

Abstract
Fragile X syndrome (FXS) is the most common inherited cause of intellectual disability and is caused by an expansion of cytosine‐guanine‐guanine (CGG) repeats in the FMR1 gene. Female premutation allele carriers (55–200 CGG repeats) are at risk to have an affected child. Currently, specific population‐based carrier screening for FXS is not recommended. Previous studies exploring female premutation carrier frequency have been limited by size or ethnicity. This retrospective study provides a pan‐ethnic estimate of the Fragile X premutation carrier frequency in a large, ethnically diverse population of women referred for routine carrier screening during a specified time period at Progenity, Inc. Patient ethnicity was self‐reported and categorized as: African American, Ashkenazi Jewish, Asian, Caucasian, Hispanic, Native American, Other/Mixed/Unknown, or Sephardic Jewish. FXS test results were stratified by ethnicity and repeat allele category. Total premutation carrier frequency was calculated and compared against each ethnic group. A total of 134,933 samples were included. The pan‐ethnic premutation carrier frequency was 1 in 201. Only the Asian group differed significantly from this frequency. Using the carrier frequency of 1 in 201, a conservative pan‐ethnic risk estimate for a male fetus to have FXS can be calculated as 1 in 2,412. This risk is similar to the highest ethnic‐based fetal risks for cystic fibrosis and spinal muscular atrophy, for which population‐wide screening is currently recommended. This study adds to the literature and supports further evaluation into specific population‐wide screening recommendations for FXS.
Keywords: carrier frequency, carrier screening, fragile X syndrome, premutation allele
1. INTRODUCTION
Expansion of CGG repeats in the FMR1 gene cause fragile X syndrome (FXS), the most common inherited cause of intellectual disability and autism (Saul & Tarleton, 1998). Women who carry a repeat allele in the premutation range (55–200) are at risk to have an affected child through expansion during meiosis. Current guidelines for FXS carrier testing in women include: a history of ovarian insufficiency; a family history of FXS/related disorders, unexplained neuropsychiatric symptoms, or premature ovarian insufficiency; and any woman who requests testing, regardless of her family history (American College of Obstetricians and Gynecologists Committee on Genetics [ACOG], 2017a, 2017b; Finucane et al., 2012; Sherman, Pletcher, & Driscoll, 2005). Some of the concerns of implementing specific population‐based carrier screening for FXS include limited data on the frequency of premutation carriers; the variability of the condition, particularly in girls; and the risk for carriers to have symptoms related to having a premutation allele (Finucane et al., 2012).
Diagnosis of FXS in affected individuals is often delayed due to the variability in symptoms in early childhood. Approximately 25% of families have a second child with FXS prior to receiving the diagnosis for their first child (Bailey, Raspa, Bishop, & Holiday, 2009; Bailey, Skinner, & Sparkman, 2003), and this information is not always shared with extended family members (Raspa, Edwards, Wheeler, Bishop, & Bailey, 2016). These factors increase the risk of missing female premutation carriers based on current screening guidelines. Therefore, professionals have advocated for exploring feasibility and appropriateness of expanded carrier testing for FXS (Abrams et al., 2012; Finucane et al., 2012; Hill, Archibald, Cohen, & Metcalfe, 2010; Sherman et al., 2005).
Estimates of the prevalence of FXS have changed over time, with more recent suggestions of approximately 1 in 4,000 individuals (Bailey et al., 2017). Previous studies have also attempted to define population frequency of female premutation allele carriers. Comparisons between studies have been difficult due to differences in the definition of premutation CGG repeat size, selection bias, and small or ethnically homogenous populations (Hill et al., 2010). Recent published estimates of female premutation carrier frequency in the United States range from 1 in 148 to 1 in 178 (Hantash et al., 2011; Maenner et al., 2013; Seltzer et al., 2012). Differences in premutation carrier frequency have been noted across ethnicities (Genereux & Laird, 2013; Weiss et al., 2014). This study furthers the literature by providing a pan‐ethnic estimate of the female premutation carrier frequency in a large, ethnically diverse population of women referred for routine carrier screening.
2. MATERIALS AND METHODS
This retrospective cohort study utilized data from all female patients referred to Progenity, Inc., a commercial molecular diagnostics laboratory, for carrier screening that included FXS testing as part of their routine clinical management during a specified time period. Informed consent was collected by the ordering provider, as required by law for clinical genetic testing in the state of sample collection. Fragile X testing through Progenity, Inc., is available as a stand‐alone test, or as part of carrier testing panels of varying numbers of conditions. Patient ethnicity was self‐reported on the test requisition form and included the following categories: African American, Ashkenazi Jewish, Asian, Caucasian, Hispanic, Native American, Other/Mixed/Unknown, and Sephardic Jewish. If a patient writes in any other ethnicity that does not match the above categories, it is classified as “Other/Mixed/Unknown.” All personal health information, with the exception of ethnicity, was de‐identified. As such, the study was determined to be exempt from institutional review board approval by the University of Miami Miller School of Medicine and Aspire IRB. A total of 134,933 samples were included in this study.
Fragile X CGG trinucleotide repeat analysis was performed at the Progenity, Inc. laboratory located in Ann Arbor, Michigan using the AmplideX™ FMR1 PCR Kit (Asuragen®, Austin, TX). The kit is a three‐primer CGG repeat primed PCR from purified genomic DNA. Amplified DNA fragments were sized on a capillary electrophoresis 3500xl Genetic Analyzer (Applied Biosystems, Foster City, CA). Data was viewed using GeneMapper software (Applied Biosystems). Asuragen® algorithms were used to convert the patient's amplicon size to CGG‐repeat number by comparing sample mobility to a known size‐standard provided with the AmplideX™ Kit. Final results were reported as FMR1 CGG‐repeat size for each patient tested. Repeat sizes were grouped into the following categories: greater than 200 repeats were classified as full mutations, 55–200 repeats as premutations, 45–54 repeats as gray zone/intermediate alleles, and <45 repeats as normal alleles (Saul & Tarleton, 1998). The accuracy of the testing methodology is ±1 for 0–54 CGG repeats, ±2 for 55–70 CGG repeats, ±3 for 71–120 CGG repeats, and ±5 for 121–200 CGG repeats.
Test results were stratified by ethnicity and repeat allele category. Descriptive statistics were used to generate demographic data. Overall frequencies were generated for each repeat size group. Total female premutation allele frequency was calculated. The overall premutation allele frequency in this study was compared to those from the Seltzer et al. (2012) and Hantash et al. (2011) studies using the assumption that the cohorts followed a Poisson process and computing a p‐value according to the method in Agresti (2002). This method could not be used to compare the frequency from this study to that of Maenner et al. (2013) due to the latter study's population structure, in which many of the individuals tested were related to one another.
Premutation allele carrier frequencies were generated for each ethnicity by modelling the frequencies as a Poisson process. Confidence intervals for carrier frequencies were estimated using the chi‐squared distribution (Garwood, 1936). Upper and lower bounds of the 95% confidence intervals were approximated as a rational number whose numerator is 1 (e.g., 1/k for some integer value of k). The value of k was determined to be that which minimized the difference between 1/k and the target frequency.
Multiple analyses were then used to test if the carrier frequencies varied by ethnicity. These included the chi‐square test for independence (McHugh, 2013), Cramer's V statistic for association, and the E‐test (Krishnamoorthy & Thomson, 2004). Power analysis was performed for the chi‐square test of independence using the GPower program (Faul, Erdfelder, Lang, & Buchner, 2007). Power was set to 0.95, α was set to 0.05, effect size w was set to 0.05, and degrees of freedom was set to 6, which provided a necessary sample size of 8,343. The E‐test was used to evaluate, for each pair of ethnicity categories, the p‐value of the observations under the null hypothesis that each ethnic group has the same carrier frequency Poisson mean (Krishnamoorthy & Thomson, 2004). Each ethnic group was also compared to the overall female premutation allele frequency. The p‐values were then Bonferroni corrected. The ethnic categories of Sephardic Jewish and Native American were excluded from these analyses due to the small number of samples in both of these categories.
3. RESULTS
Fragile X test results for 134,933 samples were analyzed. The largest ethnic group represented was Caucasian, while Sephardic Jewish and Native American individuals accounted for the smallest groups. Fifteen percent of the individuals reported Other/mixed/unknown ethnicity. Table 1 presents the results stratified by ethnicity and CGG allele type.
Table 1.
Female Fragile X testing results stratified by allele type and ethnicity
| Ethnicity | n (%)a | Normal | Gray zone | Premutation | Full mutation |
|---|---|---|---|---|---|
| African American/Black | 14,420 (10.7) | 14,165 | 199 | 54 | 2 |
| Ashkenazi Jewish | 1,118 (0.8) | 1,078 | 29 | 11 | 0 |
| Asian | 7,961 (5.9) | 7,856 | 85 | 19 | 1 |
| Caucasian/White | 65,356 (48.4) | 63,302 | 1,664 | 384 | 6 |
| Hispanic | 26,030 (19.3) | 25,625 | 301 | 103 | 1 |
| Native American | 102 (0.1) | 99 | 3 | 0 | 0 |
| Other/Mixed/Unknown | 19,850 (14.7) | 19,338 | 412 | 98 | 2 |
| Sephardic Jewish | 96 (0.1) | 91 | 3 | 1 | 1 |
N = 134,933.
The total frequencies of each CGG allele type were as follows: normal (97.5%), gray zone/intermediate (2%), premutation (0.5%), and full mutation (0.01%). The overall, pan‐ethnic premutation allele carrier frequency was found to be 1 in 201 (95% confidence interval 1 in 202 to 1 in 201). Thirteen full mutation alleles were identified in the sample population. Comparisons of the overall premutation allele frequency between this study cohort and the previous studies by Seltzer et al. (2012) and Hantash et al. (2011) using a p‐value threshold of 0.05 revealed a statistically significant difference between our cohort and both previous cohorts (p = 5.93 × 10−15 and p = 3.34 × 10−2, respectively). Table 2 lists premutation carrier frequencies by ethnic group. Of note, this could not be calculated for Native Americans, as no premutation allele carriers were identified. The ethnic groups with the highest premutation carrier frequencies were Sephardic Jewish and Ashkenazi Jewish, while the Asian group was found to have the lowest carrier frequency.
Table 2.
Fragile X female premutation allele carrier frequency by ethnic group
| Ethnicitya | Premutation allele carrier frequencyb (95% confidence interval) |
|---|---|
| African American/Black | 1 in 267 (1 in 269 to 1 in 263) |
| Ashkenazi Jewish | 1 in 102 (1 in 105 to 1 in 95) |
| Asian | 1 in 419 (1 in 428 to 1 in 404) |
| Caucasian/White | 1 in 170 (1 in 170 to 1 in 170) |
| Hispanic | 1 in 253 (1 in 254 to 1 in 251) |
| Other/Mixed/Unknown | 1 in 203 (1 in 203 to 1 in 201) |
| Sephardic Jewish | 1 in 96 (1 in 140 to 1 in 57) |
Native Americans are not included since none were found to be premutation carriers.
Overall female premutation allele carrier frequency was found to be 1 in 201 (1 in 202 to 1 in 201).
Premutation allele frequency was found to be dependent upon ethnic background according to the chi‐square test of independence (p = 7.92 × 10−7); however, this association was weak, with a Cramer's V statistic of 0.16. Pairwise comparisons of each ethnic group revealed statistically significant differences between the Caucasian group and the African American, Asian, and Hispanic groups; and between the Asian group and the Other/Mixed/Unknown group (Bonferroni corrected p < 2.38 × 10−3). Comparisons of the premutation allele frequency among each individual ethnic group and the overall pan‐ethnic frequency revealed a statistically significant difference for only the Asian group (Bonferroni corrected p < 7.14 × 10−3).
4. DISCUSSION
This study identified an overall fragile X premutation allele frequency of 1 in 201 in a large, ethnically diverse population of women. This frequency is significantly lower than what was identified previously by Seltzer et al. (2012) and Hantash et al. (2011), and may be related to the characteristics of the study cohorts. This study population utilized a larger female sample size (134,933 versus 3,474 and 13,770, respectively) with a more diverse ethnic composition (the female cohort in the Seltzer et al. (2012) study was mostly of Northern European descent), including an “Other/Mixed/Unknown” category. Maenner et al. (2013) also identified a higher premutation carrier frequency; however, their 95% confidence interval is large and overlaps with what was identified in this study (1 in 207 to 1 in 113 and 1 in 202 to 1 in 201, respectively). Both the Maenner et al. (2013) and Seltzer et al. (2012) studies utilized random population samples that had no indication for carrier screening. For this study, the specific reason for each individual undergoing screening could not be obtained; therefore, it is possible that some of the individuals could be at a higher than average risk to be premutation carriers based on personal or family history. Interestingly, a 2012 study by Tassone et al. examined the premutation carrier frequency in an unselected population of newborns undergoing newborn screening during a specified time period. The authors report a female premutation carrier frequency of 1 in 209, which is similar to what is presented in this study.
This study identified statistically significant differences in fragile X premutation allele frequency among some of the ethnic groups. However, when comparing individual groups to the overall pan‐ethnic frequency, the only group remaining significantly different was the Asian group. The lower frequency in the Asian group supports previous findings in this population (Genereux & Laird, 2013; Hill et al., 2010). Tassone et al. (2012) found a higher frequency in their Asian group than that of their overall population (1 in 123 compared to 1 in 209). This may potentially be explained by the inclusion in the Asian group of individuals who identify as Indian (these individuals would have been categorized as Other/mixed/unknown in this study). The premutation frequency in Hispanic/Latino individuals in the Tassone et al. (2012) study is lower than what was observed in this study (1 in 570 versus 1 in 253, respectively.) This difference may be partially explained by the smaller number of Hispanic individuals in the Tassone et al. (2012) study (3,493 versus 26,030, respectively). Although the individual ethnic group frequencies differ somewhat between the two studies, the overall premutation frequency is similar, suggesting that the differences seen between the individual ethnic groups could be related to the smaller sample sizes of these groups as compared to the entire population.
Estimates of the frequency of the fragile X premutation allele in the general population have increased over time, suggesting that carriers for the premutation allele are more common than previously described (Hill et al., 2010). Although professional societies have recently supported expanded carrier screening as an appropriate option for all ethnicities, population‐wide recommendations for carrier testing are currently limited to cystic fibrosis (CF) and spinal muscular atrophy (SMA) (ACOG, 2017a, 2017b; Edwards et al., 2015). Carrier frequencies for these conditions vary among different ethnicities (between 1 in 24 in Ashkenazi Jewish individuals and 1 in 94 for Asians for CF, and between 1 in 35 for Caucasians and 1 in 117 for Hispanics for SMA) (ACOG, 2017a, 2017b). These carrier frequencies are higher than the pan‐ethnic female fragile X premutation carrier frequency identified in this study (1 in 201). However, the overall fetal risk for FXS may be similar, given that the inheritance pattern of FXS only requires the mother to be a premutation allele carrier, whereas autosomal recessive diseases require both partners to be carriers of a condition.
As an example, the ethnicity‐based risk for an Ashkenazi Jewish couple to have a child with CF is 1 in 2,304: 1/24 × 1/24 × 1/4 (probability of inheriting a mutation from both parents). The pan‐ethnic risk for a couple to have a male child with FXS may be similar to this. Using the carrier frequency data from our study, a conservative estimate of male fetal risk for FXS can be calculated as: 1/201 × ½ (probability of having a male child) × ½ (probability of inheriting the premutation allele) × 1/3 (risk of expansion to a full mutation—see Figure 1), which would result in a fetal risk of 1 in 2,412. Of note, Coffee et al. (2009) analyzed 36,124 male deidentified dried blood spots from the state of Georgia's newborn screening program and identified a prevalence of FXS of 1 in 5,161 males. This is a much lower value and is likely due to factors that impact the birth rate of males with FXS. Examples of such factors include the increased risk for fertility difficulties among female premutation carriers, along with the spectrum of reproductive choices, such as not having biological children, using preimplantation diagnosis to have an unaffected child, or termination of an affected pregnancy, available to female premutation carriers.
Figure 1.
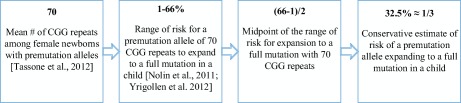
Determining an estimated risk of expansion of a premutation allele to a full mutation. Information was gathered from previous publications to determine a conservative estimate of the risk of a premutation allele expanding to a full mutation in a child [Color figure can be viewed at http://wileyonlinelibrary.com]
A pan‐ethnic fetal risk of 1 in 2,412 for FXS falls between the highest ethnic‐based risk for CF (1 in 2,304 for Ashkenazi Jewish couples) and for SMA (1 in 4,900 for Caucasian couples), disorders for which population‐wide carrier screening is currently recommended (ACOG, 2017a, 2017b). Haque et al. (2016) modeled fetal risk of genetic diseases across ethnic groups based on carrier frequencies identified among individuals undergoing expanded carrier testing, and suggested that the fetal risk for FXS is greater than that for CF and SMA for most ethnic categories. Taken together, these results suggest that the female FXS premutation carrier frequency is high enough to warrant further evaluation into population‐wide screening for FXS.
There are limitations to this study. Ethnicity was self‐reported and may not accurately represent an individual's true ethnic background. The data utilized was de‐identified and categorized based on allele type (normal, premutation, etc.). It was therefore not possible to discern each participant's reason for undergoing carrier screening or their exact CGG repeat size. The study population may include individuals who had a higher risk to be a premutation carrier based on personal or family history. The fetal risk calculation for FXS in this article was calculated using data from the Tassone et al. (2012) study to determine average premutation CGG repeat size. Without having the average repeat size of the current study available, the calculated fetal risk for FXS may therefore be an under‐ or over‐estimate.
Current guidelines do not recommend specific population‐based screening for FXS based partly on an unclear carrier frequency, variability of FXS, and the risk for carriers to have symptoms related to having a premutation allele. This study provides a pan‐ethnic risk estimate of premutation carrier frequency based on a large, diverse population, and suggests that the fetal risk for FXS is comparable to that of CF and SMA. This supports the need for further evaluation into whether population‐based screening is appropriate for FXS, including studies that address the psychosocial impact of having a premutation allele.
CONFLICT OF INTEREST
Authors KO, LD, CH, JD, and CS are paid employees of Progenity, Inc. TM was a paid employee of Progenity, Inc. during the duration of the study.
ACKNOWLEDGMENTS
The authors would like to thank Catherine Terhaar, MS, CGC, for her assistance in data collection.
Owens KM, Dohany L, Holland C, et al. FMR1 premutation frequency in a large, ethnically diverse population referred for carrier testing. Am J Med Genet Part A. 2018;176A:1304–1308. https://doi.org/10.1002/ajmg.a.38692
REFERENCES
- Abrams, L. , Cronister, A. , Brown, W. T. , Tassone, F. , Sherman, S. L. , Finucane, B. , … Berry‐Kravis, E. (2012). Newborn, carrier, and early childhood screening recommendations for fragile X. Pediatrics, 130(6), 1126–1135. [DOI] [PubMed] [Google Scholar]
- Agresti, A. (2002). Categorical data analysis (2nd ed). Hoboken, NJ: Wiley. [Google Scholar]
- American College of Obstetricians and Gynecologists Committee on Genetics . (2017a). Committee opinion No. 690: Carrier screening in the age of genomic medicine. Obstetrics and Gynecology, 129, e35–e40. [DOI] [PubMed] [Google Scholar]
- American College of Obstetricians and Gynecologists Committee on Genetics . (2017b). Committee opinion No. 691: Carrier screening for genetic conditions. Obstetrics and Gynecology, 129, e41–e55. [DOI] [PubMed] [Google Scholar]
- Bailey, D. B., Jr. , Berry‐Kravis, E. , Gane, L. W. , Guarda, S. , Hagerman, R. , Powell, C. M. , … Wheeler, A. (2017). Fragile X newborn screening: Lessons learned from a multisite screening study. Pediatrics, 139(Suppl 3), S216–S225. [DOI] [PubMed] [Google Scholar]
- Bailey, D. B. Jr. , Raspa, M. , Bishop, E. , & Holiday, D. (2009). No change in the age of diagnosis for fragile X syndrome: Findings from a national parent survey. Pediatrics, 124, 527–533. [DOI] [PubMed] [Google Scholar]
- Bailey, D. B., Jr. , Skinner, D. , & Sparkman, K. L. (2003). Discovering fragile X syndrome: Family experiences and perceptions. Pediatrics, 111, 407–416. [DOI] [PubMed] [Google Scholar]
- Coffee, B. , Keith, K. , Albizua, I. , Malone, T. , Mowrey, J. , Sherman, S. L. , & Warren, S. T. (2009). Incidence of fragile X syndrome by newborn screening for methylated FMR1 DNA. The American Journal of Human Genetics, 85, 503–514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Edwards, J. G. , Feldman, G. , Goldberg, J. , Gregg, A. R. , Norton, M. E. , Rose, N. C. , … Watson, M. S. (2015). Expanded carrier screening in reproductive medicine‐points to consider‐A joint statement of the American College of Medical Genetics and Genomics, American College of Obstetricians and Gynecologists, National Society of Genetic Counselors, Perinatal Quality Foundation, and Society for Maternal‐Fetal Medicine. Obstetrics and Gynecology, 125(3), 653–662. [DOI] [PubMed] [Google Scholar]
- Faul, F. , Erdfelder, E. , Lang, A. G. , & Buchner, A. (2007). G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behavior Research Methods, 39, 175–191. [DOI] [PubMed] [Google Scholar]
- Finucane, B. , Abrams, L. , Cronister, A. , Archibald, A. D. , Bennett, R. L. , & McConkie‐Rosell, A. (2012). Genetic counseling and testing for FMR1 gene mutations: Practice guidelines of the National Society of Genetic Counselors. Journal of Genetic Counseling, 21, 752–760. [DOI] [PubMed] [Google Scholar]
- Garwood, F. (1936). Fiducial limits for the Poisson distribution. Biometrika, 28, 437–442. [Google Scholar]
- Genereux, D. P. , & Laird, C. D. (2013). Why do fragile X carrier frequencies differ between Asian and non‐Asian populations? Genes and Genetic Systems, 88, 211–224. [DOI] [PubMed] [Google Scholar]
- Hantash, F. M. , Goos, D. M. , Crossley, B. , Anderson, B. , Zhang, K. , Sun, W. , & Strom, C. M. (2011). FMR1 premutation carrier frequency in patients undergoing routine population‐based carrier screening: Insights into the prevalence of fragile X syndrome, fragile X‐associated tremor/ataxia syndrome, and fragile X‐associated primary ovarian insufficiency in the United States. Genetics in Medicine, 13, 39–45. [DOI] [PubMed] [Google Scholar]
- Haque, I. S. , Lazarin, G. A. , Kang, H. P. , Evans, E. A. , Goldberg, J. D. , & Wapner, R. J. (2016). Modeled fetal risk of genetic diseases identified by expanded carrier screening. Journal of the American Medical Association, 316, 734–742. [DOI] [PubMed] [Google Scholar]
- Hill, M. K. , Archibald, A. D. , Cohen, J. , & Metcalfe, S. (2010). A systematic review of population screening for fragile X syndrome. Genetics in Medicine, 12, 396–410. [DOI] [PubMed] [Google Scholar]
- Krishnamoorthy, K. , & Thomson, J. (2004). A more powerful test for comparing two Poisson means. Journal of Statistical Planning and Inference, 119, 23–35. [Google Scholar]
- Maenner, M. J. , Baker, M. W. , Broman, K. W. , Tian, J. , Barnes, J. K. , Atkins, A. , … Mailick, M. R. (2013). FMR1 CGG expansions: Prevalence and sex ratios. American Journal of Medical Genetics Part B: Neuropsychiatric Genetics, 162B(5), 466–473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McHugh, M. L. (2013). The chi‐square test of independence. Biochemia Medica, 23(2), 143–149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolin, S. L. , Glicksman, A. , Ding, X. , Ersalesi, N. , Brown, W. T. , Sherman, S. L. , & Dobkin, C. (2011). Fragile X analysis of 1112 prenatal samples from 1991 to 2010. Prenatal Diagnosis, 31, 925–931. [DOI] [PubMed] [Google Scholar]
- Raspa, M. , Edwards, A. , Wheeler, A. C. , Bishop, E. , & Bailey, D. B. Jr. (2016). Family communication and cascade testing for fragile X syndrome. Journal of Genetic Counseling, 25(5), 1075–1084. [DOI] [PubMed] [Google Scholar]
- Saul, R. A. , & Tarleton, J. C. (1998). FMR1‐related disorders . In Pagon R. A., Adam M. P., Ardinger H. H., Wallace S. E., Amemiya A., Bean L. J. H., … Stephens K. (Eds.), GeneReviews® [Internet] (pp. 1993–2017). Seattle, WA: University of Washington. [Google Scholar]
- Seltzer, M. M. , Baker, M. W. , Hong, J. , Maenner, M. , Greenberg, J. , & Mandel, D. (2012). Prevalence of CGG expansions of the FMR1 gene in a US population‐based sample. American Journal of Medical Genetics Part B, Neuropsychiatric Genetics, 159, 589–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sherman, S. , Pletcher, B. A. , & Driscoll, D. A. (2005). Fragile X syndrome: Diagnostic and carrier testing. Genetics in Medicine, 7, 584–587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tassone, F. , Iong, K. P. , Tong, T.‐H. , Lo, J. , Gane, L. W. , Berry‐Kravis, E. , … Hagerman, R. J. (2012). FMR1 CGG allele size and prevalence ascertained through newborn screening in the United States. Genome Medicine, 4, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weiss, K. , Orr‐Urtreger, A. , Kaplan Ber, I. , Naiman, T. , Shomrat, R. , Bardugu, E. , … Ben‐Shachar, S. (2014). Ethnic effect on FMR1 carrier rate and AGG repeat interruptions among Ashkenazi women. Genetics in Medicine, 16(12), 940–944. [DOI] [PubMed] [Google Scholar]
- Yrigollen, C. M. , Durbin‐Johnson, B. , Gane, L. , Nelson, D. L. , Hagerman, R. , Hagerman, P. J. , & Tassone, F. (2012). AGG interruptions within the maternal FMR1 gene reduce the risk of offspring with fragile X syndrome. Genetics in Medicine, 14(8), 729–736. [DOI] [PMC free article] [PubMed] [Google Scholar]