

Abstract
The curved and dilacerated roots in the posterior teeth often present the major challenge to the clinicians during the endodontic treatments. The efficient biomechanical preparation is also affected by improper instrumentation in the curved or the constricted canals. The use of conventional instruments and techniques in the dilacerated roots may develop ledges, fractured instruments, and canal blockages which further complicate the endodontic treatments. The introduction of ProTaper Universal rotary instruments has made a significant impact in the biomechanical preparation of root canals systems. However, the fracture rate of these files and inconvenience to treat the posterior teeth in reduced mouth opening conditions limits their successful usage in endodontic treatments. The ProTaper Next rotary instruments have noted advantages such as increased flexibility, higher strength, and wear resistance over the conventional rotary endodontic systems. The current case series discusses the endodontic treatment of three severely curved root canal systems successfully treated with ProTaper Next rotary endodontic system.
Keywords: Curved root canals, endodontics, ProTaper next, root canal preparation, schneider method
Introduction
The endodontic therapy aims to treat infected dental pulp tissues in the decayed teeth and thus restoring the esthetic and functional appearance of the natural tooth.[1] The endodontic therapy involves the removal of diseased dental pulpal tissue, preparing the root canals with proper irrigation, and then sealing the prepared canals with an inert filling material.[2] The biomechanical preparation of the root canal system is considered as one of the most important stages in endodontic treatment. It includes the removal of vital and necrotic pulp tissues from the root canal system, along with removal of infected root dentine and the removal of metallic and nonmetallic obstacles in retreatment conditions.[3]
The ideal root canal preparation is one where the original canal morphology is maintained during the biomechanical preparation, along with the development of flaring from coronal to the apical portion and preserving the apical foramen.[1,2] However, the ideal root canal preparation may not be always possible due to the complexity of the root canal anatomy.[1] The biomechanical preparation of the various canal curvatures in the root canals presents a great challenge for the clinicians in regular endodontic treatment procedures. These curved canals may also limit the ideal mechanical preparation of the root canals and in turn may lead to the development of some procedural errors.[4]
To challenge the complex root canal anatomy, recent advances in the field of dentistry have led to the use of nickel-titanium (NiTi) rotary instruments in endodontic practice. The NiTi instruments have high stiffness that improves with increasing instrument sizes and aid in delivering high lateral forces in curved canals.[5] The NiTi rotary files have become popular instruments to shape root canals because of their elasticity, efficiency, and cutting capacity.[6] NiTi rotary instruments such as ProTaper (Dentsply Maillefer, Ballaigues, Switzerland) have a modified cross-sectional design that resembles a K-File configuration instead of the U-shape common to many other rotary instruments.[7] The unique feature of the ProTaper system is the progressively variable tapers of each instrument, which prepares the canal in both vertical and horizontal directions.[7] Recently, ProTaper Next rotary system is introduced with a definitive advantage over the earlier rotary systems such as safer preparation in the curved canals, duration of instrumentation, and resistance to fracture. The current case series presents three cases with curved root canals treated successfully with the ProTaper Next rotary system.
Case Reports
Case report 1
A 23-year-old female patient was referred to the Department of Dentistry, with severe pain in the lower left mandibular teeth from a local dentist. The patient gave a history of pain for 3 months that aggravates while sleeping and relieves after taking the medications. No significant medical history was observed. The intraoral examination revealed a decayed tooth in relation to #37 and a filled teeth in relation to #36. Tenderness on percussion was observed for tooth #37. The chronic irreversible pulpitis was the provisional diagnosis, and the intraoral periapical radiograph (IOPA) was advised to draw the final diagnosis and treatment plan. The IOPA revealed an ill-defined radiolucency extending into the coronal pulp, periodontal widening was observed in the apical portions of the mesial and distal roots of tooth #37. The provisional diagnosis was confirmed with the investigations, and a final diagnosis of chronic irreversible pulpitis was confirmed and the root canal treatment was advised [Figure 1a].
Figure 1.
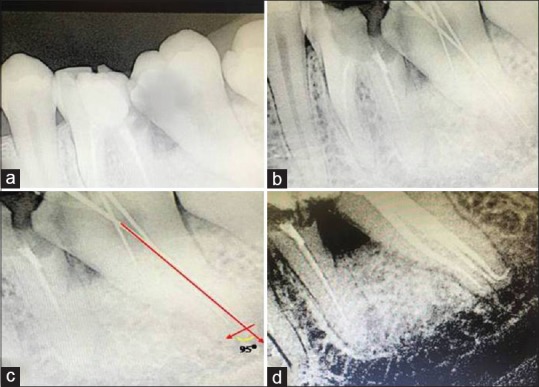
The root canal treatment pictures of case report 1. The red color arrow marks determines the Schneider angle measured by the intersection of long axis of coronal third of root to the direction of apical foramen. (a) The preoperative radiograph showing pulpally infected tooth in relation to #37. (b) The working length radiograph showing the curved distal root of tooth in relation to #37. (c) The Schneider angle determined for distal root (95°) of tooth in relation to #37. (d) The final obturation of tooth in relation to #37
After administrating inferior alveolar nerve block (2% Lignocaine 1:200000 Epinephrin), access cavity preparation was performed with size 2 round burs (KG Sorensen Zenith Dental Aps, Agerskov, Denamark). The pulp chamber was irrigated by following the standardized irrigation regimen of 5.25% of sodium hypochlorite, 17% ethylenediaminetetraacetic acid and physiological saline. The patency of the root canals was determined using No. 8 and 10 stainless steel K-files (Mani, Inc., Japan). The working length was taken with the 10 and 15 number K files [Figure 1b]. A sharp bend of around 90° was observed in the apical portion of the distal canal of tooth #37. Considering the severe dilacerated distal canal in the #37, the working length files were safely withdrawn. Gate-Glidden drills were used for enlarging the canal orifice up to size No 3. Working length was then confirmed with apex locator (Root ZX, J. Morita, Japan).
The suggested sequential method of filing for ProTaper Next was done in all the canals, where all of them were negotiated initially with the number 20 path files freely in the canal. The ProTaper Next X1 was introduced into the canals, and then with the feather touch brushing motions and preparations were completed till the apex of the canals. After copious irrigation, ProTaper Next X2 was introduced, and the preparation was completed till the root apex. Calcium hydroxide was used as an intracanal medicament and closed dressing was given for 3 days. In the next visit, the canals were flushed thoroughly with saline and dried with absorbent paper points. A master cone radiograph was taken with 6% gutta-percha points. The single cone obturation was performed using AH Plus sealer [Figure 1d]. The postendodontic restoration was done using the fiber-reinforced composite resin to maintain a good coronal seal. The postoperative instructions were given to the patient and recalled after 3 months for evaluation. At 3 months postoperative review, the patient was absolutely asymptomatic and there was no any radiographic signs of periapical disease.
Case report 2
A 10-year-old male patient referred to the Department of Dentistry with the chief complaint of severe and continuous pain in the mandibular left teeth region. The patient gave history of pain for the last 2 months and it aggrevated while sleeping and relieved only after taking the analgesics. The medical history is noncontributory. The intraoral clinical examination revealed a decayed tooth in relation to #36. The provisional diagnosis of chronic irreversible pulpitis was made based on the subjective and objective findings. The IOPA radiograph was advised in relation to #36 region. The IOPA revealed an ill-defined radiolucency extending into the pulpal region with no significant widening in the periodontal ligament [Figure 2a]. The provisional diagnosis was confirmed with the investigations, and a final diagnosis of chronic irreversible pulpitis was made for the tooth in relation to #36.
Figure 2.
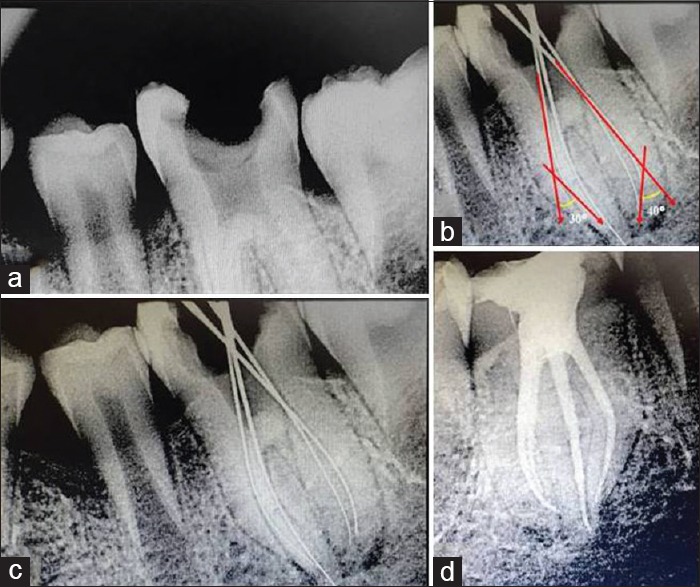
The root canal treatment pictures of case report 2. The red color arrow marks determine the Schneider angle measured by the intersection of long axis of coronal third of root to the direction of apical foramen. (a) The preoperative radiograph showing pulpally infected tooth in relation to #36. (b) The working length radiograph showing the curved mesial and distal root of tooth in relation to #36. (c) The Schneider angle determined for mesial (30°) and distal root (40°) of tooth in relation to #36. (d) The final obturation of tooth in relation to #36
The root canal treatment was indicated, and under local anesthesia (2% Lignocaine 1:200000 Epinephrin) access opening completed similar to case report 1. The tentative working length was determined with 10 and 15 number K files [Figure 2b]. The working length files have shown the curvatures in the apical portions of the mesial and distal canals. The considerations of the significant curvatures in the apical portions of mesial and distal canals the biomechanical preparation was planned with the ProTaper Next rotary system. In the next appointment, the biomechanical preparation was completed with the ProTaper Next rotary system as explained in the case report 1. The single cone obturation is completed with the 6% gutta-percha points with the AH plus sealer [Figure 2d]. The permanent restoration was done with the fiber-reinforced composite resin and the patient recalled after 3 months for evaluation.
Case report 3
A 30-year-old male patient referred to the Department of Dentistry from a local dental dentist with the chief complaint of severe and continuous pain in the mandibular right teeth region for 6 months. The patient gave a history of severe pain, and it aggrevated while taking cold and hot foods while lying down on the bed and while sleeping and the pain relieved only for few hours after taking the analgesics. No significant medical history was observed. The intraoral clinical examination revealed a decayed tooth in relation to #36. The tooth #36 was tender on percussion. The provisional diagnosis of chronic irreversible pulpitis was made based on the subjective and objective findings. An IOPA radiograph was advised in relation to #36 region. The IOPA revealed an ill-defined radiolucency extending into the pulpal region with a significant widening in the periodontal ligament at the apical region of mesial and distal canals [Figure 3a]. The provisional diagnosis was confirmed with the investigations, and a final diagnosis of chronic irreversible pulpitis was made for the tooth in relation to #36.
Figure 3.
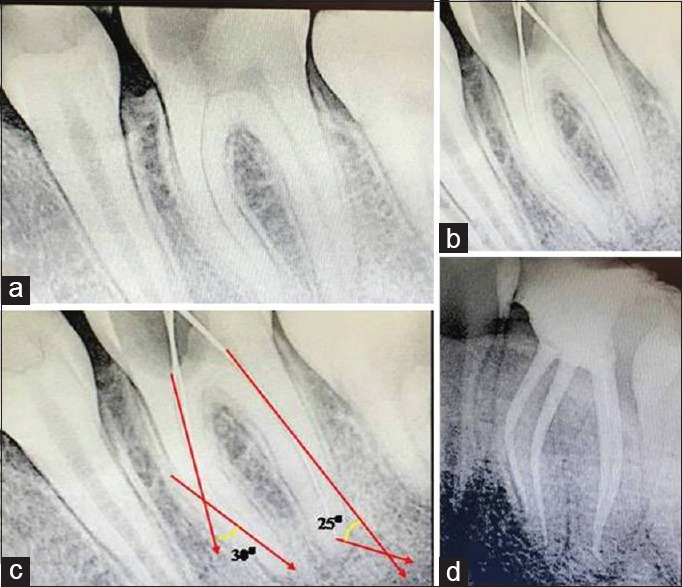
The root canal treatment pictures of case report 3. The red color arrow marks determine the Schneider angle measured by the intersection of long axis of coronal third of root to the direction of apical foramen. (a) The preoperative radiograph showing pulpally infected tooth in relation to #36. (b) The working length radiograph showing the curved mesial and distal root of tooth in relation to #36. (c) The Schneider angle determined for mesial (30°) and distal root (25°) of tooth in relation to #36. (d) The final obturation of tooth in relation to #36
The root canal treatment was planned and under local anesthesia (2% Lignocaine 1:200000 Epinephrin) access opening completed similar to case report 1. The tentative working length was determined with 10 and 15 number K files [Figure 3b]. The working length files have shown a blunt curvatures in the apical portions of the distal canal. The consideration of the significant curvatures in the apical portions of distal canals the biomechanical preparation was planned with the ProTaper Next rotary system. In the second appointment, with the copious irrigation, the biomechanical preparation was completed with the ProTaper Next rotary system as explained in the case report 1. The single-cone obturation was completed with the 6% gutta-percha points with the AH plus sealer [Figure 3d]. The permanent restoration was done with the fiber-reinforced composite resin, and the patient recalled after 3 months for evaluation.
Discussion
The tooth with straight root canals are very rare to observe in the endodontics as most of the teeth tend to exhibit some sort of curvature and multiple planes of deviations along the course of the root canal length.[3] The endodontic therapy of the pulpally infected teeth is considered successful only when a thorough cleaning and disinfection of the entire root canals system was achieved.[8] However, the root canal curvatures always made the root canal instrumentation difficult and in turn compromises the successful endodontic treatment.[9]
The broad term of root canal curvatures is specified as dilaceration by Tomes, where it implies to any kind of angulation or any sharp bend or any curve in the root or crown of the formed tooth or a deviation or bend in the linear relationship of a crown of a tooth to its root.[10] The tooth is considered to be dilacerated if the direction of the curved root is 90° or more to the long axis of the tooth and if the apical portion of the root is curved about 20° or more to the long axis of the tooth.[10] The traumatic injuries during the time of tooth development stands the main etiologic factor for the dilacerated roots.[11]
The curvatures in the root canals varies depending on the location or severity, the curvatures may be apical or gradual or S shaped.[7] The curved root canals also exhibit immense difficulty in proper disinfection of the entire root canal system.[12] Indeed, the instrumentation in the curved root canals mainly depend on the flexibility of the instruments, techniques of biomechanical preparation, location of the apical foramen, and the calcification in the root canal anatomy.[13,14] The endodontic complications such as the ledge formations, canal blockages, root canals perforations, and apical transportations are usually observed with the improper handling of the instruments or improper techniques of instrumentations.[15] Thus, evaluating the degree of root canals curvatures in the diagnostic radiograph or at the working length determination aids in the successful endodontic treatment.
Schneider in 1971 has proposed a method to determine the root canal curvatures based on the preoperative radiographs. In Schneider's method, first a line parallel to the long axis of canal in the coronal third of root canal is drawn, a second line is drawn from the apical foramina to intersect the first line. Then, Schneider's angle was determined at the intersection of these lines on a hard copy of the diagnostic radiograph.[16] Accordingly, the root canal curvatures are differentiated based on the angle of the curvatures such as straight (5° or less), moderate (10°–20°), and severe (25°–70°).[1]
The angles were determined for all the cases presented in the current case series and all the cases fall under the severe type of canal curvatures [Figure 1c, 2c, and 3c]. The severe curvatures in all the cases presented above warrant a careful biomechanical preparation to prevent the endodontic complications. The adequate biomechanical preparation in the severe type of curved canals further needs the efficient instruments and time-saving techniques of root canal preparation.
The technological advancements have led to the development of more efficient and time-saving instruments in the field of dentistry. The ProTaper Universal is a well-described NiTi rotary system of instruments manufactured with progressive taper over the length of the cutting blades, convex triangular cross-sections, and noncutting tips. However, the earlier reports by Ankrum et al. have observed that ProTaper Universal system has shown around 6% of file fracture rate in the curved canals.[6] Similarly, Wu et al., have observed a 2.6% overall incidence of ProTaper Universal rotary file separation according to the number of teeth. However, the incidence will jump to 4.9% if only molars are involved and 5.5% when only mandibular molars are analyzed.[12] Hence, the use of ProTaper Universal system in the curved roots still remains an unanswered question.
Recently, ProTaper Next (Dentsply, Tulsa Dental) has been developed with the new M Wire alloy which have an increased flexibility, higher strength, and wear resistance than similar instruments made of conventional superelastic NiTi wires. The improved properties of ProTaper Next are because of its unique nanocrystalline martensitic microstructure.[13] The ProTaper Next rotary instruments also have an innovative off centered rectangular cross-section that gives the file a snake-like swaggering movement as it progresses through the root canal. The unique asymmetric rotary motion of ProTaper Next allows to achieve fully tapered canals with fewer number of files.[14] The rotation of the off-centered cross section by ProTaper Next system generates an enlarged space for debris hauling.[15] The suggested one-time use of the ProTaper Next rotary system have the advantages such as reduced risk of file breakage, optimal cutting efficiency, and no risk for cross-contamination. The shortened design of the file head aids an efficient biomechanical preparation in the reduced mouth opening conditions when compared to the other rotary systems.[14,15]
As per directions for use, clinicians should take all instruments in both series, except ProTaper SX, passively to the working length after preparing a glide path.[14] However, although the basic sequence to shape curved root canals with ProTaper Universal system includes six instruments, three of them to prepare the coronal and middle third (SX, S1, and S2), and the other three to enlarge the apical third (F1, F2, and F3), Pro Taper Next rotary system directions for use suggest the use of only three files to shape similarly sized canals (X1 is #17/.04, X2 is #25/.06, and X3 is #30/.075). The tip diameter of X1 is close to S1, but the increment in the taper throughout the active blades is closer to the F1 ProTaper Universal instrument. The action of X1 could be the substitution of S1, S2, and F1 ProTaper Universal files. M-Wire raw material has also shown an extended fatigue life beyond the conventional NiTi alloy, which may allow getting the final desired shape with fewer instruments without increasing the risk of failure because of cyclic fatigue.[16]
The ProTaper Next rotary instrumentation technique was used for all the cases presented in the current case series. The ProTaper Next system has made an efficient cleaning of the root canals in all the cases presented above without any endodontic complications. The 3 months recall has shown no clinical or radiographic abnormality in any of the cases presented above. However, the authors further recommend the clinical trials evaluating the efficiency of ProTaper Next in the biomechanical preparation of the severely curved roots in the posterior teeth.
Conclusion
The severe root canal curvatures in the posterior teeth need to be determined to reduce the endodontic complications. The appropriate root canal instrumentation techniques need to be selected based on the root canal anatomy, calcifications, and economic factors. The Pro Taper Next rotary instrumentation has shown an efficient and time-saving biomechanical preparation in all the cases presented in the current case series and has thus, indicated for safe and efficient biomechanical preparations in curved and constricted root canal systems.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Peters OA. Current challenges and concepts in the preparation of root canal systems: A review. J Endod. 2004;30:559–67. doi: 10.1097/01.don.0000129039.59003.9d. [DOI] [PubMed] [Google Scholar]
- 2.Estrela C, Bueno MR, Sousa-Neto MD, Pécora JD. Method for determination of root curvature radius using cone-beam computed tomography images. Braz Dent J. 2008;19:114–8. doi: 10.1590/s0103-64402008000200005. [DOI] [PubMed] [Google Scholar]
- 3.Ruddle C. Cleaning and shaping the root canal system. In: Cohen S, Burns R, editors. Pathways of the Pulp. 8th ed. St. Louis, MO: Mosby; 2002. pp. 231–92. [Google Scholar]
- 4.Mounce R. Negotiating challenging mid root curvatures: Rounding the bend. Dent Today. 2007;26:108. 110, 112. [PubMed] [Google Scholar]
- 5.Bergmans L, Van Cleynenbreugel J, Wevers M, Lambrechts P. Mechanical root canal preparation with NiTi rotary instruments: Rationale, performance and safety. Status report for the American journal of dentistry. Am J Dent. 2001;14:324–33. [PubMed] [Google Scholar]
- 6.Ankrum MT, Hartwell GR, Truitt JE. K3 Endo, ProTaper, and ProFile systems: Breakage and distortion in severely curved roots of molars. J Endod. 2004;30:234–7. doi: 10.1097/00004770-200404000-00013. [DOI] [PubMed] [Google Scholar]
- 7.Ruddle CJ. The ProTaper endodontic system: Geometries, features, and guidelines for use. Dent Today. 2001;20:60–7. [PubMed] [Google Scholar]
- 8.Ingle JI. PDQ Endodontics. Hamilton, Ontario: B.C. Decker; 2005. Root canal preparation; p. 129. [Google Scholar]
- 9.Jain N, Tushar S. Curved canals: Ancestral files revisited. Indian J Dent Res. 2008;19:267–71. doi: 10.4103/0970-9290.42964. [DOI] [PubMed] [Google Scholar]
- 10.Jafarzadeh H, Abbott PV. Dilaceration: Review of an endodontic challenge. J Endod. 2007;33:1025–30. doi: 10.1016/j.joen.2007.04.013. [DOI] [PubMed] [Google Scholar]
- 11.Walia PS, Rohilla AK, Choudhary S, Kaur R. Review of dilaceration of maxillary central incisor: A mutidisciplinary challenge. Int J Clin Pediatr Dent. 2016;9:90–8. doi: 10.5005/jp-journals-10005-1341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wu J, Lei G, Yan M, Yu Y, Yu J, Zhang G, et al. Instrument separation analysis of multi-used ProTaper universal rotary system during root canal therapy. J Endod. 2011;37:758–63. doi: 10.1016/j.joen.2011.02.021. [DOI] [PubMed] [Google Scholar]
- 13.Ye J, Gao Y. Metallurgical characterization of M-wire nickel-titanium shape memory alloy used for endodontic rotary instruments during low-cycle fatigue. J Endod. 2012;38:105–7. doi: 10.1016/j.joen.2011.09.028. [DOI] [PubMed] [Google Scholar]
- 14.Tulsa Dental Specialties. Protaper Universal. Directions for use. [Last accessed on 2017 Jan 12]. Available from: http://www.tulsadentalspecialties.com/Libraries/Tab_Content_-_Endo_Access_Shaping/DFUPTNF_Rev1_10-12_ProTaperNext_DFU.sflb.ashx .
- 15.Tulsa Dental Specialties. Protaper Next. Directions for Use. [Last accessed on 2017 Jan 12]. Available from: http://www.tulsadentalspecialties.com/Libraries/Tab_Content__Endo_Access_Shaping/DFUPTNF_Rev1_10_12_ProTaperNext_DFU.sflb.ashx .
- 16.Johnson E, Lloyd A, Kuttler S, Namerow K. Comparison between a novel nickel-titanium alloy and 508 nitinol on the cyclic fatigue life of ProFile 25/.04 rotary instruments. J Endod. 2008;34:1406–9. doi: 10.1016/j.joen.2008.07.029. [DOI] [PubMed] [Google Scholar]