

Abstract
Aims
Frailty is a complex geriatric syndrome resulting in decreased physiological reserves. Frailty and polypharmacy are common in older adults and the focus of extensive studies, although little is known about the impact they may have on each other. This is the first systematic review analysing the available evidence on the relationship between frailty and polypharmacy in older adults.
Methods
Systematic review of quantitative studies. A comprehensive literature search for publications in English or Spanish was performed on MEDLINE, CINAHL, the Cochrane Database and PsycINFO in September 2017 without applying restrictions on the date of publication. Studies reporting any relationship between frailty and polypharmacy in older adults were considered.
Results
A total of 25 publications were included, all of them observational studies. Evaluation of Fried's frailty criteria was the most common approach, followed by the Edmonton Frail Scale and FRAIL scale. Sixteen of 18 cross‐sectional analyses and five of seven longitudinal analyses demonstrated a significant association between an increased number of medications and frailty. The causal relationship is unclear and appears to be bidirectional. Our analysis of published data suggests that polypharmacy could be a major contributor to the development of frailty.
Conclusions
A reduction of polypharmacy could be a cautious strategy to prevent and manage frailty. Further research is needed to confirm the possible benefits of reducing polypharmacy in the development, reversion or delay of frailty.
Keywords: frailty, older adults, polypharmacy, systematic review
Introduction
Frailty is a complex geriatric syndrome resulting in decreased physiological reserves. Over the last few years, it has attracted increasing interest due to its direct relationship with adverse health effects such as physical and functional decline and increased mortality 1, 2. There are different approaches to define and measure frailty, but all of them aim to identify or quantify vulnerability in older adults. There are two main established methods for the evaluation of frailty: i) Fried's criteria 1, which define a clinical syndrome or phenotype, including weight loss, exhaustion, weak grip strength, slow walking speed and low physical activity; and ii) the Frailty Index, first developed by Rockwood et al. 3, which counts accumulated deficits of measures such as symptoms, signs, diseases and disabilities with the hypothesis that the more deficits a person has, the more likely that person is to be frail. This method considers frailty as a multidimensional risk state and measures it by the quantity rather than by the nature of health problems. Sometimes a prefrail category is considered as a third intermediate clinical stage between robust and frail individuals 1.
Similarly, polypharmacy or the use of multiple medications has also been categorized as a geriatric syndrome and is frequently present in older adults 4. Polypharmacy is a major issue of concern for its association with adverse health outcomes, including falls, functional impairment, adverse drug reactions, increased length of hospital stay, readmissions and mortality 5, 6, 7. Multiple factors positively associated with polypharmacy such as drug–drug interactions, drug–disease interactions or potentially inappropriate prescriptions may be involved in these adverse outcomes 8. Thus, polypharmacy is considered an important and increasing challenge in clinical practice.
Frailty and polypharmacy are common and widely studied entities in geriatric patients, although little is known about the impact they may have on each other 9. It is possible to imagine a network of connections through which drugs and frailty might interact, including physiological changes, multiple pathologies and chronic diseases, life expectancy, or functional or cognitive status. Frailty may influence a number of factors, including drugs pharmacokinetics and pharmacodynamics, toxicity, and their therapeutic efficacy. In turn, these factors may be involved in the development of frailty or in ways to prevent it. In the past few years, an increasing number of studies have tried to resolve and measure the relationship between frailty and polypharmacy and its underlying mechanisms.
Here, we aim to analyse the available research evidence on the relationship between frailty and polypharmacy in older adults.
Methods
Search strategy
The study was undertaken in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) statement 10 (see Supporting Information) and the method used was based on the minimum criteria established by the Cochrane Back Review Group (CBRG) 11.
A scientific literature search was conducted in September 2017 to identify all relevant studies published in English or Spanish without applying date restrictions. Queries of the literature were performed using the electronic databases PubMed (MEDLINE), CINAHL (Cumulative Index to Nursing and Allied Health Literature), the Cochrane Library (DARE, HTA, EED, CDSR, CENTRAL), and PsycINFO.
The literature search was designed with Medical Subject Headings (MeSH) terms for MEDLINE and adapted to the other databases according to their descriptors or by using keywords. A combination of the following search terms was used: (“frail elderly” or frail*) AND (“drug prescriptions” OR “drug therapy” OR “polypharmacy” OR “prescription drugs”) (see Supporting Information). Also, the reference lists were examined to detect studies potentially eligible for inclusion.
Selection criteria
Original quantitative studies, regardless of their design, examining any relationship between frailty and polypharmacy in older adults were included. Frailty had to be defined with a validated measurement tool, or a nonvalidated but available and well described one. Case reports, case series, single‐case studies, conference proceedings, letters to the editor, dissertations, review articles or systematic reviews and meta‐analyses were excluded. Authors were contacted to provide missing data when necessary.
The exclusion criteria were:
Studies with participants with mean age <65 years.
Studies focused exclusively on cancer, due to the unique features of the patients and the treatments used.
Data extraction
Two authors (M.G.V., N.M.V.) independently screened the titles and abstracts of potentially eligible studies identified by the search strategy. If necessary, a third researcher (A.C.H.) was consulted. Next, they examined the potentially eligible articles after a first evaluation of the whole text and selected those that met the inclusion standards for this review. The reviewers extracted relevant data from the selected articles, including study design, setting, number and characteristics of study participants, analysed measurements, and outcomes. Outcome measures extracted from included studies are detailed in Table 1.
Table 1.
List of outcome measures extracted from included studies
| Outcomes of interest | Measures/units | Studies |
|---|---|---|
| Correlation between number of medications/polypharmacy groups and level of frailty |
Regression coefficient (b) Semipartial correlation coefficient (r) OR IRR |
21, 22, 25, 27 |
| Average number of medications according to frailty status | Number of medications | 17, 18, 26, 28, 30, 33, 36, 40 |
| Average frailty score according to polypharmacy group | Frailty score | 25, 34 |
| Prevalence of polypharmacy according frailty status | % participants OR | 19, 31, 36 |
| Prevalence of frailty according to polypharmacy group/number of drugs | % participants OR | 20, 23, 24, 26, 32, 35, 38, 44 |
| Incidence of polypharmacy according to frailty status | % participants OR | 39 |
| Incidence of frailty according to polypharmacy group/ number of drugs | % participants OR | 23, 35, 38, 41 |
| Transitions between frailty states according to polypharmacy group/ number of drugs | HR OR | 29, 37 |
HR, hazard ratio; IRR, incidence rate ratio; OR, odds ratio
Quality of the studies
Two researchers assessed the quality of the studies and any differences were resolved by consensus. For longitudinal observational studies, the Newcastle–Ottawa Scale (NOS) 12 was used, and for cross‐sectional studies a modified NOS (see Supporting Information) was used, as described in previous studies 13, 14. The NOS assigns up to a maximum of nine points and the adapted NOS up to a maximum of 10, based on three quality parameters: selection, comparability and outcome.
Nomenclature of targets and ligands
Key protein targets and ligands in this article are hyperlinked to corresponding entries in http://www.guidetopharmacology.org, the common portal for data from the IUPHAR/BPS Guide to PHARMACOLOGY 15, and are permanently archived in the Concise Guide to PHARMACOLOGY 2017/18 16.
Results
Search results
The search identified 1236 nonduplicated references, with 87 classified as potentially relevant after checking the titles and abstracts. After the screening of the full texts, 62 articles were excluded because they did not meet the inclusion criteria. Therefore, 25 publications were ultimately selected and included in the review 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41 (Figure 1).
Figure 1.
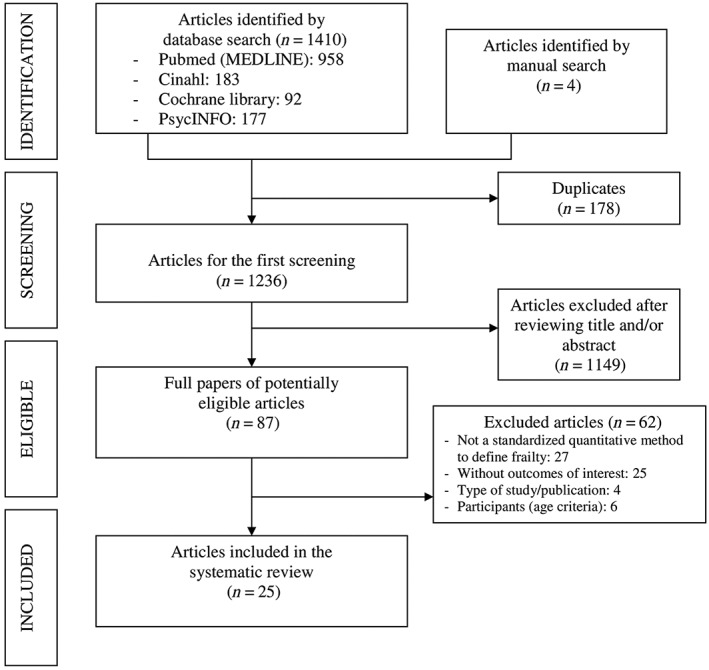
Flowchart of the selection process of study publications
Quality (risk of bias)
All 25 publications included in the study were considered of acceptable quality. Studies assessed through NOS had a median score of 7.5 out of 9 (range: 6–8). Studies assessed through adapted NOS for cross‐sectional studies had a median score of 8 out of 10 (range: 6–9). The quality assessment of the included studies is shown in Figure 2.
Figure 2.

(a) Newcastle–Ottawa Quality Assessment Scale for exposure and outcome of interest in cohort‐studies. (b) Modified Newcastle–Ottawa Quality Assessment Scale for exposure and outcome of interest in cross‐sectional studies
Characteristics of studies and participants
All studies were published from 2009 until 2017 and only five were published >5 years ago. All the studies were observational; 11 were cross‐sectional studies and 14 were prospective cohort studies. However, in some of them, outcomes of interest for this review were obtained from cross‐sectional analyses of baseline data 18, 19, 22, 28, 33, 34. Different measurements or definitions of frailty were used: Fried's criteria with various adjustments were the most used tool (in 14 studies), followed by the Edmonton Frail Scale (in four studies), the FRAIL scale (in three studies), the Frailty index (FI, based on Rockwood's cumulative deficits; in two studies), and the Portuguese version of the Tilburg Frailty Indicator and the Groningen Frailty Indicator (in one study). Frailty cut‐off scores varied depending on the method used for measurement. In some of the studies two groups of patients were defined (frail and robust/nonfrail) and other studies included a third group, consisting of prefrail subjects. Definitions of polypharmacy varied between studies, from more than three to more than six medications, but the most repeated definition is the use of five or more drugs. Some studies also defined a third category among polypharmacy groups, when 10 or more drugs were consumed: hyperpolypharmacy 24, 34, 35, 36 or excessive polypharmacy 26, 27, 38.
Sample size ranged between 31 participants in Hilmer et al. 28 and 10 039 in Zheng et al. 41. Most studies (n = 13) included patients aged 65 years or older and the cut‐off age ranged from 50 35 to 80 years 38. Based on previous data, the mean age varied noticeably between 69.6 years in Saum et al. 35 and 85.2 in Wang et al. 38. The prevalence of frailty ranged between 6.2% 31 and 76% 25. Regarding study setting, 13 studies included community‐dwelling individuals, five studies included hospitalized patients in acute units and the rest included outpatients, care home residents or mixed populations. Participants had to meet specified inclusion criteria in some of the studies, such as the use of http://www.guidetopharmacology.org/GRAC/ObjectDisplayForward?objectId=639#Inhibitors 36 or disability 22; or exclusion criteria, including shorter life expectancy 38, 39, severe cognitive 21, 33 or functional 36 impairment, or the presence of cancer or other advanced diseases 33.
Objectives and measurements analysed
The objectives and variables of the studies included in this review were heterogeneous. Most of the studies provide outcomes of interest in a circumstantial way when describing their participant characteristics, and only some studies were aimed at analysing the possible association or interaction between frailty and polypharmacy or the number of medications used 21, 23, 24, 26, 27, 29, 35, 37, 38, 39, 41. The included studies present a wide range of outcome measures of interest; the most important are shown in Table 1.
Frailty and polypharmacy/number of drugs
Eighteen cross‐sectional analyses assessed the link between polypharmacy and frailty status in various populations, and 16 demonstrated a significant association. From seven longitudinal analyses, five demonstrated significant associations. Table 2 summarizes the most relevant characteristics and outcomes extracted from included studies. Most of the results come from cross‐sectional studies. Several studies show that the mean drug consumption by frail patients is higher than that of robust ones 17, 18, 26, 28, 30, 36, 40, although in Perera et al. 33 the difference was not statistically significant for a group of hospitalized patients aged ≥70 years with atrial fibrillation. Gnjidic et al. 23 established that the optimal discriminating number of concomitant medications associated with the presence of frailty was 6.5. Other studies revealed that the prevalence of frailty was higher among patients with polypharmacy or hyperpolypharmacy (≥10 drugs) 20, 24, 35. This was not the case in the study by Wang et al. 38 in which an inverse relationship was determined with a sample of 1592 men aged ≥80 years. Another study by Gnjidic et al. also showed a greater prevalence of prefrailty in increasing polypharmacy groups 24.
Table 2.
Characteristics and main outcomes of included studies
| Authors, year [ref] | Design of the study | Country/ setting | Characteristics of the participants | Definition of frailty | Measurements | Outcomes |
|---|---|---|---|---|---|---|
| Ballew et al ., 2017 17 | Cross‐sectional study | USA. Community‐dwelling |
4987 >65 years Nonfrail 75.4 ± 5.1 Frail 78.0 ± 5.6 |
Fried ≥3: frail |
Average number of drugs according to frailty status | Nonfrail 8.8 ± 4.6 vs. frail 10.5 ± 5.0 |
| Bennett et al ., 2014 18 | Cohort study, cross‐sectional analysis of baseline data for outcomes of interest | Australia. Hospitalized |
204 ≥60 years. 80.5 ± 8.3 years 65% female |
Reported Edmonton Frail Scale ≥8: frail |
Average number of drugs according to frailty status |
At admission (nonfrail 4.4 ± 3.3 vs. frail 9.8 ± 4.3) At discharge (nonfrail 4.9 ± 3.3 vs. frail 10.3 ± 4.2) (P < 0.0001) |
| Bonaga et al ., 2017 19 | Cohort study, cross‐sectional analysis of baseline data for outcomes of interest | Spain. Population based |
773 ≥ 70 years 78.5 ± 5.8 years 59.1% female |
Fried 0: nonfrail 1–2: prefrail ≥3: frail |
Prevalence of polypharmacy (≥ 5 drugs) according to frailty status | Nonfrail 40.2% vs. prefrail 63.5% vs. frail 81.9% |
| Castell et al ., 2013 20 | Cross‐sectional study | Spain. Urban population in primary care |
1327 ≥65 years 75.4 ± 7.4 years 53.4% female |
Fried ≥3: frail |
‐ Prevalence of frailty according polypharmacy groups (≥ 5 drugs) ‐ OR for frailty according to increasing number of drugs (higher for each additional drug) |
With polypharmacy: 14.9%; without polypharmacy: 4.9%; P < 0.001 OR:1.17 (95% CI 1.08–1.26) |
| Coelho et al ., 2015 21 | Cross‐sectional study | Portugal. Community‐dwelling |
252 ≥65 years 79.2 ± 7.3 years 75.8% female |
Tilburg Frailty Indicator Portuguese version. (0–15) |
Association between number of drugs and frailty by a hierarchical multiple regression analysis |
Regression coefficient: 0.20 (P < 0.001) (95% CI 0.08–0.3) Semi‐partial correlation coefficient: 0.16 Higher number of drugs is associated to greater levels of frailty (not maintained when drug type is introduced in the regression model) |
| Crentsil et al ., 2010 22 | Cohort study, cross‐sectional analysis of baseline data | USA. Community‐dwelling |
1002 disabled women ≥65 years 78.3 ± 8.1 years |
Fried ≥3: frail <3: nonfrail |
OR for the use of a larger number of drugs according to the presence of frailty | OR:1.10 (95% CI 1.01–1.20) |
| Gnjidic et al ., 2012 23 | Cohort study | Australia. Community‐dwelling |
1705 men ≥70 years 76.9 ± 5.5 years |
Fried 0: nonfrail 1–2: prefrail ≥3: frail |
‐ Cut‐off drug score for presence of frailty: ‐ OR for frailty according increasing number of drugs (higher for each additional drug) |
Cut‐off score: 6.5 drugs OR 1.13 (95% CI 1.06–1.21) (P = 0.0002) |
| Gnjidic et al ., 2012 24 | Cohort study | Australia. Community‐dwelling |
1662 men ≥70 years 76.9 ± 5.4 years |
Fried 0: nonfrail 1–2: prefrail ≥3: frail |
‐ Prevalence of prefrailty and frailty according to polypharmacy group ‐ OR for frailty according to polypharmacy group ‐ Incidence of frailty at two years: OR for frailty according to polypharmacy group |
Robust/prefrail/frail (%) (P < 0.0001) Polypharmacy (≥5) 27.2/44.4/64.7 Hyperpolypharmacy (≥10) 1.9/5.3/17.3 Polypharmacy OR 2.55 (95% CI 1.69–3.84) Hyperpolypharmacy OR 5.80 (95% CI 2.90–11.61) Polypharmacy OR 2.45 (95% CI 1.42–4.23) Hyperpolypharmacy OR 2.5 (95% CI 0.76–8.26) |
| Hasan et al ., 2017 25 | Cross‐sectional study | Malaysia. Care home residents |
202 ≥65 years 76.8 ± 7.8 years 62% female |
Groningen Frailty Indicator (GFI) ≥4: frail |
‐ Average GFI score according to polypharmacy group ‐ Relationship between GFI and number of medications used per participant |
With polypharmacy: 7.2 ± 3.4; without polypharmacy: 5.7 ± 3.6 (P = 0.002) Significantly and positively correlated (r = 0.21, P = .002) |
| Herr et al ., 2015 26 | Cross‐sectional study | France. Community‐dwelling |
2350 ≥70 years 83.3 ± 7.5 years 59.4% female |
Fried 1–2: prefrail ≥3: frail |
‐ Average number of drugs according to frailty status ‐ For each additional drug: OR for pre‐frailty OR for frailty ‐ According to the presence of polypharmacy (5–9) OR for pre‐frailty OR for frailty ‐ According to the presence of excessive polypharmacy (≥10) OR for prefrailty OR for frailty |
Nonfrail/prefrail/frail: 4.6/6.1/7.1 (P < 0.001) OR 1.12 (95% CI 1.07–1.17) OR 1.20 (95% CI 1.12–1.28) OR 1.82 (95% CI 1.44–2.37) OR 1.77 (95% CI 1.20–2.61) OR 2.51 (95% CI 1.49–4.23) OR 4.47 (95% CI 2.37–8.42) |
| Herr et al ., 2017 27 | Cross‐sectional study | France. Community‐dwelling |
1890 ≥ 5 years 74.7 ± 7.4 years 60.5% female |
Fried ≥3: frail |
IRR number of frailty criteria ‐ polypharmacy 5–9 vs. 0–4 drugs 10+ vs. 0–4 drugs |
1.587 (P < 0.001). With confounders 1.163 (P < 0.05) 2.710 (P < 0.001). With confounders 1.451 (P < 0.001) |
| Hilmer et al ., 2011 28 | Cohort study, cross‐sectional analysis of baseline data for outcomes of interest | Australia. Hospitalized |
31 ≥65 years 77.0 ± 7.1 years 19.4% female |
Reported Edmonton Frail Scale ≥8: frail <8: not frail |
Average number of drugs according to frailty status | Frail 4.6 ± 2.0 vs. nonfrail 2.1 ± 1.8 (P = 0.001) |
| Jamsen et al ., 2016 29 | Cohort study | Australia. Community‐dwelling |
1705 men ≥70 years 76.9 ± 5.5 years |
Fried 0: robust 1–2: prefrail ≥3: frail |
HR for transition to a state of ‐ prefrailty ‐ frailty by increasing number of drugs |
HR 1.04 (95% CI 1.00–1.09) HR 1.06 (95% CI 0.99–1.13) |
| Jung et al ., 2016 30 | Cross‐sectional study | Korea. Outpatient and impatient |
103 ≥65 years 76.8 ± 6.1 years 46.6% female |
FRAIL scale (Korean version) 0: robust 1–2: prefrail ≥3: frail |
Average number of drugs according to frailty status | Robust 5.4 ± 3.7 vs. prefrail 6.4 ± 4.4 vs. frail 9.0 ± 4.3 (P = 0.014) |
| Merchant et al ., 2017 31 | Cross‐sectional study | Singapore. Community‐dwelling |
1051 71.2 years 57.2% female |
FRAIL scale 1–2: prefrail ≥3: frail |
Prevalence of polypharmacy (≥5) according to frailty status | Robust 18.1%, prefrail 29.8%, frail 41.5% (P < 0.001) |
| Moulis et al ., 2015 32 | Cross‐sectional study | France. Outpatient |
437 ≥65 years 83.05 ± 6.5 years 62.7% female |
Fried 1–2: prefrail ≥3: frail |
OR for frailty according to the presence of polypharmacy (≥6) | OR 1.85 (95% CI 1.21–2.82. P < 0.02) |
| Perera et al ., 2009 33 | Cohort study, cross‐sectional analysis of baseline data for outcomes of interest | Australia. Hospitalized |
220 ≥70 years 82.7 ± 6.3 years 54% female |
Edmonton Frail Scale | Average number of drugs according to frailty status | Frail 8.2 ± 3.2 vs. nonfrail 7.8 ± 3.6 (P NS) |
| Poudel et al ., 2016 34 | Cohort study, cross‐sectional analysis of baseline data for outcomes of interest | Australia. Hospitalized |
1418 ≥70 years 81.0 ± 6.8 years 55% female |
Frailty index Low: 0–0.25 Mean: 0.26–0.39 High: ≥ 0.4 |
Average FI according to polypharmacy group |
0–4 drugs FI 0.30 ± 0.17 5–9 FI 0.32 ± 0.15 ≥10 FI 0.34 ± 0.13 (P = 0.003) |
| Saum et al ., 2016 35 | Cohort study | Germany. Community‐dwelling |
3058 patients (50–75 years) 69.6 ± 6.3 years 52.4% female |
Fried 0: nonfrail 1–2: prefrail ≥3: frail |
‐ Prevalence of frailty according to polypharmacy group ‐ OR for prefrailty according to the presence of polypharmacy hyperpolypharmacy ‐ OR for frailty according to the presence of polypharmacy hyperpolypharmacy ‐ Incidence of frailty by polypharmacy group ‐ OR for incident prefrailty according to the presence of polypharmacy hyperpolypharmacy ‐ OR for incident frailty according to the presence of polypharmacy hyperpolypharmacy |
Hyperpolypharmacy (≥ 10): 24.9% Polypharmacy (5–9) 12.1%. No polypharmacy (0–4) 3.7% (P < 0.01) OR 1.20 (95% CI 1.00–1.44) OR 1.48 (95% CI 1.03–2.14) OR 2.30 (95% CI 1.60–3.31) OR 4.97 (95% CI 2.97–8.32) No polypharmacy: 5.8%; polypharmacy: 13.0%, hyperpolypharmacy 19.3% OR 1.33 (95% CI 1.05–1.67) OR 1.86 (95% CI 1.11–3.10) OR 1.85 (95% CI 1.24–2.76) OR 3.08 (95% CI 1.55–6.12) |
| Thai et al ., 2015 36 | Cross‐sectional study | Australia. Hospitalized (acute) |
180 patients ≥65 years, Median 78 years (IQR = 14) 47.2% female |
Reported Edmonton Frail Scale 0–7: robust ≥8: frail |
‐ Average number of drugs according to frailty status ‐ Prevalence of polypharmacy (≥ 5 drugs) according to frailty status ‐ Prevalence of 5–9 drugs according to frailty status ‐ Prevalence of hyperpolypharmacy (≥10 drugs) according to frailty status |
Robust 8 (IQR 4) vs. frail 9 (IQR 5) R 92.3% vs. F 96.9% R 64.1% vs. F 54.0% R 28.2% vs. F 42.9%. P = 0.095 |
| Trevisan et al ., 2016 37 | Cohort study | Italy. Outpatient |
2925 patients ≥65 years 74.4 ± 7.3 years 59.7% female |
Fried 1–2: prefrail ≥3: frail |
OR for transitions to prefrailty or frailty status according to use of >3 drugs |
Univariate analysis: OR from nonfrail: 1.24 (1.13–1.37) (P < 0.0001) OR from prefrail: 1.55 (1.39–1.73) (P < 0.0001) Multivariate analysis: OR from nonfrail: 1.05 (0.94–1.17) OR from prefrail: 1.04 (0.92–1.18) |
| Wang et al ., 2015 38 | Cohort study | China. Outpatient |
1592 men ≥80 years 85.2 (80–104) years |
Fried ≥3: frail |
‐ Prevalence of frailty according to baseline polypharmacy group ‐ Prevalence of frailty according to polypharmacy group at 5 years ‐ OR for incident frailty according to increasing number of drugs |
No polypharmacy (0–5): 30.5%, polypharmacy (6–9): 29.3%, excessive polypharmacy (≥ 10): 29.6% (P = 0.261). No polypharmacy: 42.7%, polypharmacy: 34.2%, excessive polypharmacy: 33.7% (P < 0.05). OR 1.06 (95% CI 1.02–1.11) |
| Woo et al ., 2014 39 | Cohort study | Hong Kong. Community‐dwelling | 4000 patients ≥65 years |
Fried 1–2: prefrail ≥3: frail |
‐ Prevalence of polypharmacy (≥ 4) after a follow‐up period according to baseline frailty status ‐ OR for polypharmacy after a follow‐up according to baseline frailty status |
Robust: 13.7%; prefrail: 18.9%; frail 21.5% (P = 0.7036). OR according to two models: 1.36 (95% CI 0.72–2.56). 1.30 (95% CI 0.68–2.48) |
| Woo and Leung, 2015 40 | Cross‐sectional study | Hong Kong. Community‐dwelling |
816 ≥65 years 58.9% ≥75 years 85.4% female |
FRAIL Scale 0: robust 1–2: prefrail ≥3: frail |
Average number of drugs according to frailty status | Frail 4.3 ± 2.9; nonfrail 2.9 ± 2.2 (P = 0.001) |
| Zheng et al ., 2016 41 | Secondary analysis of a cohort study | China. Community‐dwelling |
10 039 ≥55 years 70.5 ± 7.8 years 61.3% female |
FI 34 items Frailty FI ≥0.25 |
OR for incident frailty according to the presence of polypharmacy (≥ 4drugs) |
Adjusted OR = 1.37 (P < 0.05). |
Furthermore, several studies show the likelihood of being frail increasing with every medication added to the treatment (odds ratio 1.13–1.20) 20, 23, 26, with polypharmacy (odds ratio 1.77–2.55) 24, 26, 32, 35, and with hyperpolypharmacy (odds ratio 4.47–5.8) 24, 26, 35. Some of these studies report the same results when the status of prefrailty was examined 26, 35, although the relationship was not always linear when the three groups (robust, prefrail, frail) were considered 26. In another study by Coelho et al. 21, the association was found only with the physical frailty domain, and not with psychological and social domains. Additionally, the relationship between frailty and the use of a larger number of drugs was not significant in analyses with more complex multivariate regression models including the type of medication used. Herr et al. show that polypharmacy was associated with the number of frailty criteria in models adjusted for socio‐demographic and health characteristics in a French representative study with people aged ≥65 years 27. Poudel et al. 34 and Hasan et al. 25 identified an increase in the mean frailty index and Groningen Frailty Indicator associated to polypharmacy category: (hyperpolypharmacy>) polypharmacy>no polypharmacy. Similarly, Crentsil et al. 22 reported a higher probability of consuming more medications in association with frailty (OR 1.10). Bonaga et al. 19 and Merchant et al. 31 showed that the prevalence of polypharmacy was higher in frail patients. Furthermore, Thai et al. 36 found the same trend with polypharmacy and hyperpolypharmacy, but without statistically significant differences.
Regarding longitudinal studies, Woo et al. 39 did not find statistically significant differences in the incidence of polypharmacy (≥4) after 4 years according to baseline frailty. Other studies with a prospective design showed a higher incidence of frailty or probability of becoming frail when a larger number of drugs was taken 38 or with the presence of polypharmacy/hyperpolypharmacy 24, 35, 41. However, Jamsen et al. 29 did not find a relationship between the use of a larger number of drugs and transitions to prefrailty or frailty state after a 5‐year follow‐up period. Trevisan et al. 37, found an association between transitions to prefrailty or frailty and the use of >3 drugs with a univariate analysis, but not with a multivariate analysis after a 4‐year follow‐up.
Discussion
Here, we aim to summarize the evidence available to date on the relationship between frailty and polypharmacy in older adults. To the best of our knowledge, this is the first systematic review evaluating this relevant health issue. Frailty is a recent concept that is increasingly attracting interest, as evidenced by the contemporaneity of most of the publications evaluated.
Many different outcome measures regarding the interaction between frailty and polypharmacy have been examined, yielding a large amount of information. However, the observational design of the studies did not allow for the analysis of high‐quality evidence. Nevertheless, the association between frailty and polypharmacy in older people seems clear, despite the various study designs, measurements or patient groups evaluated.
The first difficulty encountered when analysing the ensemble of selected studies was the lack of homogeneity in the definition and quantification of frailty. The different scales used and their underlying concepts lead to a wide variability in the calculation of prevalence and incidence of frailty, prefrailty and of all outcomes associated with these syndromes 42. Additionally, different study settings, age ranges and pathologies of the participants, or differences in inclusion or exclusion criteria may influence the results and conclusions of every study.
The association between frailty and polypharmacy seems so evident that even some scales or tools to measure frailty, including the Edmonton Frail Scale, the Groningen Frailty Indicator or some versions of Frailty Index include the consumption of drugs. To properly examine the relationship between polypharmacy and frailty, the number of medications used should have been excluded for assessing frailty status, as done in the study by Poudel et al. 34.
Although polypharmacy is a widespread concept, there is not a single and clear definition for it 43. Different definitions of polypharmacy of included studies (from >3 to ≥6) 32, 37 may lead to confusion and difficulty when comparing results and drawing general conclusions. A low threshold for defining polypharmacy could explain the difficulty in demonstrating a significant association between polypharmacy and frailty. For example, Trevisan et al. 37 did not find an association between transitions to prefrailty or frailty and the use of more than three drugs with a multivariate analysis. This could be a consequence of selecting the low threshold of three drugs. In a sample of community‐dwelling men aged ≥70 years in Australia, Gnjidic et al. 23 defined a cut‐off score of 6.5 drugs as the best discriminatory number for frailty. Moulis et al. 44 presented a similar analysis with men and women aged ≥65 years in France, reporting a cut‐off score of at least six drugs. It may be interesting to assume this threshold to standardize the definition of polypharmacy in future studies about the relationship of polypharmacy and frailty, or to use the mean number of drugs instead of a cut‐off.
Another possible limitation of our analysis of published data is the fact that most of the studies were not designed to determine the association between frailty and polypharmacy (it was not the primary outcome). Thus, the sample size of some of the studies may not provide enough power to find significant associations. From the four publications that did not find any association between frailty and polypharmacy 29, 33, 36, 39, two of them did not describe it among their objectives and had small sample sizes (180 and 220) 33, 36. Jamsen et al. 29 and Woo et al. 39 had the association between frailty and polypharmacy as a primary outcome and have large sample sizes (1705 and 4000 participants). It should be noted that results from Jamsen et al. 29 and Gnjidic et al. 23, 24 come from the same pool of participants, and that Bennett et al. 18, Hilmer et al. 28, Perera et al. 33 and Thai et al. 36 all use small inpatient cohorts from the same hospital. Repeated analyses within the same or similar populations do not provide additional evidence.
Despite the obvious association, it is difficult to establish causality and determine what occurs first: frailty or polypharmacy. Longitudinal studies measuring the impact of polypharmacy in the incidence of frailty could be important in this regard. Several studies reported a higher probability of becoming frail over time in patients with polypharmacy 24, 35, 41, although in another study this association was not maintained following a multivariate analysis 37. A recent study by Veronese et al. 45, that has not been selected for this review because it included younger individuals, showed, after a 8‐year follow‐up of 4402 participants at baseline, that use of four to six medications had a higher risk of developing frailty. Those using more than seven drugs were at even higher risk. Wang et al. 38 concluded that the risk of developing frailty increases with the number of medications taken, although Jamsen et al. did not achieve conclusive results in a similar analysis after a 5‐year follow‐up period 29. Of note, all these studies used adjusted models including comorbidity as a covariate (comorbidity indexes or presence or number of different chronic diseases). Thus, comorbidities may not be the only cause of increased risk of frailty associated to polypharmacy. Conversely, Woo et al. assessed the incidence of polypharmacy over time according to frailty status but no clear association was identified 39. The relationship between frailty and polypharmacy has also been addressed in animal models. Huizer‐Pajkos et al. 46 performed an interventional mouse study of short‐term polypharmacy that showed a nonsignificant trend towards increased frailty index after 2–4 weeks of administering polypharmacy in the diet.
The association of frailty and polypharmacy may be complex and bidirectional. On the one hand, frailty is linked to certain chronic diseases and multimorbidity 47, which can consequently lead to polypharmacy. On the other hand, there are plausible mechanisms by which drugs may affect the development of frailty. As indicated by Gnjidic and Hilmer 48, several elements that may be considered clinical components or characteristics of frailty have been directly linked with the number of drugs taken, including weight loss, balance disorders, poor nutritional status, or functional deterioration 49, 50. The available evidence so far does not allow to confirm which of these elements are involved in the pathogenesis of frailty associated with polypharmacy. However, polypharmacy may be recognized as a major contributor to the development of frailty. Thus, reducing polypharmacy in older adults has been suggested as a recommended measure for both prevention and management of frailty 51. Further studies should be carried out in the future to confirm the possible benefits of reducing polypharmacy in the development, reversion or delay of frailty.
Furthermore, the consumption of a greater number of drugs is associated with an increase in other negative medication‐related variables like drug–drug interactions, potentially inappropriate prescribing, anticholinergic burden of treatments or adverse drug reactions 52, 53, 54. This may explain why some studies have found a higher proportion of these factors in frail older people and suggest other possible mechanisms by which polypharmacy interferes with frailty 18, 24, 29, 32, 36, 55, 56.
In addition to the reciprocal impact that frailty and polypharmacy may have on each other, some studies suggest that they can act as modulators for their negative effect in health outcomes, so their interaction could determine the frequency of some health‐related adverse events. Bonaga et al. 19 showed that polypharmacy was associated with an increased risk of adverse events (disability, hospitalization, emergency department visits and mortality) in prefrail and frail older adults, but not in nonfrail individuals. Herr et al. showed that excessive polypharmacy and frailty are independent risk factors for mortality, but the combination of both multiplied by 6.30 the risk of dying during a 2.6–year‐follow‐up period 26.
It is also worth noting that the relationship between frailty and medications is a very complex issue. There seems to be a stronger association between frailty and changes in pharmacokinetic responses, especially metabolism and excretion, than with chronological age 17, 28. This could also contribute to a higher risk of adverse drug reactions and toxicity in frail older people. Older people seem to have an increased sensitivity to certain drugs, but the evidence of the possible influence of frailty on pharmacodynamics and efficacy is scarce 18, 57, 58, although plausible due to physiological changes 59. Moreover, as a predictor of clinical outcomes and limited life expectancy, frailty may modify the goals of health care and its priorities, and influence decision‐making regarding the use of medicines 21, 56. These issues have been addressed more in depth in other publications 59, 60.
Finally, our study has some potential limitations. Despite the comprehensive search strategy, the heterogeneity of terms and definitions of frailty and polypharmacy may have affected the sensitivity of the search because some plausible data of interest could not be the primary outcome of the studies. Different studies comparing frail and nonfrail participants including polypharmacy in the baseline characteristics may have been missed. However, the selection bias should not affect most relevant studies evaluating the relationship between frailty and polypharmacy as a primary outcome.
Conclusions
Results from this review suggest that polypharmacy is associated with frailty in older people, although the causal relationship is unclear and, in fact, appears to be bidirectional. The lack of standardized definitions for frailty and polypharmacy hinders research in this area and leads to a wide range of outcomes. There is still scarce evidence of the mechanisms involved, and it is difficult to form conclusions on clinical practice based on the observational studies available at the moment. However, polypharmacy may be recognized as a major contributor to the development of frailty. It seems clear that frailty is an important issue that must be taken into account for decision‐making in drug prescribing to older patients, and that polypharmacy should be assessed with special caution in frail older adults. Therefore, it has been suggested that a reduction of polypharmacy could be a strategy to prevent and manage frailty. Further research is needed to confirm the possible benefits of reducing polypharmacy in the development, reversion or delay of frailty.
Competing Interests
There are no competing interests to declare.
M.G.‐V. received a grant from the Specialized Healthcare Post‐training Program from the Complejo Hospitalario de Navarra, Pamplona, Spain. The funding sources had no involvement in the design, analysis and interpretation of data, in the writing of the report or in the decision to submit the article for publication.
Contributors
M.G.‐V. and N.M.‐V. contributed to conception and design, acquisition, analysis and interpretation of data, drafting the article and final approval of published manuscript. M.Iz., M.C., Á.C.‐H. and M.In. contributed to conception and design, analysis and interpretation of data, revising the text and final approval of the version to be published.
Supporting information
Data S1 PRISMA 2009 Checklist
Data S2 Search strategy
Data S3 Modified Newcastle‐Ottawa Scale for cross‐sectional studies
Gutiérrez‐Valencia, M. , Izquierdo, M. , Cesari, M. , Casas‐Herrero, Á. , Inzitari, M. , and Martínez‐Velilla, N. (2018) The relationship between frailty and polypharmacy in older people: A systematic review. Br J Clin Pharmacol, 84: 1432–1444. doi: 10.1111/bcp.13590.
References
- 1. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56: M146–M156. [DOI] [PubMed] [Google Scholar]
- 2. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet 2013; 381: 752–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Rockwood K, Mitnitski A. Frailty in relation to the accumulation of deficits. J Gerontol A Biol Sci Med Sci 2007; 62: 722–727. [DOI] [PubMed] [Google Scholar]
- 4. Jokanovic N, Tan EC, Dooley MJ, Kirkpatrick CM, Bell JS. Prevalence and factors associated with polypharmacy in long‐term care facilities: a systematic review. J Am Med Dir Assoc 2015; 16: 535.e1–535.e12. [DOI] [PubMed] [Google Scholar]
- 5. Jyrkka J, Enlund H, Korhonen MJ, Sulkava R, Hartikainen S. Polypharmacy status as an indicator of mortality in an elderly population. Drugs Aging 2009; 26: 1039–1048. [DOI] [PubMed] [Google Scholar]
- 6. Gomez C, Vega‐Quiroga S, Bermejo‐Pareja F, Medrano MJ, Louis ED, Benito‐Leon J. Polypharmacy in the elderly: a marker of increased risk of mortality in a population‐based prospective study (NEDICES). Gerontology 2015; 61: 301–309. [DOI] [PubMed] [Google Scholar]
- 7. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf 2014; 13: 57–65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hilmer SN, Gnjidic D. The effects of polypharmacy in older adults. Clin Pharmacol Ther 2009; 85: 86–88. [DOI] [PubMed] [Google Scholar]
- 9. Palmer K, Marengoni A, Russo P, Mammarella F, Onder G. Frailty and drug use. J Frailty Aging 2016; 5: 100–103. [DOI] [PubMed] [Google Scholar]
- 10. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP, et al The PRISMA statement for reporting systematic reviews and meta‐analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 2009; 339: b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Furlan AD, Pennick V, Bombardier C, van Tulder M, Editorial Board CBRG . 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila Pa 1976) 2009; 34: 1929–1941. [DOI] [PubMed] [Google Scholar]
- 12. Wells G, Shea B, O'Connell D, Peterson J, Welch V. The Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta‐analyses. Eur J Epidemiol 2011; 25: 603–605. [DOI] [PubMed] [Google Scholar]
- 13. Herzog R, Álvarez‐Pasquin MJ, Díaz C, Del Barrio JL, Estrada JM, Gil Á. Are healthcare workers' intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013; 13: 154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Alshabanat A, Zafari Z, Albanyan O, Dairi M, FitzGerald JM. Asthma and COPD Overlap Syndrome (ACOS): a systematic review and meta analysis. PLoS One 2015; 10: e0136065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Harding SD, Sharman JL, Faccenda E, Southan C, Pawson AJ, Ireland S, et al The IUPHAR/BPS Guide to PHARMACOLOGY in 2018: updates and expansion to encompass the new guide to IMMUNOPHARMACOLOGY. Nucl Acids Res 2018; 46: D1091–D1106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Alexander SPH, Fabbro D, Kelly E, Marrion NV, Peters JA, Faccenda E, et al The Concise Guide to PHARMACOLOGY 2017/18: Enzymes. Br J Pharmacol 2017; 174: S272–S359. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Ballew SH, Chen Y, Daya NR, Godino JG, Windham BG, McAdams‐DeMarco M, et al Frailty, kidney function, and polypharmacy: the atherosclerosis risk in communities (ARIC) study. Am J Kidney Dis 2017; 69: 228–236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Bennett A, Gnjidic D, Gillett M, Carroll P, Matthews S, Johnell K, et al Prevalence and impact of fall‐risk‐increasing drugs, polypharmacy, and drug‐drug interactions in robust versus frail hospitalised falls patients: a prospective cohort study. Drugs Aging 2014; 31: 225–232. [DOI] [PubMed] [Google Scholar]
- 19. Bonaga B, Sánchez‐Jurado PM, Martínez‐Reig M, Ariza G, Rodríguez‐Mañas L, Gnjidic D, et al Frailty, polypharmacy, and health outcomes in older adults: the Frailty and Dependence in Albacete Study. J Am Med Dir Assoc 2018; 19: 46–52. [DOI] [PubMed] [Google Scholar]
- 20. Castell MV, Sanchez M, Julian R, Queipo R, Martin S, Otero A. Frailty prevalence and slow walking speed in persons age 65 and older: implications for primary care. BMC Fam Pract 2013; 14: 86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Coelho T, Paúl C, Gobbens RJJ, Fernandes L. Determinants of frailty: the added value of assessing medication. Front Aging Neurosci 2015; 7: 56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Crentsil V, Ricks MO, Xue QL, Fried LP. A pharmacoepidemiologic study of community‐dwelling, disabled older women: factors associated with medication use. Am J Geriatr Pharmacother 2010; 8: 215–224. [DOI] [PubMed] [Google Scholar]
- 23. Gnjidic D, Hilmer SN, Blyth FM, Naganathan V, Waite L, Seibel MJ, et al Polypharmacy cutoff and outcomes: five or more medicines were used to identify community‐dwelling older men at risk of different adverse outcomes. J Clin Epidemiol 2012; 65: 989–995. [DOI] [PubMed] [Google Scholar]
- 24. Gnjidic D, Hilmer SN, Blyth FM, Naganathan V, Cumming RG, Handelsman DJ, et al High‐risk prescribing and incidence of frailty among older community‐dwelling men. Clin Pharmacol Ther 2012; 91: 521–528. [DOI] [PubMed] [Google Scholar]
- 25. Hasan SS, Kow CS, Verma RK, Ahmed SI, Mittal P, Chong DWK. An evaluation of medication appropriateness and frailty among residents of aged care homes in Malaysia: a cross‐sectional study. Medicine 2017; 96: e7929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Herr M, Robine JM, Pinot J, Arvieu JJ, Ankri J. Polypharmacy and frailty: prevalence, relationship, and impact on mortality in a French sample of 2350 old people. Pharmacoepidemiol Drug Saf 2015; 24: 637–646. [DOI] [PubMed] [Google Scholar]
- 27. Herr M, Sirven N, Grondin H, Pichetti S, Sermet C. Frailty, polypharmacy, and potentially inappropriate medications in old people: findings in a representative sample of the French population. Eur J Clin Pharmacol 2017; 73: 1165–1172. [DOI] [PubMed] [Google Scholar]
- 28. Hilmer SN, Tran K, Rubie P, Wright J, Gnjidic D, Mitchell SJ, et al Gentamicin pharmacokinetics in old age and frailty. Br J Clin Pharmacol 2011; 71: 224–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Jamsen KM, Bell JS, Hilmer SN, Kirkpatrick CM, Ilomäki J, Le Couteur D, et al Effects of changes in number of medications and drug burden index exposure on transitions between frailty states and death: the concord health and ageing in men project cohort study. J Am Geriatr Soc 2016; 64: 89–95. [DOI] [PubMed] [Google Scholar]
- 30. Jung HW, Yoo HJ, Park SY, Kim SW, Choi JY, Yoon SJ, et al The Korean version of the FRAIL scale: clinical feasibility and validity of assessing the frailty status of Korean elderly. Korean J Intern Med 2016; 31: 594–600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Merchant RA, Chen MZ, Tan LWL, Lim MY, Ho HK, van Dam RM. Singapore Healthy Older People Everyday (HOPE) Study: prevalence of frailty and associated factors in older adults. J Am Med Dir Assoc 2017; 18: 734.e9–734.e14. [DOI] [PubMed] [Google Scholar]
- 32. Moulis F, Moulis G, Balardy L, Gerard S, Montastruc F, Sourdet S, et al Exposure to atropinic drugs and frailty status. J Am Med Dir Assoc 2015; 16: 253–257. [DOI] [PubMed] [Google Scholar]
- 33. Perera V, Bajorek BV, Matthews S, Hilmer SN. The impact of frailty on the utilisation of antithrombotic therapy in older patients with atrial fibrillation. Age Ageing 2009; 38: 156–162. [DOI] [PubMed] [Google Scholar]
- 34. Poudel A, Peel NM, Nissen LM, Mitchell CA, Gray LC, Hubbard RE. Adverse outcomes in relation to polypharmacy in robust and frail older hospital patients. J Am Med Dir Assoc 2016; 17: 767.e9–767.e13. [DOI] [PubMed] [Google Scholar]
- 35. Saum KU, Schottker B, Meid AD, Holleczek B, Haefeli WE, Hauer K, et al Is polypharmacy associated with frailty in older people? Results from the ESTHER cohort study. J Am Geriatr Soc 2017; 65: e27–e32. [DOI] [PubMed] [Google Scholar]
- 36. Thai M, Hilmer S, Pearson SA, Reeve E, Gnjidic D. Prevalence of potential and clinically relevant statin‐drug interactions in frail and robust older inpatients. Drugs Aging 2015; 32: 849–856. [DOI] [PubMed] [Google Scholar]
- 37. Trevisan C, Veronese N, Maggi S, Baggio G, Toffanello ED, Zambon S, et al Factors influencing transitions between frailty states in elderly adults: the Progetto Veneto Anziani longitudinal study. J Am Geriatr Soc 2017; 65: 179–184. [DOI] [PubMed] [Google Scholar]
- 38. Wang R, Chen L, Fan L, Gao D, Liang Z, He J, et al Incidence and effects of polypharmacy on clinical outcome among patients aged 80+: a five‐year follow‐up study. PLoS One 2015; 10: e0142123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Woo J, Leung J. Multi‐morbidity, dependency, and frailty singly or in combination have different impact on health outcomes. Age (Dordr) 2014; 36: 923–931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Woo J, Yu R, Wong M, Yeung F, Wong M, Lum C. Frailty screening in the community using the FRAIL Scale. J Am Med Dir Assoc 2015; 16: 412–419. [DOI] [PubMed] [Google Scholar]
- 41. Zheng Z, Guan S, Ding H, Wang Z, Zhang J, Zhao J, et al Prevalence and incidence of frailty in community‐dwelling older people: Beijing Longitudinal Study of Aging II. J Am Geriatr Soc 2016; 64: 1281–1286. [DOI] [PubMed] [Google Scholar]
- 42. Martínez‐Velilla N, Aldaz‐Herce P, Casas‐Herrero Á, Gutiérrez‐Valencia M, López‐Sáez de Asteasu M, Sola‐Mateos S, et al Heterogeneity of different tools for detecting the prevalence of frailty in nursing homes: feasibility and meaning of different approaches. J Am Med Dir Assoc 2017; 10: 898.e1–898.e8. [DOI] [PubMed] [Google Scholar]
- 43. Masnoon N, Shakib S, Kalisch‐Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr 2017; 17: 230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Moulis F, Moulis G, Balardy L, Gerard S, Sourdet S, Rouge‐Bugat ME, et al Searching for a polypharmacy threshold associated with frailty. J Am Med Dir Assoc 2015; 16: 259–261. [DOI] [PubMed] [Google Scholar]
- 45. Veronese N, Stubbs B, Noale M, Solmi M, Pilotto A, Vaona A, et al Polypharmacy is associated with higher frailty risk in older people: an 8‐year longitudinal cohort study. J Am Med Dir Assoc 2017; 18: 624–628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46. Huizer‐Pajkos A, Kane AE, Howlett SE, Mach J, Mitchell SJ, de Cabo R, et al Adverse geriatric outcomes secondary to polypharmacy in a mouse model: the influence of aging. J Gerontol A Biol Sci Med Sci 2016; 71: 571–577. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Newman AB, Boudreau RM, Naydeck BL, Fried LF, Harris TB. A physiologic index of comorbidity: relationship to mortality and disability. J Gerontol A Biol Sci Med Sci 2008; 63: 603–609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48. Gnjidic D, Hilmer SN. Potential contribution of medications to frailty. J Am Geriatr Soc 2012; 60: 401. [DOI] [PubMed] [Google Scholar]
- 49. Jyrkka J, Enlund H, Lavikainen P, Sulkava R, Hartikainen S. Association of polypharmacy with nutritional status, functional ability and cognitive capacity over a three‐year period in an elderly population. Pharmacoepidemiol Drug Saf 2011; 20: 514–522. [DOI] [PubMed] [Google Scholar]
- 50. Agostini JV, Han L, Tinetti ME. The relationship between number of medications and weight loss or impaired balance in older adults. J Am Geriatr Soc 2004; 52: 1719–1723. [DOI] [PubMed] [Google Scholar]
- 51. Morley JE, Vellas B, van Kan GA, Anker SD, Bauer JM, Bernabei R, et al Frailty consensus: a call to action. J Am Med Dir Assoc 2013; 14: 392–397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Iniesta‐Navalon C, Urbieta‐Sanz E, Gascon‐Canovas JJ. Analysis of the drug interactions associated to domiciliary drug therapy in elderly hospitalized patients. Rev Clin Esp 2011; 211: 344–351. [DOI] [PubMed] [Google Scholar]
- 53. Kuijpers MA, van Marum RJ, Egberts AC, Jansen PA, Group OS . Relationship between polypharmacy and underprescribing. Br J Clin Pharmacol 2008; 65: 130–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Sumukadas D, McMurdo ME, Mangoni AA, Guthrie B. Temporal trends in anticholinergic medication prescription in older people: repeated cross‐sectional analysis of population prescribing data. Age Ageing 2014; 43: 515–521. [DOI] [PubMed] [Google Scholar]
- 55. Cullinan S, O'Mahony D, O'Sullivan D, Byrne S. Use of a frailty index to identify potentially inappropriate prescribing and adverse drug reaction risks in older patients. Age Ageing 2016; 45: 115–120. [DOI] [PubMed] [Google Scholar]
- 56. Meid AD, Quinzler R, Freigofas J, Saum KU, Schottker B, Holleczek B, et al Medication underuse in aging outpatients with cardiovascular disease: prevalence, determinants, and outcomes in a prospective cohort study. PLoS One 2015; 10: e0136339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57. Warwick J, Falaschetti E, Rockwood K, Mitnitski A, Thijs L, Beckett N, et al No evidence that frailty modifies the positive impact of antihypertensive treatment in very elderly people: an investigation of the impact of frailty upon treatment effect in the HYpertension in the Very Elderly Trial (HYVET) study, a double‐blind, placebo‐controlled study of antihypertensives in people with hypertension aged 80 and over. BMC Med 2015; 13: 78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Williamson JD, Supiano MA, Applegate WB, Berlowitz DR, Campbell RC, Chertow GM, et al Intensive vs standard blood pressure control and cardiovascular disease outcomes in adults aged >/=75 years: a randomized clinical trial. JAMA 2016; 315: 2673–2682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Hilmer S, Gnjidic D. Prescribing for frail older people. Aust Prescr 2017; 40: 174–178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Hubbard R, O'Mahony M, Woodhouse K. Medication prescribing in frail older people. Eur J Clin Pharmacol 2013; 69: 319–326. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1 PRISMA 2009 Checklist
Data S2 Search strategy
Data S3 Modified Newcastle‐Ottawa Scale for cross‐sectional studies