

Abstract
Background:
Microtia reconstruction is a challenging procedure, especially in developing nations. The most complex part is learning how to fabricate a framework from costal cartilage. We herein propose a training regimen for ear reconstruction with the use of a plastic eraser.
Materials and Methods:
The texture of a plastic eraser made from polyvinyl chloride is similar to that of human costal cartilage. The first step of the training is carving out the sixth through eighth rib cartilages from a block of plastic eraser. The second step is a fabrication of the framework from plastic rib cartilages, referring to a template from the intact auricle.
Results:
As plastic erasers are inexpensive and universally available, inexperienced surgeons can repeatedly perform this framework training. Following several of these training sessions in developing nations, the co-authors and local surgeons successfully performed their microtia reconstructions in a reasonable operative time.
Conclusions:
This realistic carving model allows surgeons to gain experience before performing an actual ear reconstruction, even in resource-constrained circumstances.
KEY WORDS: Cartilage framework, costal cartilage, microtia reconstruction, plastic eraser, training tool
INTRODUCTION
There have been many plastic surgery missions to treat paediatric patients in developing nations.[1,2] For most missions, the highest priority conditions include orofacial clefts, tumours, hand deformities and post-burn contractures.[3] Patients with a congenital or traumatic ear deformity have been put at the bottom of the surgery list. In particular, microtia reconstructions during charitable surgical missions have been avoided due to multistage treatments, a time-consuming operation, the difficulty of postoperative care and severe donor-site morbidity including pneumothorax.
One of the co-authors (D. M.) has volunteered his services as a paediatric plastic surgeon since 2003 in Asian countries,[2] where orofacial clefts, large nevi, poly/syndactyly, hypospadias and post-burn contractures have been treated. Recently, however, ear reconstructions have also been performed due to an increase in requests from both local surgeons and patients.
Ear reconstruction for microtia is difficult and one of the most challenging procedures in paediatric plastic surgery.[4] The complex structure of the auricle, along with the inherent difficulty of placing a three-dimensional autologous rib cartilage framework within a tight skin pocket, leads to a broad spectrum of results amongst surgeons.[5] Over the years, while surgical techniques have become more refined, the core concepts remain the same.[5] As artistic sense, surgical aptitude and personal effort are all required for a successful outcome,[3] inexperienced surgeons need training to improve their surgical skills. To that end, a workshop-based instructional programme was successfully conducted in Canada,[6] where a silicone costal cartilage model was employed for the ear framework. Thus far, the use of many different materials for the framework training models has been described, but each has disadvantages including limited availability and/or lack of realism.[7]
We herein present our results using a plastic eraser for ear reconstruction training. This is a cost-effective and realistic material, and the training programme is easily repeated, even in resource-constrained circumstances. In addition, we present our clinical experiences following simulations based on the described training.
MATERIALS AND METHODS
We used an A6-sized plastic eraser made from polyvinyl chloride [Figure 1]. The thickness was 10 mm. This eraser is inexpensive (approximately 450 JPY = 4 USD) and available in almost any stationery store in Japan. As the texture of this plastic eraser was found to be very close to human cartilage, we employed it as the material for the ear framework training model.
Figure 1.
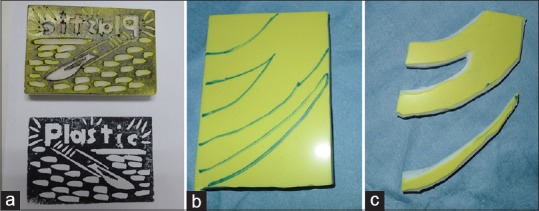
The first step of framework training using a plastic eraser. Schoolchildren engrave a postcard-sized plastic eraser in art class (a). The conjoint sixth and seventh ribs and a long piece of the eighth rib cartilage are drawn on one of the plastic erasers that was cut out into four pieces (b). The rib cartilage models are carved out and split into two pieces each with a thickness of 5 mm (c)
The first step is to carve out costal cartilage models as if harvested from the right chest. The A6-sized (150 mm × 100 mm) eraser is cut into four pieces (75 mm × 50 mm). The sixth, seventh and eighth costal cartilage models are carved out using a set of chisels and a craft knife; then, they are split into two pieces each with a thickness of 5 mm.
The second step includes fabrication of the framework. An X-ray film template was obtained from the intact auricle of the patient [Figure 2]. Attempting a Brent-type framework,[8] the base frame and antihelix were created from the sixth and seventh conjoint rib cartilage models, and the helical rim was created from the eighth rib. If necessary, the cymba of the concha was made with a remnant piece. Attention should be paid to affixing the helical rim and antihelix to the base block with 5-0 nylon sutures because the plastic eraser is slightly less fragile than real costal cartilages. For carving, however, the texture is very close to that of cartilage. Details are gouged into the framework after all parts are affixed. The co-authors continued this training until the second step (framework fabrication) could be finished within 45 min.
Figure 2.
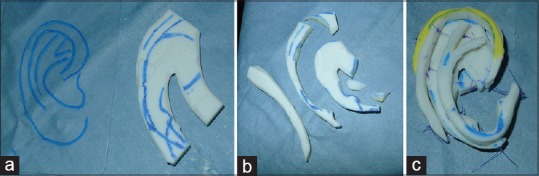
The second step of framework training using a plastic eraser. The base frame and antihelix were outlined on the sixth and seventh conjoint cartilage model by reference to a template obtained from a child's normal ear (a). The base frame and antihelix were carved out using a no. 15 scalpel, and the helical rim was created by longitudinally splitting the eighth rib model (b). All parts are affixed to the base block using 5-0 nylon sutures (c)
RESULTS
After a simulation using this eraser material and the film template obtained from the opposite normal auricle of a 9-year-old child with unilateral microtia, one co-author (DM) performed his first ear reconstruction outside of Japan in cooperation with local surgeons. While the co-author was performing lobular transposition and undermining the skin pocket, the assistant harvested a block of the sixth and seventh cartilages [Figure 3]. Then, the co-author (DM) carved the base frame and antihelix from the harvested sixth and seventh conjoint cartilages, and the assistant harvested the eighth cartilage. The eighth rib cartilage was thinned longitudinally to serve as the helix. All pieces were connected using No. 38 stainless wires and 5-0 polydioxanone sutures to form a framework while the assistant surgeon closed the donor-site incision. When details were carved into the framework using carving gouges, overcontouring was attempted as the postoperative form is not as conspicuous as the underlying framework. After inserting the framework into the skin pocket, a suction drain was placed, and the contour was packed with paraffin gauze dressing. Total surgical time from initial incision into the lobule until application of a loose, overlying dressing of fluffed cotton was 3 h and 30 min.
Figure 3.

Photographic examples of the framework (left image in each pair) and contour after the insertion (right image in each pair). The actual surgery was performed in developing nations after training simulations using plastic eraser models. Patients shown are a 9-year-old male (a and b), a 20-year-old female (c and d) and an 18-year-old male (e and f)
To date, we have performed five microtia reconstructions according to the above process in developing nations. Three patients had a Grade II microtia and two had Grade III. The mean surgical time was 4 h and 10 min. One patient suffered from a small exposure of the cartilage frame, which was treated conservatively with gentamicin ointment. The postoperative course of the other patients was uneventful.
DISCUSSION
There has been a major emphasis on learning to carve a three-dimensional ear framework from a costal cartilage model.[9] Although training videos are currently available on the internet,[9] repeated practice using a model is essential to develop artistry and surgical skills. Historically, a bar of soap or vegetables, such as potato and carrot, were used as training materials.[7,9,10] However, they were not as elastic as rib cartilage and were not as realistic. Although Brent [8] recommended the use of human cadaver rib cartilage for the framework training, the use of cadaver cartilage does not simulate live donor cartilage as it is stiff and brittle; moreover, it is not freely available.[6,9] Recently, the use of animal cartilages including bovine scapula and porcine rib has been proposed for framework training.[11,12] Those materials are very similar to human rib cartilage and are relatively available on the market, but they present the potential risk of disease transmission.[9]
To avoid such issues, the training models of costal cartilage made from dental impression material have been recommended.[13,14] This model is made from silicone and is anatomically accurate. However, it is not possible to carve out the Silhouette of the silicone model using gouges because of its different rigidity compared to the real cartilage.[14] Moreover, it costs 100 USD per silicone framework.[13]
In contrast, the A6-sized plastic eraser that we recommend is 450 JPY (4 USD). Since the eraser is cut into eight pieces and expired nylon sutures are used, it costs only 50 cents for each framework training session. For microtia reconstruction, we believe that repeated training is a more important factor than artistic sense. Using this material, one surgeon can repeat the framework training eight times.
Compared to any other training materials employed previously, ear framework training using a plastic eraser was so realistic that trainees felt as if they were carving real cartilage. It may be a disadvantage that the plastic eraser is slightly less elastic than the rib cartilage of children. Trainees may feel the fragility of the plastic eraser when they assemble the pieces together. However, by practicing with such fragile material, trainees get accustomed to careful tissue handling when it comes to use of the real cartilage.
Another disadvantage may be that the A6-sized plastic eraser is not always universally available. However, large-sized eraser can be obtained through online shopping sites. Even in resource-constrained circumstances, ordinary-sized plastic erasers are available at stationery stores. If 6 of them were glued together into a sheet, they could be used for the same type of training.
CONCLUSIONS
We have found an increased need for treating children with ear deformities in developing countries undergoing economic development. As plastic erasers are cost-effective and universally available, trainees can repeat the carving exercise as many times as they want, including sessions at home. Performing simulations before an actual ear reconstruction should result in reduced operative time. Of course, not only in developing nations but also in any nation, this realistic and repeatable carving model allows surgeons to test their aptitude and gain experience. Currently, a hands-on training workshop using the described model is under consideration in Turkey and Myanmar as well as Japan.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient's parent consent forms. In the form, the patient 's parents have given their consent for their child images and other clinical information to be reported in the journal. The patient's parents understand that their child name and initial will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Nicolai JP, Grieb N, Gruhl L, Schwabe K, Preisser P. Interplast: Five years of the Cochin project. Eur J Plast Surg. 1998;21:77–81. [Google Scholar]
- 2.Morioka D, Yoshimoto S, Udagawa A, Ohkubo F, Yoshikawa A. Primary repair in adult patients with untreated cleft lip-cleft palate. Plast Reconstr Surg. 2007;120:1981–8. doi: 10.1097/01.prs.0000287322.79619.de. [DOI] [PubMed] [Google Scholar]
- 3.Schneider WJ, Politis GD, Gosain AK, Migliori MR, Cullington JR, Peterson EL, et al. Volunteers in plastic surgery guidelines for providing surgical care for children in the less developed world. Plast Reconstr Surg. 2011;127:2477–86. doi: 10.1097/PRS.0b013e3182131d2a. [DOI] [PubMed] [Google Scholar]
- 4.Sabbagh W. Early experience in microtia reconstruction: The first 100 cases. J Plast Reconstr Aesthet Surg. 2011;64:452–8. doi: 10.1016/j.bjps.2010.07.027. [DOI] [PubMed] [Google Scholar]
- 5.Cabin JA, Bassiri-Tehrani M, Sclafani AP, Romo T., III Microtia reconstruction: autologous rib and alloplast techniques. Facial Plast Surg Clin N Am. 2014;22:623–8. doi: 10.1016/j.fsc.2014.07.004. [DOI] [PubMed] [Google Scholar]
- 6.Murabit A, Anzarut A, Kasrai L, Fisher D, Wilkes G. Teaching ear reconstruction using an alloplastic carving model. J Craniofac Surg. 2010;21:1719–21. doi: 10.1097/SCS.0b013e3181f3c755. [DOI] [PubMed] [Google Scholar]
- 7.Wilkes GH. Learning to perform ear reconstruction. Facial Plast Surg. 2009;25:158–63. doi: 10.1055/s-0029-1239452. [DOI] [PubMed] [Google Scholar]
- 8.Brent BD. Reconstruction of the auricle. In: Mathes S, editor. Plastic Surgery. 2nd ed. Vol 3. Philadelphia: Elsevier Saunders; 2006. pp. 633–98. [Google Scholar]
- 9.Wilkes GH, Wong J, Guilfoyle R. Microtia reconstruction. Plast Reconstr Surg. 2014;134:464e–79e. doi: 10.1097/PRS.0000000000000526. [DOI] [PubMed] [Google Scholar]
- 10.Vadodaria S, Mowatt D, Giblin V, Gault D. Mastering ear cartilage sculpture: The vegetarian option. Plast Reconstr Surg. 2005;116:2043–4. doi: 10.1097/01.prs.0000192399.15346.23. [DOI] [PubMed] [Google Scholar]
- 11.Shin HS, Hong SC. A porcine rib cartilage model for practicing ear-framework fabrication. J Craniofac Surg. 2013;24:1756–7. doi: 10.1097/SCS.0b013e3182902548. [DOI] [PubMed] [Google Scholar]
- 12.Agrawal K. Bovine cartilage: A Near perfect training tool for carving ear cartilage framework. Cleft Palate Craniofac J. 2015;52:758–60. doi: 10.1597/14-079R. [DOI] [PubMed] [Google Scholar]
- 13.Yamada A, Imai K, Fujimoto T, Morimoto K, Niitsuma K, Matsumoto H, et al. New training method of creating ear framework by using precise copy of costal cartilage. J Craniofac Surg. 2009;20:899–902. doi: 10.1097/scs.0b013e3181a2ef97. [DOI] [PubMed] [Google Scholar]
- 14.Thadani SM, Ladani PS. A new method for training of ear framework creation by silicon dental impression material. Indian J Plast Surg. 2012;45:134–7. doi: 10.4103/0970-0358.96614. [DOI] [PMC free article] [PubMed] [Google Scholar]