

Abstract
Congenital maxillomandibular fusion or syngnathia is a rare craniofacial disorder with only 26 cases reported in the literature. We present a case of a congenital complex zygomatico-mandibular syngnathia associated with a palatal cleft, posterior maxilla and turbinate agenesia, mild hemifacial microsomia, and a disordered dental eruption. The patient has the highest age (15 years) at diagnosis described in the literature. 3D planning of the surgery was performed to study the patient's anatomy and design the necessary osteotomies to separate the jaws. En bloc removal of the fused fragment with bilateral coronoidectomy and aggressive long-term physiotherapy for 3 months led to a stable increase in mouth opening from 0 to 21 mm inter-incisor distance. The patient reported an improvement in speech, was able to eat without restriction regarding food consistency, and could maintain a good oral hygiene.
Keywords: syngnathia, maxillomandibular fusion, rare craniofacial disorder, 3D planning, surgery
Congenital maxillomandibular fusion or syngnathia is a rare craniofacial disorder that was first reported by Burket in 1936. 1 Only 26 cases 2 have been reported in the literature. It can be unilateral or bilateral, and can affect soft and/or hard tissues from single mucosal bands (synechiae) to complete bony fusion (synostosis). 2 3 Syngnathia is used when there is fusion between the maxilla and the mandible. 4 It can interfere with facial growth and cause problems with feeding and respiration. 2 5 Fusion of the mucosal alveolar ridges is more common than maxillomandibular bony fusion. 3
We present the surgical management of a 15year-old patient (highest age at diagnosis reported with this condition) with unilateral syngnathia associated with cleft palate, hemifacial microsomia and agenesia of the turbinate, and posterior maxilla. Furthermore, a literature review is described.
Case Report
A 15-year-old male patient was referred to our institution by an NGO foundation from Senegal for surgical management of the inability to open the mouth since the age of 2 years. Oral intake has been limited since birth to strictly liquid. A discrete proptosis could be noted. Clinical examination confirmed the inability to open the mouth, and revealed an upper and lower jaw dental collapse with labioversion and dental agenesis (elements 15, 16, 17, and 18).
Blood sampling revealed a bleeding disorder (64.2% prothrombin time, INR 1.25, fibrinogen 3.6 g/L, 41.3% factor VII), which was corrected by vitamin K administration, and an iron-deficiency anemia (hemoglobin: 12.4 g/dL, iron: 5.1 µmol/L, 28 µg/dL, ferritin: 8.8 µg/L). The patient tested hepatitis B positive.
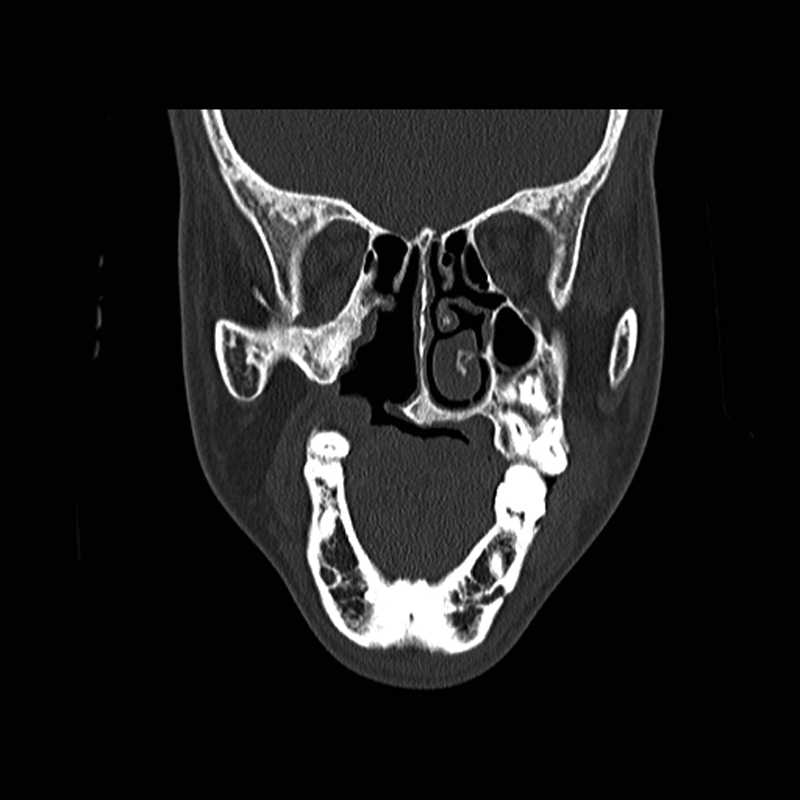
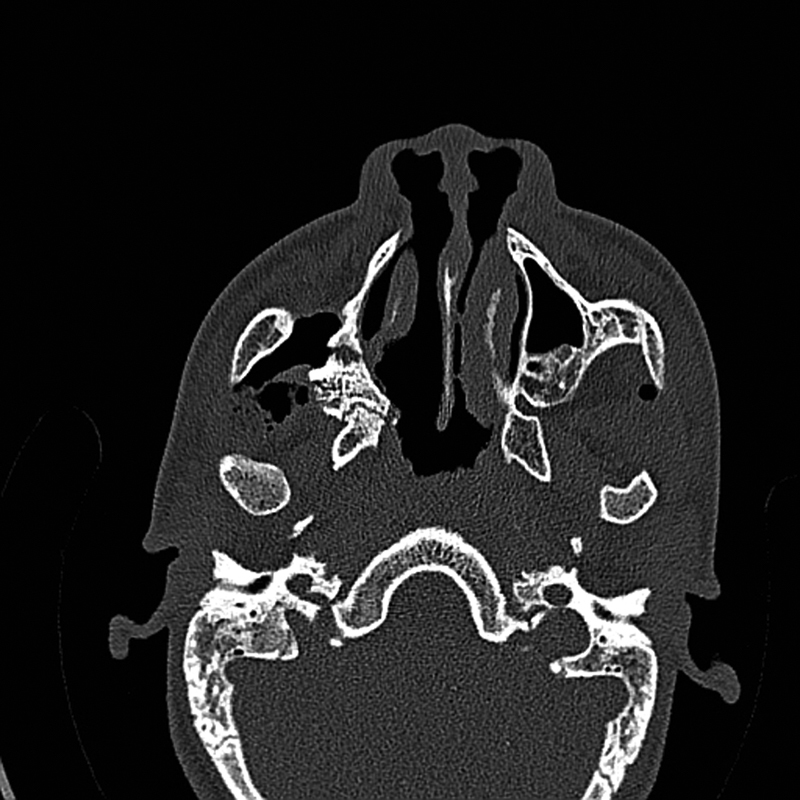
A CT scan of the head with 3D reconstruction ( Figs. 1 2 3 4 5 ) confirmed a maxillomandibular fusion associated with a cleft palate, agenesis of the right turbinate, and right hemifacial microsomia (Laster type 2b syngnathia). Both temporomandibular joints (TMJs) were normal and showed no bony ankylosis (fibrous ankylosis could not be excluded with the given data).
Fig. 1.

Preoperative CT scan. Axial view: right maxillomandibular fusion.
Fig. 2.

Preoperative CT scan. Axial view: agenesis of the right turbinate and cleft palate.
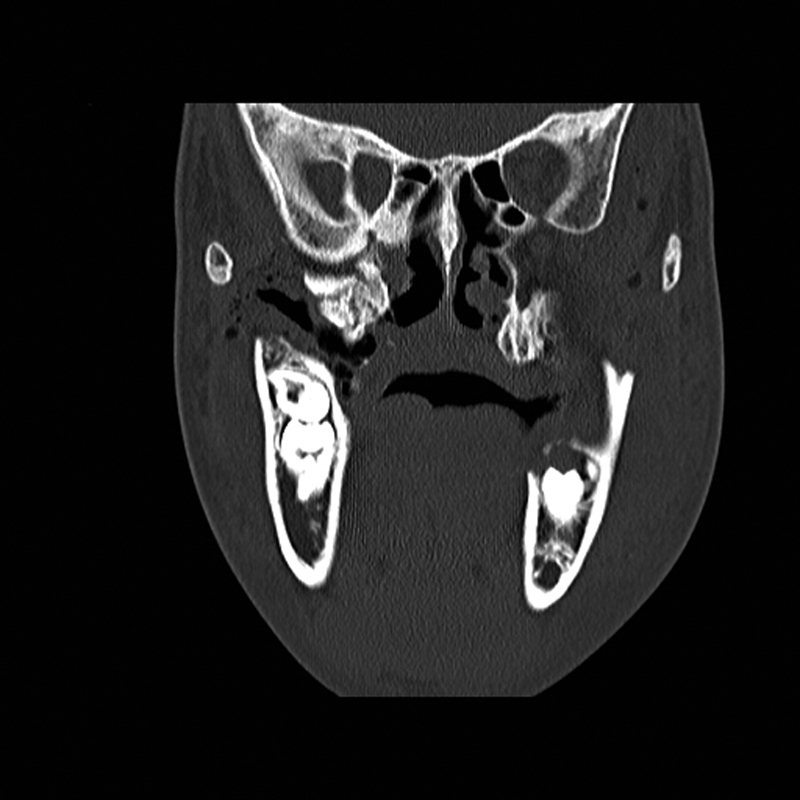
Fig. 3.

Preoperative CT scan. Coronal view: right maxillomandibular fusion.
Fig. 4.
Preoperative CT scan. Coronal view: agenesis of the right turbinate and cleft palate.
Fig. 5.

CT scan with 3D reconstruction: upper and lower jaw dental collapse with labioversion, dental agenesis, and right hemifacial microsomia.
A facial angio-CT scan was performed to study cervical vascular anatomy and to discard anatomical variants at the level of the internal maxillary artery. Heteroanamnesis revealed a family history of endogamy and second-degree consanguinity. 3D planning of the surgery was performed with SimPlant O&O (Materialise Dental/Dentsply Implants, Mölndal, Sweden) to study the patient's anatomy and design the necessary osteotomies to separate the jaws ( Figs. 6 and 7 ). Thanks to the 3D preparation, the surgical access could be decided on an intraoral approach with sufficient exposure to do the osteotomy and ostectomy seemed feasible. In case the access was insufficient, a hemicoronal approach with osteotomy of the zygomatic arch had to be considered.
Fig. 6.
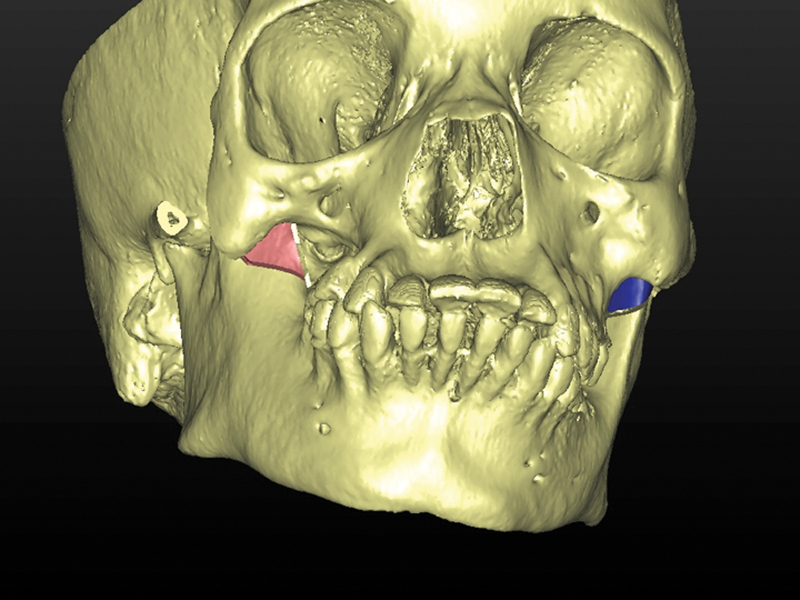
3D planning of the surgery.
Fig. 7.
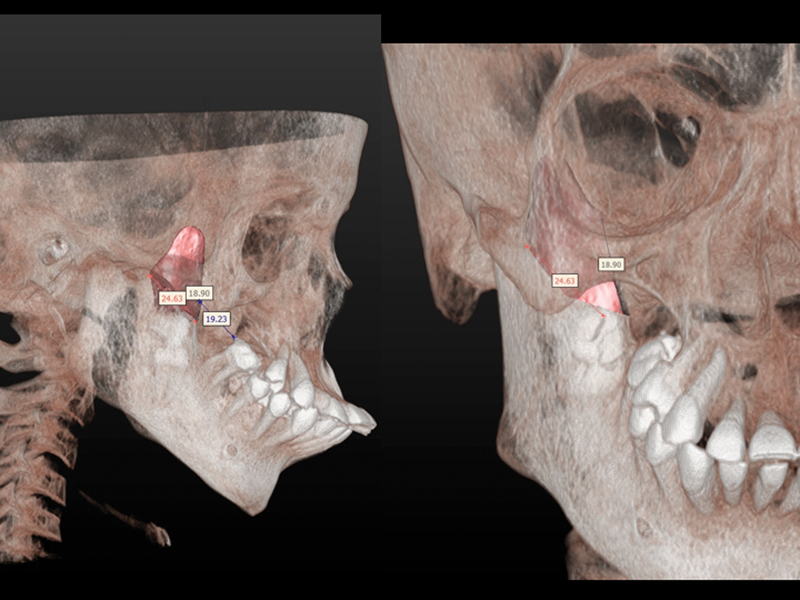
3D planning of the surgery.
Awake nasotracheal intubation was done under sedation with fiberoptic guidance through the right nostril, having the tracheostomy set on standby. A right intraoral Obwegeser approach with superior extension exposed the retromolar trigone, the coronoid process, the sigmoid notch, the malar body, the infraorbital nerve, and the ankylotic block extending from the mandibular ramus toward the pterygoid process.
The inferior part of the malar body was milled down for 2 mm to obtain a greater visibility of the ankylotic mass. After placement of an Obwegeser separator in the sigmoid notch, a liberating horizontal osteotomy in the coronoid process was performed with a reciprocating microsaw (Core; Stryker, Kalamazoo, MI) and a piezoelectric scalpel (Varios2, NSK-Nakanishi Inc., Tochigi, Japan). A mouth opening of 4 mm inter-incisor distance was achieved. The ankylotic fragment was removed by a sagittal osteotomy lateral to the pterygoid plates and stripping of the atrophic and fibrotic tendon of the temporal muscle of the fragment ( Fig. 8 ). After this maneuver, a mouth opening of 30 mm was achieved. A left coronoidectomy was performed using a piezoelectric scalpel (Varios2, NSK-Nakanishi Inc.) through an intraoral approach with detachment of the atrophic contralateral temporalis muscle tendon. A mouth opening of 54 mm inter-incisor distance was achieved. Furthermore, myotomy of fibrous bands of the fibrotic masseter muscle was performed (especially on the right side) to obtain a mouth opening of 64 mm ( Fig. 9 ). The buccal fat pad was interpositioned in the ostectomy site and the cleft palate was closed with a buccal rotation flap.
Fig. 8.

Intraoperative view and 3D planning of the surgery: liberating horizontal osteotomy in the coronoid process and sagittal osteotomy lateral to the pterygoid plates.
Fig. 9.
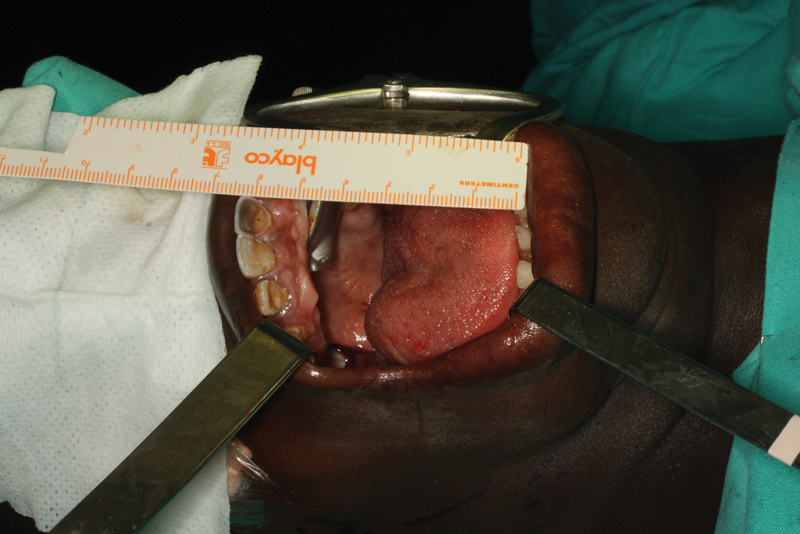
Maximum mouth opening (64 mm).
The mouth opening was gradually forced with the aid of an orthostatic mouth opener. After the operation, the anesthesiology team reassessed the airway by laryngoscopy. Tracheostomy was discarded given proper oral opening, making normal orotracheal intubation possible if necessary (Cormack I). The patient was transferred to the ICU and was discharged to the ward after a 24-hour observation. Postoperative CT scan with mouth opened was performed ( Figs. 10 11 12 ). The patient was seen by the speech therapist and the gastroenterology team to rule out a swallowing disorder and prevent aspiration issues. Furthermore, genetic counseling could not reveal a possible genetic cause. The physiotherapy team started the rehabilitation 24 hours after the surgery. Electrostimulation with a Compex device (Guildford, Surrey, United Kingdom) and active and passive opening and closing exercises helped reorganize the neuromuscular balance and regain the intraoral and perioral proprioceptivity. A TheraBite Jaw Motion Rehabilitation System (Atos Medical, Hörby, Sweden) was used to continue physiotherapy at home.
Fig. 10.
Postoperative CT scan. Axial view: right maxillomandibular fusion released.
Fig. 11.
Postoperative CT scan. Coronal view: right maxillomandibular fusion released.
Fig. 12.

3D reconstruction CT scan: postoperative CT scan with mouth opened.
After 7 days of intensive physiotherapy and rehabilitation, the patient was discharged and was seen daily initially for a week and afterward weekly in the outpatient clinic. An increase in tone of the initially atrophic masticatory muscles was noted during follow-up, allowing adequate mouth opening, lateral mandibular movements, and mastication. During follow-up, the dental team could benefit from the increased mouth opening and improved oral access to treat multiple dental caries and perform root canal treatments.
After 3 months of rehabilitation and two mobilizations of the TMJs under sedation to a mouth opening of 45 mm, the amplitude of the mouth opening stabilized at 21 mm inter-incisor distance. The patient returned to Senegal and reported an improvement in speech, was able to eat without restriction regarding food consistency, and could maintain a good oral hygiene. Patient follow-up was done by NGO Dentistas sin Fronteras in Senegal without relapse after 19 months.
Discussion
Syngnathia is an extremely rare condition and usually refers to bony fusion of the jaws. Moreover, it can also imply soft-tissue fusion between the gums, referred to as synechiae. 5 Most of the 26 cases reported in the literature were incomplete 2 6 and only 7 patients were reported to have a fusion of the ascending ramus of the mandible and the maxilla and zygomatic complex, 7 as we describe here. Early treatment is very important to avoid respiratory and feeding difficulties and prevent future problems such as ankylosis of the TMJ. We report, however, the absence of bony TMJ ankylosis in this case of a late diagnosis of congenital syngnathia in an adolescent.
Different etiological factors have been suggested, such as abnormality of the stapedial artery in the fetus, early loss of neural crestal cells, persistence of the buccopharyngeal membrane, amniotic constriction bands in the region of the developing first branchial arch, teratogenic agents, or trauma. 2 5 8 Consanguinity, as in this patient, has also been described by other authors. 5 Two cases of acquired syngnathia have been reported as a result of a fibrotic tubed pedicle and from myositis ossificans. 9 Syngnathia can be associated with Van der Woude's syndrome, 2 10 popliteal pterygium syndrome, and aglossia-adactylia syndrome. 6 It has been described in coexistence with maxillary duplication and a Tessier number 3 nasal cleft 11 and with duplication of the craniofacial midline. 12 According to Subramanian et al, 4 anomalies associated with syngnathia can be cleft palate, mandibular hypoplasia, absent or abnormal tongue morphology, hemifacial microsomia, congenital amputation of arms and legs, glossopalatine ankylosis, Horner's syndrome, cleft mandible, coloboma, scoliosis, and oblique facial clefts. Inman et al 13 reported that Foxc1 null embryos display bony syngnathia together with defects in maxillary and mandibular structures, and agenesis of the TMJ. Nanda 14 produced syngnathia and cleft palate in rats by treating them with vitamin A 3 . Dawson et al 15 classified syngnathia into types 1 and 2: type 1 being simple syngnathia with no anomalies in the head and neck region and type 2 being complex syngnathia. Type 2 was further divided into type 2a with aglossia and type 2b with agenesis or hypoplasia of the proximal mandible. This classification was later modified by Laster et al as follows: 8
Type 1a: Simple anterior syngnathia, characterized by bony fusion of the alveolar ridge only and without other congenital deformities of the head and neck region.
Type 1b: Complex anterior syngnathia, characterized by bony fusion of the alveolar ridges only and associated with other congenital deformities of the head and neck region.
Type 2a: Simple zygomatico-mandibular syngnathia, characterized by bony fusion of the mandible and the zygomatic complex causing only mandibular micrognathia.
Type 2b: Complex zygomatico-mandibular syngnathia, characterized by bony fusion of the mandible to the zygomatic complex and associated with clefts or TMJ ankylosis.
This patient can be considered as a complex zygomatico-mandibular syngnathia or type 2b, because of the bony fusion of the mandible to the zygomatic complex associated with a palatal cleft, hemifacial microsomia, agenesis of the right turbinate, and dental agenesis (elements 15, 16, 17, and 18). The patient has the highest age at diagnosis described in the literature.
Surgical treatment is a challenge as the anesthesiologic management is difficult. 5 7 We followed Hegab's treatment protocol: 5 3D surgical planning, nasotracheal intubation using fiberoptic endoscope with a tracheostomy set on standby, and long-term postoperative physiotherapy. Konaş et al described positioning a distractor between mandibular segment and maxillozygomatic complex to prevent re-ankylosis. 16 Type 2b can be associated with TMJ ankylosis, but in this patient both joints had a normal function after release of the syngnathia and the atrophic temporalis muscle. Daniels reported a similar case without TMJ ankylosis. 7 El-Hakim et al recommended placing a nasogastric tube to provide nutrition, definitely in newborns. 3 Due to the operative result at the end of the surgery and this older age, no nasogastric tube was needed. Jaw fractures during surgery have been reported in infants, 3 5 mainly due to the fragility of the mandibular bone. Re-fusion of the jaws that requires surgical re-interventions has been described. 3 To avoid this relapse, aggressive postoperative physiotherapy is mandatory. 3 We applied a protocol of daily physiotherapy for 3 months. A TheraBite Jaw Motion Rehabilitation System (Atos Medical) was used to continue physiotherapy at home. Active closure was trained, since the patient had a tendency to leave the mouth open due to atrophy of the masticatory muscles. Masticatory muscles were strengthened with electrostimulation with a Compex device (Guildford).
Conclusion
We present a case of a congenital complex zygomatico-mandibular syngnathia associated with a palatal cleft, posterior maxilla and turbinate agenesia, mild hemifacial microsomia, and a disordered dental eruption. The patient has the highest age (15 years) at diagnosis described in the literature. En bloc removal of the fused fragment with bilateral coronoidectomy and aggressive long-term physiotherapy for 3 months led to a stable increase in mouth opening from 0 to 21 mm inter-incisor distance. The patient reported an improvement in speech, was able to eat without restriction regarding food consistency, and could maintain a good oral hygiene.
References
- 1.Burket L W. Congenital bony temporomandibular ankylosis and facial hemiatrophy: Review of the literature and report of a case. J Am Med Assoc. 1936;106:1719–1722. [Google Scholar]
- 2.Fallahi H R, Naeini M, Mahmoudi M, Javaherforoosh F. Congenital zygomatico-maxillo-mandibular fusion: a brief case report and review of literature. Int J Oral Maxillofac Surg. 2010;39(09):930–933. doi: 10.1016/j.ijom.2010.04.003. [DOI] [PubMed] [Google Scholar]
- 3.El-Hakim I E, Al-Sebaei M O, Abuzennada S, AlYamani A O. Congenital fusion of the maxilla and mandible (congenital bony syngnathia) Int J Oral Maxillofac Surg. 2010;39(09):933–936. doi: 10.1016/j.ijom.2010.04.042. [DOI] [PubMed] [Google Scholar]
- 4.Subramanian B, Agrawal K, Panda K. Congenital fusion of the jaws: a management protocol. Int J Oral Maxillofac Surg. 2010;39(09):925–929. doi: 10.1016/j.ijom.2010.03.027. [DOI] [PubMed] [Google Scholar]
- 5.Hegab A, ElMadawy A, Shawkat W M. Congenital maxillomandibular fusion: a report of three cases. Int J Oral Maxillofac Surg. 2012;41(10):1248–1252. doi: 10.1016/j.ijom.2012.05.004. [DOI] [PubMed] [Google Scholar]
- 6.Parkins G E, Boamah M O. Congenital maxillomandibular syngnathia: case report. J Craniomaxillofac Surg. 2009;37(05):276–278. doi: 10.1016/j.jcms.2009.01.001. [DOI] [PubMed] [Google Scholar]
- 7.Daniels J SM. Congenital maxillomandibular fusion: a case report and review of the literature. J Craniomaxillofac Surg. 2004;32(03):135–139. doi: 10.1016/j.jcms.2004.01.005. [DOI] [PubMed] [Google Scholar]
- 8.Laster Z, Temkin D, Zarfin Y, Kushnir A. Complete bony fusion of the mandible to the zygomatic complex and maxillary tuberosity: case report and review. Int J Oral Maxillofac Surg. 2001;30(01):75–79. doi: 10.1054/ijom.2000.0009. [DOI] [PubMed] [Google Scholar]
- 9.Choi J Y, Min C G, Myoung H, Hwang S J, Kim M J, Lee J H. Acquired syngnathia. Br J Oral Maxillofac Surg. 2004;42(05):448–450. doi: 10.1016/j.bjoms.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 10.El Madi A, Khattala K, Rami M, Bouabdallah Y. Bilateral maxillo-mandibular syngnathia in a newborn. J Neonatal Surg. 2014;3(04):53. [PMC free article] [PubMed] [Google Scholar]
- 11.Patel S D, Porras S, Lypka M. Journey to chew: a case of maxillary duplication and bony syngnathia. J Craniomaxillofac Surg. 2015;43(01):57–61. doi: 10.1016/j.jcms.2014.10.010. [DOI] [PubMed] [Google Scholar]
- 12.Martín L P, Pérez M M, García E G, Martín-Moro J G, González J IR, García M B. Atypical case of congenital maxillomandibular fusion with duplication of the craniofacial midline. Craniomaxillofac Trauma Reconstr. 2011;4(02):113–120. doi: 10.1055/s-0031-1279674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Inman K E, Purcell P, Kume T, Trainor P A. Interaction between Foxc1 and Fgf8 during mammalian jaw patterning and in the pathogenesis of syngnathia. PLoS Genet. 2013;9(12):e1003949. doi: 10.1371/journal.pgen.1003949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nanda R. Maxillomandibular ankylosis in cleft palate in rat embryos. J Dental Research. 1970;49(05):1086–1090. doi: 10.1177/00220345700490051501. [DOI] [PubMed] [Google Scholar]
- 15.Dawson K H, Gruss J S, Myall R W. Congenital bony syngnathia: a proposed classification. Cleft Palate Craniofac J. 1997;34(02):141–146. doi: 10.1597/1545-1569_1997_034_0141_cbsapc_2.3.co_2. [DOI] [PubMed] [Google Scholar]
- 16.Konaş E, Aliyev A, Tunçbilek G. Congenital maxillomandibular syngnathia: a new management technique using distraction techniques. J Craniofac Surg. 2015;26(01):e68–e70. doi: 10.1097/SCS.0000000000001239. [DOI] [PubMed] [Google Scholar]