

Abstract
Diffuse gallbladder wall thickening is a common radiological finding with a wide range of differential diagnoses, many of which are not due to primary cholecystic disease. We report an unusual case of extreme diffuse gallbladder thickening in a 39-year-old lady, subsequently diagnosed with hepatitis C virus, and with complete resolution of her radiological appearances within 6 weeks—before commencing any treatment.
Keywords: Gallbladder, Wall thickening, Hepatitis C, Ultrasonography
Introduction
Diffuse gallbladder wall thickening is typically regarded as greater than 3 mm by ultrasound and can occur in a number of surgical and nonsurgical conditions [1]. Although the finding is often a characteristic hallmark of acute cholecystitis, gallbladder wall thickening is a nonspecific finding [2] and may also be due to secondary inflammatory spread from other structures such as the pancreas or the liver [3]. The differential diagnoses of gallbladder wall thickening are commonly divided into those due to primary gallbladder disease and those due to secondary extracholecystic conditions (Fig. 1) [4]. Differentiating between the 2 requires a thorough clinical examination in addition to imaging as it may determine treatment considerations such as whether the patient undergoes cholecystectomy.
Fig. 1.

Possible differential diagnoses of gallbladder thickening divided into primary or secondary (extracholecystic).
Previous literature has reported different degrees of gallbladder wall thickening and a range of underlying pathologies. For example, the mural thickening reported in acute cholecystitis is secondary to edema and inflammatory changes and is often associated with cholelithiasis and gallbladder distension. In contrast, the edematous changes seen as a result of systemic disease, such as heart or renal failure, are not associated with gallbladder inflammation and are thought to be due to raised portal pressures. The degree of wall thickening in these cases may be much more impressive and has been reported as >10 mm [3]. In addition, Baik et al. reported a mean wall thickness of 5.6 mm, which was due to serosal and muscular hypertrophy, associated with acute hepatitis [5]. Lastly, a very pronounced wall thickening shown on ultrasound or computed tomography (CT) (>10 mm) should raise concern about the possibility of malignancy, which is often associated with mural irregularity [3].
Mild gallbladder wall thickening is conventionally defined as 4-7 mm. Previous studies have reported thickening of up to 6 mm in acute hepatitis [5], [6]; however, we present a case of extreme, generalized thickening of more than 33 mm on CT imaging, which completely resolves on follow-up scan 6 weeks later.
Case report
A 39-year-old woman presented to the emergency department with a 7-day history of worsening right upper quadrant and epigastric pain. On questioning, the patient reported dark urine but no pale stools. She was a known intravenous drug user with a medical history of posttraumatic stress disorder and generalized anxiety disorder. Her drug history consisted of methylphenidate and clonazepam and she had no drug allergies.
On examination, the patient was clinically jaundiced and tender in the right upper quadrant. Murphy sign was negative, there was no rebound tenderness, and no ascites were present. There was no organomegaly. Her blood pressure, temperature, pulse, and oxygen saturations were all within normal limits. Differential diagnoses at this point included cholecystitis, hepatitis, an obstructing gallstone, and pancreatic malignancy.
Blood tests revealed markedly deranged liver function tests with an obstructive jaundice (bilirubin 155, ALP 243, ALT 2171, AST 1646, albumin 39, platelet count 77, amylase 15). There were no previous results available for comparison. Her inflammatory markers were not raised and her hemoglobin was 160. HIV serology was negative.
An ultrasound scan (Fig. 2) showed diffuse thickening of the gallbladder wall, up to 20 mm in diameter, with a lamellated hypoechoic appearance. There were no gallstones seen, and no dilatation of the intrahepatic ducts. There was no pericholecystic fluid, no gallbladder hydrops, and no emphysematous cholecystitis. No abnormality was seen in the visualized pancreas; however, there was splenomegaly, measuring up to 141 mm in length with a homogeneous echotexture. The liver was decreased in echotexture, with increased echogenicity to the portal venule walls diffusely throughout the liver, suggesting underlying hepatitis.
Fig. 2.
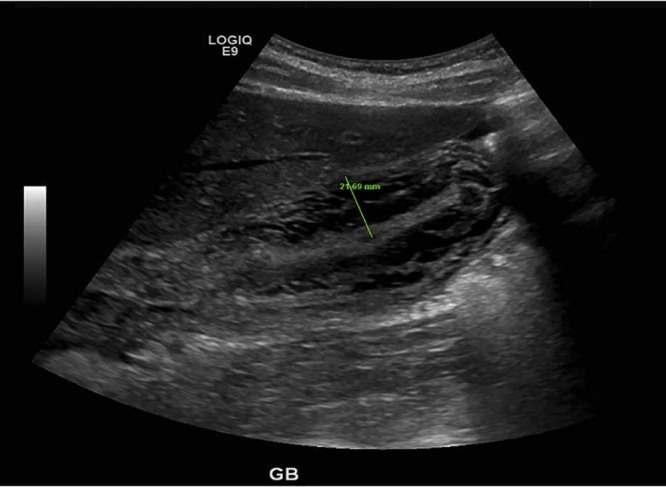
Ultrasound scan demonstrating marked gallbladder wall thickening (21 mm) and a collapsed lumen.
The same day, a triphasic CT scan of the liver was performed (Fig. 3), which again demonstrated diffuse gallbladder thickening and surrounding edema with a maximum axial thickness of 33 mm. Patchy enhancement of the liver was seen in the arterial phase, but not the venous phase, and this was thought to be perfusional and possibility related to hepatitis. A small amount of ascites in the peritoneal cavity was seen and thought to be nonspecific and secondary to hypoalbuminaemia.
Fig. 3.

A computed tomography scan with contrast demonstrating marked gallbladder wall thickening (33 mm) with a hyperdense collapsed lumen.
Serological testing confirmed an active hepatitis C infection (antibody positive, RNA positive) with a viral load of 70,207 IU/mL, and genotype testing confirmed type 1. Th patient was managed conservatively on the medical ward; however, she discharged herself before receiving specialist input. This patient is now attending hepatology outpatient clinic with a view to commencing treatment.
A repeat ultrasound scan of the abdomen (Fig. 4) was performed 6 weeks later showing complete resolution of the gallbladder thickening and no other abnormalities of the liver parenchyma.
Fig. 4.

Follow-up ultrasound scan after 6 weeks, demonstrating normal appearances of the gall bladder.
Discussion
Determining the cause of gallbladder thickening requires correlation of the imaging with the clinical history and examination findings along with laboratory investigations. In this case, the lack of raised inflammatory markers, the deranged liver function tests, and the history of drug abuse raised the suspicion of hepatitis C infection and this was subsequently confirmed on serology. There was also abnormal perfusion of the liver on CT and decreased echotexture seen on ultrasound consistent with hepatitis.
There is a well-known correlation between gallbladder wall thickening and acute hepatitis with an incidence of up to 63% [7]. There is also some evidence showing a higher incidence of primary gallbladder disease in patients with hepatitis C infection [8]. A number of mechanisms have been suggested for this including altered gallbladder mucosal function and altered dysmotility [8]. One theory is that these functional changes of the gallbladder are due to direct infection of the gallbladder itself from the hepatitis C virus, which is independent of the level of concurrent liver cirrhosis [9]. In this case, however, primary gallbladder disease was excluded and the radiological appearances seen were purely due to an acute hepatitis flare.
Our case is unusual not only because of the extreme thickening of the gallbladder wall but also because of the speed at which the gallbladder wall thickening resolved with minimal medical intervention. There are few cases reported of such marked gallbladder wall thickening in hepatitis C infection and we have not found any reports of appearances resolving this quickly [7].
Footnotes
Competing Interests: The authors have declared that no competing interests exist.
References
- 1.Van Breda Vriesman A.C., Engelbrecht M.R., Smithuis R.H.M., Puylaert J.B.C.M. Diffuse gallbladder wall thickening: differential diagnosis. Am J Roentgenol. 2007;188(2):495–501. doi: 10.2214/AJR.05.1712. [DOI] [PubMed] [Google Scholar]
- 2.Shlaer W., Leopold G., Scheible F. Sonography of the thickened gallbladder wall: a nonspecific finding. Am J Roentgenol. 1981;136(2):337–339. doi: 10.2214/ajr.136.2.337. [DOI] [PubMed] [Google Scholar]
- 3.Runner G., Corwin M., Siewert B., Eisenberg R. Gallbladder wall thickening. Am J Roentgenol. 2014;202:W1–12. doi: 10.2214/AJR.12.10386. http://www.ajronline.org/doi/pdf/10.2214/AJR.12.10386 [DOI] [PubMed] [Google Scholar]
- 4.Ralls P., Quinn M., Halls J., Boswell W. Gallbladder wall thickening: patients without intrinsic gallbladder disease. Am J Roentgenol. 1981;137(1):65–68. doi: 10.2214/ajr.137.1.65. [DOI] [PubMed] [Google Scholar]
- 5.Baik S.K., Park S.J., Kim H.S., Lee D.K., Kwon S.O. Gallbladder thickening in patients with acute hepatitis: what is the cause? Gastrointest Endosc. 2000;51(4):AB284. [Google Scholar]
- 6.Maudgal D., Wansbrough-Jones M.H., Joseph A.E. Gallbladder abnormalities in acute infectious hepatitis. Dig Dis Sci. 1984;20(3):257–260. doi: 10.1007/BF01296260. [DOI] [PubMed] [Google Scholar]
- 7.Suk K., Kim C.H., Baik S.K., Kim M.Y., Park D.H., Kim K.H. Gallbladder thickening in patients with acute hepatitis. J Clin Ultrasound. 2009;37(3):144–148. doi: 10.1002/jcu.20542. http://www.ncbi.nlm.nih.gov/pubmed/19035335 [DOI] [PubMed] [Google Scholar]
- 8.Dai C., Lin C.I., Yeh M.L., Hsieh M.H., Huang C.F., Hou N.J. Association between gallbladder stones and chronic hepatitis C: ultrasonographic survey in a hepatitis C and B hyperendemic township in Taiwan. Kaohsiung J Med Sci. 2013;29(8):430–435. doi: 10.1016/j.kjms.2012.12.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bini E., McGready J. Prevalence of gallbladder disease among persons with hepatitis C virus infection in the United States. Hepatology. 2005;41(5):1029–1036. doi: 10.1002/hep.20647. [DOI] [PubMed] [Google Scholar]