

Abstract
Cough headache can be a primary benign condition or secondary to underlying etiologies. We herein describe a case of a 52-year-old woman with cough headache that presented as reversible cerebral vasoconstriction syndrome (RCVS). Some cases of RCVS are caused by an aberrant sympathetic response to activities that cause an intracranial pressure surge. Therefore, cough headache should be recognized as a possible presentation of RCVS, even without thunderclap headache or neurological deficits.
Keywords: cough headache, reversible cerebral vasoconstriction syndrome, cerebral infarction
Introduction
Cough headache is provoked by coughing or the Valsalva maneuver. It occurs immediately after coughing and is relatively rare, with a lifetime prevalence estimated to be 1% (1). It can be a primary benign condition or secondary to underlying etiologies, most of which are associated with Arnold-Chiari malformation type I (2). By definition, primary cough headache (PCH) can be diagnosed only if the results of neuroimaging studies are normal (3).
We herein describe a patient with cough headache that presented as reversible cerebral vasoconstriction syndrome (RCVS) and highlight the possible association between PCH and RCVS.
Case Report
A 52-year-old woman without a history of headaches or prior respiratory disease was referred to an affiliated hospital because she had been experiencing sore throat and stubborn dry cough as well as recurrent and transient headaches for 2 weeks. She was diagnosed with an upper respiratory infection. The headaches, which were characterized by mild to moderate stabbing pain, developed immediately after coughing and the Valsalva maneuver and subsequently changed to a dull pain. These brief headaches were localized to the parietal regions and lasted less than 30 minutes. A diagnosis of PCH was tentatively made because her brain computed tomography scans were unremarkable.
Although loxoprofen was started at a dosage of 60 mg as needed, the intensity and frequency of headaches showed no significant improvement. The day after the consultation, she experienced transient bilateral blurred vision that resolved within 10 minutes. Five days later, although the cough stopped by the administration of benproperine phosphate, she developed a persistent and dull but bearable headache. Therefore, she revisited the medical institution. Diffusion-weighted and fluid-attenuated inversion recovery magnetic resonance imaging (MRI) revealed high-intensity lesions in the cerebral cortex of the bilateral parietal lobes (Fig. 1A). The lesions showed a decreased apparent diffusion coefficient. Magnetic resonance angiography (MRA) revealed multifocal narrowing of the cerebral arteries (Fig. 1B). She was subsequently admitted to our hospital for the further evaluation of her condition.
Figure 1.
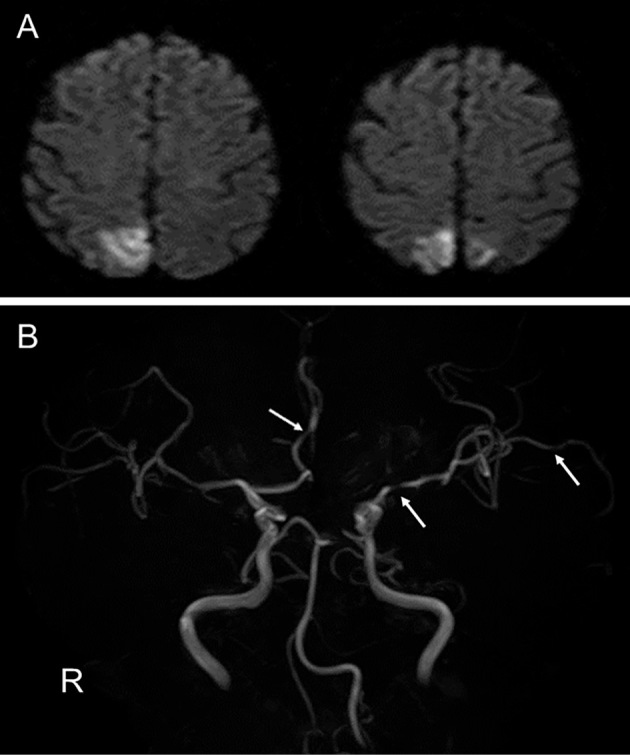
A: Diffusion-weighted magnetic resonance imaging on admission showing high-intensity lesions in the bilateral parietal lobes. B: Magnetic resonance angiography showing narrowing of the left middle and right anterior cerebral arteries (arrows).
Physical and neurological examination findings were normal. She was diagnosed with multiple cerebral infarcts due to cerebral vasoconstriction. We prescribed clopidogrel and lomerizine, and her headache gradually improved. MRA on day 8 showed no vasoconstriction of the cerebral arteries (Fig. 2). She was finally diagnosed with symptomatic cough headache with RCVS.
Figure 2.
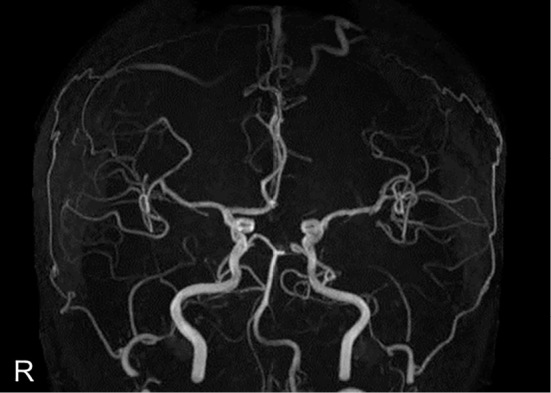
Magnetic resonance angiography showing resolution of the vessel narrowing.
Discussion
We have described a patient who experienced recurrent cough headache that seemed to fulfill the criteria for PCH as defined by the International Classification of Headache Disorders (ICHD-3 beta, code 4.1) (3). The patient's PCH did not show a benign clinical course and spontaneous recovery; in fact, brain MRI and MRA revealed multiple cerebral infarcts and RCVS, respectively. It is generally considered that cerebral infarction may occur as late as two weeks after the clinical onset of RCVS (4,5). Therefore, our patient was suspected of having had cough-induced RCVS at the time of the first headache.
The pathophysiology of PCH is not well understood, but an association with increased intracranial pressure due to coughing is suspected (6). Although the underlying causes of symptomatic cough headache are quite variable, little has been reported on RCVS as the cause of cough headache (7,8). It is important that cough headache be recognized as a possible presentation of RCVS. Some cases of RCVS are caused by an aberrant sympathetic response to activities that cause an intracranial pressure surge (9). Therefore, we emphasize that some patients with PCH might have RCVS even without clinical symptoms associated with cerebral ischemia.
Patients with RCVS rarely develop life-threatening complications, such as cerebral infarction, intracerebral hemorrhage, or reversible posterior leukoencephalopathy syndrome (4,5,10). PCH has been considered a benign condition. Based on our observations, the neurovascular imaging findings in individuals with cough headache, even without thunderclap headache or neurological deficits, need to be analyzed.
The authors state that they have no Conflict of Interest (COI).
References
- 1.Rasmussen BK, Olesen J. Symptomatic and nonsymptomatic headaches in a general population. Neurology 42: 1225-1231, 1992. [DOI] [PubMed] [Google Scholar]
- 2.Stovner LJ. Headache associated with the Chiari type I malformation. Neurology 33: 175-181, 1993. [DOI] [PubMed] [Google Scholar]
- 3.Headache Classification Committee of the International Headache Society (IHS) The international classification of headache disorders, 3rd edition (beta version). Cephalalgia 33: 629-808, 2013. [DOI] [PubMed] [Google Scholar]
- 4.Ducros A, Boukobza M, Porcher R, Sarov M, Valade D, Bousser MG. The clinical and radiological spectrum of reversible cerebral vasoconstriction syndrome. A prospective series of 67 patients. Brain 130 (Pt 12): 3091-3101, 2007. [DOI] [PubMed] [Google Scholar]
- 5.Chen SP, Fuh JL, Wang SJ, et al. . Magnetic resonance angiography in reversible cerebral vasoconstriction syndromes. Ann Neurol 67: 648-656, 2010. [DOI] [PubMed] [Google Scholar]
- 6.Cordenier A, De Hertogh W, De Keyser J, Versijpt J. Headache associated with cough: a review. J Headache Pain 14: 42, 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Pascual J, González-Mandly A, Martín R, Oterino A. Headaches precipitated by cough, prolonged exercise or sexual activity: a prospective etiological and clinical study. J Headache Pain 9: 259-266, 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Chen PK, Fuh JL, Wang SJ. Cough headache: a study of 83 consecutive patients. Cephalalgia 29: 1079-1085, 2009. [DOI] [PubMed] [Google Scholar]
- 9.Stary JM, Wang BH, Moon SJ, Wang H. Dramatic intracerebral hemorrhagic presentations of reversible cerebral vasoconstriction syndrome: three cases and a literature review. Case Rep Neurol Med 2014: 782028, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Singhal AB, Hajj-Ali RA, Topcuoglu MA, et al. . Reversible cerebral vasoconstriction syndromes: analysis of 139 cases. Arch Neurol 68: 1005-1012, 2011. [DOI] [PubMed] [Google Scholar]