

Abstract
OBJECTIVES:
The purpose of this pilot study was to evaluate the root lengths of upper incisors as an indication of the degree of orthodontically-induced apical root resorption following treatment with Smart Track® aligners and compare it with two different fixed orthodontic appliances – regular and Damon brackets – using cone-beam computerized tomography (CBCT).
MATERIALS AND METHODS:
The sample comprised 33 patients with class I malocclusion and 4–6 mm crowding divided in 3 groups; Group I: 11 patients treated with Smart Track® aligners, group II: 11 patients treated with Damon brackets, and group III: 11 patients with regular brackets. Maxillary incisors teeth lengths were assessed using Dolphin imaging software before and after treatment. All data were analyzed using analysis of variance and t-test.
RESULTS:
All groups showed statistically significant root resorption, 0–1.4 mm for clear aligners, 0.1–2.3 mm for Damon, and 0–2.5 mm for regular brackets group. However, cases treated with fixed appliance in general showed significantly higher resorption than those treated with Smart Track® aligners (P < 0.05).
CONCLUSION:
Orthodontically-induced root resorption, as evaluated by root length, is an inevitable drawback with different orthodontic techniques. However, the use of Smart Track® aligners showed less root resorption relative to regular fixed appliances.
Keywords: Apical root resorption, clear aligner, self-ligating brackets
Introduction
Orthodontically-induced root resorption is one of the common undesirable sequalae of orthodontic treatment. Literature has shown that most orthodontically-treated patients experience variable degrees of root resorption. The incidence of root resorption during orthodontic treatment varies widely among investigators.[1] In a study by Taithongchai et al.,[2] one-third of the patients treated with fixed appliances showed more than 3 mm of root resorption whereas at least 2% of orthodontic patients showed more than 5 mm of root resorption.
Orthodontically-induced root resorption can affect any tooth in the oral cavity. However, the maxillary central and lateral incisors are considered the most susceptible to resorption.[3]
The exact mechanism of orthodontically-induced root resorption is not clearly understood. However, this phenomenon presents with multifactorial etiology. Several biological, mechanical, and clinical factors were considered for root resorption following orthodontic treatment.[4] Biomechanically, the technique or the appliance used for an orthodontic treatment can be an important determinant factor in the degree of root resorption.[5] In general, light orthodontic forces usually tend to cause less resorption.[6]
The use of passive self-ligating systems with low friction brackets allowed clinicians to apply only light orthodontic forces to move the teeth.[7] However, previous studies on self-ligating bracket systems concluded that orthodontically-induced root resorption occurred similar to conventional preadjusted edgewise bracket systems.[8,9]
There is a controversy in the literature regarding the effect of clear aligners on apical root resorption. One previous study reported that some kinds of removable aligners may have the potential of minimizing orthodontically-induced root resorption due to the studied piezoelectric property by these materials.[10] On the other hand, several studies found no significant differences in the rate of root resorption following treatment with clear aligners compared to conventional fixed orthodontic appliances.[3,11]
Till now, the degree of apical root resorption following treatment with Smart Track® aligners has not been reported in the literature. Therefore, the purpose of this pilot study was to evaluate the degree of orthodontically-induced apical root resorption following treatment with Smart Track® aligners and compare it with two different fixed orthodontic appliances – regular and passive self-ligating brackets.
Materials and Methods
This study was approved by the Human Research Ethics Board (HREB) at the university of Alberta, Edmonton, Alberta. Canada (Protocol # Pro00040543). Sample size was calculated based on a study by Raza et al.,[12] with an alpha error of 0.05 and a beta of 0.2 to achieve a test power of 80%. The sample size calculation showed that 11 patients were needed in each group. Thus, a total of 33 patients were included in this pilot study.
Patients' data were collected from the orthodontic graduate clinic in University of Alberta. Patients with the following inclusion criteria and none of the exclusion criteria were included in the study.
Inclusion criteria:
Males and females between 14 and 25 years of age
Females between 14 and 25 years of age.
Minimum-to-moderate crowding.
All root apices should be completed
Patients should have a cone-beam computed tomography (CBCT) taken before and after orthodontic treatment.
Exclusion criteria:
Class II or class III malocclusion
Severe crowding (more than 7 7sio
History of previous trauma or endodontic treatment.
Patients exhibiting apical root resorption at the pretreatment stage
Patients with parafunctional habits and/or systemic conditions that may affect root resorption
Cases with deep bite (100%) or open bite.
Group I (Smart Track®): 11 patients (5 males and 6 females, mean age of 18.34 ± 2.82 years) were treated with Smart Track® aligners (San Jose, California, USA). Group II (Damon): 11 patients (4 males and 7 females, mean age of 17.71 ± 2.22 years) received treatment with Damon-Q self-ligating brackets (Ormco Corporation 1717 West Collins Avenue Orange, CA). Group III (regular brackets): 11 patients (6 males and 5 females, mean age of 17.34 ± 2.38 years) were treated with regular preadjusted edgewise brackets (3M Unitek, California, USA).
Methods
Digital Vernier caliper and brass wire were used to assess the degree of crowding in the maxillary and mandibular arches. Only patients with 4–6 mm of crowding were included in the study. Assessment of the malocclusion was based on cephalometric measurements using Dolphin imaging software version 11.8. Patients who presented with skeletal and dental class I malocclusion were included in this study. Duration of treatment for each patient was recorded; for Smart Track® group: 15.14 ± 1.94 years, for Damon group: 15.75 ± 1.74 years, and for regular brackets group: 16.22 ± 2.75. years
Radiographic examinations
The lengths of the maxillary central and lateral incisors were measured before and after treatment using CBCT using Mimics software version 19. The incisal edge and root apex were first determined on in the sagittal plane [Figure 1] based upon visual inspection only. If necessary, adjustment of their exact position was made in the coronal plane [Figure 2] and axial plane [Figure 3]. Using the Mimics software, the coordinates of these two points were determined, and the length of each tooth was recorded from the incisal edge to the apex as the distance between these two points.
Figure 1.
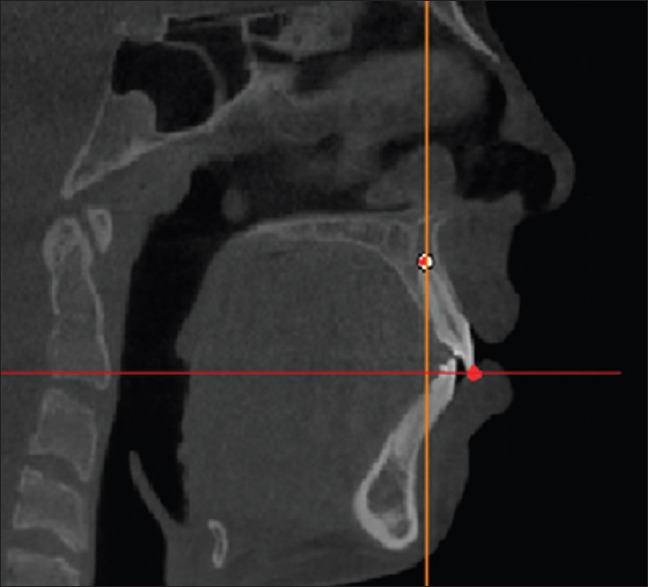
The incisal edge and root apex on in the sagittal plane
Figure 2.
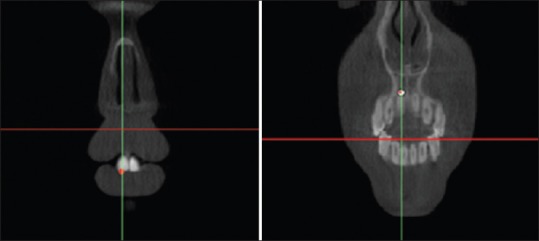
The incisal edge and root apex on in the coronal plane
Figure 3.

The incisal edge and root apex on in the axial plane
Blinding
Evaluation of root resorption was performed by one author who was blinded to the patients' treatment techniques. Further, the investigator was blinded to whether they were before or after treatment. All data were labelled with numbers and sent to a statistician who was also blinded regarding patients' groups.
Study error
Measurements from 18 randomly selected patients, 6 from each group, were repeated after 4-week interval and compared to calculate the measurement errors. Kappa statistics and Dahlberg formula (Se2 = ∑d2/ 2n) were used to calculate the accuracy of measurements,[13] where Se2 is the error variance, d is the difference between repeated measurements, and n is the number of paired repeated measurements.
Statistical analysis
Statistical analysis was performed using SPSS Version 21.0 (SPSS Inc, Chicago, Illinois). Shapiro–Wilk test was used to verify normal distribution of the data. Paired t-test was performed to detect root resorption within each group. Analysis of variance (ANOVA) test was used for comparing the mean changes among the three groups. If a statistically significant difference was found (P < 0.05), a Tukey multiple-comparison test was used.
Results
Kappa statistics showed no significant systematic errors and casual errors (Dahlberg formula) were within acceptable limits (P = 0.740 and Dahlberg = 0.371). This indicates that there was an acceptable reliability in the measurement method.
Groups were comparable regarding patients ages, treatment duration, and pre-treatment crowding as there were no significant differences among all groups (P > 0.05) [Table 1]. Measurements of teeth lengths as well as comparisons before and after treatment for all groups are shown in Tables 2-4. Comparisons among all groups are shown in Table 5.
Table 1.
Comparison of the mean age, treatment duration, and pretreatment crowding among the study groups
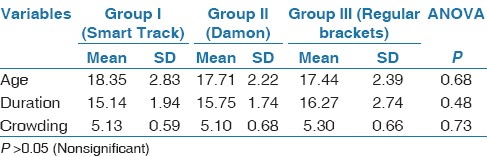
Table 2.
Changes in teeth length measurements in group I (Smart Track®)

Table 4.
Changes in teeth length measurements in group III (preadjusted edgewise brackets)

Table 5.
Comparison of the mean changes in root resorption among all groups

Table 3.
Changes in teeth length measurements in group II (Damon)

In group I (Smart Track® aligners), all maxillary incisors exhibited statistically significant decrease in root length as an indication of root resorption (0.44 ± 0.35; P < 0.05). Root resorption ranged from 0 to 1.4 mm. For group II (Damon), all maxillary incisors showed significant root resorption (0.55 ± 0.38; P < 0.05). The range of resorption was 0.1–2.3 mm. Regarding measurements in group III (preadjusted edgewise brackets), all incisors exhibited significant root resorption (1.04 ± 0.67; P < 0.05); which ranged from 0 to 2.5 mm [Figure 4].
Figure 4.
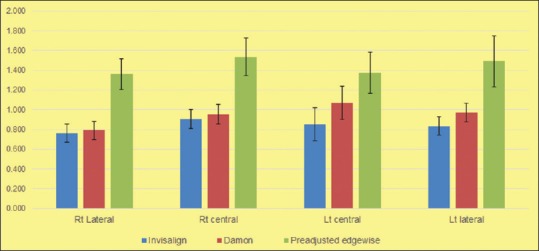
Mean differences of tooth length before and after treatment in mm
Intergroup comparison revealed significant differences in root resorption between group I (Smart Track®) and group III (preadjusted edgewise brackets) (P < 0.05), whereas no significant difference was noted between Smart Track® group and Damon group (P > 0.05). Except for maxillary lateral incisor, no statistically significant difference was found between group Damon and regular brackets groups (P > 0.05).
Discussion
Apical root resorption following orthodontic treatment is still one of the unfavorable consequences of different treatment techniques and appliances. The aim of the present study was to evaluate the degree of root resorption following Smart Track® aligners and compare it with similar cases treated with either a passive-ligating Damon-Q system and the conventional preadjusted edgewise brackets appliances.
The amount of root resorption following orthodontic treatment is associated with treatment duration due to persistent bone turnover associated with prolonged tooth movement.[14] In the current study, the mean treatment duration was similar among all the groups, thus treatment duration did not contribute to any difference in root resorption.
In the present study, only maxillary incisors were selected for evaluating the degree of orthodontically-induced root resorption because these teeth are uni-radicular and usually more affected by resorption than other teeth in the mouth.[15]
The findings of this study showed that all cases treated with Smart Track® aligners showed significantly less root resorption than those treated with conventional preadjusted edgewise brackets appliances. This result is in agreement with a study by Boyd[16] who concluded that aligners could be preprogrammed to control the magnitude of force applied on teeth, and consequently, the stresses on apical area could be controlled to prevent or even minimize the incidence of orthodontically-induced root resorption. A possible explanation of this finding may be attributed to the intermittent forces applied by removable aligners which may allow root cementum to heal, and consequently, further root resorption could be prohibited during the pause.[17] On the contrary, a recently published study[3] found similar predisposition to apical root resorption using either removable aligners or fixed appliances. They suggested that orthodontic forces with either appliances triggers a cellular and molecular responses that would result in root resorption.
The low friction Damon self-ligating bracket system was believed to produce light orthodontic forces which could be more physiological to the periodontal ligaments, and hence, less root resorption would be expected.[7] The findings of the current study did not support this hypothesis. All cases treated with Damon Q showed statistically significant root resorption following orthodontic treatment which indicated that magnitude of orthodontic force was not the main decisive factor in the process of root resorption, and consequently, light orthodontic forces can also cause root resorption.[18] Surprisingly, after analyzing all data, and despite lower values for resorption were found with aligners, we found no statistically significant root resorption between cases treated with Smart Track® aligners and those treated with Damon Q system.
Regarding the difference in root length as a reference of root resorption between self-ligating and conventional bracket systems, the results of this study suggested no significant differences between both systems. This is in accordance with several other studies[8,15] who found similar degrees of root resorption following treatment with either bracket system.
Limitations
The results of the present study should be interpreted with caution. Despite using a three-dimensional imaging method to measure teeth lengths, the use of linear measurements between incisal edge and root apex may be less accurate than the more comprehensive volumetric measures. Fortunately, an ongoing research by the authors using volumetric teeth and roots measurements is under investigation.
Conclusion
According to the results of the present study, orthodontically-induced root resorption is an inevitable drawback with different orthodontic techniques including removable aligners. However, the use of Smart Track® aligners showed less decrease in root length as an indication of decreased root resorption relative to conventional preadjusted edgewise appliances in cases of Class I malocclusion with mild to moderate crowding. No significant difference in root resorption were found between aligners and passive self-ligating Damon Q systems.
Financial support and sponsorship
The authors would like to thank Align Technology, Inc. for supporting this research through the 2016 Align Technology Research Awards Program.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Brezniak N, Wasserstein A. Root resorption after orthodontic treatment: Part 2.Literature review. Am J Orthod Dentofacial Orthop. 1993;103:138–46. doi: 10.1016/S0889-5406(05)81763-9. [DOI] [PubMed] [Google Scholar]
- 2.Taithongchai R, Sookkorn K, Killiany DM. Facial and dentoalveolar structure and the predictionof apical root shortening. Am J Orthod Dentofacial Orthop. 1996;110:296–302. doi: 10.1016/s0889-5406(96)80014-x. [DOI] [PubMed] [Google Scholar]
- 3.Iglesias-Linares A, Sonnenberg B, Solano B, Yanez-Vico RM, Solano E, Lindauer SJ, et al. Orthodontically induced external apical root resorption in patients treated with fixed appliances vs removable aligners. Angle Orthod. 2017;87:3–10. doi: 10.2319/02016-101.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Killiany DM. Root resorption caused by orthodontictreatment: An evidence-based review of literature. Semin Orthod. 1999;5:128–33. doi: 10.1016/s1073-8746(99)80032-2. [DOI] [PubMed] [Google Scholar]
- 5.Sameshima GT, Sinclair PM. Predicting and preventing root resorption: Part II. Treatment factors. Am J Orthod Dentofacial Orthop. 2001;119:511–5. doi: 10.1067/mod.2001.113410. [DOI] [PubMed] [Google Scholar]
- 6.Weltman B, Vig KW, Fields HW, Shanker S, Kaizar EE. Root resorption associated with orthodontic tooth movement: A systematic review. Am J Orthod Dentofacial Orthop. 2010;137:462–76. doi: 10.1016/j.ajodo.2009.06.021. discussion 12A. [DOI] [PubMed] [Google Scholar]
- 7.Damon DH. The Damon low-friction bracket: A biologically compatible straight-wire system. J Clin Orthod. 1998;32:670–80. [PubMed] [Google Scholar]
- 8.Handem RH, Janson G, Matias M, de Freitas KM, de Lima DV, Garib DG, et al. External root resorption with the self-ligating Damon system-a retrospective study. Prog Orthod. 2016;17:20. doi: 10.1186/s40510-016-0133-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Leite V, Conti AC, Navarro R, Almeida M, Oltramari-Navarro P, Almeida R. Comparison of root resorption between self-ligating and conventional preadjusted brackets using cone beam computed tomography. Angle Orthod. 2012;82:1078–82. doi: 10.2319/080911-501.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tawfik A, Hemeda OM, El-Bialy T. Composite Polymers Transducers for Ultrasonic and Biological Applications. Ferroelectrics Lett Section. 2003;30:1–12. [Google Scholar]
- 11.Brezniak N, Wasserstein A. Root resorption following treatment with aligners. Angle Orthod. 2008;78:1119–24. doi: 10.2319/112807-562.1. [DOI] [PubMed] [Google Scholar]
- 12.Raza H, Major P, Dederich D, El-Bialy T. Effect of low-intensity pulsed ultrasound on orthodontically induced root resorption caused by torque: A prospective, double-blind, controlled clinical trial. Angle Orthod. 2016;86:550–7. doi: 10.2319/081915-554.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Houston WJB. The analysis of errors in orthodontic measurements. Am J Orthod. 1983;83:382–390. doi: 10.1016/0002-9416(83)90322-6. [DOI] [PubMed] [Google Scholar]
- 14.Chen W, Haq AAA, Zhou Y. Root resorption of self-ligating and conventional preadjusted brackets in severe anterior crowding Class I patients: A longitudinal retrospective study. BMC Oral Health. 2015;15:115. doi: 10.1186/s12903-015-0100-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Copeland S, Green LJ. Root resorption in maxillary central incisors following active orthodontic treatment. Am J Orthod. 1986;89:51–5. doi: 10.1016/0002-9416(86)90111-9. [DOI] [PubMed] [Google Scholar]
- 16.Boyd RL. Complex orthodontic treatment using a new protocol for the Invisalign appliance. J Clin Orthod. 2007;41:525–47. quiz 523. [PubMed] [Google Scholar]
- 17.Ballard DJ, Jones AS, Petocz P, Darendeliler MA. Physical properties of root cementum: Part 11.Continuous vs intermittent controlled orthodontic forces on root resorption. A microcomputed-tomography study. Am J Orthod Dentofacial Orthop. 2009;136:8e1–8. doi: 10.1016/j.ajodo.2007.07.026. discussion 8-9. [DOI] [PubMed] [Google Scholar]
- 18.Maltha JC, van Leeuwen EJ, Dijkman GE, Kuijpers-Jagtman AM. Incidence and severity of root resorption in orthodontically moved premolars in dogs. Orthod Craniofac Res. 2004;7:115–21. doi: 10.1111/j.1601-6343.2004.00283.x. [DOI] [PubMed] [Google Scholar]