

Abstract
A pediatric mandibular fracture can cause a child severe pain and the parent or caregiver extreme worry. While the pattern of fractures in children is similar to adults, however, due to a number of factors, including the anatomical complexity of the developing mandible, management of such fractures differs from that of adults and can greatly challenge the pediatric dentist. Various treatment modalities of managing mandibular fracture are available, such as closed/open cap splint with circummandibular wiring, arch-bar fixation, and cementation of the cap splint.
Keywords: Cap splint, mandible fracture, pediatric trauma
INTRODUCTION
Pediatric fractures are rare when compared with fractures in the adult population and is estimated to occur in 5% of all maxillofacial traumas.[1] Mandibular fractures are the most common (56%) facial skeletal injury in hospitalized pediatric trauma patient.[2] Boys are affected twice as frequently as girls.[3] Major injuries affecting the face are associated with respect to hyperactivity of the child, fall, road traffic accidents assault, and child abuses which are the most frequent risks of facial bone fractures in children.[4] However, due to the elasticity of mandible, embedded tooth buds that holds the fragments together “like glue” and a short thick condylar neck which tends to resist fracture,[5] thus majority of the body and symphysis fractures in children are undisplaced. If displaced, closed reduction and immobilization are performed.[6] Most fractures have been treated conservatively by dental splints and rubber elastics and occlusal cap splint with circummandibular wires.
Cap splint provides close reduction and stabilization of mandibular fracture and allows hygiene maintenance without disturbing tooth buds.[7] A long-term follow-up is necessary to monitor the growth of tooth buds and related abnormalities. This paper reports the management of mandibular fracture in a pediatric patient with cap splint.
The purpose of this article is to provide an insight on mandibular injuries in a pediatric patient and to assist the clinician in the management of mandibular or parasymphysis fracture in children, also highlighting the role of acrylic splint with the use of circummandibular wiring technique in the management of displaced parasymphysis fracture in a 6-year-old child.
CASE REPORT
A 6-year-old boy reported to the Department of Pediatric Dentistry with a history of fall while playing 2 days ago. After the fall the child did not lose consciousness, had no history of vomiting or convulsions. There was a history of bleeding from gums, difficulty in the closing mouth and chewing food.
Clinical examination revealed a diffuse extraoral swelling in the right lower one-third of the face causing a asymmetry of the face, difficulty in opening and closing the mouth, and a cut on the chin and the lower lip. Intraoral examination revealed a vertical fracture line between right mandibular primary lateral incisor and primary canine associated with medially displaced left mandibular dentoalveolar segment with step deformity and altered occlusion leading to an open mouth appearance [Figure 1]. Preoperative orthopantamogram (OPG) was taken [Figure 2], which confirmed right parasymphisis fracture. There was an associated fracture present on the left mandibular angle region.
Figure 1.

Fracture on the right para symphysis region
Figure 2.
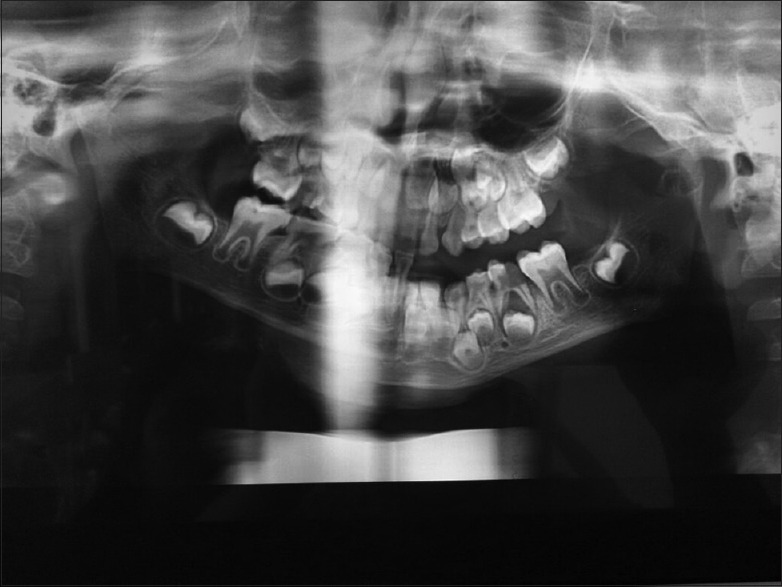
Orthopantomogram X-ray showing fracture on the right para symphysis region
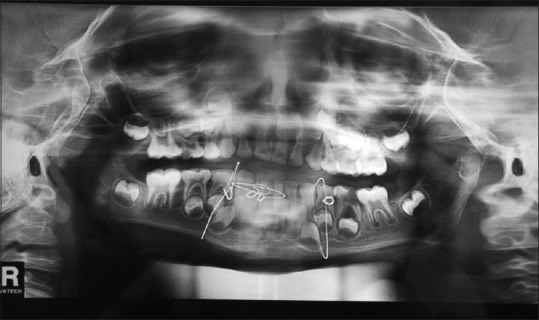
Upper and lower arch alginate impressions were taken, and stone casts were poured. An acrylic splint was fabricated, and mandibular fracture was immobilized, fixed with the acrylic splint that was retained by circum mandibular wiring. Circummandibular wiring was done under general anesthesia by placing a small-stab incision on the inferior border of mandible on the right and left side 3–4 cm from the midline. The mandibular bone awl was used to enter lingually along the body of the mandible and piercing lingual mucosa the wire was fed and passed onto buccal sulcus along the body of the mandible. Wire held together and stent stabilized by winding wire in a clockwise direction at 83.84 region. The same procedure was repeated on the left side [Figure 3]. Another circum mandibular wire was placed at the left body region to stabilize the fractured fragment at the lower border of mandible. Postoperative OPG was taken with circum mandibular wires in place [Figure 4]. The patient was reviewed every week and on the fourth postoperative week, the circum mandibular wiring and splint was removed under ketamine sedation, and OPG is taken [Figures 5 and 6]. No mobility was present at the fracture site. Postoperative recovery was uneventful and occlusion achieved was satisfactory.
Figure 3.

Circummandibular wiring done bilaterally
Figure 4.

Orthopantomogram X-ray showing circummandibular wiring is done bilaterally
Figure 5.
Four weeks after follow-up
Figure 6.

Four weeks after removal of wire
DISCUSSION
Mandibular fractures are very rare in children; however, still, mandibular fracture is the most common form of facial injury occurring in pediatric age group.[8]
The management of mandibular fractures in children differs somewhat from that of adults mainly because of the concern for possible disruption of growth. In children, the final result is determined not merely by initial treatment but by the effect that growth has on form and function.[9] The shape and shortness of deciduous crowns may make the placement of circumdental wires and arch bar slightly more difficult in children. While doing open reduction and fixation, the presence of tooth buds throughout the body of mandible must be a consideration as trauma to developing tooth buds may result in failure of eruption of permanent teeth and hence narrow alveolar ridge.[10] Several studies have recommended the use of prefabricated acrylic splints as a treatment for pediatric mandibular fractures. These splints are more reliable than open reduction or intermaxillary fixation (IMF) techniques with regard to cost-effectiveness, ease of application and removal, reduced operating time, maximum stability during healing period, minimal trauma for adjacent anatomical structures, and comfort for young patients.[11]
The patient in the present case was treated with closed reduction using custom-made cap-splint and circummandibular wiring. Various other methods have been suggested for closed reduction using prefabricated open cap splints, modified orthodontic brackets, orthodontic resin and rubber elastics, and modified orthodontic splint appliance.[12] The advantage of closed reduction over open reduction is its cost-effectiveness, lesser surgical trauma to the patient and reduced risk of any iatrogenic trauma to the developing teeth and other anatomical structures. Furthermore, the rate of associated complications is less in cases of closed reduction compared to open reduction.[13]
CONCLUSION
The anatomical complexity of the developing mandible and teeth and concerns regarding biocompatibility of implanted hardware often mandate the use of surgical techniques that differ markedly from those used in adults. In cases of mandibular fractures of a young child, disruption of periosteal envelope may have unpredictable effects on growth. Thus, if intervention is required, closed reduction is favored. Due to the technical difficulties of IMF, acrylic splints with circumferential wiring are recommended and remains the treatment of choice in young children.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Güven O. Fractures of the maxillofacial region in children. J Craniomaxillofac Surg. 1992;20:244–7. doi: 10.1016/s1010-5182(05)80435-4. [DOI] [PubMed] [Google Scholar]
- 2.Iida S, Matsuya T. Paediatric maxillofacial fractures: Their aetiological characters and fracture patterns. J Craniomaxillofac Surg. 2002;30:237–41. doi: 10.1054/jcms.2002.0295. [DOI] [PubMed] [Google Scholar]
- 3.Posnick JC, Wells M, Pron GE. Pediatric facial fractures: Evolving patterns of treatment. J Oral Maxillofac Surg. 1993;51:836–44. doi: 10.1016/s0278-2391(10)80098-9. [DOI] [PubMed] [Google Scholar]
- 4.Lalloo R. Risk factors for major injuries to the face and teeth. Dent Traumatol. 2003;19:12–4. doi: 10.1034/j.1600-9657.2003.00139.x. [DOI] [PubMed] [Google Scholar]
- 5.Kumar N, Kumar A, Syreen S, Singh S. Circummandibular wiring: A treatment approach toward management of mandibular fracture in children. Int J Clin Dent Res. 2017;1:1–3. [Google Scholar]
- 6.Mulliken JB, Kaban LB, Murray JE. Management of facial fractures in children. Clin Plast Surg. 1977;4:491–502. [PubMed] [Google Scholar]
- 7.Saoji S, Agrawal S, Bhoyar A, Shrivastava S, Mishra A, Bhusari BK, et al. Management of mandibular fracture in pediatric patient with cap splint: A case report. Int J Dent Clin. 2015;7:33–4. [Google Scholar]
- 8.Sardana D, Gauba K, Goyal A, Rattan V. Comprehensive management of pediatric mandibular fracture caused by an unusual etiology. Afr J Trauma. 2014;3:39–42. [Google Scholar]
- 9.Sharma S, Vashistha A, Chugh A, Kumar D, Bihani U, Trehan M, et al. Paediatric mandibular fractures: A review. Int J Clin Pediatric Dent. 2009;2:1–5. doi: 10.5005/jp-journals-10005-1022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yadav S, Tyagi S, Kumar P, Sharma N. Circummandibular wiring: An absolute answer to paediatric maxillofacial trauma: An unusual case report. SRM J Res Dent Sci. 2012;3:268–70. [Google Scholar]
- 11.Kocabay C, Ataç MS, Oner B, Güngör N. The conservative treatment of pediatric mandibular fracture with prefabricated surgical splint: A case report. Dent Traumatol. 2007;23:247–50. doi: 10.1111/j.1600-9657.2005.00445.x. [DOI] [PubMed] [Google Scholar]
- 12.Magennis P, Craven P. Modification of orthodontic brackets for use in intermaxillary fixation. Br J Oral Maxillofac Surg. 1990;28:136–7. doi: 10.1016/0266-4356(90)90143-9. [DOI] [PubMed] [Google Scholar]
- 13.Aizenbud D, Hazan-Molina H, Emodi O, Rachmiel A. The management of mandibular body fractures in young children. Dent Traumatol. 2009;25:565–70. doi: 10.1111/j.1600-9657.2009.00815.x. [DOI] [PubMed] [Google Scholar]