

ABSTRACT
An association between atrial myxoma and left ventricular failure is rarely described, is not completely understood, and may have multiple etiologies. We present a 49-year-old man with no history of cardiovascular disease who was admitted to our hospital with pulmonary edema. He was in atrial fibrillation with rapid ventricular response. Echocardiography showed a 10.5-cm left atrial myxoma, which had been asymptomatic until the onset of congestive heart failure in the presence of severe left ventricular systolic dysfunction. Left ventricular inflow obstruction associated with the giant atrial mass could not be the only cause for acute heart failure.
KEYWORDS: Atrial myxoma, dilated cardiomyopathy, heart failure
Atrial myxoma is the most frequent primary cardiac tumor, representing 30% to 50% of all cases.1,2 Symptoms vary and clinical presentation is usually progressive and related to size and localization of the tumor. We report a patient with a large left atrial myxoma asymptomatic until the acute onset of heart failure symptoms.
CASE PRESENTATION
A 49-year-old man with no previous history of cardiovascular diseases, having complained of only mild fatigue and wheezing over the previous few days, came to the emergency room for sudden onset of severe dyspnea and palpitations. On admission he was severely hypotensive and had a hemoglobin oxygen saturation of 80%. A systodiastolic precordial murmur radiating to the left axilla was present at the apex. An electrocardiogram showed atrial fibrillation with a rapid ventricular rate of 170 beats per minute. Transthoracic and transesophageal echocardiography (Figures 1a–1b) and computed tomography angiography (Figures 1c–1d) revealed a large oval-shaped, slightly calcified left atrial mass, contiguous to the atrial roof near the right superior pulmonary vein orifice, adherent to the inter-atrial septum. There was severe mitral regurgitation due to annular dilatation in the presence of severe left ventricular (LV) systolic dysfunction (LV ejection fraction, 26%; LV end-diastolic diameter, 68 mm). The left atrium was dilated and almost completely occupied by the mass, which partially obstructed the mitral orifice during diastole. Coronary angiography showed normal coronary arteries.
Figure 1.
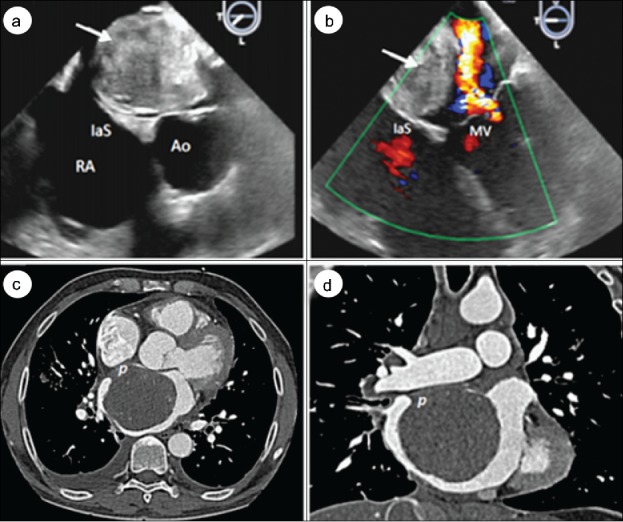
Transesophageal echocardiogram showing the huge oval-shaped and calcified left atrial mass (arrows) adherent to the (a) interatrial septum and (b) systolic jet of mitral valve insufficiency from annular dilatation. (c) Axial and (d) coronal computed tomography showing the giant and slightly calcified left atrial mass, with its pedicle attachment to the atrial roof in proximity to the right superior pulmonary vein orifice and widely adherent to the interatrial septum. RA indicates right atrium; IaS, interatrial septum; Ao, aorta; MV, mitral valve; p, pedicle.
Emergency open heart surgery was performed. Through a median sternotomy, on moderately hypothermic cardiopulmonary bypass with aortic and bicaval cannulation, the left atrium was entered through a right atriotomy and transseptal incision. A 10.5 × 9 cm myxoma was excised by resecting the pedicle implanted on the atrial roof (Figures 2a–2b). Mitral valve repair was performed with a 36-mm flexible ring annuloplasty and the left atrium appendage was closed by continuous running suture. The mass weighed 120 g. Microscopic examination of the surgical specimen confirmed the diagnosis of myxoma (Figure 2c). The patient's postoperative hospital course was uneventful, and he was discharged on the fifth postoperative day in sinus rhythm. At discharge, LV function had partially recovered (ejection fraction 43%). At 1-year follow-up, the patient was in good condition but had permanent atrial fibrillation. An echocardiogram excluded the recurrence of myxoma, the left ventricle remained dilated (LV end-diastolic diameter, 65 mm), and the ejection fraction was 45% (Figure 2d).
Figure 2.
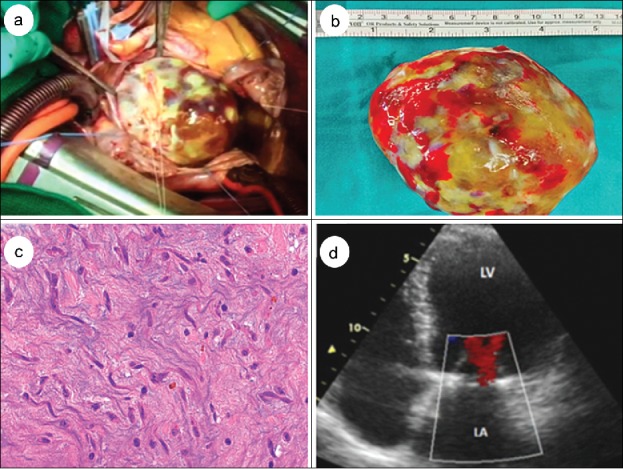
(a) Operative view of the atrial tumor almost completely occupying the left atrium. (b) Surgical specimen of the mass. (c) At microscopic examination, polygonal cells surrounded by a highly myxoid stroma are observed. (d) Apical 4-chamber transthoracic echocardiogram at 1 year follow-up showing no evidence of recurrent myxoma in the left atrium and persistent significant left ventricular dilatation. LA indicates left atrium; LV, left ventricle.
DISCUSSION
The origin and clinical manifestations of cardiac myxomas are heterogeneous. About 75% of them are located in the left atrium and 15% to 20% in the right atrium. Most originate in the interatrial septum in the proximity of the fossa ovalis.3,4 Clinical presentation may vary greatly, ranging from nonspecific cardiac symptoms (dyspnea, palpitations) to generic symptoms (fever, weight loss, fatigue) or embolic events.5,6 Cardiac symptoms are usually progressive and related to tumor size.7
Acute heart failure in patients with atrial myxoma has rarely been described, and several pathogenetic mechanisms have been proposed.8 Left atrium myxoma may cause atrial and annular dilatation with mitral insufficiency from inadequate coaptation of valve leaflets in systole and mitral stenosis from LV filling obstruction during the diastolic phase.9,10 Furthermore, in our case, the patient also presented with LV dilatation, likely related to concomitant dilated cardiomyopathy, which may have been responsible for LV dysfunction. The sudden onset of atrial fibrillation associated with ventricular tachycardia may have reduced the diastolic relaxation time, further impairing LV function and exacerbating latent chronic heart failure. Persistent ventricular dilatation and dysfunction 1 year after surgery seem to support this hypothesis. A direct cardiodepressive effect of the atrial myxoma tissue has also been reported. Release of cytokines such as interleukin (IL)-6 and IL-8 may cause myocardial tissue inflammation and biventricular hypertrophy and dilation with global ventricular dysfunction. Furthermore, studies have suggested that overproduction of IL-6 and IL-8 may induce thrombopoiesis, neutrophil migration, and myxoma cell fragment adhesion to coronary artery endothelium, leading to myocardial ischemia and infarction.11–14 In the present case, myocardial ischemia from coronary embolization of tumor fragments was excluded by normal coronary arteries in the coronary angiogram. Nevertheless, recanalization of emboli from myxoma or coronary embolization in the microvascular system could not be excluded.
As observed, acute heart failure may be the first clinical manifestation of a giant cardiac myxoma in a patient with normal coronary arteries; therefore, timely echocardiographic evaluation and surgical removal of the mass is recommended to prevent dangerous complications.
References
- 1.Di Vito A, Mignogna C, Donato G. The mysterious pathways of cardiac myxomas: a review of histogenesis, pathogenesis and pathology. Histopathology. 2015;66:321–332. doi: 10.1111/his.12531. PMID:25297937. [DOI] [PubMed] [Google Scholar]
- 2.Riberi A, Gariboldi V, Grisoli D, Collart F. Cardiac tumors. Rev Pneumol Clin. 2010;66:95–103. doi: 10.1016/j.pneumo.2009.12.012. PMID:20207301. [DOI] [PubMed] [Google Scholar]
- 3.Chiariello L, Nardi P, Saitto G, Chiariello GA. Tumori cardiaci In: Chiariello L, ed. Trattato di Chirurgia Cardiaca. Rome, Italy: Società Editrice Universo; 2016:495–502. [Google Scholar]
- 4.Reynen K. Cardiac myxomas. N Engl J Med. 1995;333:1610–1617. doi: 10.1056/NEJM199512143332407. PMID:7477198. [DOI] [PubMed] [Google Scholar]
- 5.Parato M, Pierri M, Torraca L, Scarano M. A giant myxoma of the left atrium involving the entirety of fossa ovalis: clinical course, diagnosis and treatment. Int J Cardiol. 2015;186:35–36. doi: 10.1016/j.ijcard.2015.03.216. PMID:25804463. [DOI] [PubMed] [Google Scholar]
- 6.Messina F, Romano P, Crosca S. Atrial myxomas and different clinical presentations. Int J Cardiol. 2016;203:1136–1137. doi: 10.1016/j.ijcard.2015.08.063. PMID:26442965. [DOI] [PubMed] [Google Scholar]
- 7.Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine (Baltimore). 2001;80:159–172. doi: 10.1097/00005792-200105000-00002. PMID:11388092. [DOI] [PubMed] [Google Scholar]
- 8.Raut MS, Shad S, Maheshwari A. Left atrial myxoma with biventricular dysfunction. Indian Heart J. 2016;68:S163–S165. doi: 10.1016/j.ihj.2016.03.004. PMID:27751276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Keeling IM, Oberwalder P, Anelli-Monti M, et al.. Cardiac myxomas: 24 years of experience in 49 patients. Eur J Cardiothorac Surg. 2002;22:971–977. doi: 10.1016/S1010-7940(02)00592-4. PMID:12467822. [DOI] [PubMed] [Google Scholar]
- 10.Goswami KC, Shrivastava S, Bahl VK, Saxena A, Manchanda SC, Wasir HS. Cardiac myxomas: clinical and echocardiographic profile. Int J Cardiol. 1998;63:251–259. doi: 10.1016/S0167-5273(97)00316-1. PMID:9578352. [DOI] [PubMed] [Google Scholar]
- 11.Chockalingam A, Jaganathan V, Gnanavelu G, Dorairajan S, Chockalingam V. Severe left ventricular dysfunction in left atrial myxoma: report of 2 cases. Angiology. 2006;57:119–122. doi: 10.1177/000331970605700118. PMID:16444467. [DOI] [PubMed] [Google Scholar]
- 12.Currey HL, Mathews JA, Robinson J. Right atrial myxoma mimicking a rheumatic disorder. Br Med J. 1967;1:547–548. doi: 10.1136/bmj.1.5539.547. PMID:5297370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kanda T, Takahashi T. Interleukin-6 and cardiovascular diseases. Jpn Heart J. 2004;45:183–193. doi: 10.1536/jhj.45.183. PMID:15090695. [DOI] [PubMed] [Google Scholar]
- 14.Marta L, Peres M, Alves M, Da Silva GS. Giant left atrial myxoma presenting as acute myocardial infarction. Rev Port Cardiol. 2012;31:815–819. PMID:23138051. [DOI] [PubMed] [Google Scholar]