

Abstract
Objective
Objectification theory posits that self-objectification increases risk for disordered eating.
Method
The current study sought to examine the relationship between self-objectification and disordered eating using meta-analytic techniques.
Results
Data from 53 cross-sectional studies (73 effect sizes) revealed a significant moderate positive overall effect (r = 0.39), which was moderated by gender, ethnicity, sexual orientation, and measurement of self-objectification. Specifically, larger effect sizes were associated with female samples and the Objectified Body Consciousness Scale. Effect sizes were smaller among heterosexual men and African American samples. Age, body mass index, country of origin, measurement of disordered eating, sample type and publication type were not significant moderators.
Discussion
Overall, results from the first meta-analysis to examine the relationship between self-objectification and disordered eating provide support for one of the major tenets of objectification theory and suggest that self-objectification may be a meaningful target in eating disorder interventions, though further work is needed to establish temporal and causal relationships. Findings highlight current gaps in the literature (e.g., limited representation of males, and ethnic and sexual minorities) with implications for guiding future research.
Keywords: Objectification, disordered eating, body surveillance, sociocultural, meta-analysis, review
Introduction
While clinical diagnoses of anorexia nervosa, bulimia nervosa, and binge eating disorder are relatively rare, affecting roughly .09%, 1.5%, and 3.5% of women and .03%, .05%, and 2.0% of men respectively (Hudson, Hiripi, Pope, & Kessler, 2007), engagement in subclinical levels of disordered eating (e.g., skipping meals, use of weight loss pills or extreme diets, subthreshold levels of binging/purging, etc.) is alarmingly common in both males and females (Mintz & Betz, 1988; Mond et al., 2014). Eating disorders and disordered eating place individuals at risk for a number of negative health outcomes (Fairburn, Cooper, & Waller, 2008; Mehler, Birmingham, Crow, & Jahraus, 2010; Sharp & Freeman, 1993) and are associated with significant psychosocial impairment, high rates of comorbid psychopathology, and elevated mortality rates (Agras, et al., 2004; O’Brien & Vincent, 2003). As current intervention approaches are limited in their efficacy (Berkman et al., 2006; Keel & Haedt, 2008), identification of factors that may contribute to or maintain disturbed eating patterns represents an important area of inquiry with significant implications for intervention.
Research suggests that certain environments may increase vulnerability to the development of eating disorders and disordered eating (Striegel-Moore, Silberstein, & Rodin, 1986). In particular, accruing evidence suggests that environments that promote the importance of physical appearance significantly contribute to disordered eating attitudes and behaviors (Ata, Schaefer, & Thompson, 2014). Objectification theory (Fredrickson & Roberts, 1997), which originated within a feminist framework but has since been expanded to address eating disturbances observed in men, is a sociocultural theory of eating disturbance that attempts to explain how social environments in which the female form is viewed as an aesthetic object to be evaluated by others contributes to the disproportionately high rates of disordered eating observed in girls and women. The theory suggests that females in Western societies commonly experience instances of sexual objectification wherein “a woman’s sexual parts or functions are separated out from her person, reduced to status of mere instruments, or else regarded as if they were capable of representing her” (Bartky, 1990, p.35). Examples of such sexually-objectifying experiences include catcalls, leering or sexualized gaze, sexual comments, and media images highlighting the feminine form as an object of pleasure (Calogero, Tantleff-Dunn, & Thompson, 2011).
Objectification theory proposes that repeated exposure to sexually objectifying experiences and the broader societal reinforcement of the acceptability of such practices leads young girls and women to internalize these messages, learning to view their bodies from the external observer’s perspective and to conceptualize their own bodies as objects to be scrutinized by others (referred to as self-objectification) (Fredrickson & Roberts, 1997). Women who have adopted such a view are theorized to experience increased self-consciousness regarding their physical appearance, which manifests in heightened levels of self-surveillance or body-monitoring. In other words, sexual objectification refers to the interpersonal experience of having one’s body, appearance, or sexuality highlighted by another person or entity; self-objectification refers to a learned self-schema regarding the importance of one’s body and appearance relative to other aspects of the self; and self-surveillance represents the cognitive and behavioral manifestation of self-objectification characterized by self-conscious monitoring of one’s appearance (Fitzsimmons-Craft, 2011). Fredrickson and Roberts (1997) propose that the continual monitoring and evaluation of one’s appearance leads to a number of negative psychological outcomes including body shame and appearance anxiety, which then contribute to the development of disordered eating.
In the years following Fredrickson and Robert’s original publication, objectification theory has received a considerable amount of research attention and extant work suggests that the theory may provide a useful framework for understanding the process by which individuals develop disordered eating. Indeed, a growing body of research provides support for the relationship between self-objectification (or its manifestation self-surveillance) and disordered eating (Calogero, 2009; Daubenmier, 2005; Lindner, Tantleff-Dunn, & Jentsch, 2012; Noll & Fredrickson, 1998; Tiggemann & Slater, 2001; Tiggemann & Williams, 2012). Moreover, extant work suggests a possible moderating influence of several demographic and methodological variables.
Objectification theory posits that sexual and self-objectification is largely a female experience. Consistent with theory, research suggests that although boys and men report experiences of sexual objectification, girls and women endorse considerably higher levels of sexual and self-objectification (Bryant 1993; Klonoff, 2000; Kozee, Tylka, Augustus-Horvath, & Denchik, 2007; Murnen & Smolak, 2000; Swim, Hyers, Cohen, & Ferguson, 2001). Women also appear to be more sensitive to objectifying messages, exhibiting greater psychological impact when primed with objectifying words (Roberts & Gettman, 2004). In addition, rates of both diagnosable eating disorders and disordered eating appear to be higher among females than among males (Hudson et al., 2007), and some studies suggest that the relationship between self-objectification and disordered eating may be stronger among females (Calogero, 2009). Therefore, it is possible that gender moderates the relationship between self-objectification and disordered eating.
Although the majority of the work examining self-objectification has utilized college samples, limited work using adolescent and older community samples indicates that levels of objectification among adolescent girls (age 12 to 16) may be similar to levels observed in undergraduate women (Slater and Tiggemann, 2002), but subsequently decline with increasing age (Greenleaf, 2005; Roberts, 2004; Tiggemann & Lynch, 2001). Prevalence of disordered eating appears to increase through adolescence and decline in adulthood (Heatherton, Mahamedi, Striepe, Field, & Keel, 1997; Jones, Bennett, Olmsted, Lawson, & Rodin, 2001; Polivy & Herman, 1985). Further, this is some indication that the relationship between self-objectification and disordered eating may vary with age (Greenleaf, 2005). It is therefore possible that age may moderate the relationship between self-objectification and disordered eating.
Research indicates that rates of eating pathology and associated risk factors may vary across ethnicity (Cachelin, Rebeck, Chung, & Pelayo, 2002; Field, Camargo, Taylor, Berkey, & Colditz, 1999; Gray, Ford, & Kelly, 1987; McKnight Risk Factor Study, 2000; Powell & Kahn, 1995; Wildes, Emery, & Simons, 2001; Winkleby, Gardner, & Taylor, 1996), and accruing evidence suggests that ethnicity may moderate relationships between established risk factors and engagement in disordered eating (Rancourt, Schaefer, Bosson, & Thompson, 2016; Schaefer, Thibodaux, Krenik, Arnold, & Thompson, 2015). Further, available research indicates that levels of self-objectification may differ among ethnic groups (Breitkopft, Littleton, & Berenson, 2007). In light of these findings, it is possible that ethnicity may moderate the relationship between self-objectification and disordered eating.
Objectification theory rests on the assumption that women are viewed as sexual objects for male pleasure. Thus, researchers have suggested that the tenets of objectification theory may apply primarily to heterosexual women who may be more likely to self-objectify in order to garner male attention (Tiggemann, 2011). Investigators have recently begun to examine the role of sexual orientation in self-objectification processes and disordered eating, with findings suggesting that the impact of sexual orientation may differ for men and women (Engeln-Maddox, Miller, & Doyle, 2011; Haines et al., 2008; Kozee and Tylka, 2006). Studies using male samples indicate that homosexual men evidence higher levels of self-objectification (Engeln-Maddox et al., 2011; Kozak, Frankenhauser, & Roberts, 2009) and disordered eating (Boroughs & Thompson, 2002; Martins, Tiggemann, & Kirkbride, 2007) compared to heterosexual men, while studies using female samples generally indicate comparable levels of self-objectification (Lyders, 1999) and disordered eating (Brand, Rothblum, & Solomon, 1992; Striegel-Moore, Tucker, & Hsu, 1990) among homosexual and heterosexual women. Limited research has examined the influence of sexual orientation on the relationships between self-objectification and disordered eating (Lyders, 1999; Martins et al., 2007), however findings suggest that sexual orientation may moderate the relation between self-objectification and disordered eating, especially among males.
Elevated body mass index (BMI) has been shown to predict increases in several risk factors for disordered eating, as well as the onset of bulimic pathology, binge eating, and eating disorder symptoms (Killen et al., 1994; Stice, Presnell, & Spangler, 2002; Vogeltanz-Holm et al., 2000; Wichstrom, 2000). Moreover, BMI has been shown to moderate the relations between several putative risk factors and disordered eating (Rukavina & Pkrajac-Bulian, 2006). As self-objectification is a theorized risk factor for disordered eating, it is possible that BMI may similarly moderate the association between self-objectification and disordered eating such that higher BMI will be associated with a stronger relationship between self-objectification and disordered eating.
Research has demonstrated cross-cultural differences in levels of established risk factors for eating disorders, such as internalization of appearance ideals and appearance related pressures, as well as differences in the strength of associations between putative risk factors and disordered eating (Schaefer et al., 2013). Western appearance ideals emphasize the importance thinness for women, and research suggests that disordered eating behaviors such as binging and purging may be culturally-bound, appearing largely within cultures exposed to Western beauty ideals (Keel & Klump, 2003). Although the majority of the work examining objectification theory has been conducted utilizing samples from the United States, Australia, and Britain (Calogero, 2009; Calogero & Thompson, 2009; Moradi & Huang, 2008), recent work suggests that levels of self-objectification may vary by country (Loughnan et al., 2015). Similar to other environmental risk factors, it is possible that country of origin (here, used as a proxy for one’s cultural context) may also moderate the relation between self-objectification and disordered eating such that a stronger association will be observed among samples from Western countries compared with non-Western countries.
Numerous studies conducted within non-clinical samples suggest a relationship between self-objectification and disordered eating (Lindner et al., 2012; Noll & Fredrickson, 1998; Tiggemann & Slater; 2001). The presence of significant psychopathology, particularly eating pathology, is likely to increase the strength of the association between self-objectification and disordered eating. Therefore, clinical samples comprised of individuals with diagnosed eating disorders may yield stronger effect sizes compared with non-clinical samples. Similarly, as college women have been found to exhibit heightened levels of disordered eating (Hesse-Biber, Marino, & Watts-Roy, 1999; Pyle, Neuman, Halvorson, & Mitchell, 1991), it is possible that the association between self-objectification and disordered eating may be stronger among this group compared to community samples.
Currently, there are two validated and widely-used measures of self-objectification: the Self-Objectification Questionnaire (SOQ; Noll & Fredrickson, 1998) and the Body Surveillance subscale of the Objectified Body Consciousness Scale (OBCS-BS; McKinley & Hyde, 1996). The SOQ assesses the degree to which respondents value observable physical attributes (e.g., physical attractiveness) over non-observable competence-based physical attributes (e.g., physical coordination). The OBCS Body Surveillance subscale assesses the degree to which the respondent engages in habitual monitoring of his or her appearance. Researchers have suggested that “valuing the body as a physical object [as measured by the SOQ] and behaviorally investing in the body as a physical object [as measured by the OBCS] are not the same phenomenon” (Calogero, 2011). Indeed, several studies have demonstrated that self-objectification measured by the SOQ and self-surveillance measured by the OBCS are conceptually and empirically distinguishable concepts that produce different patterns of relations with disordered eating (Greenleaf & McGreer, 2006; Hill & Fischer, 2008; Kozee & Tylka, 2006; Steer & Tiggemann, 2008; Tiggemann & Slater, 2001). Therefore, it is likely that the measure of objectification will moderate the relation between self-objectification and disordered eating.
The Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) currently recognizes three eating disorders with distinct patterns of eating behavior. Anorexia nervosa is characterized by extreme dietary restriction resulting in significantly below average weight. Bulimia nervosa is characterized by recurrent episodes of binge eating followed by compensatory behavior aimed at preventing weight gain (e.g., use of vomiting or laxatives). Finally, binge-eating disorder is characterized by binge eating without compensatory behaviors. Researchers have identified common and unique risk factors associated with these various expressions of disordered eating (Jacobi, Hayward, de Zwaan, Kraemer, & Agras, 2004). Therefore, it is possible that measures assessing anorectic, bulimic, binge eating, or global symptoms of eating pathology may exhibit different patterns of relations with self-objectification.
Demonstrated biases towards publishing manuscripts that report significant results (Dickersin, 2005; Easterbrook, Berlin, Gopalan, & Matthews, 1991) may result in differences in effect sizes between unpublished work (e.g., unpublished manuscripts, dissertations, and theses) and published manuscripts. It is therefore possible that published studies demonstrate stronger associations than unpublished studies.
The Current Study
A number of excellent narrative reviews highlight the wealth of evidence linking self-objectification to disordered eating (e.g., Moradi & Huang, 2008; Tiggemann, 2013). However, these findings have not yet been synthesized through a quantitative review. Meta-analysis provides a powerful means of synthesizing results from a series of studies on a given topic. This approach allows researchers to estimate the strength of the relationship between two variables in the population, to examine hypothesized moderators of that association, and to identify research questions that require further attention (Borenstein, Hedges, Higgins, & Rothstein, 2009). Therefore, the primary goal of the current study was to examine the association between self-objectification and disordered eating using meta-analytic techniques. A secondary goal of the study was to examine demographic and methodological characteristics that may modulate this association.
Method
Locating Studies
A literature search was conducted using PsycINFO and ProQuest Dissertations and Theses Online to identify relevant studies that examined the relationship between self-objectification and disordered eating. Search terms included self-objectification, self-surveillance, Self-Objectification Questionnaire, Objectified Body Consciousness Scale and eating disorder*. Reference sections of retained studies were also reviewed to identify additional articles for inclusion. Search returns were screened to eliminate duplicate studies. Next the full text of each study was evaluated to determine eligibility for inclusion in the meta-analysis. Studies were eligible for inclusion in the analysis if they met the following criteria: (1) included a validated measure of self-objectification (i.e., Self-Objectification Questionnaire or Objectified Body Consciousness Scale – Body Surveillance subscale), (2) included a validated measure of disordered eating, and (3) were written in English, although country of origin was not restricted. The current meta-analysis focused exclusively on cross-sectional studies given methodological difficulties associated with assessing disordered eating in laboratory settings, significant variation in the methods used to induce self-objectification, and the limited number of experimental or longitudinal studies available. Finally, all studies were examined for the inclusion of sufficient data to calculate an effect size. If sufficient data was not available from either the text or the corresponding author, the study was excluded from the meta-analysis. Figure 1 provides a flow diagram of the study selection process based on the PRISMA guidelines.
Figure 1.
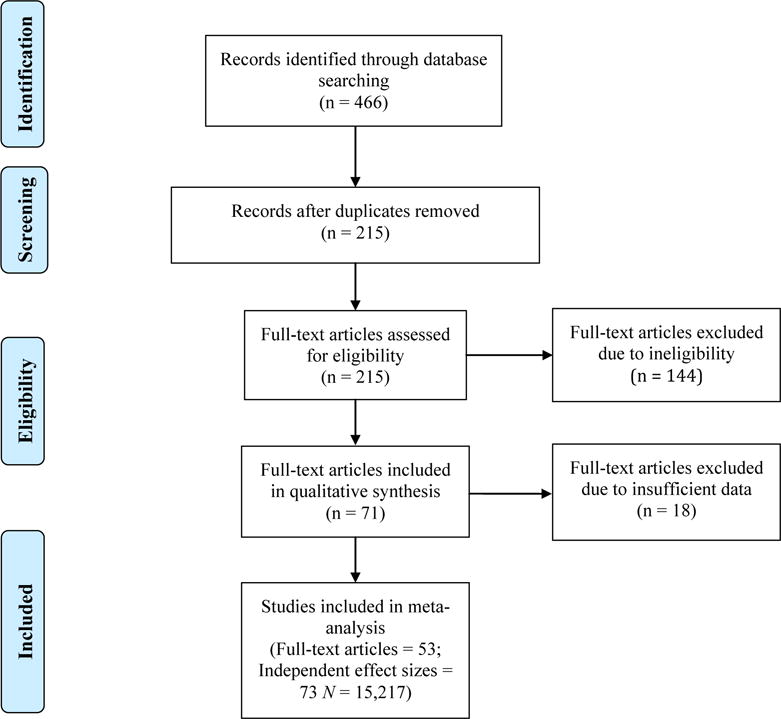
Flow Diagram of Study Selection
Coding of Study Variables
Each study was coded for the following information: (1) sample size, (2) gender, (3) mean age of sample, (4) primary ethnic group, (5) primary sexual orientation of sample, (6) mean BMI of sample, (7) country of origin, (8) sample type, (9) self-objectification measure, (10) measurement of disordered eating, (11) publication, and (12) effect size (r). All studies were double-coded by the primary author and a trained research assistant, allowing for a 100% reliability check on the data. Inter-rater agreement was assessed with the kappa coefficient for categorical variables and with the intraclass correlation coefficient for continuous variables. Instances where raters did not agree were resolved through discussion and consensus.
As outlined above, several demographic variables were coded for each study. For gender, studies were coded to indicate inclusion of all males, all females, or both genders. If both genders were included in a single study, effect sizes were considered separately for each gender if they were reported separately in the study. If the study included both genders and did not analyze results separately for each gender, the study was coded as including both genders. Age was considered as a continuous variable and the mean age of the sample was coded for each study. Ethnicity was considered as a categorical variable and each study was coded to reflect the dominant ethnic group represented in the sample. Studies were also coded to reflect the dominant sexual orientation of participants in the sample (i.e., heterosexual male/female, homosexual male/female, or mixed/unknown sexual orientation). BMI was considered as a continuous variable and mean sample BMI was recorded for each study. Country of origin was coded to assess the impact of regional/cultural differences on the association between variables of interest.
With regard to methodological moderators, the population from which the sample was drawn was recorded. Specifically, studies were coded as including samples from community, college, or clinical settings. If a study included groups drawn from different populations (e.g., community and clinical), results from each sample were coded separately if possible. All studies were coded to indicate the self-objectification measure utilized. When studies used both the Self-Objectification Questionnaire and Objectified Body Consciousness Scale – Body Surveillance subscale, both effect sizes were recorded and the average effect size calculated for inclusion in the meta-analysis. Consistent with previous meta-analyses examining correlates of disordered eating (Menzel et al., 2010; Stice, 2002), the eating disorder measures utilized were coded to indicate a focus on anorectic symptoms (e.g., Eating Disorder Inventory – Drive for Thinness subscale), bulimic symptoms (e.g., Eating Disorder Inventory – Bulimia subscale), binge eating symptoms (e.g., Binge Eating Scale), or a composite variable representing overall eating disorder symptomatology (e.g., Eating Disorder Examination Questionnaire – Global Scale). When multiple measures were utilized, the effect sizes were averaged for the calculation of the summary effect. Finally, studies were coded to reflect publication type. Both published studies and unpublished theses/dissertations were included in the analysis, however, if any portion of the thesis/dissertation was published, only the published article was used.
Calculation of Summary Effect Size
As each study included in the meta-analysis was correlational, the Pearson correlation coefficient (r) was used as the index of effect size. If the effect size was not included in the article or could not be calculated from the data presented, authors were contacted in order to obtain the relevant information. If a study yielded more than one independent effect size (e.g., effect size for women and men), these studies were coded separately. Computation of the summary effect size utilized the meta-analytic approach outlined by Hedges and Olkin (1985). Independent effect sizes were converted to z using Fisher’s r to z transformation (Fisher, 1970) and weighted by their inverse variance. The summary effect was calculated using a random-effects model. The random effects model was chosen for two reasons: (1) It was expected that the true effect size would vary across studies due to differences in sample characteristics, and (2) a random effects model would allow the findings of the current meta-analysis to be generalized beyond those studies that were included in the analysis (Borenstein, Hedges, Higgins, & Rothstein, 2009). The obtained summary effect was then transformed back from z to r for interpretation and reporting. According to guidelines set forth by Cohen (1988), effect sizes of .10, .30, and .50 are considered small, medium, and large, respectively. Effect sizes smaller than .05 were considered trivial. All analyses were completed using Comprehensive Meta-Analysis, Version 2.0 (Borenstein, Hedges, Higgins, & Rothstein, 2005).
Moderator Analyses
As discussed, the random-effects model for computing the overall summary effect size presumes that the true effect size may vary from study to study. Between study variation in effect sizes arises from two sources: 1) differences in the true effect size and 2) random error. In meta-analysis, Cochran’s heterogeneity statistic Q is used to quantify the amount of between study variation (Cochran, 1954). A statistically significant Q statistic suggests that there is significant heterogeneity in the observed study effect sizes. In other words, the between study variation in effect sizes is greater than one would be expected based on random error alone.
Moderator analyses are conducted to identify sources of between study variation. Moderator analyses for categorical variables were conducted using analog to ANOVA. A mixed effects model, which is generally recommended and allows for some true variation in effects within a subgroup, was utilized (Borenstein, Hedges, Higgins, & Rothstein, 2009). Similar to ANOVA within a single primary analysis, analog to ANOVA analyses provide information regarding both within group variance (Qwithin) and between group variance (Qbtwn). A significant Qbtwn suggests that there are significant differences in the true effect size between groups.
Continuous moderators were examined using meta-regression. A random-effects model, which is recommended when it is likely that the impact of the examined moderator captures some but not all of the true variation among effects, was used to examine the impact of the moderator on the relationship between self-objectification and disordered eating. When meta-regression is performed, significant moderation is indicated by a significant slope, similar to regression in a primary study.
Publication Bias
As discussed, research suggests that studies reporting larger effect sizes and/or significant results are more likely to be published compared with studies that report smaller effect sizes and/or non-significant results (Dickersin, 2005). This bias in the published literature is likely to be reflected in meta-analytic procedures, which primarily utilize published data. In the current study, publication bias was assessed via Orwin’s (1983) Fail-safe N analysis, which determines the number of studies with an effect size of zero that would be needed to reduce the summary effect size to a trivial amount (i.e., r = .05). Additionally, the funnel plot, which presents a visual display of the relationship between effect size and standard error, was also used to assess publication bias. Funnel plots have a symmetrical funnel shape with equal numbers of studies falling above and below the obtained summary effect when publication bias is not present. A lack of symmetry in the plot suggests publication bias. Duval and Tweedie’s trim and fill procedure (2000a; 2000b)can be used to correct this bias by imputing “missing” studies and recalculating a new unbiased summary effect.
Results
Fifty-three manuscripts yielded 73 independent effect sizes (N = 15,217). Appendix A presents the effect sizes (r) and study characteristics for each study examined in the current analysis. Inter-rater reliability was good to excellent for all study variables with coefficients ranging from .84 to 1.00. Figure 2 presents the forest plot of the correlations between self-objectification and disordered eating.
Figure 2.
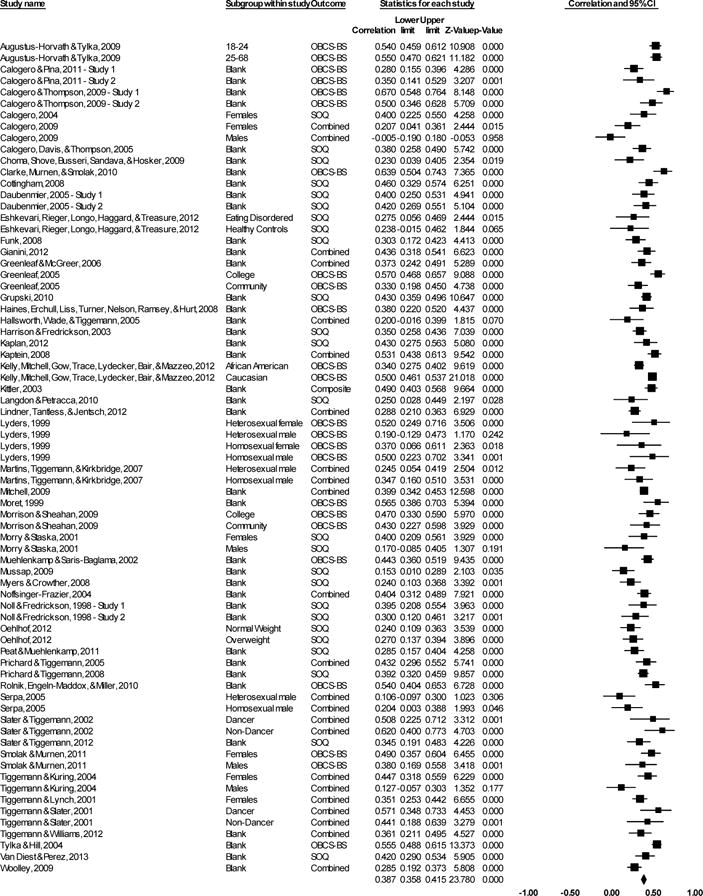
Forest plot of the correlations between self-objectification and disordered eating
Summary Effect
The overall summary effect was r = 0.39, z = 23.78, p < .001 (95% confidence interval [CI]: .36 to .42). According to Cohen’s (1988) guidelines, this exceeds the convention for medium effect sizes (.30). The effect was marked by significant heterogeneity, Q(72) = 274.75, p < .001, suggesting the presence of potential moderating factors.
Gender
Sixty-three effect sizes reflected the relationship between self-objectification and disordered eating in females. Ten effect sizes reflected the relationship between self-objectification and disordered eating in males. There were no studies that examined the relationship between self-objectification and disordered eating in mixed gender samples. The point estimate for females was r = 0.41, z = 25.73, p < .001 (95% CI: .38 to .44). The point estimate for males was r = 0.20, z = 4.57, p < .001 (95% CI: .11 to .28). Differences between groups were significant, Qbtwn(1) = 46.94, p < .001, suggesting that the relationship between self-objectification and disordered eating is stronger among women.
Age
Sixty-five effect sizes were included in the analysis to examine mean age as a potential moderator of the relationship between self-objectification and disordered eating. Eight studies were excluded from the analysis as they did not report a mean sample age. Results revealed that mean age was not a significant moderator, slope = -.002, SEslope = .001, p = .200. In light of research suggesting that disordered eating and self-objectification may increase through adolescence and decrease in adulthood (Heatherton et al., 1997; Tiggemann & Lynch, 2001), the scatterplot was examined for evidence of a possible u-shaped or non-linear relationship between age and effect size. Visual inspection of the scatterplot did not support a non-linear relationship.
Ethnicity
Many studies (k = 17) did not report sample demographics related to race/ethnicity and were therefore excluded from relevant moderator analyses. Among effect sizes for which race/ethnicity data was provided (k = 55), 52 effect sizes were computed using primarily Caucasian participants, two effect sizes were computed using primarily African American/Black participants, and one effect size was computed using Asian American participants. When all genders were included, the point estimate for studies utilizing primarily Caucasian samples was r = 0.41, z = 21.40, p < .001 (95% CI: .38 to .45). The point estimate for studies utilizing primarily African American samples was r = 0.34, z = 11.92, p < .001 (95% CI: .29 to .39). The observed effect for the single study utilizing a primarily Asian American sample was 0.42, z = 5.14, p < .001 (95% CI: .27 to .55). Differences between groups were marginally significant, Qbtwn(2) = 5.21, p = 0.074. Given research suggesting that ethnic differences in disordered eating may vary across genders (Croll, Neumark-Stzainer, Story, & Ireland, 2002; Field, Camargo, Taylor, Berkey, & Colditz, 1999; Gray, Ford, & Kelly, 1987; Kelly, Cottern, Tanofsky-Kraff, & Mazzea, 2015; Wildes, Emery, & Simons, 2001), the impact of ethnicity was also examined among males and females separately. When analyses were restricted to include only female samples, ethnicity significantly moderated the association between disordered eating and self-objectification, Qbtwn(2) = 6.348, p = 0.039. The point estimate for Caucasian females was r = 0.42, z = 21.96, p < .001 (95% CI: .39 to .45). The point estimate for Asian American females was r = 0.42, z = 5.14, p < .001 (95% CI: .27 to .55). The point estimate for African American females was r = 0.34, z = 11.91, p < .001 (95% CI: .29 to .39). All male samples were primarily Caucasian and therefore moderator analyses were not conducted to examine the impact of ethnicity among men. Results suggest that the relationship between self-objectification and disordered eating is moderated by ethnicity for women. In particular, the relationship was strongest among primarily Caucasian and Asian American samples of women and weakest among primarily African American samples of women.
Sexual Orientation
The majority of studies (k = 58) did not report sample demographics related to sexual orientation and were therefore excluded from relevant moderator analyses. Seven studies utilized samples primarily comprised of heterosexual females, three primarily utilized heterosexual males, two primarily utilized homosexual females, and three studies utilized samples primarily comprised of homosexual males. The point estimate for heterosexual females was r = 0.39, z = 11.30, p < .001 (95% CI: .33 to .45). The point estimate for heterosexual males was r = 0.23, z = 3.51, p < .001 (95% CI: .10 to .35). The point estimate for homosexual females was r = 0.38, z = 5.03, p < .001 (95% CI: .24 to .50). The point estimate for homosexual males was r = 0.32, z = 4.65, p < .001 (95% CI: .19 to .44). Differences between groups were significant, Qbtwn(3) = 7.91, p = 0.048, suggesting that the relationship between self-objectification and disordered eating is moderated by sexual orientation. In particular, the relationship appears to be strongest among heterosexual women and weakest among heterosexual males.
Body Mass Index
Forty-eight effect sizes were included in the analysis to examine mean BMI as a potential moderator of the relationship between self-objectification and disordered eating. Twenty-four studies were excluded from the analysis as they did not report a mean sample BMI. Results reveal that mean BMI was not a significant moderator, slope = −0.01, SEslope = .001, p = .483.
Country of Origin
As all studies reported information regarding the country of origin, all effect sizes (k = 73) were included in the relevant moderator analyses. Forty-four studies utilized samples from the United States, fifteen utilized samples from Australia, seven utilized samples from England, two studies utilized samples from Ireland, two studies utilized samples from Canada, and one study utilized a sample drawn from both the United States and Canada. The point estimate for the United States was r = 0.41, z = 20.62, p < .001 (95% CI: .37 to .44). The point estimate for Australia was r = 0.36, z = 10.41, p < .001 (95% CI: .30 to .42). The point estimate for England was r = 0.27, z = 4.30, p < .001 (95% CI: .15 to .38). The point estimate for Ireland was r = 0.46, z = 7.14, p < .001 (95% CI: .34 to .56). The point estimate for Canada was r = 0.35, z = 3.50, p < .000 (95% CI: .16 to .52). The observed effect size for the combined United States and Canada sample was r = 0.40, z = 7.92, p < .001 (95% CI: .31 to .49). Differences between groups were not significant, Qbtwn(5) = 8.46, p = 0.132, suggesting that the relationship between self-objectification and disordered eating did not differ among the countries assessed in this analysis.
Sample Type
All studies reported information regarding the type of sample utilized and therefore all studies (k = 73) were included in the relevant moderator analyses. Forty-one studies utilized college samples, twenty utilized community samples, nine utilized samples drawn from both college and community populations, two studies utilized samples drawn from eating disorder clinical populations, and one study utilized a sample drawn from a general clinical population. The point estimate for college samples was r = 0.40, z = 14.38, p < .001 (95% CI: .36 to .43). The point estimate for community samples was r = 0.35, z = 14.01 p < .001 (95% CI: .31 to .40). The point estimate for college/community samples was r = 0.39, z = 6.46, p < .001 (95% CI: .28 to .49). The point estimate for eating disorder clinical samples was r = 0.35, z = 6.18, p < .001 (95% CI: .25 to .45). The observed for the general clinical sample was r = 0.57, z = 5.39, p < .000 (95% CI: .39 to .70). Differences between groups were not significant, Qbtwn(4) = 6.41, p = 0.171, suggesting that the relationship between self-objectification and disordered eating did not differ among college, community, and clinical samples.
Measurement of Self-Objectification
All studies (k = 73) reported information regarding the measure used to assess objectification. Twenty-five studies utilized the SOQ exclusively, while 24 studies utilized the OBCS-BS exclusively. Twenty-four studies utilized both the OBCS-BS and SOQ yielding an average composite effect. One such study created an objectification composite score and provided the correlation with measures of disordered eating; the remaining 23 studies provided correlations between the individual measures of self-objectification and disordered eating, which were averaged to provide a composite effect. The point estimate for studies using the OBCS-BS was r = 0.48, z = 18.21, p < .001 (95% CI: .43 to .52). The point estimate for studies using the SOQ was r = 0.34, z = 17.99 p < .001 (95% CI: .30 to .37). The observed effect for the study that utilized a composite of both the OBCS-BS and SOQ was r = 0.49, z = 9.66, p < .001 (95% CI: .40 to .57). Finally, the point estimate for studies in which both the OBCS-BS and SOQ were utilized and the resultant effects averaged for use in the current meta-analysis was r = 0.34, z = 12.01, p < .001 (95% CI: .29 to .40). In order to assess the moderating influence of self-objectification measure, studies that utilized multiple measures were removed from moderator analyses. There was a significant difference in effect sizes obtained from studies utilizing the OBCS-BS compared with studies utilizing the SOQ, Qbtwn(1) = 22.48, p < 0.001. Specifically, larger effect sizes were observed among studies utilizing the OBCS-BS, while smaller effect sizes were observed among studies utilizing the SOQ.
Measurement of Disordered Eating
All studies (k = 73) were included in the moderator analyses to examine possible differences in effect size across type of eating disorder symptoms. Twelve studies assessed anorectic/restrictive symptoms, two studies assessed bulimic symptoms, and 59 studies assessed global eating disorder symptoms (i.e., restrictive behaviors, binge/purge behaviors, and body image concerns). The point estimate for studies assessing anorectic/restrictive symptoms was r = 0.37, z = 8.96, p < .001 (95% CI: .29 to .44). The point estimate for studies assessing bulimic symptoms was r = 0.33, z = 2.65, p = .008 (95% CI: .09 to .53). The point estimate for studies assessing global eating disorder symptoms was r = 0.39, z = 21.67, p = .008 (95% CI: .36 to .42). There was not a significant difference among effect sizes observed in studies assessing anorectic/restrictive, bulimic, or global eating disorder symptoms Qbtwn(2) = 0.64, p = 0.726.
Publication Type
All studies (k = 73) were included in the moderator analyses to assess the effect of publication type on the relationship between self-objectification and disordered eating. Fifty-eight journal articles and 15 dissertations were examined. The point estimate for journal articles was r = 0.39, z = 20.03, p < .001 (95% CI: .35 to .42). The point estimate for dissertations was r = 0.38, z = 12.74 p < .001 (95% CI: .33 to .43). Effect sizes extracted from journal articles were not significantly different from those extracted from dissertations Qbtwn(1) = 0.07, p = 0.793.
Publication Bias
Orwin’s Fail-safe N analysis indicated that 547 additional studies with a mean effect of zero would be needed to reduce the summary effect to a trivial effect size (i.e., r = .05). Examination of the funnel plot (Figure 3) indicates that the effect sizes were largely symmetrically distributed around the summary effect. Duval and Tweedie’s trim and fill procedure did not identify any “missing” studies. Therefore, the adjusted or unbiased summary effect computed using a random effects model was equivalent to the observed summary effect.
Figure 3.
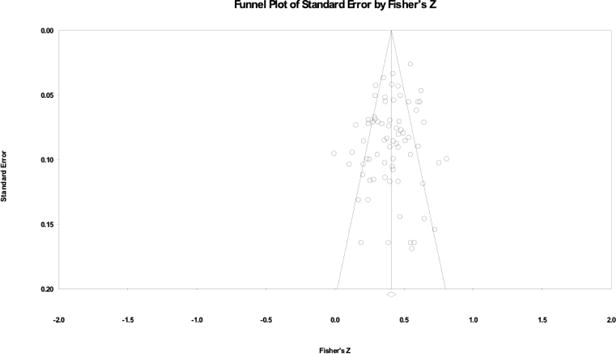
Funnel plot of observed effects
Discussion
Objectification theory implicates self-objectification in the etiology of disordered eating and numerous studies have sought to examine the relationship between these constructs empirically. Results from the current meta-analysis suggest a positive, moderate, and significant (r = .39) bivariate relationship such that greater objectification of one’s body is related to higher levels of disordered eating attitudes and behaviors. Importantly, the magnitude of this effect is similar to effect sizes observed in meta-analyses examining other established risk factors and correlates of disordered eating, including appearance comparisons (Meyers & Crowther, 2009), weight teasing (Menzel et al., 2010), perceived pressures for thinness, and thin ideal internalization (Stice, 2002).
Moderators of the Relationship Between Self-Objectification and Disordered Eating
The overall summary effect was characterized by significant heterogeneity. Subsequent analyses indicated that several moderator variables including gender, ethnicity, sexual orientation, and the measurement of self-objectification may partially account for this heterogeneity. Mean sample age, mean sample BMI, country of origin, sample type, measurement of disordered eating, and publication type were not significant moderators.
As expected, there was a stronger relationship between self-objectification and disordered eating for women compared with men. These results may not be surprising in light of research indicating that women are more consistently objectified in media, report more objectifying experiences and self-objectification, more frequently feel evaluated solely based on their physical appearance, and experience a greater impact when exposed to objectifying messages (Archer, Iritani, Kimes, & Barrios, 1983; Bryant 1993; Fredrickson & Roberts, 1997; Klonoff, 2000; Kozee, Tylka, Augustus-Horvath, & Denchik, 2007; Murnen & Smolak, 2000; Swim, Hyers, Cohen, & Ferguson, 2001; Unger & Crawford, 1996). Indeed, objectification theory derives from a feminist framework that attempts to explain how women’s gendered experiences contribute to their elevated rates of disordered eating. Importantly, although considerably fewer studies examined the relationships of interest in male samples, the cumulative results suggest the potential role of self-objectification in disordered eating among men as well as women. In particular, moderator analyses suggest that this association may be especially strong for homosexual males (further discussed below). The current analysis highlights the importance of self-objectification processes in disordered eating among women, the potential role of these processes among men, and the need for further work among males.
Although previous meta-analyses examining the relationship between proposed risk factors (e.g., appearance comparisons, exposure to thin media images, weight-related teasing) and disordered eating have found a moderating influence of age, such that effect sizes are larger among younger samples (Groesz, Levine, & Murnen, 2002; Menzel et al, 2010; Myers & Crowther, 2009), age was not a significant moderator in the current study. While the range of mean sample age was somewhat limited (lowest mean sample age: 13.40, highest mean sample age: 48.95), results suggest that self-objectification is as strongly related to disordered eating among adolescents as it is among young and middle-aged adults. Limited research among adult women aged 18 to 84 has found that levels of self-objectification and disordered eating decrease with age, and that self-objectification may mediate the relationship between age and disordered eating (Tiggemann & Lynch, 2001). This finding, paired with the current meta-analytic results, suggest that changes in self-objectification may play an important role in the etiology, maintenance, and remittance of disordered eating across age groups, though longitudinal work is needed to examine these prospective associations. Additional work utilizing adolescent and older adult samples is also encouraged.
Ethnicity emerged as a marginally significant moderator when male and female samples were considered together, with primarily Caucasian and Asian American samples evidencing the largest effect sizes and African American samples evidencing smaller effect sizes. When the moderating influence of ethnicity was examined among female samples alone, ethnicity significantly moderated the association between self-objectification and disordered eating. Again, Caucasian and Asian American women evidenced the largest effect sizes, with African American women evidencing smaller effect sizes. As all male samples were primarily Caucasian, moderator analyses were not conducted for males. Importantly, very few studies (k = 3) were conducted within primarily non-Caucasian (i.e., African American and Asian American) samples, and samples representing additional ethnic groups (e.g., Hispanic) were not available. Therefore, results must be interpreted in light of these significant limitations. On a methodological level, many studies did not report information regarding race/ethnicity. As research increasingly suggests the importance of examining ethnicity in the etiology, maintenance, and treatment of disordered eating (Bucchianeri, Fernandes, Loth, Hannan, Eisenberg, & Neumark-Sztainer, 2015; Kelly et al., 2015), inclusion of information regarding the ethnic composition of the sample is encouraged. Overall, findings indicate a possible influence of ethnicity and highlight the need for further work examining the constructs of interest in ethnic minority groups.
Sexual orientation significantly moderated the relationship between self-objectification and disordered eating. Point estimates were highest for heterosexual and homosexual women, followed by homosexual males. Effect sizes were weakest among heterosexual males. Previous research suggests that heterosexual and homosexual women report comparable levels of disordered eating and results from the current study suggest that that self-objectification may play an equally important role in understanding the etiology and maintenance of maladaptive eating patterns in these groups. Interestingly, results among males suggest that self-objectification may play a larger role in disordered eating attitudes and behaviors for homosexual men compared with heterosexual men. Consistent with Objectification Theory’s assertion that “male gaze” contributes to experiences of sexual and self-objectification among women (Fredrickson & Roberts, 1997), it is possible that this same phenomenon similarly contributes to objectification experiences among homosexual men. As homosexual men evidence higher levels of both disordered eating and self-objectification compared to heterosexual men (Boroughs & Thompson, 2002; Engeln-Maddox et al., 2011; Kozak et al., 2009; Tiggemann et al., 2007), prevention and treatment interventions aimed at this population may consider self-objectification as a particularly relevant treatment target. Results also suggest the importance of reporting such demographic information in research related to the constructs of interest.
BMI did not moderate the association between self-objectification and disordered eating, suggesting that a tendency to self-objectify and engage in habitual body monitoring is moderately related to disordered eating across the BMI spectrum. Notably, the majority of studies reported mean BMIs in the normal range (18.5 to 25.0) and only one study utilized a sample comprised of obese individuals, restricting the range of BMI examined in the current analysis. As elevated BMI is associated with disordered eating and its risk factors (Killen et al., 1994; Stice et al., 2002; Vogeltanz-Holm et al., 2000; Wichstrom, 2000), further evaluation in individuals with overweight and obesity may be warranted.
Country of origin was not a significant moderator in the current study. Notably, however, all studies were conducted with samples drawn from Western industrialized countries (i.e., United States, Australia, England, Ireland, Canada) where rates of disordered eating and associated risk factors (e.g., emphasis on a thin body ideal) are relatively homogeneous (Mautner, Owen, & Furnham, 2000; Swami et al., 2010). As research indicates that rates of disordered eating and associated risk factors are typically higher in Western compared with Eastern societies (Keel & Klump, 2003; Miller & Pumariega, 2001), it is possible that effect sizes may differ in non-Western samples. Therefore, examination of the relationship between self-objectification and disordered eating in non-Western cultures is an area for future investigation.
Sample type was also not a significant moderator in the current analysis, suggesting that the relationship between self-objectification and disordered eating may be consistent across college, community, clinical eating disorder, and general clinical samples. It is therefore possible that self-objectification processes are equally impactful regardless of the presence of an eating disorder diagnosis. Alternatively, it is possible that results may be due to methodological artifact. Only two studies examined the constructs of interest within samples of individuals with diagnosed eating disorders. Both of these studies assessed self-objectification via the SOQ, which moderator analyses suggest is associated with smaller effect sizes. Among college, community, and general clinical samples, self-objectification was often assessed via the OBCS-BS, which may yield higher effect sizes. Future work with clinical samples may seek to include the OBCS-BS in order to capture the self-monitoring aspect of self-objectification, which appears to be more closely associated with disordered eating.
Consistent with researchers’ assertions that an objectifying orientation towards the self and habitual body monitoring represent distinct constructs (Calogero, 2011), the OBCS-BS and SOQ produced significantly different mean effect sizes in the current meta-analysis. Specifically, the OBCS-BS was associated with larger effect sizes compared with the SOQ. These results suggest that the degree to which an individual engages in habitual monitoring of his or her appearance is more predictive of disordered eating than the degree to which an individual values his or her observable physical attributes over non-observable competence-based physical attributes. It is possible that the attitudinal aspect of self-objectification (as measured by the SOQ) developmentally precedes the behavioral manifestation of self-objectification (as measured by the OBCS-BS), such that habitual monitoring represents a more proximal etiological factor. Longitudinal data and meditational models are needed to examine this potential etiological model.
Previous meta-analytic work suggests that associations with some proposed risk factors may vary across anorectic, bulimic, and binge eating pathology (Stice, 2002), while other risk factors demonstrate consistent associations with distinct forms of eating pathology (Menzel et al., 2010). In the current study, measurement of disordered eating did not emerge as a significant moderator, suggesting that self-objectification is comparably related to disordered eating when assessed via measures of anorectic, bulimic, and global eating pathology. Notably, most effect sizes reflected general eating pathology symptoms either through the use of a global measure (e.g., the Eating Disorder Examination Questionnaire) or through the averaging of measures reflecting anorectic and bulimic symptoms (e.g., Eating Disorder Inventory – Drive for Thinness subscale and Eating Disorder Inventory – Bulimia subscale), which may have obscured possible differences in effect sizes. Future work should examine this possibility. Additionally, there were no studies that examined associations with measures of binge eating symptoms, highlighting a complementary area for future investigation. As binge eating disorder may be less closely associated with overvaluation of shape/weight and preoccupation with the body (core features of anorexia nervosa and bulimia nervosa) (American Psychiatric Association, 2013; Grilo et al., 2009) it is possible that measures of binge eating may produce weaker associations with self-objectification.
Given the tendency for studies with significant results to reach publication, while studies with non-significant results often go unpublished, moderator analyses examining publication type may serve as a signal of potential publication bias. Additionally, as journal articles undergo extensive peer-review prior to publication, publication type may also be viewed as a proxy for methodological rigor. In the current study, publication type was not a significant moderator – studies published in peer-reviewed journals and unpublished dissertations exhibited similar mean effect sizes. These results suggest an absence of publication bias. Further, formal publication bias analyses including Fail-safe N analyses, trim and fill procedures, and examination of the funnel plot suggest minimal publication bias in the obtained summary effect.
Limitations and Future Directions
There are several limitations to the current study. First, it is likely that variables not examined in the present study operate as moderators of the relationship between self-objectification and disordered eating. Candidate variables for future research include appearance importance, appearance ideal internalization, body dissatisfaction, relationship status, neurobiological factors, and genetic factors. Second, although the current study attempted to include numerous potential theoretical and methodological moderators, proposed analyses may have been underpowered for some variables (e.g., country of origin, measurement of disordered eating). Relatedly, often studies did not include important demographic information regarding participant ethnicity or sexual orientation. As both variables emerged as significant moderators, future studies should seek to collect and report these demographics, and to conduct further work in ethnic and sexual minority groups. Although country of origin did not significantly moderate the summary effect, it is notable that countries representing non-Western cultures were not available for inclusion in the current analysis. Future work should seek to examine this association in non-Western samples. Although measurement of disordered eating did not moderate the summary effect, most studies assessed global eating disorder symptoms, which may have obscured potential differences, and no studies examined associations with symptoms of binge eating disorder. Further work may seek to examine potential differences in associations with anorectic, bulimic, and binge eating phenomena. An additional point to consider relates to the measurement of both disordered eating and self-objectification. The SOQ, OBCS and numerous measures of disordered eating were developed utilizing primarily Caucasian heterosexual female samples. It is therefore possible that these measures may more readily assess experiences of self-objectification and disordered eating most relevant to those groups. To date, no study has examined measurement invariance for the SOQ or OBCS among individuals of different genders, sexual orientation, or ethnic backgrounds. Therefore, caution should be exercised when interpreting findings using male, non-Caucasian, and non-heterosexual samples. Finally, the cross-sectional nature of all included studies precludes the ability to establish temporal precedence or causality. Therefore, we are not able to draw conclusions regarding the role of self-objectification as a casual risk or maintenance factor for disordered eating based solely on the current meta-analysis. However, a small body of work suggests that experimentally-induced changes in state self-objectification (manipulated by instructing participants to wear bulky versus revealing clothing in front of a mirror) may relate to decreased consumption of snack foods in a laboratory setting (Fredrickson, Roberts, Noll, Quinn, & Twenge, 1998; Martins et al., 2007), although this effect has not been consistently demonstrated (Hebl, King, & Lin, 2004). Future research should continue to examine the relationship between self-objectification and disordered eating using a range of methodologies including longitudinal and experimental designs. In particular, as objectification theory proposes that self-objectification serves as a risk factor for disordered eating, examination of the temporal relationships between these variables represents an important area of inquiry. Accordingly, prospective studies that examine the ability of baseline self-objectification levels to predict the emergence of disordered eating or growth in symptoms are recommended to examine the role of self-objectification as a risk factor for disordered eating. Additionally, longitudinal studies examining self-objectification as a predictor of symptom persistence versus remittance among initially ill individuals would provide information regarding the role of self-objectification as a possible maintenance factor for disordered eating. Finally, experimental intervention studies targeting self-objectification are needed to provide important information regarding potential causal relationships between self-objectification and disordered eating. Such work would also serve to clarify whether self-objectification represents a modifiable and meaningful treatment target within disordered eating interventions.
Clinical Implications
Eating disorders and disordered eating are multifactorial problems likely arising from a complex interplay between biological, psychological, and environmental variables. The current study indicates a moderate relationship between disordered eating and the psychological experience of self-objectification. Moreover, the strength of this association appears to be comparable to that of other well-established risk factors (e.g., pressures for thinness, thin ideal internalization). Further, a small body of work suggests that changes in self-objectification may be causally related to increases in restrained eating behaviors (Fredrickson et al., 1998; Martins et al., 2007). Therefore, there is growing evidence to suggest that self-objectification may represent an important element to consider in work related to the conceptualization, treatment, and prevention of disordered eating (Tiggemann, 2013). We have suggested avenues for additional research examining the temporal and causal significance of self-objectification, as well its relevance to disordered eating interventions. Should self-objectification emerge as a causal risk or maintenance factor for disordered eating, existing interventions may seek to address both the cognitive and behavioral manifestations of this experience using empirically-supported techniques. For example cognitive restructuring and dissonance-based approaches may be used to challenge self-schemas that emphasize the importance of appearance over other self-attributes. Mindfulness-based approaches may be used to encourage attention to internal experiences and reduce negative appearance-based judgements regarding oneself and others (Tiggemann, 2013).
Conclusions
In sum, objectification theory posits that self-objectification acts as a risk factor in the development of disordered eating among women. Following the introduction of the theory in 1997, the association between self-objectification and disordered eating has drawn considerable research interest. The current meta-analysis represents the first quantitative review of the resulting 20 years of scientific inquiry. Results suggest a significant moderate positive correlation between self-objectification and disordered eating. Significant heterogeneity in observed effects may be at least partially explained by gender, sexual orientation, ethnicity, and measurement of self-objectification. Although the current study is limited by the use of cross-sectional data and therefore cannot explicitly identify self-objectification as a risk or maintenance factor (Stice, 2002), the results suggest that self-objectification processes (particularly high levels of body surveillance) are highly related to eating disordered attitudes and behaviors. Given this relationship, interventions aiming to reduce levels of self-objectification may also positively impact disordered eating (Menzel, 2013). Future work should continue to clarify the potential causal role of self-objectification in the development of disordered eating and further examine demographic and methodological moderators of this relationship.
Acknowledgments
This work was supported by the National Institute of Mental Health (grant number T32 MH082761).
Appendix A: Characteristics of all studies included in the meta-analysis
| Author(s), year | Sample size | Sample gender | Mean age | Primary ethnic group | Primary sexual orientation | Mean BMI | Country of origin | Sample type | Measurement of SO | Measurement of DE | Publication type | Effect size (r) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Augustus-Horvath & Tylka, 2009 | ||||||||||||
| 18–24 y/o | 329 | Female | 19.90 | Caucasian | N/A | 24.13 | USA | College, Community | OBCS-BS | Global | Journal | .54 |
| 25–68 y/o | 330 | Female | 29.74 | Caucasian | N/A | 26.74 | USA | College, Community | OBCS-BS | Global | Journal | .55 |
| Calogero, 2009 | ||||||||||||
| Females | 139 | Female | N/A | Caucasian | N/A | N/A | England | College | OBCS-BS, SOQ | Global | Journal | .21 |
| Males | 113 | Male | N/A | Caucasian | N/A | N/A | England | College | OBCS-BS, SOQ | Global | Journal | −.01 |
| Calogero, 2004 | 104 | Female | N/A | Caucasian | N/A | 21.71 | USA | College | SOQ | AN | Journal | .40 |
| Calogero, Davis, & Thompson, 2005 | 209 | Female | 22.90 | Caucasian | N/A | 19.70 | USA | Clinical-ED | SOQ | AN | Journal | .38 |
| Calogero & Pina, 2011 | ||||||||||||
| Study 1 | 225 | Female | 21.60 | Caucasian | Heterosexual | 21.92 | England | College | OBCS-BS | AN | Journal | .28 |
| Study 2 | 80 | Female | 21.89 | Caucasian | Heterosexual | 22.01 | England | College | OBCS-BS | AN | Journal | .35 |
| Calogero & Thompson, 2009 | ||||||||||||
| Study 1 | 104 | Female | 18.63 | Caucasian | N/A | 21.71 | USA | College | OBCS-BS | Global | Journal | .67 |
| Study 2 | 111 | Female | 22.00 | N/A | N/A | 21.89 | England | College | OBCS-BS | Global | Journal | .50 |
| Choma, Shove, Busseri, Sandava, & Hosker, 2009 | 104 | Female | 19.12 | Caucasian | N/A | 23.60 | Canada | College | SOQ | Global | Journal | .23 |
| Clarke, Murnen, & Smolak, 2010 | 98 | Female | N/A | Caucasian | N/A | N/A | USA | College | OBCS-BS | AN | Journal | .64 |
| Cottingham, 2008 | 161 | Female | 19.83 | Caucasian | N/A | N/A | USA | College | SOQ | Global | Dissertation | .46 |
| Daubenmier, 2005 | ||||||||||||
| Study 1 | 139 | Female | 37.16 | Caucasian | N/A | N/A | USA | Community | SOQ | Global | Journal | .40 |
| Study 2 | 133 | Female | 20.46 | Asian | N/A | 22.1 | USA | College | SOQ | Global | Journal | .42 |
| Eshkevari, Rieger, Longo, Haggard, & Treasure, 2012 | ||||||||||||
| Clinical | 78 | Female | 23.50 | N/A | N/A | 18.50 | England | Clinical-ED | SOQ | Global | Journal | .28 |
| Healthy Control | 61 | Female | 24.00 | N/A | N/A | 21.50 | England | College, Community | SOQ | Global | Journal | .24 |
| Funk, 2008 | 202 | Female | 20.10 | Caucasian | N/A | 21.83 | USA | College | SOQ | Global | Dissertation | .30 |
| Gianini, 2012 | 204 | Female | 19.44 | Caucasian | N/A | 23.55 | USA | College | OBCS-BS, SOQ | Global | Dissertation | .44 |
| Greenleaf, 2005 | ||||||||||||
| College | 200 | Female | 20.96 | Caucasian | N/A | 22.98 | USA | College | OBCS-BS | Global | Journal | .57 |
| Community | 194 | Female | 48.95 | Caucasian | N/A | 25.16 | USA | Community | OBCS-BS | Global | Journal | .33 |
| Greenleaf & McGreer, 2006 | 185 | Female | 20.52 | Caucasian | N/A | 23.05 | USA | College | OBOBCS-BS, SOQ | Global | Journal | .38 |
| Grupski, 2010 | 539 | Female | 20.43 | Caucasian | Heterosexual | 23.16 | USA | College | SOQ | AN | Dissertation | .43 |
| Haines, Erchull, Liss, Turner, Nelson, Ramsey, & Hurt, 2008 | 126 | Female | 35.12 | Caucasian | Homosexual | N/A | USA | Community | OBCS-BS | Global | Journal | .38 |
| Hallsworth, Wade, Tiggemann, 2005 | 83 | Male | 27.59 | N/A | N/A | 35.79 | Australia | College, Community | OBCS-BS, SOQ | BN | Journal | .20 |
| Harrison & Fredrickson, 2003 | 374 | Female | 13.40 | African American | N/A | N/A | USA | Community | SOQ | Global | Journal | .35 |
| Kaplan, 2012 | 125 | Female | 19.86 | Caucasian | N/A | 22.78 | USA | College | SOQ | BN | Dissertation | .43 |
| Kaptein, 2008 | 263 | Female | 21.40 | Caucasian | N/A | 22.53 | Canada | College | OBCS-BS, SOQ | Global | Dissertation | .53 |
| Kelly, Mitchell, Gow, Trace, Lydecker, Bair, & Mazzeo, 2012 | ||||||||||||
| African American | 741 | Female | N/A | African American | N/A | N/A | USA | College | OBCS-BS | Global | Journal | .34 |
| Caucasian | 1467 | Female | N/A | Caucasian | N/A | N/A | USA | College | OBCS-BS | Global | Journal | .50 |
| Kittler, 2003 | 328 | Female | 18.70 | Caucasian | N/A | 22.10 | USA | College | OBCS-BS, SOQ composite | Global | Dissertation | .49 |
| Langdon & Petracca, 2010 | 77 | Female | 22.91 | Caucasian | N/A | N/A | USA | Community | SOQ | AN | Journal | .25 |
| Lindner, Tantleff-Dunn, & Jentsch, 2012 | 549 | Female | 19.78 | Caucasian | Heterosexual | 23.23 | USA | College | OBCS-BS, SOQ | Global | Journal | .29 |
| Lyders, 1999 | ||||||||||||
| Heterosexual female | 40 | Female | 37.18 | Caucasian | Heterosexual | 24.57 | USA | Community | OBCS-BS | Global | Journal | .52 |
| Heterosexual male | 40 | Male | 37.00 | Caucasian | Heterosexual | 26.44 | USA | Community | OBCS-BS | Global | Journal | .19 |
| Homosexual female | 40 | Female | 35.43 | Caucasian | Homosexual | 25.75 | USA | Community | OBCS-BS | Global | Journal | .37 |
| Homosexual male | 40 | Male | 35.75 | Caucasian | Homosexual | 25.03 | USA | Community | OBCS-BS | Global | Journal | .50 |
| Martins, Tiggemann, & Kirkbridge, 2007 | ||||||||||||
| Heterosexual male | 103 | Male | 27.59 | N/A | Heterosexual | 25.38 | Australia | College, Community | OBCS-BS, SOQ | AN | Journal | .25 |
| Homosexual male | 98 | Male | 27.61 | N/A | Homosexual | 24.54 | Australia | College, Community | OBCS-BS, SOQ | AN | Journal | .35 |
| Mitchell, 2009 | 893 | Female | 19.09 | Caucasian | N/A | 23.96 | USA | College | OBCS-BS, SOQ | Global | Dissertation | .40 |
| Moret, 1999 | 74 | Female | 28.04 | Caucasian | N/A | N/A | USA | Clinical-General | OBCS-BS | Global | Dissertation | .57 |
| Morrison & Sheahan, 2009 | ||||||||||||
| College | 140 | Female | 20.42 | N/A | N/A | 21.93 | Ireland | College | OBCS-BS | Global | Journal | .47 |
| Community | 76 | Female | 23.61 | N/A | N/A | 22.28 | Ireland | Community | OBCS-BS | Global | Journal | .73 |
| Morry & Staska, 2001 | ||||||||||||
| Females | 89 | Female | 18.80 | N/A | N/A | N/A | Canada | College | SOQ | Global | Journal | .40 |
| Males | 61 | Male | 19.80 | N/A | N/A | N/A | Canada | College | SOQ | Global | Journal | .17 |
| Muehlenkamp & Saris-Baglama, 2002 | 396 | Female | 19.50 | Caucasian | N/A | N/A | USA | College | OBCS-BS | Global | Journal | .44 |
| Mussap, 2009 | 189 | Female | 27.34 | N/A | N/A | 23.59 | Australia | Community | SOQ | AN | Journal | .15 |
| Myers & Crowther, 2008 | 195 | Female | 19.60 | Caucasian | N/A | 23.30 | USA | College | SOQ | Global | Journal | .24 |
| Noffsinger-Frazier, 2004 | 345 | Female | 30.52 | Caucasian | Heterosexual | 25.90 | USA, Canada | Community | OBCS-BS, SOQ | Global | Dissertation | .40 |
| Noll & Fredrickson, 1998 | ||||||||||||
| Study 1 | 93 | Female | 18.80 | Caucasian | N/A | 21.40 | USA | College | SOQ | Global | Journal | .40 |
| Study 2 | 111 | Female | 18.30 | Caucasian | N/A | 22.10 | USA | College | SOQ | Global | Journal | .30 |
| Oehlhof, 2012 | ||||||||||||
| Normal weight | 212 | Female | 19.17 | Caucasian | N/A | 21.02 | USA | College | SOQ | Global | Dissertation | .24 |
| Overweight | 201 | Female | 19.71 | Caucasian | N/A | 30.69 | USA | College | SOQ | Global | Dissertation | .27 |
| Peat & Muehlenkamp, 2011 | 214 | Female | 20.09 | Caucasian | N/A | 23.24 | USA | College | SOQ | Global | Journal | .29 |
| Prichard & Tiggemann, 2008 | 571 | Female | 35.99 | N/A | N/A | 23.80 | Australia | Community | SOQ | Global | Journal | .39 |
| Prichard & Tiggemann, 2005 | 157 | Female | 32.15 | N/A | N/A | 22.63 | Australia | Community | OBCS-BS, SOQ | Global | Journal | .43 |
| Rolnik, Engeln-Maddox, & Miller, 2010 | 127 | Female | 18.14 | Caucasian | N/A | N/A | USA | College | OBCS-BS | Global | Journal | .54 |
| Serpa, 2005 | ||||||||||||
| Heterosexual male | 96 | Male | 33.97 | Caucasian | Heterosexual | N/A | USA | Community | OBCS-BS, SOQ | Global | Journal | .11 |
| Homosexual male | 96 | Male | 37.45 | Caucasian | Homosexual | N/A | USA | Community | OBCS-BS, SOQ | Global | Journal | .21 |
| Slater & Tiggemann, 2002 | ||||||||||||
| Dancer | 38 | Female | 14.50 | Caucasian | N/A | 18.60 | Australia | Community | OBCS-BS, SOQ | Global | Journal | .51 |
| Non-dancer | 45 | Female | 14.10 | Caucasian | N/A | 20.50 | Australia | Community | OBCS-BS, SOQ | Global | Journal | .62 |
| Slater & Tiggemann, 2012 | 141 | Female | 14.45 | Caucasian | N/A | N/A | Australia | Community | SOQ | Global | Journal | .35 |
| Smolak & Murnen, 2011 | ||||||||||||
| Females | 148 | Female | N/A | Caucasian | N/A | N/A | USA | College | OBCS-BS | AN | Journal | .49 |
| Males | 76 | Male | N/A | Caucasian | N/A | N/A | USA | College | OBCS-BS | AN | Journal | .38 |
| Tiggemann & Kuring, 2004 | ||||||||||||
| Females | 171 | Female | 21.92 | N/A | N/A | N/A | Australia | College | OBCS-BS, SOQ | Global | Journal | .45 |
| Males | 115 | Male | 22.43 | N/A | N/A | N/A | Australia | College | OBCS-BS, SOQ | Global | Journal | .13 |
| Tiggemann & Lynch, 2001 | 332 | Female | 45.02 | N/A | N/A | 25.37 | Australia | Community | OBCS-BS, SOQ | Global | Journal | .35 |
| Tiggemann & Slater, 2001 | ||||||||||||
| Dancer | 50 | Female | 20.30 | N/A | N/A | 21.50 | Australia | College, Community | OBCS-BS, SOQ | Global | Journal | .55 |
| Non-dancer | 51 | Female | 19.40 | N/A | N/A | 22.70 | Australia | College, Community | OBCS-BS, SOQ | Global | Journal | .44 |
| Tiggemann & Williams, 2012 | 146 | Female | 20.40 | Caucasian | N/A | 23.61 | Australia | College | OBCS-BS, SOQ | Global | Journal | .36 |
| Tylka & Hill, 2004 | 460 | Female | 21.40 | Caucasian | N/A | N/A | USA | College | OBCS-BS | Global | Journal | .56 |
| Van Diest & Perez, 2013 | 177 | Female | 19.25 | Caucasian | N/A | 21.28 | USA | College | SOQ | Global | Journal | .42 |
| Woolley, 2009 | 395 | Female | N/A | Caucasian | Heterosexual | N/A | USA | College, Community | OBCS-BS, SOQ | Global | Dissertation | .29 |
Contributor Information
Lauren M. Schaefer, Neuropsychiatric Research Institute
J. Kevin Thompson, University of South Florida.
References
- Agras WS, Brandt HA, Bulik CM, Dolan-Sewell R, Fairburn CG, Halmi KA, et al. Report of the National Institutes of Health workshop to overcoming barriers to treatment research in anorexia nervosa. International Journal of Eating Disorders. 2004;35(4):509–521. doi: 10.1002/eat10261. [DOI] [PubMed] [Google Scholar]
- Archer D, Iritani B, Kimes DD, Barrios M. Face-ism: Five studies of sex differences in facial prominence. Journal of Personality and Social Psychology. 1983;45:725–735. [Google Scholar]
- Ata R, Schaefer LM, Thompson JK. Sociocultural theories of eating disorders. In: Levine M, Smolak L, editors. The Wiley-Blackwell Handbook of Eating Disorders. West Sussex, UK: John Wiley and Sons, Ltd; 2014. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. Arlington, VA: American Psychiatric Publishing; 2013. [Google Scholar]
- Augustus-Horvath CL, Tylka TL. A test and extension of objectification theory as it predicts disordered eating: Does women’s age matter? Journal of Counseling Psychology. 2009;56(2):253–265. doi: 10.1037/a0014637. [DOI] [Google Scholar]
- Bartky SL. Femininity and domination: Studies in the phenomenology of oppression. New York, NY: Routledge; 1990. [Google Scholar]
- Berkman ND, Bulik CM, Brownley KA, Lohr KN, Sedway JA, Rooks A, Gartlehner G. Management of eating disorders. Evidence Report/Technology Assessment. 2006;135:1–166. [PMC free article] [PubMed] [Google Scholar]
- Borenstein M, Hedges L, Higgins J, Rothstein H. Comprehensive Meta-Analysis (Version 2.0) [computer software] Englewood, NJ: Biostat; 2005. [Google Scholar]
- Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to meta-analysis. Chichester, UK: Wiley; 2009. [Google Scholar]
- Boroughs M, Thompson JK. Exercise status and sexual orientation as moderators of body image disturbance and eating disorders in males. International Journal of Eating Disorders. 2002;31(3):307–311. doi: 10.1002/eat.10031. [DOI] [PubMed] [Google Scholar]
- Brand PA, Rothblum ED, Solomon LJ. A comparison of lesbians, gay men, and heterosexuals on weight and restrained eating. International Journal of Eating Disorders. 1992;11(3):253–259. doi: 10.1002/1098-108X(199204. [DOI] [Google Scholar]
- Breitkopft CR, Littleton H, Berenson A. Body image: A study in a tri-ethnic sample of low income women. Sex Roles. 2007;56:373–380. doi: 10.1007/s11199-006-9177-x. [DOI] [Google Scholar]
- Bryant AL. Hostile hallways: The AAUW survey on sexual harassment in America’s schools. Journal of School Health. 1993;63(8):355–357. doi: 10.1111/j.1746-1561.1993.tb07153.x. [DOI] [PubMed] [Google Scholar]
- Bucchianeri MM, Fernandes N, Loth K, Hannan PJ, Eisenberg ME, Neumark-Sztainer D. Body Dissatisfaction: Do Associations With Disordered Eating and Psychological Well-Being Differ Across Race/Ethnicity in Adolescent Girls and Boys? Cultural Diversity And Ethnic Minority Psychology. 2015 doi: 10.1037/cdp0000036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cachelin FM, Rebeck RM, Chung GH, Pelayo E. Does ethnicity influence body-size preference? A comparison of body image and body size. Obesity Research. 2002;10(3):158–166. doi: 10.1038/oby.2002.25. [DOI] [PubMed] [Google Scholar]
- Calogero RM. A Test of objectification theory: The effect of the male gaze on appearance concerns in college women. Psychology of Women Quarterly. 2004;28(1):16–21. doi: 10.1111/j.1471-6402.2004.00118.x. [DOI] [Google Scholar]
- Calogero RM. Objectification processes and disordered eating in British women and men. Journal of Health Psychology. 2009;14(3):394–402. doi: 10.1177/1359105309102192. [DOI] [PubMed] [Google Scholar]
- Calogero RM. Operationalizing self-objectification: Assessment and related methodological issues. In: Calogero RM, Tantleff-Dunn S, Thompson JK, editors. Self-objectification: Causes, consequences, and counteractions. Washington, DC: American Psychological Association; 2011. pp. 139–159. [Google Scholar]
- Calogero RM, Davis WN, Thompson JK. The role of self-objectification in the experience of women with eating disorders. Sex Roles. 2005;52(1–2):43–50. doi: 10.1007/s11199-005-1192-9. [DOI] [Google Scholar]
- Calogero RM, Pina A. Body guilt: Preliminary evidence for a further subjective experience of self-objectification. Psychology of Women Quarterly. 2011;35(3):428–440. doi: 10.1177/0361684311408564. [DOI] [Google Scholar]
- Calogero RM, Tantleff-Dunn S, Thompson JK. Objectification theory: An introduction. In: Calogero RM, Tantleff-Dunn S, Thompson JK, editors. Self-objectification: Causes, consequences, and counteractions. Washington, DC: American Psychological Association; 2011. pp. 3–21. [Google Scholar]
- Calogero RM, Thompson JK. Sexual self-esteem in American and British college women: Relations with self-objectification and eating problems. Sex Roles. 2009;60(3–4):160–173. doi: 10.1007/s11199-008-9517-0. [DOI] [Google Scholar]
- Choma BL, Shove C, Busseri MA, Sadava SW, Hosker A. Assessing the role of body image coping strategies as mediators or moderators of the links between self-objectification, body shame, and well-being. Sex Roles. 2009;61(9–10):699–713. doi: 10.1007/s11199-009-9666-9. [DOI] [Google Scholar]
- Clarke PM, Murnen SK, Smolak L. Development and psychometric evaluation of a quantitative measure of ‘fat talk’. Body Image. 2010;7(1):1–7. doi: 10.1016/j.bodyim.2009.09.006. [DOI] [PubMed] [Google Scholar]
- Cochran W. The combination of estimates from different experiments. Biometrics. 1954;10(1):101–129. doi: 10.2307/3001666. [DOI] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Cottingham ME. Doctoral dissertation. 2008. The role of spirituality in self-objectification and disordered eating in college women. Retrieved from ProQuest Dissertations and Theses database. (3299121) [Google Scholar]
- Croll J, Neumark-Sztainer D, Story M, Ireland M. Prevalence and risk and protective factors related to disordered eating behaviors among adolescents: Relationship to gender and ethnicity. Journal of Adolescent Health. 2002;31(2):166–175. doi: 10.1016/s1054-139x(02)00368-3. [DOI] [PubMed] [Google Scholar]
- Daubenmier JJ. The relationship of yoga, body awareness, and body responsiveness to self-objectification and disordered eating. Psychology of Women Quarterly. 2005;29(2):207–219. doi: 10.111/j.1471-6402.2005.00183.x. [DOI] [Google Scholar]
- Dickersin K. Publication bias: Recognizing the problem, understanding its origins and scope, and preventing harm. In: Rothstein HR, Sutton AJ, Borenstein M, editors. Publication bias in meta-analysis: Prevention, assessment, and adjustments. Chichester: John Wiley & Sons Ltd; 2005. [Google Scholar]
- Duval S, Tweedie R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics. 2000a;56(2):455–463. doi: 10.1111/j.0006-341X.2000.00455.x. [DOI] [PubMed] [Google Scholar]
- Duval S, Tweedie R. A nonparametric ‘trim and fill’ method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association. 2000b;95(449):89–98. doi: 10.1080/01621459.2000.10473905. [DOI] [Google Scholar]
- Easterbrook PJ, Berlin JA, Gopalan R, Matthews DR. Publication bias in clinical research. Lancet. 1991;337:867–872. doi: 10.1016/0140-6736(91)90201-y. http://dx.doi.org/10.1016/0140-6736(91)90201-Y. [DOI] [PubMed] [Google Scholar]
- Engeln-Maddox R, Miller SA, Doyle DM. Test of objectification theory in gay, lesbian, and heterosexual community samples: Mixed evidence for proposed pathways. Sex Roles. 2011;65(7–8):518–532. doi: 10.1007/s11199-011-9958-8. [DOI] [Google Scholar]
- Eshkevari E, Rieger E, Longo MR, Haggard P, Treasure J. Increased plasticity of the bodily self in eating disorders. Psychological Medicine. 2012;42(4):819–828. doi: 10.1017/S0033291711002091. [DOI] [PubMed] [Google Scholar]
- Fairburn CG, Cooper Z, Waller D. The patients: Their assessment, preparation for treatment and medical management. In: Fairburn CG, editor. Cognitive behavior therapy and eating disorders. New York: The Guilford Press; 2008. pp. 35–44. [Google Scholar]
- Field AE, Camargo CA, Taylor CB, Berkey CS, Colditz GA. Relation of peer and media influences to the development of purging behaviors among preadolescent and adolescent girls. Archives of Pediatric Adolescent Medicine. 1999;153(11):1184–1189. doi: 10.1001/archpedi.153.11.1184. [DOI] [PubMed] [Google Scholar]
- Fisher RA. Statistical methods for research workers. 14th. Edinburgh: Oliver and Boyd; 1970. [Google Scholar]
- Fitzsimmons-Craft EE. Social psychological theories of disordered eating in college women: Review and integration. Clinical Psychology Review. 2011;31(7):1224–1237. doi: 10.1016/j.cpr.2011.07.011. [DOI] [PubMed] [Google Scholar]
- Fredrickson BL, Roberts T. Objectification theory: Toward understanding women’s lived experiences and mental health risks. Psychology of Women Quarterly. 1997;21(2):173–206. doi: 10.1111/j.1471-6402.1997.tb00108.x. [DOI] [Google Scholar]
- Fredrickson BL, Roberts T, Noll SM, Quinn DM, Twenge JM. That swimsuit becomes you: Sex differences in self-objectification, restrained eating, and math performance. Journal of Personality and Social Psychology. 1997;75(1):369–284. doi: 10.1037/h0090332. [DOI] [PubMed] [Google Scholar]
- Funk RS. Doctoral dissertation. 2008. Sexual harassment and disordered eating symptomatology in females: Objectification, silencing, and symbolic expression of self. Retrieved from ProQuest Dissertations and Theses database. (3277035) [Google Scholar]
- Gray JJ, Ford K, Kelly LM. The prevalence of bulimia in a Black college population. International Journal of Eating Disorders. 1987;6(6):733–740. doi: 10.1002/1098-108X(198711)6:6<733::AID-EAT2260060606>3.0.CO;2-U. [DOI] [Google Scholar]
- Gianini L. Doctoral dissertation. 2012. The unique properties of self-objectification and social and individual influences on its expression. Retrieved from ProQuest Dissertations and Theses database. (3473176) [Google Scholar]
- Greenleaf C. Self-objectification among physically active women. Sex Roles. 2005;52(1–2):51–62. doi: 10.1007/s11199-005-1193-8. [DOI] [Google Scholar]
- Greenleaf C, McGreer R. Disordered eating attitudes and self-objectification among physically active and sedentary female college students. Journal of Psychology. 2006;140:187–198. doi: 10.3200/JRLP.140.3.187-198. [DOI] [PubMed] [Google Scholar]
- Grilo CM, Crosby RD, Masheb RM, White MA, Peterson CB, Wonderlich SA, Mitchell JE. Overvaluation of shape and weight in binge eating disorder, bulimia nervosa, and sub-threshold bulimia nervosa. Behaviour Research And Therapy. 2009;47(8):692–696. doi: 10.1016/j.brat.2009.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Groesz LM, Levine MP, Murnen SK. The effect of experimental presentation of thin media images on body satisfaction: A meta-analytic review. International Journal of Eating Disorders. 2002;31:1–16. doi: 10.1002/eat.10005. [DOI] [PubMed] [Google Scholar]
- Grupski A. Doctoral dissertation. 2010. Classifying exercise activities according to motivation, self-objectification, and disordered eating: How can we target change? Retrieved from ProQuest Dissertations and Theses database. (3392054) [Google Scholar]
- Haines ME, Erchull MJ, Liss M, Turner LM, Nelson JA, Ramsey LR, Hurt MM. Predictors and effects of self-objectification in lesbians. Psychology of Women Quarterly. 2008;32(2):181–187. doi: 10.1111/j.1471-6402.2008.00422.x. [DOI] [Google Scholar]
- Hallsworth L, Wade T, Tiggemann M. Individual differences in male body-image: An examination of self-objectification in recreational body builders. British Journal of Health Psychology. 2005;10(3):453–465. doi: 10.1348/135910705X26966. [DOI] [PubMed] [Google Scholar]
- Harrison K, Fredrickson BL. Women’s sports media, self-objectification, and mental health in black and white adolescent females. Journal of Communication. 2003;53(2):216–232. doi: 10.1111/j.1460-2466.2003.tb02587.x. [DOI] [Google Scholar]
- Heatherton TF, Mahamedi F, Striepe M, Field AE, Keel P. A 10-year longitudinal study of body weight, dieting, and eating disorder symptoms. Journal of Abnormal Psychology. 1997;106(1):117–125. doi: 10.1037/0021-843X.106.1.117. [DOI] [PubMed] [Google Scholar]
- Hebl MR, King EB, Lin J. The swimsuit becomes us all: Ethnicity, gender, and vulnerability to self-objectification. Personality and Social Psychology Bulletin. 2004;30:1322–1331. doi: 10.1177/0146167204264052. [DOI] [PubMed] [Google Scholar]
- Hedges LV, Olkin I. Statistical methods for meta-analysis. New York, NY: Academic; 1985. [Google Scholar]
- Hesse-Biber S, Marino M, Watts-Roy D. A longitudinal study of eating disorders among college women: Factors that influence recovery. Gender and Society. 1999;13:385–408. doi: 10.1177/089124399013003007. [DOI] [Google Scholar]
- Hill MS, Fischer AR. Examining objectification theory: Lesbian and heterosexual women’s experiences with sexual and self-objectification. Counseling Psychologist. 2008;36(5):745–776. doi: 10.1177/0011000007301669. [DOI] [Google Scholar]
- Hudson JI, Hiripi E, Pope HG, Kessler RC. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biological Psychiatry. 2007;61(3):348–358. doi: 10.1016/j.biopsych.2006.03.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacobi C, Hayward C, de Zwaan M, Kraemer HC, Agras WS. Coming to Terms With Risk Factors for Eating Disorders: Application of Risk Terminology and Suggestions for a General Taxonomy. Psychological Bulletin. 2004;130(1):19–65. doi: 10.1037/0033-2909.130.1.19. [DOI] [PubMed] [Google Scholar]
- Jones JM, Bennett S, Olmstead MP, Lawson ML, Rodin G. Disordered eating attitudes and behaviours in teenaged girls: A school-based study. Canadian Medical Association Journal. 2001;165(5):547–552. [PMC free article] [PubMed] [Google Scholar]
- Kaplan A. Doctoral dissertation. 2012. Risk and protective factors: An integration of cognitive behavioral and feminist perspectives in explaining bulimic symptoms in female university students. Retrieved from ProQuest Dissertations and Theses database. (3463183) [Google Scholar]
- Kaptein SA. Doctoral dissertation. 2008. Mirror, mirror, on the wall: A study of objectification theory in female exercisers. Retrieved from ProQuest Dissertations and Theses database. (NR32054) [Google Scholar]
- Keel PK, Haedt A. Evidence-based psychosocial treatments for eating problems and eating disorders. Journal of Clinical Child and Adolescent Psychology. 2008;37(1):39–61. doi: 10.1080/15374410701817832.. [DOI] [PubMed] [Google Scholar]
- Keel PK, Klump KL. Are eating disorders culture-bound syndromes? Implications for conceptualizing their etiology. Psychological Bulletin. 2003;129(5):747–769. doi: 10.1037/0033-2909.129.5.747. [DOI] [PubMed] [Google Scholar]
- Kelly NR, Cotter EW, Tanofsky-Kraff M, Mazzeo SE. Racial variations in binge eating, body image concerns, and compulsive exercise among men. Psychology Of Men & Masculinity. 2015;16(3):326–336. doi: 10.1037/a0037585. [DOI] [Google Scholar]
- Kelly NR, Mitchell KS, Gow RW, Trace SE, Lydecker JA, Bair CE, Mazzeo S. An evaluation of the reliability and construct validity of eating disorder measures in white and black women. Psychological Assessment. 2012;24(3):608–617. doi: 10.1037/a0026457. [DOI] [PubMed] [Google Scholar]
- Killen JD, Taylor CB, Hayward C, Wilson D, Haydel K, Hammer L, Kraemer H. Pursuit of thinness and onset of eating disorder symptoms in a community sample of adolescent girls: A three-year prospective analysis. International Journal of Eating Disorders. 1994;16(3):227–238. doi: 10.1002/1098-108x(199411)16:3<227::aid-eat2260160303>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- Kittler JE. Doctoral dissertation. 2003. Print media exposure as a predictor of disordered eating: The role of self-objectification, body shame, and appearance responsibility. Retrieved from ProQuest Dissertations and Theses database. (3079474) [Google Scholar]
- Klonoff EA. Sexist discrimination may account for well-known gender differences in psychiatric symptoms. Psychology of Women Quarterly. 2000;24(1):93–99. doi: 10.1111/j.1471-6402.2000.tb01025.x. [DOI] [Google Scholar]
- Kozak M, Frankenhauser H, Roberts TA. Objects of desire: Objectification as a function of male sexual orientation. Psychology of Men & Masculinity. 2009;10(3):225–230. doi: 10.1037/a0016257. [DOI] [Google Scholar]
- Kozee HB, Tylka TL. A test of objectification theory with lesbian women. Psychology of Women Quarterly. 2006;30(4):348–357. doi: 10.1111/j.1471-6402.2006.00310.x. [DOI] [Google Scholar]
- Kozee HB, Tylka TL, Augustus-Horvath C, Denchik A. Development and psychometric evaluation of the Interpersonal Sexual Objectification Scale. Psychology of Women Quarterly. 2007;31(2):176–189. doi: 10.1111/j.147106402.2007.00351.x. [DOI] [Google Scholar]
- Langdon SW, Petracca G. Tiny dancer: Body image and dancer identity in female modern dancers. Body Image. 2010;7(4):360–363. doi: 10.1016/j.bodyim.2010.06.005. [DOI] [PubMed] [Google Scholar]
- Lindner D, Tantleff-Dunn S, Jentsch F. Social comparison and the ‘circle of objectification’. Sex Roles. 2012;67(3–4):222–235. doi: 10.1007/s11199-012-0175-x. [DOI] [Google Scholar]
- Loughnan S, Fernandez-Campos S, Vaes J, Anjum G, Aziz M, Harada C, et al. Exploring the role of cultural in sexual objectification: A seven nations study. International Review of Social Psychology. 2015;28(1):125–152. [Google Scholar]
- Lyders GC. Doctoral dissertation. 1999. Oct, Body image and attitudes toward eating: The influence of objectified body consciousness and variations by gender and sexual orientation. Retrieved from ProQuest Dissertations and Theses database. (9928691) [Google Scholar]
- Martins Y, Tiggemann M, Kirkbride A. Those speedos become them: The role of self-objectification in gay and heterosexual men’s body image. Personality and Social Psychology Bulletin. 2007;33(5):634–647. doi: 10.1177/0146167206297403. [DOI] [PubMed] [Google Scholar]
- Mautner RD, Owen SV, Furnham A. Cross-cultural explanations of body image disturbancein Western cultural samples. International Journal Of Eating Disorders. 2000;28(2):165–172. doi: 10.1002/1098-108X(200009)28:2<165::AID-EAT5>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- McKinley NM, Hyde JS. The Objectified Body Consciousness Scale: Development and validation. Psychology of Women Quarterly. 1996;20(2):181–215. doi: 10.1111/j.1471-6402.1996.tb00467.x. [DOI] [Google Scholar]
- McKnight Risk Factor Study. Ethnic group differences in disordered eating attitudes and behaviors and related risk factors. Paper presented at the Ninth International Conference on Eating Disorders; New York. 2000. Mar, [Google Scholar]
- Mehler PS, Birmingham LC, Crow SJ, Jahraus JP. Medical complications of eating disorders. In: Grilo CM, Mitchel JE, editors. The treatment of eating disorders: A clinical handbook. New York: Guilford Press; 2010. pp. 66–80. [Google Scholar]
- Menzel JE. Doctoral dissertation. 2014. Efficacy of a dissonance-based intervention for self-objectification: A randomized controlled trial. Retrieved from ProQuest Dissertations and Theses database. (3604838) [Google Scholar]
- Menzel JE, Schaefer LM, Burke NL, Mayhew LL, Brannick MT, Thompson JK. Appearance-related teasing, body dissatisfaction, and disordered eating: A meta-analysis. Body Image. 2010;7(4):261–270. doi: 10.1016/j.bodyim.2010.05.004. [DOI] [PubMed] [Google Scholar]
- Miller MN, Pumariega AJ. Culture and eating disorders: A historical and cross-cultural review. Psychiatry. 2001;64:93–110. doi: 10.1521/psyc.64.2.93.18621. [DOI] [PubMed] [Google Scholar]
- Mintz LB, Betz NE. Prevalence and correlations of eating disordered behaviors among undergraduate women. Journal of Counseling Psychology. 1988;35(4):463–471. doi: 10.1037/0022-0167.35.4.463.. [DOI] [Google Scholar]
- Mitchell KS. Doctoral dissertation. 2009. Evaluation of a structural model of objectification theory and eating disorder symptomatology among ethnically diverse undergraduate women. Retrieved from ProQuest Dissertations and Theses database. (3348091) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mond J, Hall A, Bentley C, Harrison C, Gratwick‐Sarll K, Lewis V. Eating‐disordered behavior in adolescent boys: Eating disorder examination questionnaire norms. International Journal Of Eating Disorders. 2014;47(4):335–341. doi: 10.1002/eat.22237. [DOI] [PubMed] [Google Scholar]
- Moradi B, Huang Y. Objectification theory and psychology of women: A decade of advances and future directions. Psychology of Women Quarterly. 2008;32:377–398. [Google Scholar]
- Moret LB. Doctoral dissertation. 1999. Oct, Eating disordered symptomatology, body image concerns, and social support of female survivors of sexual abuse. Retrieved from ProQuest Dissertations and Theses database. (9925117) [Google Scholar]
- Morrison TG, Sheahan EE. Gender-related discourses as mediators in the association between internalization of the thin-body ideal and indicants of body dissatisfaction and disordered eating. Psychology of Women Quarterly. 2009;33(4):374–383. doi: 10.1111/j.1471-6402.2009.01515.x. [DOI] [Google Scholar]
- Morry MM, Staska SL. Magazine exposure: Internalization, self-objectification, eating attitudes, and body satisfaction in male and female university students. Canadian Journal of Behavioural Science/Revue Canadienne Des Sciences Du Comportement. 2001;33(4):269–279. doi: 10.1037/h0087148. [DOI] [Google Scholar]
- Muehlenkamp JJ, Saris-Baglama RN. Self-objectification and its psychological outcomes for college women. Psychology of Women Quarterly. 2002;26(4):371–379. doi: 10.1111/1471-6402.t01-1-00076. [DOI] [Google Scholar]
- Murnen SK, Smolak L. The experience of sexual harassment among grade-school students: Early socialization of female subordination? Sex Roles. 2000;43(1–2):1–17. [Google Scholar]
- Mussap AJ. Strength of faith and body image in Muslim and non-Muslim women. Mental Health, Religion & Culture. 2009;12(2):121–127. doi: 10.1080/13674670802358190. [DOI] [Google Scholar]
- Myers TA, Crowther JH. Is self-objectification related to interoceptive awareness? An examination of potential mediating pathways to disordered eating attitudes. Psychology Of Women Quarterly. 2008;32(2):172–180. doi: 10.1111/j.1471-6402.2008.00421.x. [DOI] [Google Scholar]
- Myers TA, Crowther JH. Social comparison as a predictor of body dissatisfaction: A meta-analytic review. Journal of Abnormal Psychology. 2009;118(4):683–698. doi: 10.1037/a0016763. [DOI] [PubMed] [Google Scholar]
- Noffsinger-Frazier NA. Doctoral dissertation. 2004. Objectification theory and disordered eating: The impact of feminist identification, internalization of sociocultural standards of appearance, and sexual orientation. Retrieved from ProQuest Dissertations and Theses database. (3137803) [Google Scholar]
- Noll SM, Fredrickson BL. A meditational model linking self-objectification, body shame, and disordered eating. Psychology of Women Quarterly. 1998;22(4):623–636. doi: 10.1111/k.1471-6401.1998.tb00181.x. [DOI] [Google Scholar]
- O’Brien KM, Vincent NK. Psychiatric comorbidity in anorexia and bulimia nervosa: Nature, prevalence, and causal relationships. Clinical Psychology Review. 2003;23(1):57–74. doi: 10.1016/S0272-7358(02)00201-5. [DOI] [PubMed] [Google Scholar]
- Oehlhof MW. Doctoral dissertation. 2012. Self-objectification among overweight and obese women: An application of structural equation modeling. Retrieved from ProQuest Dissertations and Theses database. (3493149) [Google Scholar]
- Orwin RG. A fail-safe N for effect size. Journal of Educational Statistics. 1983;8(2):157–159. [Google Scholar]
- Peat CM, Muehlenkamp JJ. Self-objectification, disordered eating, and depression: A test of mediational pathways. Psychology of Women Quarterly. 2011;35(3):441–450. doi: 10.1177/0361684311400389. [DOI] [Google Scholar]
- Polivy J, Herman CP. Dieting and binging: A causal analysis. American Psychologist. 1985;40(2):193–201. doi: 10.1037/0003-066X.40.2.193. [DOI] [PubMed] [Google Scholar]
- Powell AD, Kahn AS. Racial differences in women’s desires to be thin. International Journal of Eating Disorders. 1995;17(2):191–195. doi: 10.1002/1098-108x(199503)17:2<191::aid-eat2260170213>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- Prichard I, Tiggemann M. Objectification in fitness centers: Self-objectification, body dissatisfaction, and disordered eating in aerobic instructors and aerobic participants. Sex Roles. 2005;53(1–2):19–28. doi: 10.1007/s11199-005-4270-0. [DOI] [Google Scholar]
- Prichard I, Tiggemann M. Relations among exercise type, self-objectification, and body image in the fitness centre environment: The role of reasons for exercise. Psychology of Sport And Exercise. 2008;9(6):855–866. doi: 10.1016/j.psychsport.2007.10.005. [DOI] [Google Scholar]
- Pyle RL, Neuman PA, Halvorson PA, Mitchell JE. An ongoing cross- sectional study of the prevalence of eating disorders in freshman college students. International Journal of Eating Disorders. 1991;10:667–677. doi: 10.1002/1098-108X(199111)10:6b667:AID-EAT2260100605N3.0.CO;2-K. [DOI] [Google Scholar]
- Rancourt D, Schaefer LM, Bosson JK, Thompson JK. Differential impact of upward and downward comparisons on diverse women’s disordered eating behaviors and body image. International Journal Of Eating Disorders. 2016;49(5):519–523. doi: 10.1002/eat.22470. [DOI] [PubMed] [Google Scholar]
- Rolnik AM, Engeln-Maddox R, Miller SA. Here’s looking at you: Self-objectification, body image disturbance, and sorority rush. Sex Roles. 2010;63(1–2):6–17. doi: 10.1007/s11199-010-9745-y. [DOI] [Google Scholar]
- Rukavina T, Pokrajac-Bulian A. Thin-ideal internalization, body dissatisfaction, and symptoms of eating disorders in Croatian adolescent girls. Eating and Weight Disorders. 2006;11(1):31–37. doi: 10.1007/BF03327741. [DOI] [PubMed] [Google Scholar]
- Roberts TA. Female trouble: The menstrual self-evaluation scale and women’s self-objectification. Psychology of Women Quarterly. 2004;28(1):22–26. doi: 10.1111/j.1471-6402.2004.00119.x. [DOI] [Google Scholar]
- Roberts TA, Gettman JY. Mere exposure: Gender differences in the negative effects of priming a state of self-objectification. Sex Roles. 2004;51(1–2):17–27. doi: 0360-0025/04/0700-0017/0. [Google Scholar]
- Schaefer LM, Burke NL, Thompson JK, Heinberg LJ, Calogero RM, Bardone-Cone AM, Swami V. Comparing internalization of appearance ideals and appearance-related pressures among American, Italian, English, and Australian women. Poster presented at the annual Academy of Eating Disorders International Conference on Eating Disorders; Montreal, Canada. 2013. May, [Google Scholar]
- Schaefer LM, Thibodaux LK, Krenik D, Arnold E, Thompson JK. Physical appearance comparisons in ethnically diverse college women. Body Image. 2015;15:153–157. doi: 10.1016/j.bodyim.2015.09.002. [DOI] [PubMed] [Google Scholar]
- Serpa JG. Doctoral dissertation. 2005. A new measure of body dissatisfaction and its relation to self-objectification, eating disorders, and depression in gay and heterosexual men. Retrieved from ProQuest Dissertations and Theses database. (3161378) [Google Scholar]
- Sharp CW, Freeman CP. The medical complications of anorexia nervosa. British Journal of Psychiatry. 1993;162:452–462. doi: 10.1192/bjp.162.4.452. [DOI] [PubMed] [Google Scholar]
- Slater A, Tiggemann M. A test of objectification theory in adolescent girls. Sex Roles. 2002;46(9–10):343–349. doi: 10.1023/A:1020232714705. [DOI] [Google Scholar]
- Slater A, Tiggemann M. Time since menarche and sport participation as predictors of self-objectification: A longitudinal study of adolescent girls. Sex Roles. 2012;67(9–10):571–581. doi: 10.1007/s11199-012-0200-0. [DOI] [Google Scholar]
- Smolak L, Murnen SK. Gender, self-objectification and pubic hair removal. Sex Roles. 2011;65(7–8):506–517. doi: 10.1007/s11199-010-9922-z. [DOI] [Google Scholar]
- Steer A, Tiggemann M. The role of self-objectification in women’s sexual functioning. Journal of Social and Clinical Psychology. 2008;27(3):205–225. doi: 10.1521/jscp.2008.27.3.205. [DOI] [Google Scholar]
- Stice E. Risk and maintenance factors for eating pathology: A meta-analytic review. Psychological Bulletin. 2002;128(5):825–848. doi: 10.1037/0033-2909.128.5.825. doi: 0.1037//0033-2909.128.5.825. [DOI] [PubMed] [Google Scholar]
- Stice E, Presnell K, Spangler D. Risk factors for binge eating onset in adolescent girls: A 2-year prospective investigation. Health Psychology. 2002;21(2):131–138. doi: 10.1037/0278-6133.21.2.131. [DOI] [PubMed] [Google Scholar]
- Striegel-Moore RH, Silberstein LR, Rodin J. Toward an understanding of risk factors for bulimia. American Psychologist. 1986;41:246–263. doi: 10.1037/0003066X.41.3.246. [DOI] [PubMed] [Google Scholar]
- Striegel-Moore RH, Tucker N, Hsu J. Body image dissatisfaction and disordered eating in lesbian college students. International Journal of Eating Disorders. 1990;9(5):493–500. doi:0.1002/1098-108X(199009)9:5<493::AID-EAT2260090504>3.0.CO;2-C. [Google Scholar]
- Swami V, Frederick DA, Aavik T, Alcalay L, Allik J, Anderson D, Zivcic-Becirevic I. The attractive female body weight and female body dissatisfaction in 26 countries across 10 world regions: Results of the international body project I. Personality And Social Psychology Bulletin. 2010;36(3):309–325. doi: 10.1177/0146167209359702. [DOI] [PubMed] [Google Scholar]
- Swim JK, Hyers LL, Cohen LL, Ferguson MJ. Everyday sexism: Evidence for its incidence, nature, and psychological impact from three daily diary studies. Journal of Social Issues. 2001;57(1):31–53. doi: 10.1111/0022-4537.00200. [DOI] [Google Scholar]
- Tiggemann M. Mental health risks of self-objectification: A review of the empirical evidence for disordered eating, depressed mood, and sexual dysfunction. In: Calogero RM, Tantleff-Dunn S, Thompson JK, editors. Self-objectification: Causes, consequences, and counteractions. Washington, DC: American Psychological Association; 2011. pp. 139–159. [Google Scholar]
- Tiggemann M. Objectification theory: Of relevance for eating disorder researchers and clinicians? Clinical Psychologist. 2013;17(2):35–45. doi: 10.111/cp.12010. [DOI] [Google Scholar]
- Tiggemann M, Kuring J. The role of body objectification in disordered eating and depressed mood. British Journal of Clinical Psychology. 2004;43(3):299–311. doi: 10.1348/0144665031752925. [DOI] [PubMed] [Google Scholar]
- Tiggemann M, Lynch JE. Body image across the life span in adult women: The role of self-objectification. Developmental Psychology. 2001;37(2):243–253. doi: 10.1037/0012-1649.37.2.243. [DOI] [PubMed] [Google Scholar]
- Tiggemann M, Martins Y, Kirkbride A. Oh to be lean and muscular: Body image ideals in gay and heterosexual men. Psychology of Men and Masculinity. 2007;8(1):15–24. doi: 10.1037/1524-9220.8.1.15.. [DOI] [Google Scholar]
- Tiggemann M, Slater A. A test of objectification theory in former dancers and non-dancers. Psychology of Women Quarterly. 2001;25(1):57–64. doi: 10.1111/1471-6402.00007. [DOI] [Google Scholar]
- Tiggemann M, Williams E. The role of self-objectification in disordered eating, depressed mood, and sexual functioning among women: A comprehensive test of objectification theory. Psychology of Women Quarterly. 2012;36(1):66–75. doi: 10.1177/0361684311420250. [DOI] [Google Scholar]
- Tylka TL, Hill MS. Objectification theory as it relates to disordered eating among college women. Sex Roles. 2004;51(11–12):719–730. doi: 1573-2762; 0360-0025. [Google Scholar]
- Unger RK, Crawford ME. Women and gender: A feminist psychology. 2nd. New York: McGraw-Hill; 1996. [Google Scholar]
- Van Diest AK, Perez M. Exploring the integration of thin-ideal internalization and self-objectification in the prevention of eating disorders. Body Image. 2013;10(1):16–25. doi: 10.1016/j.bodyim.2012.10.004. [DOI] [PubMed] [Google Scholar]
- Vogeltanz-Holm ND, Wonderlich SA, Lewis BA, Wilsnack SC, Harris TR, Wilsnack RW, Kristjanson AF. Longitudinal predictors of binge eating, intense dieting, and weight concerns in a national sample of women. Behavior Therapy. 2000;31(2):221–235. doi: 10.1016/S0005-7894(00)80013-1. [DOI] [Google Scholar]
- Wichstrom L. Psychological and behavioral factors unpredictive of disordered eating: A prospective study of the general adolescent population in Norway. International Journal of Eating Disorders. 2000;28(1):33–42. doi: 10.1002/(sici)1098-108x(200007)28:1<33::aid-eat5>3.0.co;2-h. [DOI] [PubMed] [Google Scholar]
- Wildes JE, Emery RE, Simons AD. The roles of ethnicity and culture in the development of eating disturbance and body dissatisfaction: A meta-analytic review. Clinical Psychology Review. 2001;21(4):521–551. doi: 10.1016/So272-7358(99)00071-9. [DOI] [PubMed] [Google Scholar]
- Winkelby MA, Gardner CD, Taylor CB. The influence of gender and socioeconomic factors on Latina/White differences in body mass index. Preventive Medicine. 1996;25(2):203–211. doi: 10.1006/pmed.1996.0047. [DOI] [PubMed] [Google Scholar]
- Woolley LM. The relationship of yoga, self-objectification, disordered eating, and depressed mood in college-aged women. Doctoral dissertation. 2009 Retrieved from ProQuest Dissertations and Theses database. (3384574) [Google Scholar]