

Abstract
Objective
The need to consider gender when studying exercise in eating disorder (ED) has been underscored. The study aimed to test the psychometric properties and factor structure of the exercise and eating disorder (EED) questionnaire for males with and without ED, to highlight gender differences, and to explore issues relevant for a male version of the EED questionnaire.
Method
This cross sectional study included 258 male participants: 55 ED patients (inpatients and outpatients) and 203 student controls. The patient group consisted of 54.5% (n = 30) with AN, 18.2% (n = 10) with BN, 27.2% (n = 15) with unspecified ED. The ED sample was treated as transdiagnostic in all analyses. t Tests, chi‐square test, correlations analyses, and a principal component analysis were conducted.
Results
The analyses confirmed that the EED questionnaire had adequate psychometric properties, and a four‐factor solution: (a) compulsive exercise, (b) positive and healthy exercise, (c) awareness of bodily signals, and (d) weight and shape exercise. The questionnaire discriminated significantly (p < .01– < .001) between patients and controls on the global score, subscales, and 16 out of 18 individual items. Convergent validity was demonstrated by high correlations between the EED questionnaire and the eating disorder examination questionnaire (r = .65).
Discussion
The results indicated that the EED questionnaire is a valid and reliable tool for males. It is a clinically derived, self‐report questionnaire to assess compulsive exercise among ED patients, regarding attitudes and thoughts toward compulsive exercise and identification of treatment targets and priorities
Keywords: compulsive exercise, eating disorders, gender differences, males, questionnaire
1. INTRODUCTION
There is consensus that unhealthy exercise is a common trait in persons with eating disorders (EDs). Research findings have generally indicated the nature of exercise in EDs as more compulsive than addictive (Cunningham, Pearman, & Brewerton, 2016), and it has been suggested that the term compulsive exercise is a more appropriate description of the complexity among patients than other terms (Adkins & Keel, 2005; Meyer & Taranis, 2011; Noetel, Dawson, Hay, & Touyz, 2017). Additionally, clinicians and researchers have underscored the need to consider gender when studying exercise in EDs (Murray, Griffiths, Rieger, & Touyz, 2013; Stanford & Lemberg, 2012; Strother, Lemberg, Stanford, & Turberville, 2012).
EDs are less common among men than among women (Duncan, Ziobrowski, & Nicol, 2017; Preti et al., 2009), but prevalence estimates remain uncertain (Dahlgren & Wisting, 2016; Raevuori et al., 2009). One important limitation is that most assessment instruments are based on observations of EDs in women, which may not necessarily recognize specific men's issues (Raevuori, Keski‐Rahkonen, & Hoek, 2014; Stanford & Lemberg, 2012). Gender differences regarding body image challenges among ED patients have been suggested as an important factor. The body ideal of an athletic, lean, and muscular body held among men, in contrast to the drive for thinness commonly found among women, and that men more often than women choose exercise as a method to achieve the male body ideal (Furnham, Badmin, & Sneade, 2002; Stanford, & Lemberg, 2012). Reported prevalence data of compulsive exercise among men with ED are scarce, but in one study it has been estimated as 56% (Weltzin et al., 2012). In this situation, it has been emphasized that men with EDs may be at risk of being overlooked, misunderstood, and underdiagnosed (Strother et al., 2012). Validation of ED measures in men is therefore important (Raevuori et al., 2014), and the inclusion of specific items has been suggested as one way to increase the utility of measures (Darcy et al., 2012).
Self‐report questionnaires are frequently used to assess different aspects of exercise. Commonly, the questionnaires focus on unhealthy exercise in general, and do not target the specific challenges of compulsive exercise in ED patients (Cash, Novy, & Grant, 1994; Hausenblas & Downs, 2010; Ogden, Veale, & Summers, 1997; Steffen & Brehm, 1999). The exercise and eating disorder (EED) questionnaire is a clinically derived measurement tool that was developed in our ED unit to assess attitudes and thoughts toward compulsive exercise among ED patients. It includes a section for self‐reported amount of exercise. The EED questionnaire is meant for use in clinical settings and for identifying treatment targets and priorities (Danielsen, Bjornelv, & Ro, 2015; Danielsen, Bratberg, & Ro, 2012). It has been validated in female ED patients and shown good psychometric properties (Danielsen et al., 2015). Other questionnaires that have been tested in clinical ED samples are the commitment to exercise scale (CES) (Davis et al., 1995; Zeeck et al., 2017) and the compulsive exercise test (CET) (Meyer et al., 2016; Taranis, Touyz, & Meyer, 2011). Neither of these instruments has been validated in male ED patients.
The aims of our study were
-
Validation of the EED questionnaire in males
To investigate the psychometric properties of the EED questionnaire in a clinical ED sample of males compared with male controls.
To investigate the factor structure of the EED questionnaire in males.
To compare the self‐reported amount of exercise in males with EDs and in controls.
-
Gender differences
To compare EED scales in male and female ED participants.
To explore additional motives for exercise in male and female controls.
2. METHOD
2.1. Participants and procedure
The validation of the EED questionnaire was based on cross sectional data from male ED participants and male student controls from the general population (Sample 1). To elucidate gender differences, we used data from our previous EED validation study, which included female ED patients and female student controls (Danielsen et al., 2015). The different samples included in our study are presented in Figure 1, and the age and body mass index (BMI) of the investigated samples are listed in Table 1.
Figure 1.
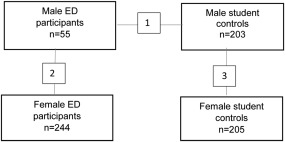
Investigated samples in the study. Sample 1: Validation of EED and comparisons of amount of exercise in males. Sample 2: Gender differences of the EED in a clinical sample. Sample 3: Gender differences in motives of exercise in a nonclinical sample
Table 1.
Age and BMI in groups and differences in Samples 1, 2, and 3
| Male ED (n = 55) | Male controls (n = 203) | Female ED (n = 244) | Female controls (n = 205) | Difference malesa | Difference male and female EDᵇ | Difference male and female controlsᶜ | |
|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) |
t (256) p‐value |
t (297) p‐value |
t (406) p‐value |
|
| Age (years) | 29.8 (10.8) | 23.0 (7.3) | 27.1 (9.5) | 21.4 (6.3) | 4.39 | 1.85 | 2.40 |
| Range | 17.6–63.2 | 16.0–53.0 | 16.0–59.0 | 16.0–59.0 | <.001 | .07 NS | <.05 |
| n = 55 | n = 191 | n = 244 | n = 203 | t(244) | t(295) | t(390) | |
| BMI | 22.1 (9.6) | 24.4 (3.8) | 22.4 (9.4) | 23.6 (3.6) | 1.72 | .22 | 2.22 |
| Range | 9.3–59.6 | 17.0–38.4 | 8.7–62.1 | 17.3–37.6 | .09 NS | .82 NS | <.05 |
Note. NS = not significant. Reduced n is due to missing BMI data in individuals in male and female student control groups. Independent t test between
Sample 1: male ED participants and male student controls. bSample 2: male and female ED participants. cSample 3: male and female student controls.
2.2. Male ED participants
The sample consisted of 55 male ED participants who were inpatients and outpatients in the period January 2005 to December 2017. They were recruited from nine specialist eating disorder units in Norway. Diagnostic evaluation was based on clinical interviews and assessment according to the International Classification of Disease (ICD‐10), and was performed by licensed specialists in psychology and psychiatry. All included patients met the criteria in the ED section of ICD‐10, F50.0 to F50.9, with the following diagnostic distribution: 54.5% (n = 30) anorexia nervosa patients (AN F50.0 and atypical AN F50.1), 18.2% (n = 10) bulimia nervosa (BN F50.2 and atypical BN F50.3), and 27.2% (n = 15) with an unspecified ED diagnosis F50.4‐F50.9 (including binge eating). Due to the limited numbers in the diagnostic groups, the sample was treated as transdiagnostic in all analyses.
2.3. Male student controls
Of the 214 male students invited to participate, 203 (95%) were included. A total of 11 students were excluded: five reported having an ED, five reported EDE‐Q global scores within the clinical range (three with scores just below 4.0, and two others above), and one was excluded due to incomplete data. The majority (n = 171) of the 203 controls were recruited in 2013 and 2014. The data collection procedure, participants, and representativeness are described in a previous paper (Danielsen et al., 2015). Following the same collecting procedures, 32 male students were recruited in 2017.
2.4. Female ED participants and female student controls
The sample in the female validation study consisted of 244 female ED participants (inpatients and outpatients) and 205 female student controls. Details of this sample are described in the female EED validation paper (Danielsen et al., 2015).
To elucidate gender differences in persons with EDs, comparative analyses were performed in two different samples: a clinical sample and a nonclinical sample. In the clinical sample (Sample 2), EED global scores and subscale scores were compared between male and female ED participants. Three additional items related to motives for exercise were compared in a nonclinical sample consisting of the male and female controls (Sample 3).
The study was approved by the Data Access Committee of Nord‐Trøndelag Hospital Trust, and REC Central, the Regional Committee for Medical and Health Research Ethics. Before inclusion, all participants gave their consent to participate, in accordance with REC guidelines.
2.5. The exercise and eating disorder questionnaire
The exercise and eating disorder questionnaire (EED) questionnaire is a short questionnaire with 18 items on a 6‐point response scale (0–5) and higher scores indicate increased severity of symptoms. The questionnaire yields clinically relevant information about attitudes toward compulsive exercise in EDs. The EED questionnaire has been validated in females and shown good psychometric properties, and a four‐factor structure (Danielsen et al., 2015). Significant discriminant validity between patients and controls, satisfactory test–retest stability, convergent validity between EED scales and ED pathology, and good internal consistency with Cronbach's alpha coefficients ranging from 0.80 to 0.93 (global score and subscales) were found. The subscales cover four dimensions: (a) compulsive exercise, (b) positive and healthy exercise, (c) awareness of bodily signals, and (d) exercise for weight and shape reasons (Danielsen et al., 2015). To assist in clinical work, a clinical severity scale based on EED global scores in female ED patients was estimated. This scale should be interpreted as a continuum. In a followup study, EED questionnaire scores were found as predictors of improvement in ED psychopathology (Danielsen, Ro, Romild, & Bjornelv, 2016). Cronbach's alpha coefficients for the study relating to males are listed in the result section.
The EED questionnaire has been developed mainly based on observations of female ED patients. To extend the utility of the questionnaire in males, three additional items were included for its use on control groups: (a) I am physically active to become strong, (b) I am physically active to get big muscles, and (c) I am physically active to get big. The content of these items is based on clinical experience of male ED patients and of published literature. Especially the two first elements have been highlighted as male‐specific (e.g., Furnham et al., 2002; Raevuori et al., 2014; Stanford & Lemberg, 2012).
In addition to the 18 EED questionnaire items, one section for the self‐reported amount of exercise (frequency, intensity, and duration) is included in the questionnaire. These questions were previously used in a longitudinal population health study in Norway, the HUNT study (Kurtze, Rangul, Hustvedt, & Flanders, 2008). They have been validated against objective measures (maximal oxygen consumption, ActiReg), and the International Physical Activity Questionnaire, and indicated as a relevant measure of leisure‐time exercise for men (Kurtze et al., 2008). Each exercise item has several response categories. Frequency of exercise has five response alternatives, ranging from “never” to “almost every day”. Intensity has three alternatives, ranging from “I take it easy without breaking into a sweat or losing my breath” to “I push myself to near exhaustion” and duration has four alternatives, ranging from “<15 minutes” to “more than one hour”. In the study, the responses were dichotomized into low‐level and high‐level exercise categories. High‐level exercise was defined as the most strenuous response alternative (shown in italics above), while the low‐level category covered the other alternatives. The categories were compared between male ED participants and male controls.
2.6. The eating disorder examination questionnaire 6.0
The eating disorder examination questionnaire (EDE‐Q) is based on the eating disorder examination interview (Fairburn & Beglin, 2008). It covers core ED attitudes and behavior over the past 28 days. The response scale has seven alternatives (0–6), and higher scores indicate higher severity levels. The EDE‐Q consists of four subscales: (a) dietary restraint, (b) weight concern, (c) shape concern, and (d) eating concern. EDE‐Q norms have been established for males in Norway (Dahlgren, Stedal, & Ro, 2017; Reas, Overas, & Ro, 2012). In our study, the EDE‐Q Global score served two purposes: first, it was used as a screening instrument for male controls; and second, it was used to investigate convergent validity. Cronbach's alpha coefficients for the EDE‐Q global score were: 0.95 (male sample), 0.93 (male ED participants), and 0.89 (male controls).
2.7. Statistical analyses
Independent t tests and χ2 tests were performed to test group differences. In some of the analyses, the Levene's test of homogeneity of variances was statistically significant, and thus unequal variances were assumed. ANCOVA was performed to investigate the possible influence of age and BMI in comparative analyses of the EED questionnaire. Convergent validity was estimated by Pearson's correlation factor. A principal component analysis (PCA) was conducted to investigate the factor structure of the EED questionnaire in the whole male sample, in the same way as in the female validation study (Danielsen et al., 2015), but not in groups, due to low numbers of male ED participants. This included the Kaiser–Meyer–Olkin (KMO) measure of sampling adequacy, a correlation matrix, and two criteria for retaining factors (Kaiser's criterion and scree plot). Due to expected correlation between factors, an oblique rotation (direct oblim) was chosen (Field, 2009). Effect sizes were calculated and reported in the relevant analyses, and Cronbach's alpha coefficients represented the degree of internal consistency of the scales. Post hoc power analyses were performed based on mean differences of the EED Questionnaire scores between male ED patients and male controls. Comparisons of the global score and the compulsive exercise subscale score were considered the most important comparisons. With the given sample sizes, the estimates of mean scores of the controls (Table 2) and assumed standard deviations (SD) of difference in means of 0.9 and 1.5. Our method had 80% power to detect mean differences of 0.38 for the global score and 0.64 for the compulsive exercise score. We assumed that a minimum clinical relevant effect would be above these estimates. The data were analyzed using SPSS version 24, and results for the whole male sample and subgroups are presented below. Acceptable levels of reported values were set at p < .05 for two‐tailed significance, 0.40 for factor loading, and values above > 0.70 as the criterion for acceptable internal consistency.
Table 2.
Differences in EED questionnaire scores (items, subscales and global scores) in male ED participants versus male student controls
| Items, subscales, and global score |
Patients (n = 55) Mean (SD) |
Controls (n = 203) Mean (SD) |
t(256) p‐value |
Diffa (95% CI) | Effect size Cohens d | Diffb adjusted for age and BMI (95% CI) |
|---|---|---|---|---|---|---|
| Compulsive exercise | ||||||
| I am physically active to avoid dealing with negative emotions | 1.89 (1.50) | 0.69 (0.95) | 5.62*** | 1.20 (0.77; 1.62) | 0.92 | 1.32 (0.96; 1.69) |
| It feels wrong if I can't be active every day | 1.89 (1.96) | 0.87 (1.02) | 3.72*** | 1.02 (0.47; 1.57) | 0.65 | 1.08 (0.65; 1.51) |
| If I haven't been physically active, I don't eat | 1.20 (1.34) | 0.17 (0.56) | 5.46*** | 1.03 (0.65.; 1.40) | 1.00 | 1.03 (0.74; 1.32) |
| If I haven't been physically active, I can't relax | 1.75 (1.65) | 0.48 (0.85) | 5.51*** | 1.27 (0.81; 1.73) | 0.97 | 1.19 (0.81; 1.57) |
| If I haven't been physically active, I get a bad conscience | 2.56 (1.71) | 1.14 (1.34) | 5.85*** | 1.43 (0.94; 1.91) | 0.92 | 1.50 (1.06; 1.93) |
| If I haven't been physically active, my body feels big | 1.95 (1.77) | 0.57 (0.92) | 5.56 *** | 1.37 (0.88; 1.87) | 0.98 | 1.46 (1.05; 1.86) |
| If I haven't been physically active, my body feels disgusting | 2.02 (1.72) | 0.60 (0.91) | 5.90*** | 1.42 (0.94; 1.90) | 1.03 | 1.50 (1.11; 1.90) |
| Factor 1, mean score | 1.89 (1.45) | 0.65 (0.64) | 6.20*** | 1.23 (0.84; 1.65) | 1.11 | 1.30 (0.99; 1.61) |
| Awareness of bodily signals | ||||||
| I notice when I get tired | 1.29 (1.13) | 1.25 (1.39) | .22 NS | 0.05 (−0.36; .45) | 0.03 | 0.03 (−0.41; 0.47) |
| I notice when I get thirsty | 1.55 (1.39) | 0.97 (1.23) | 2.79** | 0.58 (0.17; .99) | 0.44 | 0.67 (0.25; 1.10) |
| I notice when I get hungry | 2.04 (1.44) | 0.94 (1.26) | 5.13*** | 1.10 (0.67; 1.52) | 0.81 | 1.15 (0.71; 1.58) |
| I notice when I feel fit/in shape | 1.82 (1.36) | 0.97 (1.20) | 4.22*** | 0.85 (0.45; 1.23) | 0.66 | 0.95 (0.54; 1.36) |
| I listen to my body | 2.60 (1.31) | 1.51 (1.22) | 5.75*** | 1.09 (0.72; 1.46) | 0.86 | 1.23 (0.73; 1.52) |
| Factor 2, mean score | 1.77 (0.94) | 1.13 (1.08) | 3.99*** | 0.64 (0.32; .96) | 0.63 | 0.69 (0.35; 1.04) |
| Positive and healthy exercise | ||||||
| I enjoy being physically active | 2.07 (1.69) | 1.48 (1.50) | 2.35* | 0.59 (0.09; 1.09) | 0.37 | 0.23 (−0.29; 0.75) |
| I like to exercise with other people | 2.49 (1.62) | 1.56 (1.36) | 3.90*** | 0.93 (0.46; 1.40) | 0.62 | 0.69 (0.20; 1.18) |
| I am physically active to be healthy | 2.25 (1.59) | 1.64 (1.47) | 2.71** | 0.61 (0.17; 1.06) | 0.40 | 0.46 (−0.05; .96) |
| Factor 3, mean score | 2.27 (1.40) | 1.56 (1.30) | 3.53*** | 0.71 (0.31; 1.11) | 0.53 | 0.46 (0.01; .91) |
| Weight and shape exercise | ||||||
| I am physically active to become thin | 2.02 (1.90) | 1.06 (1.20) | 3.56** | 0.96 (0.42; 1.50) | 0.60 | 1.12 (0.67; 1.56) |
| I am physically active to burn calories I've eaten | 2.09 (1.87) | 0.79 (1.01) | 4.96*** | 1.30 (0.76; 1.82) | 0.87 | 1.40 (0.98; 1.83) |
| I am physically active for appearance reasons | 2.36 (1.79) | 1.98 (1.55) | 1.47 NS | 0.39 (−0.14; .92) | 0.23 | 0.71 (0.19; 1.24) |
| Factor 4, mean score | 2.16 (1.61) | 1.28 (0.94) | 3.88*** | 0.88 (0.43: 1.34) | 0.67 | 1.08 (0.70; 1.46) |
| Global score | 2.00 (0.76) | 1.16 (0.51) | 7.79*** | 0.84 (0.63; 1.06) | 1.30 | 0.86 (0.67; 1.04) |
Note. t Tests for independent samples, two tailed. Cohens d: Small effect size = 0.2, medium = 0.5, and large = 0.8.
Diff: Mean differences in EED scores between patients and controls, 95% CI: 95% confidence intervals. bDiff: Mean differences in EED scores between patients and controls adjusted for age and BMI.
*p < .05, **p < .01, ***p < .001.
2.8. Missing data
The percent of missing EED and EDE‐Q scores data in the whole male sample was 0.92%. Four male ED participants and three male controls did not complete the EDE‐Q. Single missing items were replaced for each person by a calculated mean on the actual subscale. However, in five male student controls, three to six items were missing in one subscale and could not be replaced. Body mass index (BMI) could not be calculated in 12 male controls due to lack of reported weight and height. Three male ED participants did not report the frequency of their exercise, and six did not report exercise intensity or duration. The corresponding missing data among male student controls was one (frequency), four (intensity), and five (duration). Differences in sample size due to missing data are reported in text and listed in the Tables.
3. RESULTS
3.1. Psychometric properties of the EED questionnaire in males (Sample 1)
The results of analyses showed that the EED questionnaire discriminated significantly (p < .01–.001) between male ED participants and male student controls in global scores, subscales, and 16 out of 18 items. Calculated effect sizes (Cohen's d) ranged from moderate to high, indicating a satisfactory magnitude of group differences. The mean scores (SD), mean differences, and 95% confidence intervals (CIs) in males are presented in Table 2. Among male the ED participants, a significant correlation was found between EED questionnaire global score and BMI r = .29, p < .05, but not regarding age. No significant correlation was found between global score and either age or BMI among male student controls. The EED questionnaire subscales were based on the PCA analyses that are presented in the section “Factor structure of the EED Questionnaire”.
3.2. Convergent validity between EED questionnaire scores and EDE‐Q global score (Sample1)
Correlations between the EED Questionnaire (global score and subscales) and the EDE‐Q global score indicated convergent validity. The correlation coefficients and significance levels are presented in Table 3. The strongest association with ED pathology was found in EED subscales representing the compulsive elements of exercise and exercise for weight and shape reasons. In these groups, the associations were stronger among patients than controls.
Table 3.
Correlation between EED questionnaire scores and EDE‐Q global score in males
| EED | |||||
|---|---|---|---|---|---|
| EDE‐Q global score | Global score | Compulsive | Positive & healthy | Bodily signals | Weight & shape |
| Whole male sample (n = 251)a | 0.66** | 0.65** | 0.13 | 0.24** | 0.61** |
| Male ED participants (n = 51)a | 0.65** | 0.67** | −0.07 | 0.17 | 0.65** |
| Male student control (n = 200)a | 0.35** | 0.39** | −0.02 | 0.10 | 0.54** |
Note. EED = Exercise and eating disorders questionnaire; EDE‐Q = eating disorder examination‐questionnaire.
Reduced n is due to missing EDE‐Q data.
**Correlation significant at the 0.01 level.
3.3. Factor structure of the EED questionnaire in males and principal component analysis (Sample 1)
Sample size and tests confirmed the adequate values for performing a principal component analysis (PCA) for the total male sample (Field, 2009). The KMO measure verified sampling adequacy (MSA = 0.89) and Bartlett's test of sphericity, X 2(153) 3087.564, p < .001, indicated satisfactory large correlations between items. The number of male ED participants was too low to perform a separate PCA in the patient group. Based on the two criteria for retaining factors (Kaiser's criterion and scree plot), both a three‐factor and four‐factor solution were considered. The analysis showed three factors with an eigenvalue above 1.0, explaining 67.6% of the variance. The inflexion point of the scree plot indicated the relevance of a four‐factor structure. The eigenvalue of the fourth factor was 0.97, and the explained variance increased to 73%. The different solutions were evaluated from a statistical and a clinical perspective, and the four‐factor solution was chosen. The factor loadings, explained variance, and scale reliability are listed in Table 4. All items, except one, showed a positive factor loading above 0.4. The item, “I am physically active for appearance reasons” had a factor loading in the fourth factor of 0.33. This factor also showed a negative loading of 0.44 in the third factor. However, for reasons of clinical relevance, corresponding results to the female validation study (Danielsen et al., 2015), and a positive loading value close to 0.4 (Field, 2009), the item was retained in the fourth factor: “exercise for weight and shape reasons”.
Table 4.
PCA of the EED questionnaire for the whole sample (n = 258)
| Rotated factor loading | ||||
|---|---|---|---|---|
| Factors and items | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
| Factor 1: Compulsive exercise | ||||
| If I haven't been physically active, I can't relax | 0.93 | 0.01 | 0.05 | −0.11 |
| If I haven't been physically active, I get a bad conscience | 0.87 | 0.01 | −0.09 | −0.02 |
| It feels wrong if I can't be active every day | 0.81 | 0.04 | −0.21 | −0.11 |
| If I haven't been physically active, my body feels disgusting | 0.80 | −0.04 | 0.01 | 0.14 |
| If I haven't been physically active, I don't eat | 0.79 | 0.02 | 0.09 | 0.11 |
| If I haven't been physically active, my body feels big | 0.64 | −0.03 | 0.09 | 0.33 |
| I am physically active to avoid dealing with negative emotions | 0.61 | −0.02 | −0.04 | 0.24 |
| Factor 2: Awareness of bodily signals | ||||
| I notice when I am thirsty | −0.02 | 0.93 | −0.03 | −0.04 |
| I notice when I am hungry | 0.04 | 0.87 | 0.08 | −0.04 |
| I notice when I feel fit/in shape | 0.08 | 0.86 | 0.09 | −0.09 |
| I notice when I get tired | −0.18 | 0.81 | −0.16 | 0.12 |
| I listen to my body | 0.26 | 0.59 | 0.27 | 0.13 |
| Factor 3: Positive and healthy exercise | ||||
| I enjoy being physically active | −0.10 | −0.05 | 0.92 | 0.09 |
| I like to exercise with other people | 0.04 | 0.02 | 0.87 | 0.03 |
| I am physically active to be healthy | 0.01 | 0.07 | 0.85 | −0.08 |
| Factor 4: Weight and shape related exercise | ||||
| I am physically active to become thin | −0.04 | 0.03 | −0.02 | 0.94 |
| I am physically active to burn calories I have eaten | 0.24 | 0.05 | 0.03 | 0.71 |
| I am physically active for appearance reasons | 0.21 | −0.04 | −0.44 | 0.33 |
| Eigenvalue | 6.27 | 4.02 | 1.89 | 0.97 |
| % of variance | 34.81 | 22.33 | 10.46 | 5.39 |
| Cronbach's alpha | 0.92 | 0.89 | 0.88 | 0.72 |
Note. Factor loadings above 0.4 are marked in bold.
3.4. Self‐reported amount of exercise in male ED participants and male student controls (Sample 1)
The analyses showed no significant difference between male ED participants and male student controls regarding defined high‐level and low‐level exercise in terms of frequency, intensity and duration. The results were respectively: frequency of exercise x 2(1) = 1.58 p < .21, intensity of exercise x 2(1) = 0.02, p < .90, and duration of exercise x 2(1) = 0.59 p < .44. These differences were not affected when adjusted for age and BMI. Figure 2 shows the dichotomized categories of low‐level and high‐level exercise in groups of male ED participants and males controls.
Figure 2.
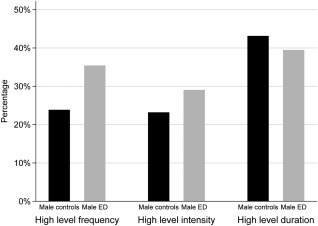
Self‐reported frequency, intensity and duration of exercise of high‐level exercise in male ED participants and male controls adjusted for age and BMI. Percent of participants in groups
Correlation analyses between EED questionnaire global score and self‐reported amount of activity among male ED participants showed a significant positive correlation related to intensity of exercise (r = .34, p < .05). In contrast to male controls, for whom negative significant correlations were found between EED questionnaire global score, and frequency of exercise (r = −31, p < .01) and duration of exercise (r = −31, p < .01).
3.5. EED scores in male ED participants compared with female ED participants (Sample 2)
Comparative analyses of EED Questionnaire scales in male and female ED participants revealed that male ED participants had, on average, lower scores in all scales. These results, which are listed in Table 5, were not affected by age and BMI as covariates. Since the item (“I listen to my body”) changed the factor‐loading scale in males (Table 2) and this was in contrast to our previous findings for females (Danielsen et al., 2015), it was left out of analyses of the actual subscales (i.e., “compulsive exercise and awareness of bodily signals”).
Table 5.
EED scores in male and female ED patients, global score, and subscales
|
Male ED patients (n = 55) Mean (SD) |
Female ED patients (n = 244) Mean (SD) |
t(297) p values |
Mean difference 95% CI | Effect size Cohens d | |
|---|---|---|---|---|---|
| EED global score | 1.99 (0.76) | 2.49 (0.96) | 3.74*** | 0.48 (0.23; 0.73) | 0.55 |
| EED compulsive | 1.89 (1.46) | 2.57 (1.50) | 3.04** | 0.68 (0.24; 1.12) | 0.46 |
| EED positive and healthy | 2.27 (1.40) | 2.41 (1.36) | .67 NS | 0.14 (−0.27; 0.54) | 0.09 |
| EED bodily signals | 1.59 (0.95) | 1.86 (1.18) | 1.82 NS | 0.27 (−0.03; .57) | 0.24 |
| EED weight and shape | 2.16 (1.63) | 3.00 (1.60) | 3.52 ** | 0.84 (0.37; 1.31) | 0.51 |
Note. NS = not significant. Diff: Mean: differences between patients and controls, 95% CI: 95% confidence intervals. t Tests for independent samples, two tailed. Cohens d: Small effect size = 0.2, medium = 0.5, and large = 0.8.
p < .05, p < .01, p < .001.
3.6. Gender difference in additional motives for exercise compared in male and female student controls (Sample 3)
The results showed that the items “I am physically active to get big muscles and I am physically active to get big” discriminated significantly (p < .001) between male and female student controls, with higher mean scores among males. Mean values and SD of the item “I am physically active to get big muscles” were: 2.09 (1.60) in males and 1.25 (1.20) in females, t(388) = 5.92 and Cohen's d = 0.59. In the item “I am physically active to get big”, the values were: 1.46 (0.11) in males and 0.75 (0.05) in females, t(388) = 9.87, Cohen's d = 8.3. Exercising for increased muscle strength was reported as equally important in male and female controls, and the mean (SD) values were, respectively, 2.81 (1.59) and 2.80 (1.43), t(388) = 0.01, p = .993. Age and BMI as covariates did not change the results.
4. DISCUSSION
Adequate psychometric properties and a four‐factor structure of the EED questionnaire were confirmed in the study. Good discriminant validity was found between males with ED and controls in EED global scores and subscales, and in 16 out of 18 items. The values for internal consistency in the scales were good in the global score and three subscales, and satisfactory in the fourth subscale (Field, 2009). Correlation was found between attitudes toward compulsive exercise (EED questionnaire scales) and ED pathology (the EDE‐Q global score), indicating convergent validity.
These results emphasized the need for assessments across different dimensions of attitudes toward compulsive exercise in males, and extended the utility of the EED questionnaire as a clinical measurement among males. Additionally, the findings are in accordance with clinical experience, and with theoretically derived knowledge of compulsive exercise in persons with EDs (Meyer, Taranis, Goodwin, & Haycraft, 2011). In the literature, compulsive exercise in AN patients has received most attention compared with other types of ED patients (Murray et al., 2012; Noetel et al., 2017). Low numbers in groups in males restricted investigations of compulsive exercise in our study. However, no significant differences between AN, BN, and unspecified eating disorders were found in the female validation study (Danielsen et al., 2015). This may indicate that the EED questionnaire covers more shared attitudes and thoughts toward compulsive exercise, thus supporting the clinical utility of the scale among ED patients. Female binge eating disorder (BED) patients showed similarities and differences compared with other diagnostic groups (Danielsen et al., 2015), thus indicating the EED questionnaire scale as less useful for BED patients. All comparative analyses in this study were investigated for the influence of age and BMI. In the majority of analyses, these factors did not affect the results. Due to low number of males with ED, these results are preliminary.
Our findings related to adequate psychometric properties and the four‐factor structure of the EED questionnaire corresponded closely to results from the female validation study, and the total explained variance was 73% in both studies (Danielsen et al., 2015). Similarly, the magnitude of differences between ED participants and controls was mainly at the same level in both studies, suggesting that the questionnaire discriminates satisfactorily between ED patients and controls in both genders. The strength of convergent validity in males (whole male sample) was at the same level as found among females (Danielsen et al., 2015). Such correlations have also been reported in studies of other exercise measures (Cunningham et al., 2016; Young et al., 2016), but Cunningham et al. reported a weaker correlation in males. These studies investigated other exercise measures than the EED questionnaire, and therefore it is difficult to make direct comparisons. The difference in the strength of the correlation between our study and Cunningham et al.'s study may also be due to the nonclinical nature of their sample, although ED diagnosis based on EDE‐Q scores was used.
However, some differences between the former female validation study and the male validation study should be acknowledged. Two of the items did not discriminate significantly between male groups. For the item “I am physically active for appearance reasons”, there was a tendency for higher scores among male ED participants, and for the item “I notice when I get tired” the mean scores were almost identical in males. With one exception, all items loaded in the same way in the male and female samples. In male groups, two of the subscales did not show a significant correlation with ED pathology measured by the EDE‐Q: the “awareness of bodily signals and positive and healthy exercise” subscales. In the female validation study, significant associations were found for all subscales, but with weaker associations for the two aforementioned subscales. The differences between the two validation studies should be investigated in a larger clinical male sample to clarify whether the results are due to gender differences or differences in sample size.
In the literature, it has been emphasized that quantitative measures are difficult to compare across studies due to the diversity of measures (Meyer & Taranis, 2011). Our investigations of the male sample were based on self‐reported information about the frequency, intensity, and duration of exercise. We did not find any significant differences between male ED participants and male controls, and correlations between amount of exercise and the EED Questionnaire global scale showed inconsistent results. Our findings supporting those of researchers who have emphasized that it is more important to address attitudes and thoughts towards compulsive dimensions of exercise than quantitative amounts of exercise in ED patients (Adkins & Keel, 2005; Meyer & Taranis, 2011).
Recognizing gender differences in ED is important in a clinical setting in order to offer adequate treatment. Our results showed that males with ED on average reported lower scores in EED questionnaire scales than females with ED, especially in the global score and two of the subscales (i.e., “compulsive exercise and exercise for weight and shape reasons”). Such gender differences are in agreement with reports of lower scores in ED measures in general among males (Dahlgren et al., 2017; Darcy et al., 2012; Reas et al., 2012). We are not aware of comparable studies that investigated attitudes towards compulsive exercise and gender differences in transdiagnostic ED samples. Despite differences in the samples and measurements, our finding of exercise for weight and shape reasons as less important than compulsive elements was found in a clinical AN sample using the CET as measure of compulsive exercise (Murray et al., 2012).
Our final aim was to extend the utility of the EED questionnaire in males through exploration of items in the nonclinical sample (Sample 3). On average, male students reported that they exercised to get big muscles and to get big as significantly more important than female students. This finding was in accordance with previous reports of gender differences related to muscularity and body size in the literature (e.g., Furnham et al., 2002). The item related to increased muscle strength was found equally important in male and female students in our sample. However, it seems reasonable to include all three items in a male EED questionnaire version for testing in a clinical sample.
4.1. Strengths and limitations
This study reported in this paper is one of few to investigate compulsive exercise in a clinical male ED sample. It extended the utility of EED Questionnaire as a clinical measurement tool in males. Further, the study was beneficial because comparisons were made between male ED patients and both male controls and female ED patients. However, when interpreting the results, several limitations should be noted. First, there were challenges related to the male ED sample. It was too small both to perform a separate PCA for patients and comparative analyses between diagnostic groups. The transdiagnostic sample included patients with a great range in BMI, which may imply differences that were not illuminated in our study. In comparative analyses, it is also necessary to be aware of challenges due to differences in sample size between male ED participants and male controls. Hence, to increase the generalization of our results, it would be necessary to replicate the results in a larger clinical sample of males with ED. Additionally, other factors should be recognized. In common with many ED measures, the EDE‐Q may not necessarily recognize specific men's issues, and the use of the EDE‐Q as a measure to investigate convergent validity in our study may have had limitations. To investigate convergent and concurrent validity properly, future research may benefit from investigations using a recognized male‐specific eating disorder assessment tool. In the context of self‐reported data, general considerations related to under‐reporting and over‐reporting are well known. In our study, this also applied to self‐reported weight in controls. When patients from different treatment centers are included in a study, differences in diagnostic procedures may appear. However, in our study, all patients were evaluated in specialized eating disorder units by licensed psychologists and psychiatrists to confirm that they suffered from an ED and that the transdiagnostic sample would eliminate the influence of the results.
5. CONCLUSION
The results of our study indicated the EED questionnaire is a valid and reliable clinical tool in males, across different attitudes and thoughts toward compulsive exercise. When such attitudes and thoughts toward compulsive exercise are investigated in males with ED, it is important to acknowledge that males with EDs should be compared with healthy males. Our intention has been to increase the utility of the EED questionnaire in males, but also to keep the questionnaire short and easy to administer. To achieve this, we have chosen to include three additional items regarding muscle size, body size, and muscle strength.
CONFLICT OF INTEREST
The authors indicate no conflicts of interest.
ACKNOWLEDGMENTS
The authors thank eight eating disorder units in Norway for their contribution to the recruitment of males with EDs to their study. They also wish to thank research staff member Tove Haga for assistance and good work in the data collection phase, statistician Tor Åge Myklebust is thanked for providing good advice on statistical questions, the Research Department, Nord‐Trøndelag Hospital Trust is thanked for financial support for the writing of this article and Catriona Turner for language checking.
Danielsen M, Bjørnelv S, Bratberg GH, Rø Ø. Validation of the exercise and eating disorder questionnaire in males with and without eating disorders. Int J Eat Disord. 2018;51:429–438. https://doi.org/10.1002/eat.22855
Funding information The Research Department, Nord‐Trøndelag Hospital Trust
REFERENCES
- Adkins, E. C. , & Keel, P. K. (2005). Does “excessive” or “compulsive” best describe exercise as a symptom of bulimia nervosa? International Journal of Eating Disorders, 38(1), 24–29. https://doi.org/10.1002/eat.20140 [DOI] [PubMed] [Google Scholar]
- Cash, T. F. , Novy, P. L. , & Grant, J. R. (1994). Why do women exercise? Factor analysis and further validation of the reasons for exercise inventory. Perceptual and Motor Skills, 78(2), 539–544. [DOI] [PubMed] [Google Scholar]
- Cunningham, H. E. , Pearman, S. III , & Brewerton, T. D. (2016). Conceptualizing primary and secondary pathological exercise using available measures of excessive exercise. International Journal of Eating Disorders, 49(8), 778–792. https://doi.org/10.1002/eat.22551 [DOI] [PubMed] [Google Scholar]
- Dahlgren, C. L. , Stedal, K. , & Ro, O. (2017). Eating disorder examination questionnaire (EDE‐Q) and clinical impairment assessment (CIA): Clinical norms and functional impairment in male and female adults with eating disorders. Nordic Journal Psychiatry, 71(4), 256–261. https://doi.org/10.1080/08039488.2016.1271452 [DOI] [PubMed] [Google Scholar]
- Dahlgren, C. L. , & Wisting, L. (2016). Transition from DSM‐IV to DSM‐5: A systematic review of eating disorder prevalence assessment. International Journal of Eating Disorders, 49(11), 975–997. https://doi.org/10.1002/eat.22596 [DOI] [PubMed] [Google Scholar]
- Danielsen, M. , Bjornelv, S. , & Ro, O. (2015). Validation of the exercise and eating disorders questionnaire. International Journal of Eating Disorders, 48(7), 983–993. https://doi.org/10.1002/eat.22393 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Danielsen, M. , Bratberg, G. H. , & Ro, O. (2012). A pilot study of a new assessment of physical activity in eating disorder patients. Eating and Weight Disorders: EWD, 17(1), e70–e77. https://doi.org/10.1007/bf03325332 [DOI] [PubMed] [Google Scholar]
- Danielsen, M. , Ro, O. , Romild, U. , & Bjornelv, S. (2016). Impact of female adult eating disorder inpatients' attitudes.to compulsive exercise on outcome at discharge and follow‐up. Journal of Eating Disorders, 4(1), 7 https://doi.org/10.1186/s40337-016-0096-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darcy, A. M. , Doyle, A. C. , Lock, J. , Peebles, R. , Doyle, P. , & Le Grange, D. (2012). The eating disorders examination in adolescent males with anorexia nervosa: How does it compare to adolescent females? International Journal of Eating Disorders, 45(1), 110–114. https://doi.org/10.1002/eat.20896 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis, C. , Kennedy, S. H. , Ralevski, E. , Dionne, M. , Brewer, H. , Neitzert, C. , & Ratusny, D. (1995). Obsessive compulsiveness and physical activity in anorexia nervosa and high‐level exercising. Journal of Psychosomatic Research, 39(8), 967–976. [DOI] [PubMed] [Google Scholar]
- Duncan, A. E. , Ziobrowski, H. N. , & Nicol, G. (2017). The prevalence of past 12‐month and lifetime DSM‐IV eating disorders by BMI category in US men and women. European Eating Disorders Review, 25(3), 165–171. https://doi.org/10.1002/erv.2503 [DOI] [PubMed] [Google Scholar]
- Fairburn, C. G. , & Beglin, S. J. (2008). The eating disorder examination questionnaire (EDE‐Q 6.0) In Fairburn C. G. (Ed.), Cognitive behavior therapy and eating disorders. New York, NY: Guilford Press. [Google Scholar]
- Field, A. (2009). Discovering statistics using SPSS (3rd ed.). London, UK: Sage Publications Ltd. [Google Scholar]
- Furnham, A. , Badmin, N. , & Sneade, I. (2002). Body image dissatisfaction: Gender differences in eating attitudes, self‐esteem, and reasons for exercise. Journal of Psycholology, 136(6), 581–596. https://doi.org/10.1080/00223980209604820 [DOI] [PubMed] [Google Scholar]
- Hausenblas, H. , & Downs, D. S. (2010). How much is too much? The development and validation of the exercise dependence scale. Psychology and Health, 17(4), 387 https://doi.org/10.1080/0887044022000004894 [Google Scholar]
- Kurtze, N. , Rangul, V. , Hustvedt, B. E. , & Flanders, W. D. (2008). Reliability and validity of self‐reported physical activity in the Nord‐Trondelag Health Study: HUNT 1. Scandinavian Journal of Public Health, 36(1), 52–61. https://doi.org/10.1177/1403494807085373 [DOI] [PubMed] [Google Scholar]
- Meyer, C. , Plateau, C. R. , Taranis, L. , Brewin, N. , Wales, J. , & Arcelus, J. (2016). The compulsive exercise test: Confirmatory factor analysis and links with eating psychopathology among women with clinical eating disorders. Journal of Eating Disorders, 4(1), 22 https://doi.org/10.1186/s40337-016-0113-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer, C. , & Taranis, L. (2011). Exercise in the eating disorders: Terms and definitions. European Eating Disorders Review, 19(3), 169–173. https://doi.org/10.1002/erv.1121 [DOI] [PubMed] [Google Scholar]
- Meyer, C. , Taranis, L. , Goodwin, H. , & Haycraft, E. (2011). Compulsive exercise and eating disorders. European Eating Disorders Review, 19(3), 174–189. https://doi.org/10.1002/erv.1122 [DOI] [PubMed] [Google Scholar]
- Murray, S. B. , Griffiths, S. , Rieger, E. , & Touyz, S. (2013). A comparison of compulsive exercise in male and female presentations of anorexia nervosa: What is the difference? Advances in Eating Disorders: Theory, Research and Practice, 2(1), 65–70. https://doi.org/10.1080/21662630.2013.839189 [Google Scholar]
- Murray, S. B. , Rieger, E. , Hildebrandt, T. , Karlov, L. , Russell, J. , Boon, E. , … Touyz, S. W. (2012). A comparison of eating, exercise, shape, and weight related symptomatology in males with muscle dysmorphia and anorexia nervosa. Body Image, 9(2), 193–200. https://doi.org/10.1016/j.bodyim.2012.01.008 [DOI] [PubMed] [Google Scholar]
- Noetel, M. , Dawson, L. , Hay, P. , & Touyz, S. (2017). The assessment and treatment of unhealthy exercise in adolescents with anorexia nervosa: A Delphi study to synthesize clinical knowledge. International Journal of Eating Disorders, 50(4), 378–388. https://doi.org/10.1002/eat.22657 [DOI] [PubMed] [Google Scholar]
- Ogden, J. , Veale, D. , & Summers, Z. (1997). The development and validation of the exercise dependence questionnaire. Addiction Research, 5, 343–356. [Google Scholar]
- Preti, A. , Girolamo, G. D. , Vilagut, G. , Alonso, J. , Graaf, R. D. , Bruffaerts, R. , … Morosini, P . (2009). The epidemiology of eating disorders in six European countries: Results of the ESEMeD‐WMH project. Journal of Psychiatrc Research, 43(14), 1125–1132. https://doi.org/10.1016/j.jpsychires.2009.04.003 [DOI] [PubMed] [Google Scholar]
- Raevuori, A. , Hoek, H. W. , Susser, E. , Kaprio, J. , Rissanen, A. , & Keski‐Rahkonen, A. (2009). Epidemiology of anorexia nervosa in men: A nationwide study of Finnish twins. PLoS One, 4(2), e4402 https://doi.org/10.1371/journal.pone.0004402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Raevuori, A. , Keski‐Rahkonen, A. , & Hoek, H. W. (2014). A review of eating disorders in males. Current Opinion in Psychiatry, 27(6), 426–430. https://doi.org/10.1097/YCO.0000000000000113 [DOI] [PubMed] [Google Scholar]
- Reas, D. L. , Overas, M. , & Ro, O. (2012). Norms for the eating disorder examination questionnaire (EDE‐Q) among high school and university men. Eating Disorders: Journal of Treatment and Prevention, 20(5), 437–443. https://doi.org/10.1080/10640266.2012.715523 [DOI] [PubMed] [Google Scholar]
- Stanford, S. C. , & Lemberg, R. (2012). Measuring eating disorders in men: Development of the eating disorder assessment for men (EDAM). Eating Disorders: Journal of Treatment and Prevention, 20(5), 427–436. https://doi.org/10.1080/10640266.2012.715522 [DOI] [PubMed] [Google Scholar]
- Steffen, J. J. , & Brehm, B. J. (1999). The dimensions of obligatory exercise. Eating Disorders: Journal of Treatment and Prevention, 7(3), 219–226. https://doi.org/10.1080/10640269908249287 [Google Scholar]
- Strother, E. , Lemberg, R. , Stanford, S. C. , & Turberville, D. (2012). Eating disorders in men: Underdiagnosed, undertreated, and misunderstood. Eating Disorders, 20(5), 346–355. https://doi.org/10.1080/10640266.2012.715512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Taranis, L. , Touyz, S. , & Meyer, C. (2011). Disordered eating and exercise: Development and preliminary validation of the compulsive exercise test (CET). European Eating Disorders Review, 19(3), 256–268. https://doi.org/10.1002/erv.1108 [DOI] [PubMed] [Google Scholar]
- Young, S. , Touyz, S. , Meyer, C. , Arcelus, J. , Rhodes, P. , Madden, S. , … Hay, P. (2016). Validity of exercise measures in adults with anorexia nervosa: The EDE, compulsive exercise test and other self‐reportscales. International Journal of Eating Disorders, 50(5), 533–541. https://doi.org/10.1002/eat.22633 [DOI] [PubMed] [Google Scholar]
- Weltzin, T. E. , Cornella‐Carlson, T. , Fitzpatrick, M. E. , Kennington, B. , Bean, P. , & Jefferies, C. (2012). Treatment issues and outcomes for males with eating disorders. Eating Disorders: Journal of Treatment and Prevention, 20(5), 444–459. https://doi.org/10.1080/10640266.2012.715527 [DOI] [PubMed] [Google Scholar]
- Zeeck, A. , Schlegel, S. , Giel, K. E. , Junne, F. , Kopp, C. , Joos, A. , … Hartmann, A. (2017). Validation of the German version of the commitment to exercise scale. Psychopathology, 50(2), 146–156. https://doi.org/10.1159/000455929 [DOI] [PubMed] [Google Scholar]