; HABCPPB, health ABC physical performance battery; ISOM, peak torque (Nm) measured by isometric knee extension strength at 120 deg; RTD, rate of torque development; SPPB, short physical performance battery; 2.5 min walk, the distance covered by 2.5 min walk at usual pace; 400 m walk, time to complete 400 m walk at fast pace; 6 m fast, gait speed at fast pace in 6 m; 6 m usual, gait speed at usual pace in 6 m.
log transformed. All models, P < 0.0001.
Values are standardized regression coefficient from generalized linear regression models. In each physical performance test, Models 1 and 2 were adjusted for age, race, and body mass index. Model 3 was adjusted for variables in Model 1 + ISOM. Model 4 was adjusted for variables in Model 3 + appendicular lean mass and whole body fat free mass.
We then examined relationships between RTD and isokinetic peak torque with lower extremity performance using similar multivariate linear regression models (Tables 3a and 3b). Similar to the results using isometric peak torque, in men, RTD was significantly correlated with all tests of lower extremity performance except the 400 m walk (P = 0.39) and the 2.5 min walk (P = 0.19). Again, in women, RTD was significantly associated with the 6 m fast speed but not with any other lower extremity performance test.
Table 3a.
The relationship of rate of torque development or concentric, isokinetic knee extension at 30 deg/sec with physical function tests in men
| Men | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||||||
| RTDa | ISOK | RTDa | ISOK | RTDa | ISOK | |||||||||||
| β | P value | R 2 | β | P value | R 2 | β | P value | β | P value | R 2 | β | P value | β | P value | R 2 | |
| 400 m walk (sec) (n = 234) | −0.14 | 0.01 | 0.46 | −0.19 | 0.001 | 0.47 | −0.05 | 0.39 | −0.16 | 0.02 | 0.48 | −0.06 | 0.35 | −0.12 | 0.11 | 0.48 |
| 2.5 min walk (m) (n = 226) | 0.14 | 0.03 | 0.22 | 0.14 | 0.06 | 0.22 | 0.11 | 0.19 | 0.07 | 0.42 | 0.22 | 0.11 | 0.19 | 0.03 | 0.72 | 0.23 |
| 6 m fast (m/s) (n = 314) | 0.24 | <0.0001 | 0.38 | 0.28 | <0.0001 | 0.38 | 0.14 | 0.02 | 0.19 | 0.01 | 0.39 | 0.14 | 0.02 | 0.18 | 0.01 | 0.39 |
| 6 m usual (m/s) (n = 317) | 0.22 | <0.0001 | 0.29 | 0.19 | 0.002 | 0.27 | 0.19 | 0.005 | 0.07 | 0.35 | 0.29 | 0.18 | 0.01 | 0.05 | 0.50 | 0.30 |
| HABCPPB (n = 308) | 0.22 | <0.0001 | 0.38 | 0.15 | 0.01 | 0.35 | 0.22 | 0.001 | 0.01 | 0.91 | 0.38 | 0.21 | 0.001 | 0.03 | 0.68 | 0.39 |
| CS5pace (times/s) (n = 314) | 0.17 | 0.003 | 0.22 | 0.11 | 0.08 | 0.20 | 0.17 | 0.01 | 0.00 | 1.00 | 0.22 | 0.15 | 0.02 | 0.07 | 0.36 | 0.28 |
| CS10pace (times/s) (n = 314) | 0.20 | 0.001 | 0.22 | 0.17 | 0.01 | 0.21 | 0.16 | 0.02 | 0.07 | 0.38 | 0.22 | 0.14 | 0.03 | 0.14 | 0.08 | 0.28 |
| SPPB (n = 305) | 0.26 | <0.0001 | 0.23 | 0.18 | 0.004 | 0.20 | 0.24 | 0.001 | 0.03 | 0.68 | 0.23 | 0.24 | 0.001 | 0.04 | 0.63 | 0.24 |
CS5pace, chair stands per second for five stands; CS10pace, chair stands per second for 10 stands; HABCPPB, health ABC physical performance battery; ISOK, peak torque (Nm) measured by concentric, isokinetic knee extension strength at 30 deg/s; RTD, rate of torque development; SPPB, short physical performance battery; 2.5 min walk, the distance covered by 2.5 min walk at usual pace; 400 m walk, time to complete 400 m walk at fast pace; 6 m fast, gait speed at fast pace in 6 m; 6 m usual, gait speed at usual pace in 6 m.
log transformed. All models, P < 0.0001.
Values are standardized regression coefficient from generalized linear regression models. In each physical performance test, Model 1 and 2 were adjusted for age, race, and body mass index. Model 3 was adjusted for variables in Model 1 + ISOK; Model 4 was adjusted for variables in Model 3 + appendicular lean mass and whole body fat free mass.
Table 3b.
The relationship of rate of torque development or concentric, isokinetic knee extension peak torque at 30 deg/sec with physical function tests in women
| Women | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||||||
| RTDa | ISOK | RTDa | ISOK | RTDa | ISOK | |||||||||||
| β | P value | R 2 | β | P value | R 2 | β | P value | β | P value | R 2 | β | P value | β | P value | R 2 | |
| 400 m walk (s) (n = 201) | −0.18 | 0.001 | 0.53 | −0.32 | <.0001 | 0.57 | −0.04 | 0.48 | −0.29 | <.0001 | 0.57 | −0.05 | 0.44 | −0.27 | 0.0004 | 0.57 |
| 2.5 min walk (m) (n = 191) | 0.14 | 0.03 | 0.34 | 0.24 | 0.001 | 0.36 | 0.04 | 0.65 | 0.21 | 0.02 | 0.36 | 0.04 | 0.66 | 0.21 | 0.03 | 0.36 |
| 6 m fast (m/s) (n = 309) | 0.19 | <.0001 | 0.48 | 0.16 | 0.001 | 0.47 | 0.16 | 0.004 | 0.07 | 0.26 | 0.48 | 0.17 | 0.002 | 0.01 | 0.88 | 0.49 |
| 6 m usual (m/s) (n = 310) | 0.10 | 0.048 | 0.31 | 0.05 | 0.38 | 0.31 | 0.11 | 0.07 | −0.02 | 0.78 | 0.32 | 0.12 | 0.05 | −0.06 | 0.45 | 0.32 |
| HABCPPB (n = 306) | 0.11 | 0.03 | 0.37 | 0.14 | 0.01 | 0.37 | 0.06 | 0.32 | 0.10 | 0.14 | 0.37 | 0.06 | 0.34 | 0.11 | 0.13 | 0.37 |
| CS5pace (times/s) (n = 312) | 0.08 | 0.15 | 0.24 | 0.11 | 0.08 | 0.24 | 0.04 | 0.57 | 0.08 | 0.25 | 0.24 | 0.03 | 0.67 | 0.16 | 0.04 | 0.30 |
| CS10pace (times/s) (n = 309) | 0.08 | 0.12 | 0.26 | 0.15 | 0.01 | 0.27 | 0.02 | 0.81 | 0.14 | 0.05 | 0.27 | 0.00 | 0.96 | 0.22 | 0.003 | 0.34 |
| SPPB (n = 309) | 0.08 | 0.18 | 0.20 | 0.11 | 0.07 | 0.20 | 0.03 | 0.69 | 0.10 | 0.19 | 0.20 | 0.02 | 0.76 | 0.13 | 0.11 | 0.21 |
CS5pace, chair stands per second for five stands; CS10pace, chair stands per second for 10 stands; HABCPPB, health ABC physical performance battery; ISOK, peak torque (Nm) measured by concentric, isokinetic knee extension strength at 30 deg/s; RTD, rate of torque development; SPPB, short physical performance battery; 2.5 min walk, the distance covered by 2.5 min walk at usual pace; 400 m walk, time to complete 400 m walk at fast pace; 6 m fast, gait speed at fast pace in 6 m; 6 m usual, gait speed at usual pace in 6 m.
log transformed. All models, P < 0.0001.
Values are standardized regression coefficient from generalized linear regression models. In each physical performance test, Model 1 and 2 were adjusted for age, race, and body mass index. Model 3 was adjusted for variables in Model 1 + ISOK; Model 4 was adjusted for variables in Model 3 + appendicular lean mass and whole body fat free mass.
In sensitivity analyses limited to participants 60 years and older, findings were substantially similar to those that included all participants. Two exceptions were noted. In men older than 60 years, RTD was no longer significantly associated with the chair stand tests. In women, the relationship between RTD and the 6 m fast was no longer significant. (See Supporting Information, Tables S4a and b and S5a)
Discussion
In men, rate of force development, independent of isometric or isokinetic peak torque, is significantly associated with most measures of physical performance, except those that are designed to especially reflect endurance. Surprisingly, in women, RTD was independently correlated with the 6 m fast walk, but not with any other performance test. RTD and peak torque appear to contribute differently by sex to physical performance.
These findings vary in part from prior work, potentially due to differences in populations, how RTD is calculated, or types of performance measures. In a small study of older adults aged 65–80, (38.1% male; n = 21), Altubasi found that knee extension RTD assessed as time from onset to peak torque, rather than by 50 ms epoch, was moderately correlated with stair climbing (r = −0.57) but not with the timed up and go, ramp up, or 4 m walk with usual pace tests.30 In patients affected by multiple sclerosis (26% male; n = 35), Kjolhede et al. failed to demonstrate an independent effect of peak RTD adjusted for body weight on a usual pace 2 min walk after accounting for concentric, isokinetic knee extensor peak torque.31
Why would RTD mostly affect performance on shorter rather than longer tasks? In another study of older adults assessing task‐dependent associations among muscle strength, muscle contraction velocity, and physical function,32 muscle contraction velocity was found to be more important than muscle strength for walking tasks but less important for SPPB.32 In our study, physical performance tests significantly associated with peak RTD did not necessarily represent tasks that require maximum muscle contraction, endurance, or rapid force development. In other words, the contribution of peak RTD to performance seems to be more relevant during short quick movements. Longer activities such as long distance walks require prolonged muscle action and endurance, which depend heavily on the capacity to generate energy over time. The differential relationship of RTD with performance based on energy requirements should be assessed in future studies.
We found important differences in the relationship between RTD and performance by sex. Sex differences in RTD have been reported. In one study, compared with women, men had greater knee extension RTD at 250 ms from force onset.15 Another study, assessing RTD at 150 ms from onset, also reported higher knee extension RTD in men compared with women and suggested that the sex difference might be attribute to muscle size.20 Indeed, various measures of body composition and muscle strength are known to differ by sex and have been reported to predict mobility function better in men than women.33, 34, 35, 36 Because over the life span, women consistently have lower muscle strength and mass relative to body weight, women may use different strategies to move, relying less on pure strength and more on coordination and timing of synergies among muscle groups. Menopause may also play a role in sex differences. As shown in Figure 1, while RTD in men declines linearly with age, in women, RTD starts declining more rapidly around the age of menopause. In animal studies, oestrogen affects the contractile properties of contractile proteins and skeletal muscle, leading to changes in force development.37, 38 Furthermore, there are sex differences in rates of conditions that might alter the effect of strength on performance. Women have higher rates of osteoarthritis and osteoporosis than men, perhaps reducing the influence of strength on mobility performance.39 Other factors that differ by sex include rates of physical activity and the proportion of body weight accounted for by fat, which may affect the capacity to generate muscle power, also resulting in a need to use alternative strategies to move successfully.40 Ultimately, these important sex differences in effects on physical performance should be tested in future studies. The alternative strategies used by women should be explicated. These sex differences could inform how exercise interventions might be tailored to different needs by sex.
Rate of torque development is not yet a standardized test and lacks a protocol that specifies joint angles, verbal instructions, or how to define and use time periods. As a result, absolute RTD values, even when age and sex are similar, vary across the literature. For example, in one study, at a 90 deg knee joint angle, maximum RTD among men in their 40s was 801 Nm/s, while it was 601 Nm/s for men in their 60s.41 In another study at a 120 deg knee joint angle, peak RTD in middle‐aged men (50.6 years) was 1744 Nm/s, while it was 1215 Nm/s in men with an average age in the late 60s.42 The knee joint angle in our study is also 120 deg, but our peak RTD values are lower. One potential difference is the specific verbal instructions used. We asked participants ‘to push as hard as possible’. Higher RTD may be achieved by using the instruction ‘as fast as possible’.43 These variations in how to measure RTD might affect results of tests of associations between RTD and physical performance. Consistent standardization of RTD could provide a way to compare relationships across studies.
Our study has important strengths. Our sample size is large, with a broad distribution of age, sex, and race. To determine independent associations between RTD and performance, we accounted for measures of peak torque and other confounders. We performed a sensitivity analysis to determine how associations might differ in a sample limited to those over age 60. Our study also has limitations. Not all participants completed all the performance tests; 11% did not complete the 400 m walk test due to health status or other problems.28 It is possible that informative censoring might explain the lack of association between RTD and some of the long walks. This initial study is limited to cross‐sectional associations. Although the BLSA assesses multiple aspects of performance, the ability to generate ballistic movements is not assessed. Because in physically active young men, knee extensor RTD is known to correlate with ballistic movements such as 10 m sprint performance (r = −0.66) and jump performance (r = 0.68),44, 45 RTD in our study might have shown associations with tasks that are more dependent on ballistic motion.
We find that, in men, RTD contributes to physical performance independent of peak torque, whether assessed by isokinetic or isometric dynamometry. The role of RTD appears to be stronger in men than women, but the mechanisms underlying this discrepancy remain unclear. Longitudinal studies of both sexes and a broad age range should include standardized measures of RTD, a broader array of performance measures and indicators of other factors that affect performance, especially those related to motor control.
Conflict of interest
Yusuke Osawa, Stephanie A. Studenski, and Luigi Ferrucci declare no conflicts of interest.
Supporting information
Table S4a. Relationship of rate of torque development or isometric knee extension peak torque with physical function tests in men over 60 years old
Table S4b. Relationships of rate of torque development or isometric knee extension peak torque with physical function tests in women over 60 years old
Table S5a. Relationships of rate of torque development or concentric, isokinetic peak torque at 30 deg/s with physical function tests in men over 60 years old
Fig. S2. Relationship between age and peak torque in isometric knee extension at 120 deg. In men, the solid line is a piecewise regression with a breakpoint estimated at 63.0 [51.2‐74.8] years old. In women, the solid line is a piecewise regression with a breakpoint estimated at 61.9 [55.0‐67.7] years old.
Fig. S3. The relationship between age and peak torque in concentric, isokinetic knee extension at 30 deg/s. In men, the solid line is a piecewise regression with a breakpoint estimated at 63.0 [51.9‐74.0] years old. In women, the solid line is a piecewise regression with a breakpoint estimated at 61.0 [54.0‐68.0] years old.
Acknowledgements
This research was supported by the Intramural Research Program of the National Institutes of Health, National Institute on Aging. The authors certify that they comply with the ethical guidelines for authorship and publishing of the Journal of Cachexia, Sarcopenia, and Muscle.46
Osawa, Y. , Studenski, S. A. , and Ferrucci, L. (2018) Knee extension rate of torque development and peak torque: associations with lower extremity function. Journal of Cachexia, Sarcopenia and Muscle, 9: 530–539. doi: 10.1002/jcsm.12285.
References
- 1. Bean JF, Leveille SG, Kiely DK, Bandinelli S, Guralnik JM, Ferrucci L. A comparison of leg power and leg strength within the InCHIANTI study: which influences mobility more? J Gerontol A Biol Sci Med Sci 2003;58:728–733. [DOI] [PubMed] [Google Scholar]
- 2. Byrne C, Faure C, Keene DJ, Lamb SE. Ageing, muscle power and physical function: a systematic review and implications for pragmatic training interventions. Sports Med 2016;46:1311–1332. [DOI] [PubMed] [Google Scholar]
- 3. Mayson DJ, Kiely DK, LaRose SI, Bean JF. Leg strength or velocity of movement: which is more influential on the balance of mobility limited elders? Am J Phys Med Rehabil 2008;87:969–976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ferrucci L, Guralnik JM, Buchner D, Kasper J, Lamb SE, Simonsick EM, et al. Departures from linearity in the relationship between measures of muscular strength and physical performance of the lower extremities: the Women's Health and Aging Study. J Gerontol A Biol Sci Med Sci 1997;52:M275–M285. [DOI] [PubMed] [Google Scholar]
- 5. Visser M, Goodpaster BH, Kritchevsky SB, Newman AB, Nevitt M, Rubin SM, et al. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well‐functioning older persons. J Gerontol A Biol Sci Med Sci 2005;60:324–333. [DOI] [PubMed] [Google Scholar]
- 6. Reid KF, Fielding RA. Skeletal muscle power: a critical determinant of physical functioning in older adults. Exerc Sport Sci Rev 2012;40:4–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Sands WA, McNeal JR, Ochi MT, Urbanek TL, Jemni M, Stone MH. Comparison of the Wingate and Bosco anaerobic tests. J Strength Cond Res 2004;18:810–815. [DOI] [PubMed] [Google Scholar]
- 8. Aagaard P, Simonsen EB, Andersen JL, Magnusson P, Dyhre‐Poulsen P. Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol (1985). 2002;93:1318–1326. [DOI] [PubMed] [Google Scholar]
- 9. Tillin NA, Pain MT, Folland J. Explosive force production during isometric squats correlates with athletic performance in rugby union players. J Sports Sci 2013;31:66–76. [DOI] [PubMed] [Google Scholar]
- 10. Korhonen MT, Cristea A, Alen M, Hakkinen K, Sipila S, Mero A, et al. Aging, muscle fiber type, and contractile function in sprint‐trained athletes. J Appl Physiol (1985). 2006;101:906–917. [DOI] [PubMed] [Google Scholar]
- 11. Sapega AA, Drillings G. The definition and assessment of muscular power. J Orthop Sports Phys Ther 1983;5:7–9. [DOI] [PubMed] [Google Scholar]
- 12. Juneja H, Verma S, Khanna G. Isometric strength and its relationship to dynamic performance: a systematic review. J Exerc Sci Physiother 2012;6:60. [Google Scholar]
- 13. Thompson BJ, Ryan ED, Herda TJ, Costa PB, Herda AA, Cramer JT. Age‐related changes in the rate of muscle activation and rapid force characteristics. Age (Dordr) 2014;36:839–849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. LaRoche DP, Cremin KA, Greenleaf B, Croce RV. Rapid torque development in older female fallers and nonfallers: a comparison across lower‐extremity muscles. J Electromyogr Kinesiol 2010;20:482–488. [DOI] [PubMed] [Google Scholar]
- 15. Ditroilo M, Forte R, Benelli P, Gambarara D, De Vito G. Effects of age and limb dominance on upper and lower limb muscle function in healthy males and females aged 40‐80 years. J Sports Sci 2010;28:667–677. [DOI] [PubMed] [Google Scholar]
- 16. Bento PC, Pereira G, Ugrinowitsch C, Rodacki AL. Peak torque and rate of torque development in elderly with and without fall history. Clin Biomech (Bristol, Avon) 2010;25:450–454. [DOI] [PubMed] [Google Scholar]
- 17. Pohl PS, Duncan P, Perera S, Long J, Liu W, Zhou J, et al. Rate of isometric knee extension strength development and walking speed after stroke. J Rehabil Res Dev 2002;39:651–657. [PubMed] [Google Scholar]
- 18. Moreau NG, Falvo MJ, Damiano DL. Rapid force generation is impaired in cerebral palsy and is related to decreased muscle size and functional mobility. Gait Posture 2012;35:154–158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. DiPiro ND, Holthaus KD, Morgan PJ, Embry AE, Perry LA, Bowden MG, et al. Lower extremity strength is correlated with walking function after incomplete SCI. Top Spinal Cord Inj Rehabil 2015;21:133–139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Hannah R, Minshull C, Buckthorpe MW, Folland JP. Explosive neuromuscular performance of males versus females. Exp Physiol 2012;97:618–629. [DOI] [PubMed] [Google Scholar]
- 21. Folland JP, Buckthorpe MW, Hannah R. Human capacity for explosive force production: neural and contractile determinants. Scand J Med Sci Sports 2014;24:894–906. [DOI] [PubMed] [Google Scholar]
- 22. Ferrucci L. The Baltimore Longitudinal Study of Aging (BLSA): a 50‐year‐long journey and plans for the future. J Gerontol A Biol Sci Med Sci 2008;63:1416–1419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Shenoy S, Mishra P, Sandhu J. Peak torque and IEMG activity of quadriceps femoris muscle at three different knee angles in a collegiate population. J Exerc Sci Fitness 2011;9:40–45. [Google Scholar]
- 24. de Ruiter CJ, Kooistra RD, Paalman MI, de Haan A. Initial phase of maximal voluntary and electrically stimulated knee extension torque development at different knee angles. J Appl Physiol (1985) 2004;97:1693–1701. [DOI] [PubMed] [Google Scholar]
- 25. Lynch NA, Metter EJ, Lindle RS, Fozard JL, Tobin JD, Roy TA, et al. Muscle quality. I. Age‐associated differences between arm and leg muscle groups. J Appl Physiol (1985). 1999;86:188–194. [DOI] [PubMed] [Google Scholar]
- 26. Lindle RS, Metter EJ, Lynch NA, Fleg JL, Fozard JL, Tobin J, et al. Age and gender comparisons of muscle strength in 654 women and men aged 20‐93 yr. J Appl Physiol (1985). 1997;83:1581–1587. [DOI] [PubMed] [Google Scholar]
- 27. Simonsick EM, Newman AB, Nevitt MC, Kritchevsky SB, Ferrucci L, Guralnik JM, et al. Measuring higher level physical function in well‐functioning older adults: expanding familiar approaches in the Health ABC study. J Gerontol A Biol Sci Med Sci 2001;56:M644–M649. [DOI] [PubMed] [Google Scholar]
- 28. Simonsick EM, Schrack JA, Glynn NW, Ferrucci L. Assessing fatigability in mobility‐intact older adults. J Am Geriatr Soc 2014;62:347–351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, et al. A short physical performance battery assessing lower extremity function: association with self‐reported disability and prediction of mortality and nursing home admission. J Gerontol 1994;49:M85–M94. [DOI] [PubMed] [Google Scholar]
- 30. Altubasi IM. Is quadriceps muscle strength a determinant of the physical function of the elderly? J Phys Ther Sci 2015;27:3035–3038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Kjolhede T, Vissing K, Langeskov‐Christensen D, Stenager E, Petersen T, Dalgas U. Relationship between muscle strength parameters and functional capacity in persons with mild to moderate degree multiple sclerosis. Mult Scler Relat Disord 2015;4:151–158. [DOI] [PubMed] [Google Scholar]
- 32. Sayers SP, Guralnik JM, Thombs LA, Fielding RA. Effect of leg muscle contraction velocity on functional performance in older men and women. J Am Geriatr Soc 2005;53:467–471. [DOI] [PubMed] [Google Scholar]
- 33. Visser M, Deeg DJ, Lips P, Harris TB, Bouter LM. Skeletal muscle mass and muscle strength in relation to lower‐extremity performance in older men and women. J Am Geriatr Soc 2000;48:381–386. [DOI] [PubMed] [Google Scholar]
- 34. Fragala MS, Clark MH, Walsh SJ, Kleppinger A, Judge JO, Kuchel GA, et al. Gender differences in anthropometric predictors of physical performance in older adults. Gend Med 2012;9:445–456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Hicks GE, Shardell M, Alley DE, Miller RR, Bandinelli S, Guralnik J, et al. Absolute strength and loss of strength as predictors of mobility decline in older adults: the InCHIANTI study. J Gerontol A Biol Sci Med Sci 2012;67:66–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Lauretani F, Russo CR, Bandinelli S, Bartali B, Cavazzini C, Di Iorio A, et al. Age‐associated changes in skeletal muscles and their effect on mobility: an operational diagnosis of sarcopenia. J Appl Physiol (1985) 2003;95:1851–1860. [DOI] [PubMed] [Google Scholar]
- 37. Moran AL, Nelson SA, Landisch RM, Warren GL, Lowe DA. Estradiol replacement reverses ovariectomy‐induced muscle contractile and myosin dysfunction in mature female mice. J Appl Physiol (1985). 2007;102:1387–1393. [DOI] [PubMed] [Google Scholar]
- 38. Kadi F, Karlsson C, Larsson B, Eriksson J, Larval M, Billig H, et al. The effects of physical activity and estrogen treatment on rat fast and slow skeletal muscles following ovariectomy. J Muscle Res Cell Motil 2002;23:335–339. [DOI] [PubMed] [Google Scholar]
- 39. Murtagh KN, Hubert HB. Gender differences in physical disability among an elderly cohort. Am J Public Health 2004;94:1406–1411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Lee DC, Shook RP, Drenowatz C, Blair SN. Physical activity and sarcopenic obesity: definition, assessment, prevalence and mechanism. Future Sci OA 2016;2:FSO127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Izquierdo M, Ibanez J, Gorostiaga E, Garrues M, Zuniga A, Anton A, et al. Maximal strength and power characteristics in isometric and dynamic actions of the upper and lower extremities in middle‐aged and older men. Acta Physiol Scand 1999;167:57–68. [DOI] [PubMed] [Google Scholar]
- 42. Thompson BJ, Ryan ED, Sobolewski EJ, Conchola EC, Cramer JT. Age related differences in maximal and rapid torque characteristics of the leg extensors and flexors in young, middle‐aged and old men. Exp Gerontol 2013;48:277–282. [DOI] [PubMed] [Google Scholar]
- 43. Christ CB, Boileau RA, Slaughter MH, Stillman RJ, Cameron J. The effect of test protocol instructions on the measurement of muscle function in adult women. J Orthop Sports Phys Ther 1993;18:502–510. [DOI] [PubMed] [Google Scholar]
- 44. McLellan CP, Lovell DI, Gass GC. The role of rate of force development on vertical jump performance. J Strength Cond Res 2011;25:379–385. [DOI] [PubMed] [Google Scholar]
- 45. West DJ, Owen NJ, Jones MR, Bracken RM, Cook CJ, Cunningham DJ, et al. Relationships between force‐time characteristics of the isometric midthigh pull and dynamic performance in professional rugby league players. J Strength Cond Res 2011;25:3070–3075. [DOI] [PubMed] [Google Scholar]
- 46. von Haehling S, Morley JE, Coats AJS, Anker SD. Ethical guidelines for publishing in the Journal of Cachexia, Sarcopenia and Muscle: update 2015. J Cachexia Sarcopenia Muscle 2015;6:315–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S4a. Relationship of rate of torque development or isometric knee extension peak torque with physical function tests in men over 60 years old
Table S4b. Relationships of rate of torque development or isometric knee extension peak torque with physical function tests in women over 60 years old
Table S5a. Relationships of rate of torque development or concentric, isokinetic peak torque at 30 deg/s with physical function tests in men over 60 years old
Fig. S2. Relationship between age and peak torque in isometric knee extension at 120 deg. In men, the solid line is a piecewise regression with a breakpoint estimated at 63.0 [51.2‐74.8] years old. In women, the solid line is a piecewise regression with a breakpoint estimated at 61.9 [55.0‐67.7] years old.
Fig. S3. The relationship between age and peak torque in concentric, isokinetic knee extension at 30 deg/s. In men, the solid line is a piecewise regression with a breakpoint estimated at 63.0 [51.9‐74.0] years old. In women, the solid line is a piecewise regression with a breakpoint estimated at 61.0 [54.0‐68.0] years old.