

Abstract
A study of anthropometric variation and craniofacial growth in individuals with the Prader-Labhart-Willi syndrome (PLWS) illustrates the utility of anthropometry in clinical evaluation and research. Anthropometric measurements, including head length and breadth, minimum frontal diameter, and head circumference, were obtained on 38 PLWS individuals (21 with chromosome 15 deletions) with an age range from 2 weeks to 39 years. No anthropometric differences were found between the two chromosome subgroups. A relative deceleration in the growth of certain craniofacial dimensions (head circumference and length) is suggested by the negative correlations between age and Z-scores for the measurements. Raw values for minimum frontal diameter and head breadth were near or below the 5th percentile curve, while almost all values for head length and circumference fell within normal limits. The data support suggestions that dolichocephaly be considered an early diagnostic feature of PLWS. Furthermore, the status of narrow bifrontal diameter as a major feature of PLWS is confirmed.
Keywords: Anthropometry, Medical genetics
Anthropometric methods have become increasingly important in the clinical evaluation of individuals with genetic disorders and other dysmorphic conditions. Recently, Meaney and Farrer (1986) have reviewed more than forty hereditary and congenital disorders for which published anthropometric data are available. The accomplishments and possibilities of growth analysis in clinical genetics have been reviewed by Opitz et al. (1985). These writers describe growth analysis as one of the two most powerful methodologic advances in clinical genetics which “is done least frequently and least well.” An ongoing study of anthropometric variation and craniofacial growth in the Prader-Labhart-Willi syndrome (PLWS) reported below illustrates the utility of anthropometry in medical genetic research and clinical evaluation.
Over 500 cases of PLWS have been reported since the syndrome was first described in 1956 (Prader et al., 1956). Zellweger (1979, 1981) has described two phases in the development of this disorder, the first varying in duration from a few months to as late as until two years of age. Diagnostic features in the first phase include nonprogressive hypotonia, feeding problems (and usually failure to thrive), and, in males, micropenis, hypoplastic scrotum, and cryptorchidism. In the second phase, signs include developing obesity, mostly with accompanying reports of hyperphagia, mental deficiency, behavioral problems, short stature, hypogonadism, muscular hypotonia, somewhat characterisitic facies, and slowing in the growth of the hands and/or feet, sometimes resulting in acromicria.
Recently, Zellweger (1981) has listed dolichocephaly with small bifrontal diameter and brachycephaly in other cases as symptoms of the first phase of PLWS. Hall and Smith (1972) were first to suggest that a narrow bifrontal diameter, particularly in younger patients, was a major feature of the syndrome. Interestingly, there seems to be considerable variability from one sample of PLWS patients to another in the frequency of narrow bifrontal diameter. Hall (personal communication) found a frequency of 40% in one clinical study of PLWS individuals (Washington State) and a frequency of 87% in another clinical group (San Francisco). Holm (1981) reported a frequency of less than one-third based on a questionnaire study. Zellweger and Schneider (1968) reported finding a dolichocephalic head shape in seven (including the two youngest) of the 14 patients they had followed.
Regarding head size, one finds a variety of results from clinical studies of PLWS individuals. Smith (1976) listed microcephaly as an occasional abnormality, whereas Holm (1981) did not mention microcephaly as a problem, based on questionnaire data, but rather noted that 8% of individuals in her sample had large heads. Dunn et al. (1981) found 14 of 17 classical PLWS individuals to be normocephalic (within ± 2 SD for chronological age). Two of the other three individuals had abnormally large heads (greater than 2 SD for age), and the other had microcephaly. The present paper reports data on head size as well as head shape in a clinical population of PLWS individuals.
MATERIALS AND METHODS
Thirty-eight individuals diagnosed as having PLWS were assessed anthropometrically in a cytogenetic and clinical study by a team of investigators at the Indiana University School of Medicine. Diagnosis of PLWS was made on the basis of the following specific criteria: infantile hypotonia, hypogonadism, delayed developmental milestones and/or mental retardation, early childhood obesity, small hands and feet, and short stature. This group of PLWS individuals consisted of 22 males and 16 females ranging in age at time of first examination from 2 weeks to 39 years of age. For 16 of the 38 individuals, it has been possible to obtain measurements on more than one occasion.
All measurements were made by one of the authors (F.J.M.) according to standard techniques (Weiner and Lourie, 1969; Cameron, 1984). The anthropometric evaluation of each individual consisted of 26 measurements in total, including the following four craniofacial dimensions: head circumference, head length, head breadth, and minimum frontal diameter. In addition to these data, medical histories, hand X-rays, hand- and footprints, and blood for chromosome tests were obtained. Analyses of some of these data have been reported previously (Butler and Meaney, 1985; Butler et al., 1986; Reed and Butler, 1984). Of the 38 PLWS individuals, 21 (55%) were found to have a deletion of the proximal long arm of chromosome 15 (Butler and Meaney, 1987).
For certain analyses of the anthropometric data, measurements were converted to Z scores to control for age and sex effects. Appropriate published standards (Snyder et al., 1977; Farkas, 1981) were used for the four craniofacial variables. Z-score variables were plotted against age to determine whether there was any residual effect of age. Correlations were computed for each of the comparisons between a Z-score variable and age. Finally, to illustrate the anthropometric findings in PLWS, the raw measurements were plotted against standards obtained from published sources (Snyder et al., 1977; Farkas, 1981).
RESULTS
A summary of PLWS craniofacial measurements is shown in Table 1. With χ2 statistical analyses, no differences are found between the chromosome subgroups of deletion v. nondeletion individuals, or were differences between these subgroups found for craniofacial Z scores when these variables were included in a discriminant analysis using the full set of anthropometric Z-score variables.
TABLE 1.
Summary of Prader-Labhart-Willi syndrome craniofacial measurements
| Measurement | Proband chromosome subgroup (%)
|
|
|---|---|---|
| Deletion | Nondeletion | |
| Head circumference | ||
| < −2 SD | 6/21 (29) | 2/17 (12) |
| < −1 SD | 12/21 (57) | 8/17 (47) |
| Head length | ||
| < −2 SD | 3/21 (14) | 2/17 (12) |
| < −1 SD | 10/21 (48) | 7/17 (41) |
| Head breadth | ||
| < −2 SD | 9/21 (43) | 9/17 (53) |
| < −1 SD | 17/21 (81) | 16/17 (94) |
| Frontal diameter | ||
| < −2 SD | 15/17 (88) | 12/14 (86) |
| < −1 SD | 17/17 (100) | 14/14 (100) |
| Dolicocephaly | ||
| C.I.1 < 75% | 11/21 (52) | 12/17 (71) |
| C.I. < 77% | 14/21 (67) | 15/17 (88) |
C.I. is cephalic index, which is equal to head breadth/head length × 100.
The correlation values for each craniofacial Z-score variable with age and for cephalic index with age are shown in Table 2. Correlations between these variables and age are negative for head circumference and head length. No relationship is found between age and the Z-scores for head breadth and minimum frontal diameter. A positive correlation is shown between the cephalic index and age.
TABLE 2.
Correlations between Z scores for craniofacial variables and age in Prader-Labhart-Willi syndrome individuals (N = 38)
| Variable | r |
|---|---|
| Head circumference | −0.44* |
| Head length | −0.42* |
| Head breadth | 0.15 |
| Minimum frontal diameter (N = 31) | −0.32 |
| Cephalic index | 0.58** |
p < .02.
p < .001.
Figures 1 and 2 show the raw values for head circumference and head length, respectively, against standards for these measurements (Snyder et al., 1977). Most of the values for head circumference fall within normal limits. There is a tendency for more of the female values to fall on or below the 5th percentile curve. Length of the head does not seem to be affected in this syndrome. Almost all values fall within normal limits.
Fig. 1.
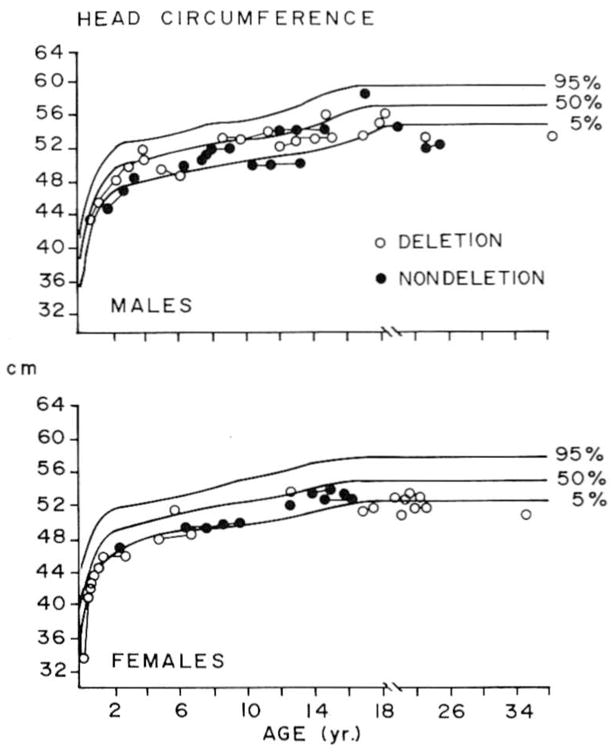
Head circumference measurements in deletion and nondeletion PLWS males and females plotted on standard curves. Measurements for an individual are represented with a line.
Fig. 2.
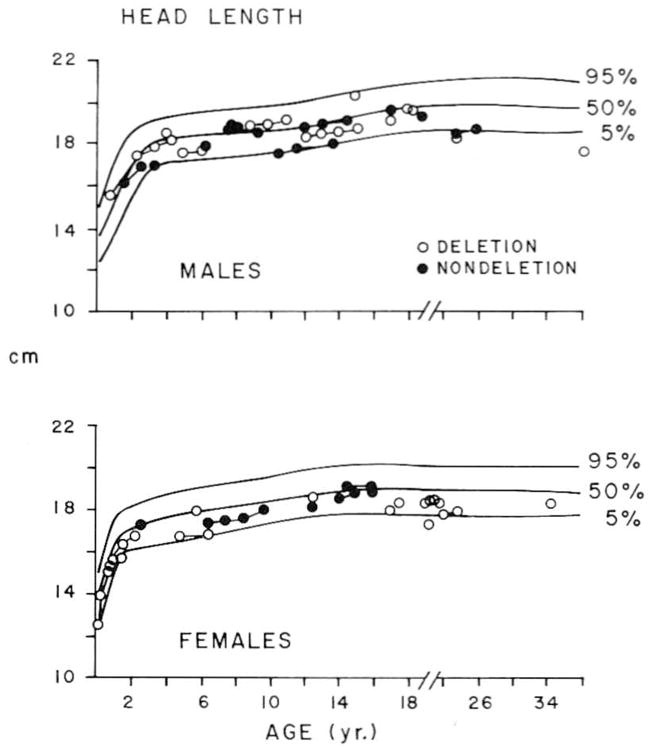
Head length measurements in deletion and nondeletion PLWS males and females plotted on standard curves. Measurements for an individual are represented with a line.
Figures 3 and 4 display the raw values for head breadth and minimum frontal diameter, respectively, plotted against standards for these craniofacial dimensions (Snyder et al., 1977; Farkas, 1981). Head breadth measurements among PLWS individuals are constantly below the 50th percentile, with the majority of values approaching, if not at or below, the 5th percentile curve. The minimum frontal diameter seems to be more severely affected than head breadth in this condition. Most of the values fall well below the 5th percentile for both males and females (perhaps all values for females).
Fig. 3.

Head breadth measurements in deletion and nondeletion PLWS males and females plotted on standard curves. Measurements for an individual are represented with a line.
Fig. 4.
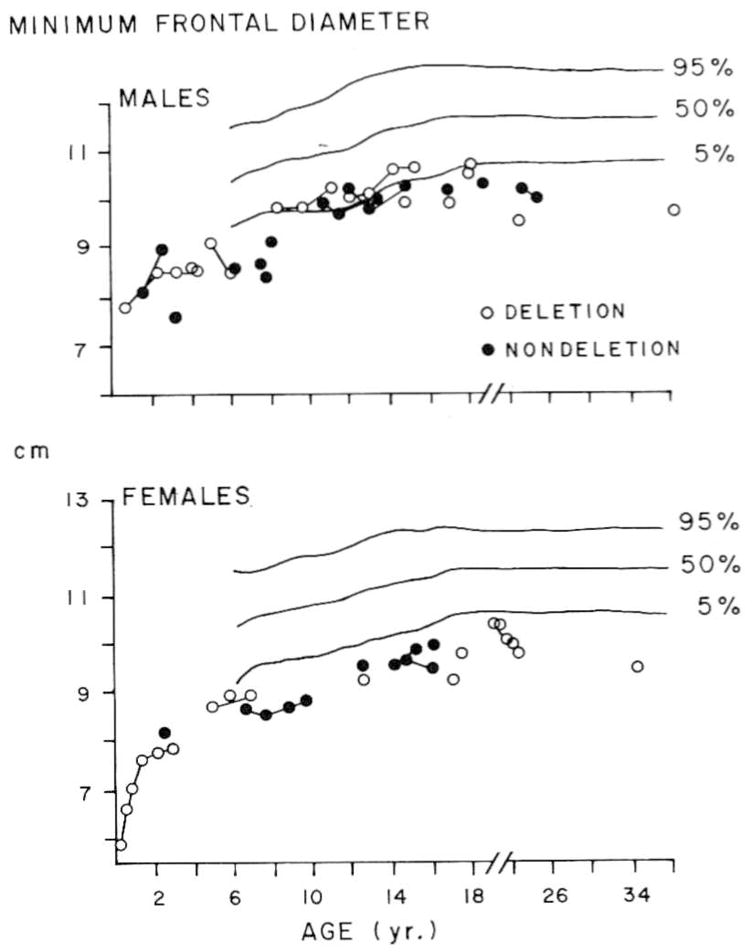
Minimum frontal diameter measurements in deletion and nondeletion PLWS males and females plotted on standard curves. Measurements for an individual are represented with a line.
The cephalic indices are plotted against age for both males and females in Figure 5. The dotted lines represent the generally accepted cut-offs for brachycephaly (80%) and dolichocephaly (75%) from Harrison et al. (1977). The low positive correlation between cephalic index and age (Table 2) demonstrates a tendency for the index to increase with age. However, dolichocephaly may persist in some PLWS individuals well into the late adolescent age period, as can be seen in Figure 5. Almost two-thirds of the PLWS individuals are dolichocephalic at the time of latest measurements by the more conservative cut-off of 75% for the cephalic index. Only one subject, the oldest male, is brachycephalic.
Fig. 5.

Cephalic indices in deletion and nondeletion PLWS males and females plotted against chronological age. Measurements for an individual are represented with a line.
DISCUSSION
Although anthropometric measurements have been converted to Z scores to standardize for age and sex, several Z-score variables for linear measurements and two craniofacial dimensions, head circumference and head length, have been found to be inversely correlated with age (Meaney and Butler, 1987). It has been suggested elsewhere (Meaney and Butler, 1987) that these relationships may represent a relative slowing down in linear growth with increasing age in PLWS individuals relative to normal standards. This relative deceleration of growth may also be true for certain craniofacial dimensions as reported herein. These outcomes might in part be due to delayed pubertal growth in PLWS individuals. Further longitudinal research is needed to clarify the validity of this relative growth deceleration hypothesis.
The results for head size in this sample of PLWS individuals support for the most part the work of previous investigators. The values for head circumference fall primarily within normal limits. Unlike the case in some previous reports (Holm, 1981; Dunn et al., 1981), no individuals were found to have abnormally large head size. The plotted data for head circumference suggest that microcephaly is more than just an occasional abnormality in adults with PLWS. Five of the eight PLWS individuals over 18 years of age had head circumference values well below the 5th percentile.
The percentage of dolichocephaly in this study using the 75% cephalic index value as a cut-off (Harrison et al., 1977) compares favorably with previously reported clinical data (Zellweger and Schneider, 1968). The dolicocephalic head shape seems to be the predominant pattern in the infant and preschool age groups in this condition. In contrast to the report of Zellweger (1981), no cases of brachycephaly were found in any of the first-phase subjects in the present study, but the number of such individuals is small. Dolichocephaly persists in some PLWS individuals into the adolescent and adult stages. The data support the suggestion of Zellweger (1981) that dolichocephaly be considered an early diagnostic feature of PLWS.
Previous clinical reports have suggested that narrow bifrontal diameter can be considered a major feature of PLWS (Hall and Smith, 1972). Differences in the reported frequency of narrow bifrontal diameter in other clinical populations may reflect variability in observational techniques or the measurement used to assess frontal diameter. In the present study, using minimum frontal diameter, the frequency of narrow bifrontal diameter is extremely high (more than 85%). These data support the conclusion that narrow bifrontal diameter should be considered a major feature of PLWS over the entire age range. Values above the 5th percentile curve were found in only a few individuals. Accurate anthropometric-evaluation of bifrontal diameter should be undertaken in other clinical populations of PLWS individuals to verify the findings reported herein, and, most certainly, accinate measurement of bifrontal diameter should become part of the diagnostic evaluation of any child suspected of having this disorder.
No differences in anthropometric dimensions, including craniofacial measurements, have been substantiated between the deletion and nondeletion subgroups of PLWS individuals (Meaney and Butler, 1987). Larger, comprehensive surveys of PLWS individuals and further longitudinal studies will be required before any final conclusion can be reached concerning anthropometric differences between the two chromosome subgroups. Research in progress using a DNA probe for bands q11–q13 on chromosome 15 to confirm the deletion may present an opportunity to investigate size of the deletion in relation to clinical findings. Collaborative efforts between the cytogeneticist, molecular geneticist, and clinical anthropometrist may offer a unique approach to the heterogeneity in this disorder.
Acknowledgments
The authors thank Drs. Rebecca Wappner, Bryan Hall, Patricia Bader, and Andree Walczak for allowing us to evaluate their patients. We also thank Brenda Wilkinson for her expert assistance in preparation of the final draft. The authors acknowledge use of the facilities of Computing Services, Indiana University—Purdue University, Indianapolis, and the assistance of staff in the Department of Medical illustrations, Indiana University Medical Center, Indianapolis, with the figures. An earlier version of this paper was presented by the senior author at the symposium “Quantitative Methods in the Diagnosis and Treatment of Craniofacial Anomalies” on April 12, 1986, at the Fifty-Fifth Annual Meeting of the American Association of Physical Anthropologists in Albuquerque, New Mexico. This research was supported in part by Oral-Facial Genetics Training Grant PHS-T32 DE 07043 (F.J.M.) and by Public Health Service Grant PHS-5T32 GM 07468 (M.G.B.)
LITERATURE CITED
- Butler MG, Meaney FJ. Metacarpophalangeal pattern profile analysis in Prader-Willi syndrome: A follow-up report on 38 cases. Clin Genet. 1985;28:27–30. doi: 10.1111/j.1399-0004.1985.tb01213.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Meaney FJ. An anthropometric survey of 38 individuals with Prader-Labhart-Willi syndrome. Am J Med Genet. 1987;26:445–455. doi: 10.1002/ajmg.1320260224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Meaney FJ, Palmer CG. Clinical and cytogenetic survey of 39 individuals with Prader-Labhart-Willi syndrome. Am J Med Genet. 1986;23:793–809. doi: 10.1002/ajmg.1320230307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cameron N. The Measurement of Human Growth. London: Croom Helm; 1984. [Google Scholar]
- Dunn HG, Tze WJ, Alisharon RM, Schulzer M. Clinical experience with 23 cases of Prader-Willi syndrome. In: Holm VA, Sulzbacher S, Pipes PL, editors. The Prader-Willi Syndrome. Baltimore: University Park Press; 1981. pp. 69–88. [Google Scholar]
- Farkas CG. Anthropometry of the Head and Face in Medicine. New York: Elsevier North Holland; 1981. [Google Scholar]
- Hall BD, Smith DW. Prader-Willi syndrome. J Pediatr. 1972;81:286–293. doi: 10.1016/s0022-3476(72)80297-x. [DOI] [PubMed] [Google Scholar]
- Harrison GA, Weiner JS, Tanner JM, Barnicot NA. Human Biology: An Introduction to Human Evolution, Variation, Growth and Ecology. Oxford: Oxford University Press; 1977. p. 196. [Google Scholar]
- Holm VA. The diagnosis of Prader-Willi syndrome. In: Holm VA, Sulzbacher S, Pipes PL, editors. The Prader-Willi Syndrome. Baltimore: University Park Press; 1981. pp. 27–44. [Google Scholar]
- Meaney FJ, Butler MG. The developing role of anthropologists in medical genetics: anthropometric assessment of the Prader-Labhart-Willi syndrome as an illustration. Med Anthropol. 1987 doi: 10.1080/01459740.1989.9965971. in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meaney FJ, Farrer LA. Clinical anthropometry and medical genetics: A compilation of body measurements in genetic and congenital disorders. Am J Med Genet. 1986;25:343–359. doi: 10.1002/ajmg.1320250221. [DOI] [PubMed] [Google Scholar]
- Opitz JM, Mendez HMM, Hall JG. Growth analysis in clinical genetics. In: Papadatos CJ, Bartsocas CS, editors. Endocrine Genetics and Genetics of Growth. New York: Alan R. Liss, Inc; 1985. pp. 33–64. [Google Scholar]
- Prader A, Labhart A, Willi H. Ein syndrom von adipositas, kleinwuchs, Kryptorchismus und Oligophrenie nach myatonieartigen Zustand im Neugeborenenalter. Schweiz Med Wochenschr. 1956;86:1260–1261. [Google Scholar]
- Reed T, Butler MG. Dermatoglyphic features in Prader-Willi syndrome with respect to chromosomal findings. Clin Genet. 1984;25:341–346. doi: 10.1111/j.1399-0004.1984.tb02001.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith DW. Recognizable Patterns of Human Malformation: Genetic, Embryologic and Clinical Aspects. 2. Philadelphia: W.B. Saunders Company; 1976. [PubMed] [Google Scholar]
- Snyder RG, Schneiden LW, Owings CL, Reynolds HM, Gollomb DH, Schork MA. Anthropometry of Infants, Children, and Youths to Age 18 for Product Safety Design SP-450. Warrendale, PA: Society of Automobile Engineers, Inc; 1977. [Google Scholar]
- Weiner JS, Lourie JA. International Biological Programme Handbook No. 9. Oxford: Blackwell Scientific Publications; 1969. Human Biology: A Guide to Field Methods. [Google Scholar]
- Zellweger H. Prader-Willi syndrome. In: Bergsma D, editor. Birth Defects Compendium. 2. New York: Alan R. Liss, Inc; 1979. pp. 883–885. [Google Scholar]
- Zellweger H. Diagnosis and therapy in the first phase of Prader-Willi syndrome. In: Holm VA, Sulzbacher S, Pipes PL, editors. The Prader-Willi Syndrome. Baltimore: University Park Press; 1981. pp. 55–68. [Google Scholar]
- Zellweger H, Schneider HJ. Syndrome of hypotonia-hypomentia-hypogonadism-obesity (HHHO) or Prader-Willi syndrome. Am J Dis Child. 1968;115:588–598. doi: 10.1001/archpedi.1968.02100010590009. [DOI] [PubMed] [Google Scholar]