

Introduction
Takotsubo cardiomyopathy (TCM) or transient left ventricular (LV) apical ballooning syndrome was first noted in 1991 in five Japanese men and is characterized by a clinical syndrome mimicking acute myocardial infarction (1). Although the exact pathogenesis of TCM has not been described yet, catecholamine surge and alteration of responses to different types of receptors on the endocardium leading to microvascular dysfunction is currently the most widely accepted theory (2). A recent systematic review demonstrated that despite emotional or physical stress, catecholamine surge resulted from pharmacologic stress could also precipitate TCM and that the most common medication associated with drug-induced TCM was epinephrine followed by dobutamine, a strong β1 agonist (3). Dobutamine stress echocardiography (DSE) is a noninvasive test used to assess any stress-induced regional wall motion abnormalities. Vasospasm and/or a catecholamine surge may be triggered by dobutamine due to its inotropic effect (4).
Although DSE is generally considered a safe procedure, it has been shown that TCM can occur either during the peak stress or recovery period of the test (5). Here, we report a case of DSE-induced TCM along with a systematical review of 21 studies (22 patients) with similar scenarios and present clinical difference between DSE-induced and classic TCM.
Case Report
A 74-year-old female was referred for evaluation of pain in the left arm. She reported no chest pain or dyspnea on exertion, but her past medical history was noteworthy due to hypertension, diabetes, and dyslipidemia. Her baseline electrocardiogram (ECG) showed sinoatrial node arrest without a significant ST-T change (Fig. 1, panel C). Her resting echocardiogram was normal, but to evaluate a possible regional wall motion abnormality (RWMA), DSE was performed. A standard dobutamine/atropine protocol was used with 10 mcg/kg/min dose increments at 3 min intervals. At stage 5, the dobutamine dose was increased to 40 mcg/kg/min and the patient experienced severe diaphoresis but no chest pain. ECG revealed a significant ST segment elevation in the anterolateral leads, along with premature ventricular couplet contractions (Fig. 1, panel D); in a concomitant echocardiographic image, we noticed an akinetic myocardium from the mid to apical part of the septum and a reduced left ventricular ejection fraction (LVEF) of 25% at the peak of the test (Fig. 1, panel B).
Figure 1.
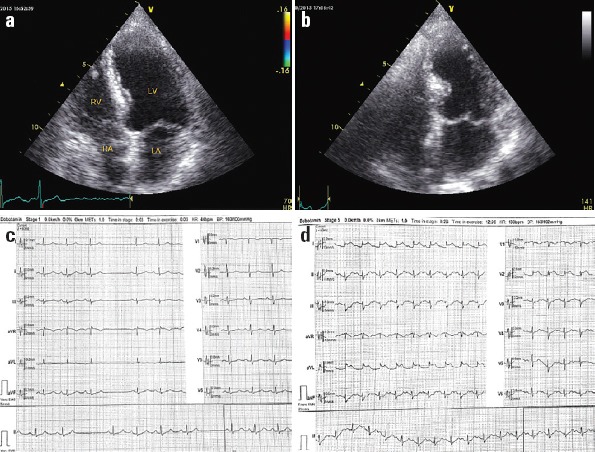
Baseline TTE showed no wall motion abnormality in a 4-chamber view with LVEF of 55% (panel A), and a concomitant ECG showed a sinus rhythm with SA arrest and no ST-T change (panel C). TTE at peak of the test in 4-chamber view showed akinetic myocardium from the mid to apical part of septum with LVEF of 25% (panel B), and a concomitant ECG showed an ST elevation in I, aVL, V2 with subtle ST depression in inferior leads at peak of test (panel D). ECG -electrocardiogram; LA - left atrium; LV - left ventricle; LVEF - left ventricle ejection fraction; RA - right atrium; RV - right ventricle; SA - sinoatrial node; TTE - transthoracic echocardiogram
The patient underwent an immediate coronary angiography; it showed normal epicardial coronary arteries, but a left ventriculogram revealed features suggestive of TCM (Fig. 2). Peak serum troponin I concentration was elevated to 7 µg/L. Our patient received diuretics, β-blockers, nitrates, and angiotensin converting enzyme (ACE) inhibitors and a follow-up echocardiography in 4 weeks, which showed a good systolic function with no resting RWMA.
Figure 2.
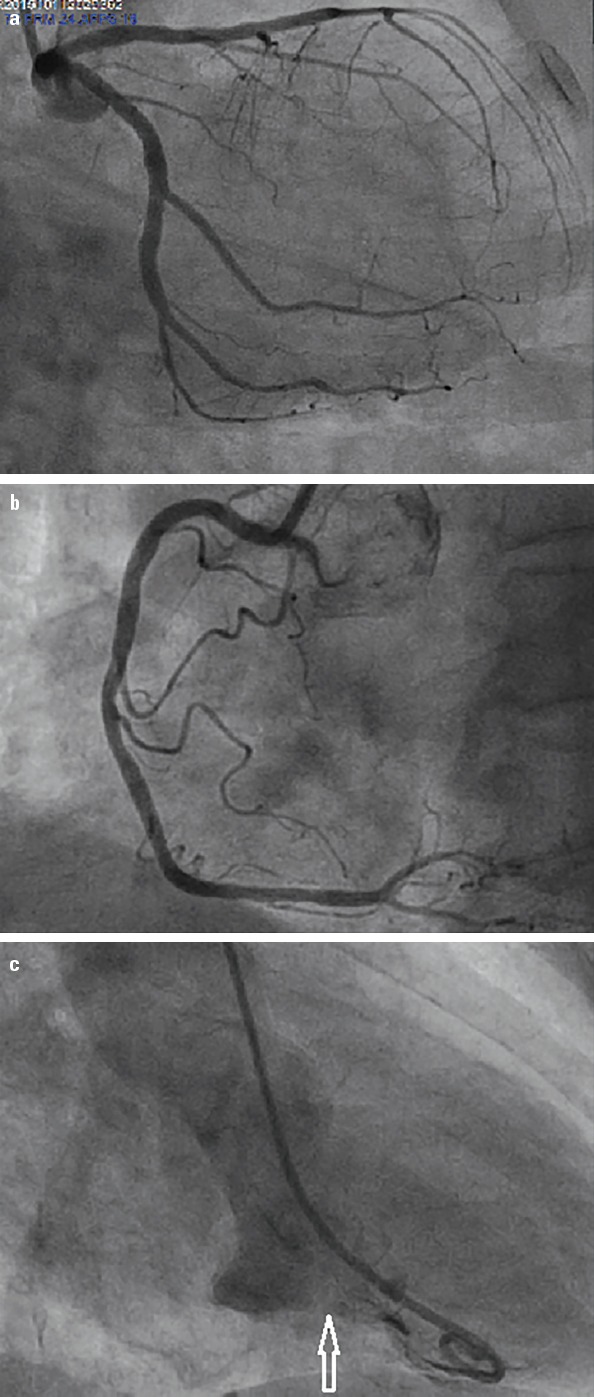
Panel A and B. Left and right injection showing no obstructing lesion in left and right coronary arteries. Panel C. Left ventriculogram showing hyper dynamic basal myocardial segments associated with anterior akinesia (white arrow)
Literature and Discussion
This systematic review was performed according to the Preferred Reporting Items and checklist for Systematic Reviews and Meta-Analyses (PRISMA) (6). We searched the Cochrane Library, MEDLINE (via PUBMED), and EMBASE (up to May 20, 2017) to identify relevant reports. The search terms were selected according to the Medical Subject Heading terms: “Broken Heart Syndrome”, “Takotsubo Syndrome”, “Transient Apical Ballooning Syndrome”, “Apical Ballooning Syndrome”, “Takotsubo cardiomyopathy”, “Inverted Takotsubo”, “Reverse Takotsubo” and “Dobutamine stress echocardiography.” These themes were combined with “Dobutamine” using “AND”. Also, we included “Case report” publications in any language and in title and abstract.
Preliminary searches resulted in 34 records. All records imported from Cochrane Library, MEDLINE, and EMBASE are shown in a table (Supplementary File 1). This table was used for study selection based on eligibility criteria.
Eligibility criteria
Development of TCM only after pharmacologic stress with dobutamine during stress echocardiography or myocardial perfusion scan or MRI
Absence of other comorbidities that could precipitate or induce cardiomyopathy including Duchenne muscular dystrophy, heart transplant, subarachnoid hemorrhage, and consumption of chemotherapy agents
Articles in English language
Two expert cardiologists identified 21 relevant publications (22 patients; Fig. 3). Data extraction of 22 patients was performed and demographic variables, clinical presentation, type of TCM, ECG findings, cardiac enzymes, and outcome of all patients were studied. Categorical variables are expressed as percentage and continuous variables as mean±SD. A written consent was obtained from our patient for publishing her medical records.
Figure 3.
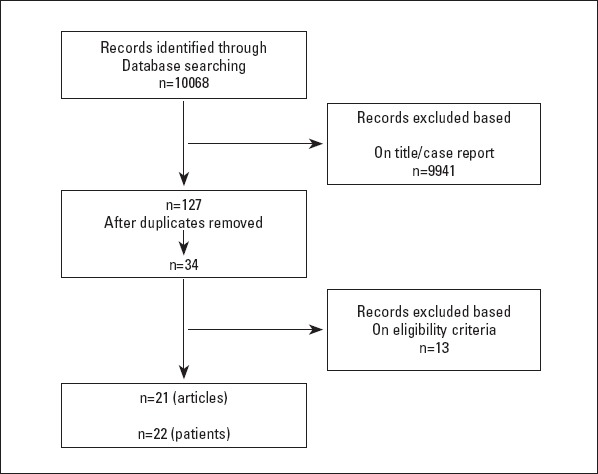
Flow diagram describing searching strategy and study selection
We identified 22 patients from 21 articles of TCM associated with dobutamine stress imaging either echocardiography or myocardial perfusion scan (Table 1). The mean age of presentation was 64.86±11.64 years, with strong female predominance (n=19; 86%). The most common presenting symptoms were chest pain (n=13; 56%), dyspnea (n=2), and abdominal pain (n=1); six patients were asymptomatic. The dose of dobutamine given when symptoms began was 30-40 mcg/kg/min (n=16), 20 mcg/kg/min (n=1), 10 mcg/kg/min (n=1), 5 mcg/kg/min (n=1) and symptoms began during the recovery period in three patients. The most common type of TCM was the apical type (n=19); other types including inverted type (n=2) and midventricular type (n=1) were also seen. Patients younger than 55 years were more likely to have inverted type or midventricular type of cardiomyopathy. The mean cardiac troponin I level was 2.68±2.70 ng/dL, with normal value <0.01 ng/dL; however, the levels were not increased in two patients and were not available in five. ECG during peak stress revealed an ST elevation in most patients (n=15), no ST-T change (n=3), T wave abnormalities (n=2), ST depression (n=1), and left anterior fascicular block (n=1). A ventricular bigeminy was detected in two patients. Among three patients who did not evolve any ST-T change on ECG, two of them were asymptomatic. A complete resolution of any wall motion abnormality was achieved (n=20), except for a near complete resolution in one patient and death of one patient; patient developed pulseless electrical activity and could not be resuscitated. The patient’s family declined an autopsy. The diagnosis of LV apical ballooning syndrome with LVOT obstruction secondary to dobutamine stress testing was presumed (16).
Table 1.
Analysis of 22 patients with dobutamine stress test-induced takotsubo cardiomyopathy
| Study | Age | Sex | Type | Symptom | ECG | Dose of Dobutamine | cTnI level | Follow-up | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Arias AM et al.8 | 77 | Female | Apical type EF: 34% | CP | ST- elevation | 40 mcg/ kg/min | Not available | Complete resolution |
| 2 | Mosley ll et al.4 | 50 | Female | Apical type EF: 20% | CP | ST- elevation | 30 mcg/ kg/Min | 2.56 | Near Complete resolution |
| 3 | Silberbauer J et al.19 | 75 | Female | Apical type | CP | ST- elevation | 30 mcg/ kg/min | 1.06 | Complete resolution |
| 4 | Mosley ll et al.4 | 74 | Female | Apical type EF: 35% | CP | ST elevation | 40 mcg/ kg/min | 2.40 | Complete resolution |
| 5 | Margey R et al.20 | 61 | Female | Apical type | Dyspnea | ST elevation, ventricular bigeminy | 40 mcg/ kg/min | 4.8 | Complete resolution |
| 6 | Shah BN et al.5 | 85 | Female | Apical type | Dyspnea | ST elevation | Recovery period | 2.62 | Complete resolution |
| 7 | Cherian J et al.16 | 85 | Female | Apical type EF: 35% | Asymptomatic | ST elevation | Recovery period | Not available | Patient expired |
| 8 | Chia PL et al.13 | 53 | Male | Inverted type EF: 20% | CP | No ST-T change | 40 mcg/ kg/min | Not increased | Complete resolution |
| 9 | Chandraprakasam et al.14 | 48 | Female | Midventricular type | CP | LAHB, ventricular bigeminy | 40 mcg/ kg/min | 0.41 | Complete resolution |
| 10 | Kumar A et al.21 | 66 | Female | Apical type | CP | ST elevation | 40 mcg/ kg/min | 0.73 | Complete resolution |
| 11 | Cadeddu C et al.12 | 48 | Female | Inverted type EF: 28% | Asymptomatic | No ST-T change | 40 mcg/ kg/min | Not increased | Complete resolution |
| 12 | Yu AF et al.22 | 52 | Male | Apical type | Abdominal pain | ST elevation | 40 mcg/ kg/min | Not available | Complete resolution |
| 13 | Vasconcelos FFJ et al.23 | 76 | Female | Apical type | Asymptomatic | ST elevation | 40 mcg/ kg/min | 0.8 | Complete resolution |
| 14 | D’Aloia A et al.24 | 56 | Female | Apical type EF: 35% | CP | ST depression | 30 mcg/ kg/min | 5.65 | Complete resolution |
| 15 | Skolnick AH et al.25 | 53 | Female | Apical type | CP | ST elevation | 40 mcg/ kg/min | 7 | Complete resolution |
| 16 | Meimoun P et al.26 | 63 | Female | Apical type + SAM | Asymptomatic | No ST change | 30 mcg/ kg/min | - | Complete resolution |
| 17 | Chaparro-Muñoz M et al.27 | 62 | Female | Apical type | CP | T wave abnormalities | 20 mcg/ kg/min | 1.83 | Complete resolution |
| 18 | Uznanska B et al.28 | 59 | Female | Apical typ EF: 45%e | CP | T wave abnormalities | 10 mcg/ kg/min | 0.28 | Complete resolution |
| 19 | Brewington SD et al.17 | 72 | Female | Apical type | CP | ST elevation, PVC | recovery | - | Complete resolution |
| 20 | Bruder O et al.29 | 65 | Female | Apical type | CP | ST elevation | 40 mcg/ kg/min | 9 | Complete resolution |
| 21 | Sonmez O et al.30 | 74 | Female | Apical type EF: 45% | Asymptomatic | ST elevation | 5 mcg/ kg/min | 0.5 | Complete resolution |
| 22 | Fineschi M et al.31 | 73 | Male | Apical type | Asymptomatic | ST elevation | 40 mcg/ kg/min | 0.6 | Complete resolution |
CP - chest pain; cTnI - cardiac troponin I (normal value <0.01 ng/dL=mcg/L); DSE - dobutamine stress echocardiography; EF - ejection fraction; LAHB - left anterior hemiblock; WMA - wall motion abnormalities; SAM - systolic anterior motion of the mitral valve, TCM - takotsubo cardiomyopathy
TCM is rare and sometimes an incidental finding affecting nearly 2%-3% of people, mostly in postmenopausal women who are diagnosed with myocardial infarction. According to the Mayo Clinic criteria, we need all of the following four criteria for a diagnosis of TCM: 1) transient hypokinesis, akinesis, or dyskinesis of the LV mid-segments; 2) the absence of obstructive coronary disease or angiographic evidence of acute plaque rupture; 3) new ECG abnormalities or an elevation in cardiac troponin levels; and 4) the absence of pheochromocytoma or myocarditis (7).
DSE is a noninvasive test that evaluates the “inotropic reserve” of dysfunctional but viable myocardium at rest by the administration of an inotropic agent. The standard protocol for DSE is graded dobutamine infusion in five 3-min stages starting at 5 mcg/kg/min followed by 10, 20, 30, and 40 mcg/kg/min. Atropine in a divided dose of 0.5 mg to a total of 2 mg is also administered as needed to increase the heart rate. During transthoracic echocardiography, an improvement in global or regional contractile function (inotropic reserve) suggests viable myocardium (9). Dobutamine stress testing is generally safe and well tolerated. Although both cardiac (e.g., arrhythmia, chest pain, left ventricular outflow tract obstruction) and noncardiac side effects can occur, serious complications such as ventricular fibrillation and myocardial infarction are rare, occurring in one of every 2000 studies (10). One of the rare complications of DSE is TCM since the main proposed and widely accepted mechanism of TCM is an excess of catecholamine secretion; a condition that happens during DSE.
Our review showed that pharmacologic beta-adrenergic drug-induced TCM occurs in population similar to classic TCM, mostly in women aged 65 years or more. The most common presenting symptom in pharmacologic beta- adrenergic drug-induced TCM was chest pain and the most common ECG change was ST segment elevation; findings that were consistent with the International Takotsubo Registry study. However, in our review, six patients developed TCM without any symptoms; a finding that was inconsistent with classic TCM (11, 18). The troponin level was elevated in 11 (50%) patients with DSE-induced TCM, consistent with previous studies that showed troponin levels were elevated in nearly 87% of patients with TCM, with mean levels similar to those in patients with an acute coronary syndrome (12).
Our review along with previous studies showed that the most common type of wall motion abnormality is apical type, followed by inverted type in patients younger than 55 years (12, 13) or midventricular type of cardiomyopathy (14). A recent systematic review demonstrated that patients aged 45 years or less were less likely to have apical variant cardiomyopathy compared with patients aged 45 years or more (15). Although in most patients TCM occurred when the dose of dobutamine reached 30-40 mcg/kg/min, in three patients, it happened in the recovery period (5, 16, 17). Considering the outcomes, except for one patient, the wall motion abnormality was transient.
Conclusion
Pharmacologic stress including dobutamine infusion during stress echocardiography could precipitate TCM. In contrast to classic TCM, it can present even without any symptoms and can also occur in the recovery phase of the test. Mortality was seen in only one patient, but TCM could be a complicating factor while performing pharmacological stress tests and clinicians need to be vigilant throughout the test and the recovery period (1, 6).
Acknowledgements:
The authors wish to thank Rozhin Pahlevani for guidance in literature review and data interpreting.
Footnotes
Funding: Scott R Jafarian-Kerman was supported by Grant NIH T32 GM007569.
References
- 1.Gianni M, Dentali F, Grandi AM, Sumner G, Hiralal R, Lonn E. Apical ballooning syndrome or takotsubo cardiomyopathy:a systematic review. Eur Heart J. 2006;27:1523–9. doi: 10.1093/eurheartj/ehl032. [DOI] [PubMed] [Google Scholar]
- 2.Nef HM, Möllmann H, Kostin S, Troidl C, Voss S, Weber M, et al. Tako-tsubo cardiomyopathy:intraindividual structural analysis in the acute phase and after functional recovery. Eur Heart J. 2007;28:2456–64. doi: 10.1093/eurheartj/ehl570. [DOI] [PubMed] [Google Scholar]
- 3.Kido K, Guglin M. Drug-Induced Takotsubo Cardiomyopathy. J Cardiovasc Pharmacol Ther. 2017;22:552–63. doi: 10.1177/1074248417708618. [DOI] [PubMed] [Google Scholar]
- 4.Mosley WJ, 2nd, Manuchehry A, McEvoy C, Rigolin V. Takotsubo cardiomyopathy induced by dobutamine infusion:a new phenomenon or an old disease with a new name. Echocardiography. 2010;27:E30–3. doi: 10.1111/j.1540-8175.2009.01089.x. [DOI] [PubMed] [Google Scholar]
- 5.Shah BN, Simpson IA, Rakhit DJ. Takotsubo (apical ballooning) syndrome in the recovery period following dobutamine stress echocardiography:a first report. Eur J Echocardiogr. 2011;12:E5. doi: 10.1093/ejechocard/jeq107. [DOI] [PubMed] [Google Scholar]
- 6.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions:explanation and elaboration. PLoS Med. 2009;6:e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, et al. Systematic review:transient left ventricular apical ballooning:a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med. 2004;141:858–65. doi: 10.7326/0003-4819-141-11-200412070-00010. [DOI] [PubMed] [Google Scholar]
- 8.Arias AM, Oberti PF, Pizarro R, Falconi ML, de Arenaza DP, Zeffiro S, et al. Dobutamine-Precipitated Takotsubo Cardiomyopathy Mimicking Acute Myocardial Infarction A Multimodality Image Approach. Circulation. 2011;124:e312–5. doi: 10.1161/CIRCULATIONAHA.110.008557. [DOI] [PubMed] [Google Scholar]
- 9.Pellikka PA, Nagueh SF, Elhendy AA, Kuehl CA, Sawada SG American Society of Echocardiography. American Society of Echocardiography recommendations for performance, interpretation, and application of stress echocardiography. J Am Soc Echocardiogr. 2007;20:1021–41. doi: 10.1016/j.echo.2007.07.003. [DOI] [PubMed] [Google Scholar]
- 10.Mathias W, Jr, Arruda A, Santos FC, Arruda AL, Mattos E, Osório A, et al. Safety of dobutamine-atropine stress echocardiography:a prospective experience of 4033 consecutive studies. J Am Soc Echocardiogr. 1999;12:785–91. doi: 10.1016/s0894-7317(99)70182-3. [DOI] [PubMed] [Google Scholar]
- 11.Templin C, Ghadri JR, Diekmann J, Napp LC, Bataiosu DR, Jaguszewski M, et al. Clinical Features and Outcomes of Takotsubo (Stress) Cardiomyopathy. N Engl J Med. 2015;373:929–38. doi: 10.1056/NEJMoa1406761. [DOI] [PubMed] [Google Scholar]
- 12.Cadeddu C, Nocco S, Cadeddu F, Deidda M, Bassareo P, Serra A, et al. Inverted Takotsubo cardiomyopathy induced by dobutamine stress echocardiography with atypical presentation. Case Rep Cardiol. 2011;2011:413645. doi: 10.1155/2011/413645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chia PL, Lee E. Reverse Takotsubo pattern stress cardiomyopathy in a male patient induced during dobutamine stress echocardiography. Ann Acad Med Singapore. 2012;41:264. [PubMed] [Google Scholar]
- 14.Chandraprakasam S, Kanuri S, Hunter C. Mid-ventricular variant of dobutamine-induced stress cardiomyopathy. Res Cardiovasc Med. 2015;4:e25223. doi: 10.5812/cardiovascmed.4(2)2015.25223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nazir S, Lohani S, Tachamo N, Ghimire S, Poudel DR, Donato A. Takotsubo cardiomyopathy associated with epinephrine use:A systematic review and meta-analysis. Int J Cardiol. 2017;229:67–70. doi: 10.1016/j.ijcard.2016.11.266. [DOI] [PubMed] [Google Scholar]
- 16.Cherian J, Kothari S, Angelis D, Atef A, Downey B, Kirkpatrick J., Jr Atypical Takotsubo Cardiomyopathy:Dobutamine-Precipitated Apical Ballooning with Left Ventricular Outflow Tract Obstruction. Tex Heart Inst J. 2008;35:73–5. [PMC free article] [PubMed] [Google Scholar]
- 17.Brewington SD, Abbas AA, Dixon SR, Grines CL, O'Neill WW. Reproducible microvascular dysfunction with dobutamine infusion in Takotsubo cardiomyopathy presenting with ST segment elevation. Catheter Cardiovasc Interv. 2006;68:769–74. doi: 10.1002/ccd.20514. [DOI] [PubMed] [Google Scholar]
- 18.Eitel I, von Knobelsdorff-Brenkenhoff F, Bernhardt P, Carbone I, Muellerleile K, Aldrovandi A, et al. Clinical characteristics and cardiovascular magnetic resonance findings in stress (takotsubo) cardiomyopathy. JAMA. 2011;306:277–86. doi: 10.1001/jama.2011.992. [DOI] [PubMed] [Google Scholar]
- 19.Silberbauer J, Hong P, Lloyd GW. Takotsubo cardiomyopathy (left ventricular ballooning syndrome) induced during dobutamine stress echocardiography. Eur J Echocardiogr. 2008;9:136–8. doi: 10.1016/j.euje.2007.04.006. [DOI] [PubMed] [Google Scholar]
- 20.Margey R, Diamond P, McCann H, Sugrue D. Dobutamine stress echo-induced apical ballooning (Takotsubo) syndrome. Eur J Echocardiogr. 2009;10:395–9. doi: 10.1093/ejechocard/jen292. [DOI] [PubMed] [Google Scholar]
- 21.Kumar A, Jenkins LA, Perez-Verdia A, Roongsritong C. Transient left ventricular apical ballooning during dobutamine myocardial perfusion imaging. Int J Cardiol. 2008;124:378–80. doi: 10.1016/j.ijcard.2006.11.248. [DOI] [PubMed] [Google Scholar]
- 22.Yu AF, Mitter SS, Chaudhry HW. Apical ballooning syndrome precipitated by dobutamine stress testing. Heart Asia. 2013;5:47–8. doi: 10.1136/heartasia-2013-010292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Vasconcelos Filho FJ, Gomes CA, Queiroz OA, Barreto JE. Dobutamine stress echocardiography-induced broken heart syndrome (Takotsubo Syndrome) Arq Bras Cardiol. 2009;93:e5–7. doi: 10.1590/s0066-782x2009000700014. [DOI] [PubMed] [Google Scholar]
- 24.D'Aloia A, Caretta G, Vizzardi E, Zanini G, Bugatti S, Bonadei I, et al. Heart failure syndrome due to dobutamine stress echocardiography:Tako-Tsubo induced-cardiomiopathy. Panminerva Med. 2012;54:53–5. [PubMed] [Google Scholar]
- 25.Skolnick AH, Michelin K, Nayar A, Fisher D, Kronzon I. Transient apical ballooning syndrome precipitated by dobutamine stress testing. Ann Intern Med. 2009;150:501–2. doi: 10.7326/0003-4819-150-7-200904070-00015. [DOI] [PubMed] [Google Scholar]
- 26.Meimoun P, Clerc J, Botoro T, Elmkies F, Martis S, Zemir H, et al. Systolic anterior motion of the mitral valve in tako-tsubo cardiomyopathy:still a matter of debate? Ann Cardiol Angeiol (Paris) 2015;64:385–9. doi: 10.1016/j.ancard.2015.09.048. [DOI] [PubMed] [Google Scholar]
- 27.Chaparro-Muñoz M, Recio-Mayoral A, Kaski JC, Brecker S, Sutherland GR. Myocardial stunning identified by using strain/strain rate imaging during dobutamine stress echocardiography in a rare late recurrence of Tako–Tsubo syndrome. Int J Cardiol. 2010;145:e9–12. doi: 10.1016/j.ijcard.2008.12.095. [DOI] [PubMed] [Google Scholar]
- 28.Uznańska B, Plewka M, Wierzbowska-Drabik K, Chrzanowski Ł, Kasprzak JD. Early prediction of ventricular recovery in Takotsubo syndrome using stress and contrast echocardiography. Med Sci Monit. 2009;15:CS89–94. [PubMed] [Google Scholar]
- 29.Bruder O, Hunold P, Jochims M, Waltering KU, Sabin GV, Barkhausen J. Reversible late gadolinium enhancement in a case of Takotsubo cardiomyopathy following high-dose dobutamine stress MRI. Int J Cardiol. 2008;127:e22–4. doi: 10.1016/j.ijcard.2007.01.081. [DOI] [PubMed] [Google Scholar]
- 30.Sonmez O, Duman C, Duzenli MA, Tokac M. Special attention for elderly women:atypical left ventricular apical ballooning syndrome induced by dobutamine stress test:a case report. J Am Geriatr Soc. 2009;57:1735–6. doi: 10.1111/j.1532-5415.2009.02424.x. [DOI] [PubMed] [Google Scholar]
- 31.Fineschi M, D'Ascenzi F, Sirbu V, Mondillo S, Pierli C. The role of optical coherence tomography in clarifying the mechanisms for dobutamine stress echocardiography-induced takotsubo cardiomyopathy. Echocardiography. 2013;30:E121–4. doi: 10.1111/echo.12107. [DOI] [PubMed] [Google Scholar]