

Abstract
Objective
The purpose of this exploratory study was to validate and extend previous research on social support by identifying which dimensions of social support are most commonly exchanged on health-related social networking sites and how social network structure varies with each support dimension exchanged.
Methods
This research applies a multiple case study approach by examining two social networking sites that focus on pregnancy and prenatal health. For one month, support seeking and providing messages were content analyzed and a social network analysis examined the connections between members.
Results
The sample size consisted of 525 support-seeking messages and 1965 support-providing messages. Findings indicate that participants requested informational and emotional support more than esteem and network support, with no requests for tangible support. Findings also suggest participants substituted emotional support for informational support when they were unable to provide the information sought. The social network analysis showed that network structure varied across support dimensions, with the informational and emotional support networks having the largest number of members and greatest density and reciprocity.
Conclusions
This study suggests that online support networks are fairly effective in meeting participants’ needs. The support dimension sought was generally provided and when it was not another dimension of support may have been substituted; thus, participants may have benefitted in unintended ways. The data also suggest there may be an optimal network size to support member engagement, whereby too large of a network may facilitate diffusion of responsibility and too small a network may not facilitate enough momentum to support a well-connected community.
Keywords: social networking sites, social support, social network analysis, content analysis, social media
Introduction
While pregnancy may be a joyful experience for many women, research suggests it may also be associated with stress and anxiety.1–4 However, studies have found social support can mitigate prenatal stress and anxiety, and facilitate positive health outcomes.5–6 Moreover, while the availability of social support has traditionally been constrained to an individual’s immediate social ties, the Internet has made access to new, additional sources of social support easy and convenient for everyone with an Internet connection. Indeed, research indicates that individuals are going online to find others who share similar health issues, especially after a change in health status.7–8
In the era of social media, social networking sites have emerged as popular online platforms for individuals to find similar others and exchange social support. While research suggests that participation on health-related social networking sites can have positive outcomes,9–11 little is known about the network structure of these communities and how it is associated with the exchange of social support. Moreover, with social media becoming increasingly important in health care services, understanding their strengths and weaknesses as health promotion tools is essential.
Using content analysis and social network analysis, the current study contributes to social support research by mapping the flow of support through two pregnancy-focused social networking sites and examining the resultant support networks formed around each support dimension. This exploratory study identifies the kinds of social support most frequently requested and provided and, therefore, who is most likely to benefit from participation. Before describing the study in detail, we briefly review the literature on pregnancy, social support and social networks.
Theory and background
Pregnancy and social support
While pregnancy may elicit strong feelings of happiness in women,12 research also suggests it may be associated with anxiety and stress due to women’s concerns about their baby’s development, labor and delivery, financial matters, childcare and parenting.1–4 Traditionally, women sought social support from offline sources;13 however, studies indicate that pregnant women do not always receive the support they need from family and friends.14 This poses a risk for women because a lack of social support and prenatal stress have been associated with lower birthweight babies, preterm delivery and postpartum depression.15–20
Since the widespread diffusion of the Internet, however, new opportunities for pregnant women to pursue online sources of social support and information have emerged and research indicates that women use online sources to fulfill prenatal health information and support needs.21–23 However, rather than providing a resource for women who lack social support, research suggests that pregnant women with more offline social support are more likely to seek information online.24 While few studies have examined online social support communities and pregnancy specifically, a larger body of research has explored online social support in the context of a variety of health issues, including those that confront new parents. These studies will inform the current research, thus we describe some findings from this work below.
Online social support
While an extensive history of research has shown the positive effects social support has on health and well-being,25–32 more recent research also indicates the benefits of social support are not restricted to face-to-face contexts. Instead, the exchange of social support in online communities is also associated with positive outcomes.33–35 Social networking sites, in particular, have emerged as the latest online spaces where individuals can exchange social support about health issues. While Facebook and Twitter may be the most well-known social networking sites, there is a growing body of research examining other social networking sites that specifically focus on health issues.10,36–38 These sites differ from other online communities that offer anonymity to participants by instead encouraging users to construct an individual profile and a social network that is visible to other participants. Creating an identity is inherent in these sites and is the basis for the network structure.
Social networking sites are important new contexts to study the exchange of social support due to their widespread popularity. In the US, 62% of all adult Internet users—or nearly half (46%) of all adults—use social networking sites and 15% of social networking site users have gotten health information from these sites.8 Moreover, one in five American Internet users has gone online to find others in a similar health situation.7 Clearly, millions of people are using social networking sites and research has found that members can benefit from participation in these communities.9–11
Research on social networking sites, as a specific online context, suggests that new parents are going online in search of social support and health information, and this finding has been shown across a variety of contexts, such as low income African American mothers,39 parents in Berlin, Germany,40 and teenage mothers in Australia.41 These studies have examined the motivations and benefits of social networking site use and they suggest individuals are searching for both information and social support and that participants perceive various benefits of participation, such as feelings of social connectedness and helpful information,39–42 although for some people, participation can increase fears related to the health issue.23,40
Social support and social network theory
While the exchange of social support has evolved from face-to-face contexts to also include online contexts, so, too, has the application of long-standing social support theories. There exists an extensive history of social support research anchored in both psychological and sociological perspectives and these perspectives inform the current study. From a psychological perspective, researchers have identified how individuals’ perceptions of social support, as well as actual support received, are associated with outcomes.43–45 In this paradigm, social support can be defined as “the social resources that persons perceive to be available or that are actually provided to them by nonprofessionals in the context of both formal support groups and informal helping relationships.”44 Social support is theorized as a multi-dimensional construct whose dimensions are often referred to as the functional content of relationships because of the functions they serve, such as providing information or emotional support.46
Several typologies of social support have been created, including Cutrona and Suhr’s47 typology that has been used in previous online studies.48–51 This typology distinguishes between five dimensions of support: informational; emotional; esteem; network; and tangible. Studies of online social support have found that online communities are frequently robust sources of informational and emotional support, with mixed findings related to the other dimensions.33,50–54
While a psychological approach to social support focuses on the functional content of relationships, a sociological perspective examines how an individual’s social connections provide social support and predict health-related outcomes. In this paradigm, social network analysis provides insight into how network characteristics, such as size, density, and reciprocity, are associated with social support.55–56 Larger networks with greater density—more connections across members—and reciprocity have the potential to be more supportive and yield more health benefits than smaller networks and networks that are less dense with fewer reciprocal connections.25,56–60
Scholars have suggested that analyzing both the quality of support as well as the social network provides a richer analysis;45,61 however, few studies have combined both approaches with social network analysis. Only one study was identified in a recent literature review that applied social network analysis in an online health context to compare network characteristics of a multiplex network, reflecting all dimensions of support, and uniplex networks, in which only one dimension of support was exchanged. Chang’s48 study of an online psychosis support group in Taiwan found the multiplex network was the largest, followed by informational, network, emotion, and esteem. Network densities of the uniplex networks ranged from .007 to .03, with the esteem network having the highest density (.03) and the informational network having the lowest (.007). Moreover, Chang suggests some characteristics of these networks may be influenced by the collectivist cultural context of Taiwan; therefore, the current study provides an American counterpoint to Chang’s analyses.
Chang’s48 findings reflect previous analyses that indicate online networks are largely weak tie networks that exchange informational support.62–64 Tie strength is a network characteristic that describes the contact between individuals and several factors are associated with it including frequency of contact and reciprocity. Strong ties refer to relationships that have a greater emotional bond while weak ties refer to ties between diverse individuals with less emotional investment.65 Weak tie networks are beneficial because they provide individuals access to new information, while strong ties are more likely to link individuals who are homogenous and have access to the same information.65 Therefore, strong ties typically form a dense network with members more likely to exchange emotional support, while weak ties form a less dense network, with members more likely to exchange informational support.66
The current study validates and extends previous research by examining the functional content of supportive relationships through a social network perspective. The study examines social support on two social networking sites for pregnant women and identifies how network characteristics vary based on the dimensions of support exchanged. Moreover, the study extends research on how social media facilitate supportive relationships and therefore identifies potential benefits and weaknesses of these platforms. Based on the literature review, the study addresses the following three hypotheses and one research question:
H1: More informational support is exchanged on prenatal social networking sites than other support dimensions.
H2: Prenatal social networking sites contain more weak ties than strong ties.
- H3: The dimension of support exchanged varies as a function of tie strength:
- Weak ties exchange more informational support.
- Strong ties exchange more emotional support.
RQ1: How does the structure of the support network vary based on the dimension of support provided?
Methods
The study methodology was reviewed and approved by the Institutional Review Board (IRB). Informed consent was not required because participants were engaged in a public discussion and no personally identifiable information was collected.
Sample
A sampling frame of eight social networking sites that focused on pregnancy was identified through a key word search using Google search engine. Of these sites, two general pregnancy forums were selected for analysis, identified as Sites “A” and “B”, due to their level of member engagement, which included enough messages to provide a robust sample of approximately 300 posts per month. The sample of messages included all original posts (i.e. requests for support) and the first 10 responses for a one month period. Follow-up posts from the advice seeker, posts from the site owner/moderator(s), and solicitations were excluded from the sample.
Content analysis methodology
Pilot testing
Content analysis code sheets and a coding manual were developed based on the literature. The instruments were pilot-tested by the first author and two research assistants by coding a sub-sample of messages. These results were then compared to identify discrepancies, which were discussed and refinements were made to the code sheets and coding protocol as needed, until all disagreements were eliminated. Discrepancies were resolved by comparing how each coder interpreted and applied the coding scheme (based on previous training and the coding manual) with particular attention paid to how earlier studies48–50 also applied a similar coding scheme. Every effort was made to be consistent with earlier research and retain the validity of the social support taxonomy.
Interrater reliability
After pilot testing the instrument, only two coders participated in the remainder of the study. Interrater reliability was assessed on an independent sample of 15% of both the advice seeking and provision messages. Reliability was computed with simple percent agreement, one of the most popular coefficients of reliability,67 because of its ease of understanding and the difficulty that Cohen’s kappa and Scott’s pi have with calculating reliability when distributions are extreme (i.e. have low variance).67–71 For the seeking and providing of each dimension of support, reliability was as follows: (1) informational support, 93% and 83%; (2) emotional support, 81% and 80%; (3) esteem support, 97% and 93%; (4) relationship support, 89% and 92%; and (5) tangible support, 100% in each reliability sample.
Protocol
Two coders independently coded two weeks of messages from each site, resulting in one month of data from each site. The messages were first coded on paper code sheets and later the data were entered into electronic datasets using Qualtrics online survey software. Content analysis data were analyzed with SPSS. Each message was coded for the presence of five dimensions of social support. In addition, the screen name of each participant was also coded and later converted into a numeric identifier to facilitate the social network analysis. Descriptive statistics were conducted to identify the frequency of exchange of each support dimension and nonparametric chi-square analyses tested for significant differences among support dimensions in two sub-samples of messages that contained only one dimension of social support. Chi square analyses also tested for differences among a subsample of support provision messages that compared strong ties and weak ties, based on a variable that captured the frequency of contact between participants.
Unit of analysis
The unit of analysis included the support seeking and provision messages as well as the tie between two members (for the social network analysis).
Measures
Social support
Cutrona and Suhr’s47 typology of social support was used to code the support content of the messages. Five dimensions of social support were coded: informational; emotional; esteem; network; and tangible. This support typology was informed by studies50–51 in which network support was defined as an attempt to create structural connections, links between people, as opposed to emotional connections. Table 1 indicates the social support coding scheme for support-seeking messages. A similar scheme, though not included here, was also used for support-provision messages.
Table 1.
Coding scheme for support-seeking messages.
| Dimension | Description | Examples |
|---|---|---|
| Informational support | Requests for knowledge or information about a specific issue or situation. | Suggestions/advice: Someone to offer ideas and suggest actions (e.g. “When should I tell my boss I’m pregnant?”). Referrals: Referral to another source of information, such as a website or book (but excluding a person/network connection) (e.g. “Where can I find information about licensed daycare providers in my area?”). Situation appraisal: Someone to reassess or redefine the situation (e.g. “I’m only 30 years old and my doctor has suggested an amniocentesis. I thought these were only recommended after age 35. Why would he recommend one now?”). Teaching: Someone to explain the facts, or news about a situation or about the skills needed to deal with the situation (e.g. “What are the risks associated with an amniocentesis?”). |
| Emotional support | Problem is framed in terms of emotion and participant is seeking some kind of emotional feedback or understanding. The focus of the message will typically be about feelings, not information. |
Affection: Includes “virtual” physical contact such as sending hugs, or using emoticons. Generally this kind of support is provided, without being asked for (e.g.:  ). Sympathy: Someone to feel sorrow or regret for the support-seeker’s situation (e.g. “I wanted to tell everyone that I miscarried my baby at 9 weeks.”). Understanding/empathy: Someone to understand the situation, often through personal experience (e.g. “Am I the only one whose mother-in-law is making them crazy??!!”). Encouragement: Someone to provide the recipient with hope and confidence (e.g. “I am really scared of going through labor. I don’t think I can push this baby out.”). Prayers: Someone to pray with/for another member (e.g. “Please pray for me and my baby, that everything will be okay.”). ). Sympathy: Someone to feel sorrow or regret for the support-seeker’s situation (e.g. “I wanted to tell everyone that I miscarried my baby at 9 weeks.”). Understanding/empathy: Someone to understand the situation, often through personal experience (e.g. “Am I the only one whose mother-in-law is making them crazy??!!”). Encouragement: Someone to provide the recipient with hope and confidence (e.g. “I am really scared of going through labor. I don’t think I can push this baby out.”). Prayers: Someone to pray with/for another member (e.g. “Please pray for me and my baby, that everything will be okay.”). |
| Esteem support | Refers to regard for one’s skills, abilities, and intrinsic value. It is distinguished from emotional support because it focuses on a person’s self-perceptions rather than their emotions about something else. | Validation: Someone to express agreement with the support-seeker’s perspective on the situation (e.g. “Did I do the right thing by telling my mother-in-law that I don’t want her in the delivery room?”). Relief of blame: Someone to alleviate the support-seeker’s feelings of guilt about the situation (e.g. “I am feeling so guilty that something I did caused my miscarriage.”). Compliment (coded in the provision of support only): Saying positive things about a support-seeker (e.g. “You are so strong for handling everything the way you did.”). |
| Network support | Attempts to create structural connections with other individuals or groups. | Access: Someone to provide access to new companions, including access to another support group (e.g. “My baby tested positive for Down’s Syndrome, do you know anyone else who’s gone through this that I could talk to?”). Friendship: An explicit request to make friends and participate in the group. Also includes any exchange of personal email addresses or requests/offers to talk at a later date or in a private conversation (e.g. “I just joined this group because I’d like to make some new friends with other moms-to-be.”). Physical presence: Someone looking to meet other women in same geographic location (e.g. “Is anyone else living in the Boston area who would like to meet for coffee?”). Companions: Someone who needs to be reminded of the availability of existing companions with whom they can talk to about a problem (e.g. “I don’t think there’s anyone in my life who I can really talk to about how I’m feeling right now.”). |
| Tangible support | Requests for physical aid. | Loan: A request to lend the support-seeker something including money. Gift: A request to give the support-seeker something, including money. Direct task: A request to perform a task directly for the support-seeker (e.g. babysitting). |
Social network analysis methodology
Social network data were collected from the content analysis and included member screen names (converted into numeric identifiers), the dimensions of support sought and provided, and the frequency of contact between members. Social network data were converted from the SPSS data file and analyzed with UCINET 6.00.72
Social network measures
Network structure was assessed with the following metrics: network size (how many members in the network); mean in-degree and out-degree (average number of support messages received and given for each member); density (proportion of connections relative to the total number possible); in-degree centralization (variance of in-degree scores; a higher in-degree metric reflects a network that is highly organized around one central individual receiving the most support73), out-degree centralization (variance of out-degree scores; a higher out-degree metric reflects a network that is highly organized around one central individual providing the most support73) and reciprocity (ratio of reciprocal ties to all ties). Tie strength was assessed through frequency of support provision (how many times the same person provided support to another) and reciprocity (whether the support provision was mutual). Weak ties were identified as those wherein participants only provided support one time to another member, while strong ties are those that had three or more support provisions. Reciprocity was assessed through the reciprocal provision of support between two participants.
Results
Social support exchange
During the study period, there were 704 participants across both sites. These members posted 525 messages that contained explicit requests for support. As Figure 1 shows, across both sites, the majority of messages sought informational support (87%), followed by emotional support (49%), with network (4%) and esteem support (4%) far less in demand, and no requests for tangible support.
Figure 1.
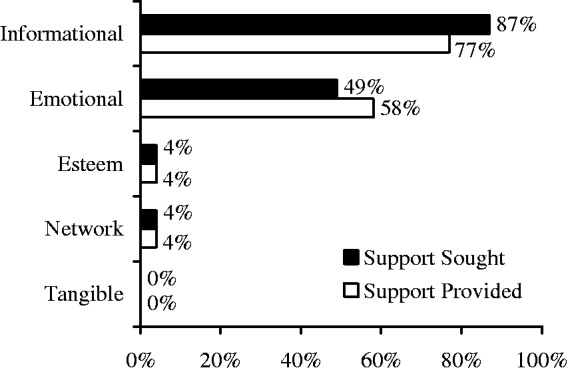
The exchange of five dimensions of social support.
In response to the support requests, 1965 messages were posted, with a mean of 3.44 and mode of 1 per original message. Similar to support requests, the majority of messages contained informational support; however, the amount of information provided did not match the demand for it. Specifically, as Figure 1 indicates, while 87% of messages sought informational support, only 77% of responses provided it. Further, 49% of messages sought emotional support while 58% of messages provided it. There was, however, an even exchange of esteem and network support and no requests or provisions of tangible support.
Nonparametric chi-square analyses tested for significant differences among the four support dimensions in two sub-samples of messages that contained only one dimension of support. As Table 2 shows, significantly more of these support-seeking messages sought informational support than emotional (227 vs. 15, χ2 (1) = 185.72, p < .001) or network support (227 vs. 27, χ2 (1) = 157.48, p < .001). Similarly, in the support-providing messages, there were significant differences in the frequency of each dimension of support provided, with informational support being provided significantly more than the other dimensions. Therefore, Hypothesis 1 was supported.
Table 2.
Non parametric chi-square analyses comparing the frequency of social support dimensions within messages that sought or provided only one dimension of support.
| Informational | Emotional | Esteem | Network | |
|---|---|---|---|---|
| Support- seeking | 227a | 15b | 0 | 27b |
| Support- providing | 654a | 253b | 3c | 68d |
Numbers in the same row with different letter superscripts are significantly different from one another at the level of at least p < .05.
Tie strength
As Figure 2 illustrates, the majority of contact (≥80%) between members was a one-time support provision. Moreover, as Table 3 indicates, these networks had low reciprocity (Site A = .07 and Site B = .006), indicating that 7% of the ties were reciprocal on Site A and less than 1% were reciprocal on Site B. Therefore, these networks were weak tie networks that primarily consisted of one-time support provision between members with low reciprocity. Thus, Hypothesis 2 was supported.
Figure 2.
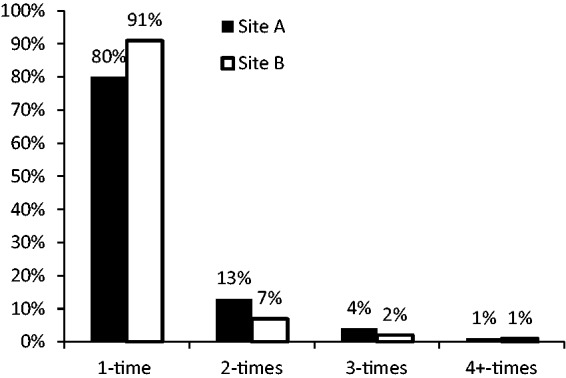
Frequency of support provision within dyads across both sites.
Table 3.
Comparison of five support networks on social networking sites A and B.
| Multiplex network |
Informational support |
Emotional support |
Esteem support |
Network support |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Site A | Site B | Site A | Site B | Site A | Site B | Site A | Site B | Site A | Site B | |
| Number of nodes | 199 | 465 | 181 | 417 | 170 | 364 | 41 | 35 | 29 | 75 |
| Mean degree | 6.14 | 1.59 | 4.65 | 1.25 | 3.45 | .98 | .41 | .07 | .12 | .13 |
| Normalized mean degree | .35 | .07 | .26 | .07 | .35 | .07 | .05 | .01 | .03 | .01 |
| Out-degree centralization | 4.84 | 1.14 | 3.80 | 1.17 | 4.52 | 1.23 | 1.22 | .42 | .48 | .35 |
| In-degree centralization | 5.97 | .80 | 4.70 | .96 | 4.83 | 1.01 | 1.72 | 1.28 | 1.75 | .35 |
| Average density | .03 | .003 | .02 | .003 | .02 | .002 | .00 | .00 | .00 | .00 |
| Reciprocity | .07 | .006 | .06 | .01 | .05 | .01 | .00 | .00 | .00 | .00 |
To test Hypothesis 3, chi square analyses compared whether weak ties were more likely to provide informational support and whether strong ties were more likely to provide emotional support. Across both social networking sites, significantly more messages between weak ties contained informational support than those that did not (Site A: 555 vs. 177, χ2 (1) = 195.20, p < .001 and Site B: 495 vs. 103, χ2 (1) = 256.96, p < .001). Analyses of strong ties, however, showed no significant difference in the frequency of messages that contained emotional support than those that did not (Site A: 112 vs. 126, χ2 (1) = .82, NS and Site B: 22 vs. 26, χ2 (1) = .33, NS). Therefore, Hypothesis 3 was only partially supported.
Social network structure
Five support networks were constructed for the two social networking sites: one multiplex network examined overall support and four uniplex networks reflected each dimension of support provided on the sites. On Site A, the multiplex network consisted of 199 people with 927 ties between them and Site B had 465 people with 659 ties between them. Table 3 reports the mean in- and out-degree, degree centralization, density, and reciprocity measures. The data show that the smaller network (Site A), in terms of number of members, was the more active network, with a mean degree of 6.14 compared to 1.59 for the larger site (Site B), indicating that, on average, each member on Site A had ties to six other members, whereas on Site B, each member connected with less than two other participants which is reflected in the density metrics of .03 for Site A and .003 for Site B. However, even the more active network, Site A, was not a very dense network, with only 3% of all possible ties being realized, while on Site B less than 1% of all possible ties had been made. Further, both sites had low reciprocity, suggesting that support only flowed one way on Site B, while on Site A there was some minimal reciprocal support provision.
Site A was more centralized on in-degree, suggesting some participants were receiving more support than others. On Site B the support networks were generally more centralized on out-degree, although not strongly. Higher measures of out-degree centralization suggest the provision of support was not evenly distributed throughout the network. However, on both sites esteem support was more centralized on in-degree indicating that a few members, in particular, received more esteem support than others. In regards to network support, Site B had the same in- and out-degree centralization measure suggesting that the network was not strongly centralized on either of these measures.
The most prominent similarity across both sites was that the support networks became less centralized and less dense as the dimension of support provided varied (Table 3). There were some key participants holding the informational support network together; however, these central figures dropped out of the network, along with many other members, with the other support dimensions, resulting in a more decentralized network. For example, Figure 3 illustrates how much larger and more dense the informational and emotional support networks are on Site A, in comparison to the esteem and network support networks. Thus, the structure of the support networks varied widely across each dimension of support exchange.
Figure 3.

Sociometric diagrams depicting four networks of support exchange on Site A.
A = informational support provision; B = emotional support provision; C = esteem support provision; D = network support provision.
Discussion
Similar to previous social support research,33,50–54,74 the current study found informational and emotional support were most in demand on pregnancy-related social networking sites. There were far fewer requests for esteem and network support, and none for tangible support. These findings are consistent with previous research that found that pregnant women rely on the Internet to find both information and social support.22,24 Moreover, the data indicate most support needs were met on the sites. Thus, these sites represent a valuable source of social support, particularly informational and emotional, for pregnant women. Findings suggest participants generally received the type of support they requested and when they did not, as in the case of informational support, emotional support was substituted instead. While studies have found contradictory impacts of unsolicited support,75–77 researchers suggest unsolicited support may be beneficial when there is a greater overall need for support.78 Thus, the provision of unsolicited emotional support, in lieu of the informational support that was sought on these sites, may be beneficial for participants because it reflects an attentive community trying to be supportive; however, future research is needed to verify this suggestion.
The findings also indicate these social networking sites were weak ties networks with infrequent repetitive contact. While this study supports previous research that weak ties are more likely to provide informational support,65 the study could not confirm that strong ties were more likely to provide emotional support. These data suggest that informational support is the backbone of online support networks and that tie strength may have different implications in an online context.
In terms of network structure, the smaller multiplex network was the more active site, indicating that, despite having more members to provide support, larger communities are not necessarily more supportive. In fact, smaller networks may facilitate more interaction among participants because members can more easily connect with a majority of the network, which becomes more difficult as network size increases79 and responsibility for support provision may diffuse across the network. The smaller multiplex network was also more centralized than the larger multiplex network, indicating that there were some very active participants at the center of Site A, while participation on Site B was more diffuse. This suggests that online communities benefit from some more active individuals, such as moderators, at the center of the network to help engage the community. From a public health perspective, there may be an opportunity for moderators to act as peer health educators,80 in which, with some training, they could provide some more qualified advice and support.
Not all small networks are well connected, though, as illustrated in the smaller uniplex networks formed on these sites. Analyses of the uniplex networks revealed that network structure changed with each dimension of social support provided. The informational and emotional support networks were more robust than the others, with the most participants, and also the greatest density and reciprocity. This suggests members feel most comfortable and willing to exchange informational and emotional support in this context. The uniplex networks with fewer members—those created around esteem and network support—were not well connected with no reciprocity and no density. Therefore, these data indicate there may be an optimal network size that is large enough to facilitate engagement among participants but not too large so responsibility for participation becomes too widely diffused across the network. Moreover, these data indicate the robustness of networks is not solely associated with their size, but also the content or function of their connections.
The current study’s findings are similar to Chang’s48 study of a Taiwanese sample in that the informational network had the largest number of participants. However, in Chang’s study network support was the second most in-demand support dimension and the emotional support network had less than half the number of participants than the informational support network. Thus, there were differences in the support networks between Chang’s study and the current one. These differences may be attributed to traditional, cultural differences related to the public display of emotion or they may reflect differences related to gender or the health issue under discussion. The current study included an all-female sample who may feel more comfortable exchanging emotional support, and/or there may be an interaction effect between the topic (pregnancy) and gender of participants that is associated with the exchange of more emotional support.
Our findings also illustrate the importance of combining content analysis with a network perspective enabling us to investigate how these support networks function. While the study found an even exchange of esteem and network support, the support networks formed around these support dimensions were not nearly as robust as the networks formed around informational and emotional support. Therefore, by combining these two methodologies researchers can learn more about both the availability of social support in an online context, as well as how the functional content of supportive relationships is associated with social network structure.
Limitations and directions for future research
This research focused on two health-related social networking sites in a US context; therefore, findings are not generalizable to the entire population of online social support networks. Thus, future research should consider a larger sample size and researchers should also consider sites that address different health issues with different populations. The current study focused on sites primarily used by American women, additional studies should examine whether there are differences among sites that are more popular with men only as well as mixed-gender sites and sites targeted for users in other cultural contexts. In addition, future research should further examine the role that cultural influences may play in online networks. The study also was grounded in Cutrona and Suhr’s47 typology of social support; therefore, the findings may change when using other support typologies.
The current study suggests several areas of inquiry for future research. More research is needed to validate the finding of support substitution, such as when emotional support was substituted for informational support, and the potential impact of such substitutions on support-recipients. More studies are also needed to examine the quality of informational support provided. Informational support was the dimension of support most frequently exchanged among members; however, more research is needed about the quality and accuracy of the informational support provided and whether members follow the advice received in this context. If members accept and act on erroneous information, this could result in serious, negative health outcomes. More research is also needed as to why there is such a high demand for informational support on these social networking sites. This high demand may suggest informational needs are not being met in a pregnant woman’s clinical relationships with her health care team. Qualitative research that directly elicits feedback from women about their experiences would also add to the literature.
Additional studies are also needed to better understand the factors that facilitate a more connected support network and to identify whether there is an “ideal” network size for the exchange of support. Prior research has suggested that larger networks have more potential resources for support provision;25,56–60 however, the current study found the largest multiplex network was not the most connected. Therefore, more research is needed to identify whether a larger network encourages a diffusion of responsibility wherein members may not participate because they think someone else will. Conversely, more research is needed to identify why the smallest uniplex support networks were not well-connected either. These data suggest that too small a network may also impede engagement. Finally, more research is needed with a larger sample to further examine the differences between the uniplex support networks. Since so few messages exchanged esteem and network support the current comparison of uniplex networks is limited.
Conclusion
The findings from this study confirm social networking sites are active forums for the exchange of informational and emotional support. The findings suggest support seekers’ needs are generally being met on these sites and when they are not—as in the case of information—another support dimension may be substituted. The findings also indicate the structure of support networks varies across individual support dimensions, such that all networks are not equally connected and robust. However, these networks are primarily weak tie networks that exchange informational support, with little reciprocity and low density. For health care practitioners, this study serves as another important reminder that patients are acquiring health care information online, which may or may not be factually accurate. Therefore, these findings suggest health care practitioners, particularly in a US context, should consider how they can better meet their patients’ needs for informational support, either offline or through their own moderated support network, so as to ensure patients are receiving accurate information and the support they need to cope with their health issues.
Acknowledgements
None
Conflict of interest
The authors declare there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
The Institutional Review Board of the University of Southern California approved this study [Approval no. UP-08-00209].
Contributorship
HH researched literature and conceived of the study. SM and TV provided feedback and study design modifications. HH gained ethical approval, collected data, and performed analyses, with feedback and direction from SM and TV. HH wrote first draft of manuscript. All authors reviewed and edited the manuscript and approved final version of the manuscript.
Guarantor
: HH
Peer Review
This manuscript was reviewed by Wendy Hall, University of British Columbia and Dianne Rodger, The University of Adelaide.
References
- 1.Dunkel-Shetter C. Maternal stress and preterm delivery. Prenatal Neonatal Med 1998; 3: 39–42. [Google Scholar]
- 2.Gurang RAR, Dunkel-Schetter C, Collins N, et al. Psychosocial predictors of prenatal anxiety. J Soc Clin Psychol 2005; 24: 497–519. [Google Scholar]
- 3.Huizink AC, Mulder EJ, Robles de Medina PG, et al. Is pregnancy anxiety a distinct disorder? Early Hum Dev 2004; 79: 81–91. [DOI] [PubMed] [Google Scholar]
- 4.Weisberg R, Paquette J. Screening and treatment of anxiety disorders in pregnant and lactating women. Women’s Health Issues 2002; 12: 32–36. [DOI] [PubMed] [Google Scholar]
- 5.Duman N, Kocak C. The effect of social support on state anxiety levels during pregnancy. Soc Behav Personal 2013; 41: 1153–1163. [Google Scholar]
- 6.Emmanuel E, St John W, Sun J. Relationship between social support and quality of life in childbearing women during the perinatal period. J Obstet Gynecol Neonatal Nurs 2012; 41: E62–E70. [DOI] [PubMed] [Google Scholar]
- 7.Fox S. Peer-to-peer healthcare: Many people—especially those living with chronic or rare diseases—use online connections to supplement professional medical advice. Report, Pew Internet and American Life Project, 28 February 2011. Available at: http://www.pewinternet.org/∼/media//Files/Reports/2011/Pew_P2PHealthcare_2011.pdf (accessed 8 December 2015).
- 8.Fox, S., The social life of health information, 2011. Report, Pew Internet and American Life Project, 12 May 2011. Available at: http://www.pewinternet.org/files/old-media//Files/Reports/2011/PIP_Social_Life_of_Health_Info.pdf (accessed 8 December 2015).
- 9.Ballantine PW, Stephenson RJ. Help me, I’m fat! Social support in online weight loss networks. J Consum Behav 2011; 10: 332–337. [Google Scholar]
- 10.Phua J. Participating in health issue-specific social networking sites to quit smoking: How does online social interconnectedness influence smoking self-efficacy? J Comm 2013; 63: 933–952. [Google Scholar]
- 11.Takahashi Y, Uchida C, Miyaki K, et al. Potential benefits and harms of a peer support social network service on the internet for people with depressive tendencies: Qualitative content analysis and social network analysis. J Med Int Res 2009; 11: e29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Malhotra R, Mudgal R, Dharmarha S, et al. How happy are pregnant women? A socio-demographic analysis. Clin Epidemiol Glob Health 2015; 3: 117–124. [Google Scholar]
- 13.Liese LH, Snowden LR, Ford LK. Partner status, social support, and psychological status during pregnancy. Fam Relat 1989; 38: 311–316. [Google Scholar]
- 14.Agostini F, Neri E, Salvatori P, et al. Antenatal depressive symptoms associated with specific life events and sources of social support among Italian women. Matern Child Health J 2015; 19: 1131–1141. [DOI] [PubMed] [Google Scholar]
- 15.Conway KS, Kennedy LF. Maternal depression and the production of infant health. South Econ J 2004; 71: 260–286. [Google Scholar]
- 16.Cronenwett LR. Network structure, social support, and psychological outcomes of pregnancy. Nurs Res 1985; 34: 93–99. [PubMed] [Google Scholar]
- 17.Dejin-Karlsson E, Hanson BS, Ostergren P, et al. Association of a lack of psychosocial resources and the risk of giving birth to small for gestational age infants: A stress hypothesis. BJOG 2000; 107: 89–100. [DOI] [PubMed] [Google Scholar]
- 18.Feldman PJ, Dunkel-Schetter C, Sandman CA, et al. Maternal social support predicts birth weight and fetal growth in human pregnancy. Psychosom Med 2000; 62: 715–725. [DOI] [PubMed] [Google Scholar]
- 19.Sable MR, Wilkinson DS. Impact of perceived stress, major life events and pregnancy attitudes on low birth weight. Fam Plann Perspect 2000; 32: 288–294. [PubMed] [Google Scholar]
- 20.Shapiro G, Fraser W, Frasch M, et al. Psychosocial stress in pregnancy and preterm birth: associations and mechanisms. J Perinat Med 2013; 41: 631–645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bernhardt JM, Felter EM. Online pediatric information seeking among mothers of young children: Results from a qualitative study using focus groups. J Med Internet Res 2004; 6: e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Da Costa D, Zelkowitz P, Bailey K, et al. Results of a needs assessment to guide the development of a website to enhance emotional wellness and healthy behaviors during pregnancy. J Perinat Educ 2015; 24: 213–224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Weston C, Anderson JL. Internet use in pregnancy. Br J Midwifery 2014; 22: 488–493. [Google Scholar]
- 24.Guillory J, Niederdeppe J, Kim H, et al. Does social support predict pregnant mothers’ information seeking behaviors on an educational website? Matern Child Health J 2014; 18: 2218–2225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Berkman LF. Assessing the physical health effects of social networks and social support. Annu Rev Public Health 1984; 5: 413–432. [DOI] [PubMed] [Google Scholar]
- 26.Berkman LF. The role of social relations in health promotion. Psychosom Med 1995; 57: 245–254. [DOI] [PubMed] [Google Scholar]
- 27.Berkman LF, Glass T. Social integration, social networks, social support, and health. In: Berkman LF, Kawachi I. (eds). Social epidemiology, New York: Oxford Press, 2000, pp. 137–173. [Google Scholar]
- 28.Cohen J. Social relationships and susceptibility to the common cold. In: Ryff CD, Singer BH. (eds). Emotion, social relationships, and health, New York: Oxford University Press, 2001, pp. 221–233. [Google Scholar]
- 29.House JS, Landis KR, Umberson D. Social relationships and health. Science 1988; 241: 540–545. [DOI] [PubMed] [Google Scholar]
- 30.Seeman TE. How do others get under our skin? Social relationships and health. In: Ryff CD, Singer BH. (eds). Emotion, social relationships, and health, New York: Oxford University Press, 2001, pp. 189–210. [Google Scholar]
- 31.Schaffer MA, Lia-Hoagberg B. Effects of social support on prenatal care and health behaviors of low-income women. J Obstet Gynecol Neonatal Nurs 1997; 26: 433–440. [DOI] [PubMed] [Google Scholar]
- 32.Spiegel D, Kimerling R. Group psychotherapy for women with breast cancer: Relationships among social support, emotional expression, and survival. In: Ryff CD, Singer BH. (eds). Emotion, social relationships, and health, New York: Oxford University Press, 2001, pp. 97–123. [Google Scholar]
- 33.Dunham PJ, Hurshman A, Litwin E, et al. Computer mediated social support: Single young mothers as a model system. Am J Community Psychol 1998; 26: 281–306. [DOI] [PubMed] [Google Scholar]
- 34.Miyata K. Social support for Japanese mothers online and offline. In: Wellman B, Haythornthwaite C. (eds). The Internet in everyday life, Malden, MA: Blackwell Publishers, 2002, pp. 520–548. [Google Scholar]
- 35.Rogers S, Chen Q. Internet community group participation: Psychosocial benefits for women with breast cancer. Jour Comp-Med Comm 2005; 10(4): article 5. DOI: DOI: 10.1111/j.1083-6101.2005.tb00269.x. [Google Scholar]
- 36.Chuang K, Yang C. Interaction patterns of nurturant support exchanged in online health social networking. J Med Internet Res 2012; 14: 371–391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Colineau N, Paris C. Talking about your health to strangers: Understanding the use of online social networks by patients. New Review of Hypermedia and Multimedia 2010; 16: 141–160. [Google Scholar]
- 38.Palmen M, Kouri P. Maternity clinic going online: Mothers’ experiences of social media and online health information for parental support in Finland. J Commun Healthc 2012; 5: 190–198. [Google Scholar]
- 39.Asiodu I, Waters C, Dailey D, et al. Breastfeeding and use of social media among first-time African American mothers. J Obstet Gynecol Neonatal Nurs 2015; 44: 268–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Gabbert T, Metze B, Bührer C, et al. Use of social networking sites by parents of very low birth weight infants: Experiences and the potential of a dedicated site. Eur J Pediatr 2013; 172: 1671–1677. [DOI] [PubMed] [Google Scholar]
- 41.Nolan S, Hendricks J, Towell A. Social networking sites (SNS); exploring their uses and associated value for adolescent mothers in Western Australia in terms of social support provision and building social capital. Midwifery 2015; 31: 912–919. [DOI] [PubMed] [Google Scholar]
- 42.Antheunis M, Tates K, Nieboer T. Patients’ and health professionals’ use of social media in health care: Motives, barriers and expectations. Patient Educ Couns 2013; 92: 426–431. [DOI] [PubMed] [Google Scholar]
- 43.House JS, Kahn RL, McLeod JD, et al. Measures and concepts of social support. In: Cohen S, Syme SL. (eds). Social support and health, Orlando, FL: Academic Press, Inc, 1985, pp. 83–108. [Google Scholar]
- 44.Cohen J, Gottlieb BH, Underwood LG. Social relationships and health. In: Cohen S, Underwood LG, Gottlieb BH. (eds). Social support measurement and intervention: A guide for health and social scientists, New York: Oxford University Press, 2000, pp. 3–25. [Google Scholar]
- 45.Barrera M., Jr Distinctions between social support concepts, measures, and models. Am J Community Psychol 1986; 14: 413–445. [Google Scholar]
- 46.Uchino BN. Social support and physical health, New Haven: Yale University Press, 2004. [Google Scholar]
- 47.Cutrona CE, Suhr JA. Controllability of stressful events and satisfaction with spouse support behaviors. Comm Res 1992; 19: 154–174. [Google Scholar]
- 48.Chang HJ. Online supportive interactions: Using a network approach to examine communication patterns within a psychosis social support group in Taiwan. J Am Soc Inf Sci Technol 2009; 60: 1504–1518. [Google Scholar]
- 49.Coulson NS. Receiving social support online: An analysis of a computer-mediated group for individuals living with irritable bowel syndrome. Cyberpsychol Behav 2005; 8: 580–584. [DOI] [PubMed] [Google Scholar]
- 50.Coulson NS, Greenwood N. Families affected by childhood cancer: an analysis of the provision of social support within online support groups. Child Care Health Dev 2011; 38: 870–877. [DOI] [PubMed] [Google Scholar]
- 51.Braithwaite DO, Waldron VR, Finn J. Communication of social support in computer-mediated groups for people with disabilities. Health Comm 1999; 11: 123–151. [DOI] [PubMed] [Google Scholar]
- 52.Cousineau TM, Rancourt D, Green TC. Web chatter before and after the Women’s Health Initiative results: A content analysis of on-line menopause message boards. J Health Comm 2006; 11: 133–147. [DOI] [PubMed] [Google Scholar]
- 53.Gray J. Feeding on the web: Online social support in the breastfeeding context. Commun Res Rep 2013; 30: 1–11. [Google Scholar]
- 54.Loane S, D’Alessandro S. Communication that changes lives: Social support within an online health community for ALS. Commun Q 2013; 61: 236–251. [Google Scholar]
- 55.House JS, Kahn RL. Measures and concepts of social support. In: Cohen S, Syme SL. (eds). Social support and health, San Francisco: Academic Press, 1985, pp. 83–108. [Google Scholar]
- 56.Achat H, Kawachi I, Levine S, et al. Social networks, stress and health-related quality of life. Qual Life Res 1998; 8: 735–750. [DOI] [PubMed] [Google Scholar]
- 57.Benson P. Network characteristics, perceived social support, and psychological adjustment in mothers of children with autism spectrum disorder. J Autism Dev Disord 2012; 42: 2597–2610. [DOI] [PubMed] [Google Scholar]
- 58.Heaney CA and Israel BA. Social networks and social support. In: Glanz K, Rimer BK and Lewis FM (eds) Health Behavior and Health Education. San Francisco, CA: Jossey-Bass, 2002, pp.185--209.
- 59.Luke DA, Harris JK. Network analysis in public health: History, methods, and applications. Annu Rev Public Health 2007; 28: 69–93. [DOI] [PubMed] [Google Scholar]
- 60.Wellman B, Wortley S. Different strokes from different folks: Community ties and social support. Am J Sociol 1990; 96: 558–588. [Google Scholar]
- 61.Stansfeld SA. Social support and social cohesion. In: Marmot M, Wilkinson R. (eds). Social determinants of health, Oxford: Oxford University Press, 2006, pp. 148–171. [Google Scholar]
- 62.Walther JB, Boyd S. Attraction to computer-mediated support. In: Lin CA, Atkin DJ. (eds). Communication and society: Audience adoption and uses, Cresskill, NJ: Hampton Press, 2002, pp. 153–188. [Google Scholar]
- 63.Wellman B and Gulia M. Virtual communities as communities: Net surfers don't ride alone. In: Smith MA and Kollock P (eds) Communities in cyberspace. London: Routledge, 1999, pp. 167--194.
- 64.Wright KB, Bell SB. Health-related support groups on the internet: Linking empirical findings to social support and computer-mediated communication theory. J Health Psychol 2003; 8: 39–54. [DOI] [PubMed] [Google Scholar]
- 65.Granovetter M. The strength of weak ties. Am J Sociol 1973; 78: 1360. [Google Scholar]
- 66.Granovetter M. The strength of weak ties: A network theory revisited. Soc Theory 1983; 1: 201. [Google Scholar]
- 67.Neuendorf KA. The content analysis guidebook, Thousand Oaks, CA: Sage Publications, 2002. [Google Scholar]
- 68.Feinstein AR, Cicchetti DV. High agreement but low kappa: The problems of two paradoxes. J Clin Epidemiol 1990; 43: 543–549. [DOI] [PubMed] [Google Scholar]
- 69.Perreault WD, Jr, Leigh LE. Reliability of nominal data based on qualitative judgments. J Mark Res 1989; 26: 135–148. [Google Scholar]
- 70.Potter WJ, Levine-Donnestein D. Rethinking validity and reliability in content analysis. J Appl Commun Res 1999; 27: 258–284. [Google Scholar]
- 71.Viera AJ, Garrett JM. Understanding interobserver agreement: The Kappa statistic. Fam Med 2005; 37: 360–363. [PubMed] [Google Scholar]
- 72.Borgatti SP, Everett MG, Freeman LC. Ucinet 6 for Windows: Software for social network analysis, Harvard, MA: Analytic Technologies, 2002. [Google Scholar]
- 73.Freeman LC. Centrality in social networks: I. Conceptual clarification. Social Networks 1979; 1: 215–239. [Google Scholar]
- 74.Finn J. An exploration of helping processes in an online self-help group focusing on issues of disability. Health Soc Work 1999; 24: 220–231. [DOI] [PubMed] [Google Scholar]
- 75.Bolger N, Amarel D. Effects of social support visibility on adjustment to stress: Experimental evidence. J Pers Soc Psychol 2007; 92: 458–475. [DOI] [PubMed] [Google Scholar]
- 76.Deelstra J, Peeters M, Wilmar BS, et al. Receiving instrumental support at work: When help is not welcome. J Appl Psychol 2003; 88: 324–331. [DOI] [PubMed] [Google Scholar]
- 77.Thoits P. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav 2011; 52: 145–161. [DOI] [PubMed] [Google Scholar]
- 78.Song L, Chen W. Does receiving unsolicited support help or hurt? Receipt of unsolicited job leads and depression. J Health Soc Behav 2014; 55: 144–160. [DOI] [PubMed] [Google Scholar]
- 79.Borgatti SP, Everett MG, Johnson JC. Analyzing social networks, Los Angeles: Sage, 2013, pp. 149–162. [Google Scholar]
- 80.Young S. Analysis of online social networking peer health educators. Stud Health Technol Inform 2012; 181, 253--259. [PubMed]