

Abstract
Background:
High-power level lasers used in health sciences have important photothermal effect. The maximum absorption of the diode laser correlates with the absorption range of hemoglobin, suggesting that red color may be the required chromophore. Hence, we hypothesized that by providing artificial external red chromophore, we can improve the cutting efficiency of diode laser in noninflamed tissue. The aim of the present study was to assess the efficacy and collateral thermal damage produced by a 940 nm diode laser on stained and unstained porcine tissue sample.
Materials and Methods:
Eight porcine meat samples of specific dimensions were divided into four groups of two pieces each. Group I was stained with beetroot extract, Group II stained with 3% erythrosine dye, Group III stained with hibiscus extract, and Group IV left unstained. A 940 nm diode laser was used at 1.2 W in an intermittent wave mode, to make a standardized dimension incision in all the samples. One sample from each group was stored in 10% formalin and sent for histopathological examination to evaluate the depth and width of incision and amount of lateral thermal damage. The other sample from each group was observed under video profilometer to evaluate the surface characteristics.
Results:
Staining of tissues with external chromophore using 3% erythrosine dye improved the efficacy of 940 nm diode laser, as evidenced from the sharper, wider cuts and clean incision with minimal charring as compared to beetroot, hibiscus, and saline.
Conclusion:
The use of staining can be an adjunct to the lasers in improvement of efficacy.
Keywords: Dye, efficiency, lasers, staining
Introduction
The scalpel and the conventional electrosurgery unit are the instruments of choice for soft-tissue surgery. In addition, lasers are an alternative to conventional surgical systems. Scalpels have been used for many years because of their ease of use, accuracy, and minimal damage to the surrounding tissue. On the other hand, scalpels cannot provide the hemostasis that is helpful for use on highly vascular tissue.[1]
Clinical experience suggests that advantages for using laser over scalpel surgical procedures include greater precision, a relatively bloodless surgical and postsurgical course, sterilization of the surgical area, minimal swelling and scarring, coagulation, vaporization, and cutting, minimal or no suturing, and much less or no postsurgical pain.[2,3,4,5,6]
Various laser types (Nd: YAG, Er, Cr: YSGG, Er: YAG, CO2) that correspond to wavelengths (1064, 2780, 2940, and 10600 nm) became available to the dentists to address their needs for hard- and soft-tissue procedures. Diode lasers can be used for a multitude of oral procedures which are predominantly soft-tissue procedures and include soft-tissue surgery, periodontal pocket therapy, and peri-implantitis but can also be used for root canal disinfection and laser-assisted tooth whitening.
Laser light is monochromatic, bright, unidirectional, and coherent. Diode lasers are widely used with dental practitioners. Although diode lasers include wavelength from 800 to 1064 nm, the 940 devices predominate. Wavelength has a dual impact attributable to its absorption coefficient in different chromophores as well as the depth of penetration from the skin surface, which roughly increases as the wavelength increases in the visible and near infrared spectrum. After carefully choosing a proper wavelength for a particular chromophore, the laser surgeon has a difficult task of delivering maximum number of photons to the target chromophore before they are snatched by competing chromophores which are present before the target. Laser beam that encounters skin surface may be reflected, transmitted, scattered, or absorbed at each layer. Once the laser beam falls on the tissue, from this point onward, we should think about it not as a light but as a continuous or pulsed source of photons.[7] Photon as a particle can only interact with matter by transferring the amount of energy. Therefore, only absorbed photons can produce tissue effect.
For photon absorption in a tissue, a chromophore is required.[8] The maximum absorption of the diode laser correlates with the absorption range of hemoglobin, suggesting that red color may be the required chromophore.[5] Chromophore being a material present either endogenous in the tissues or exogenous which absorbs a particular wavelength depending on its absorption coefficient.[9,10] In inflamed tissues, the role of endogenous chromophores is played by red/reddish/bright red/fiery red color of tissue, but noninflammatory tissue lacks the benefits of these natural chromophores, and hence, we hypothesized that we can increase the photon absorption by reducing its reflectance, scattering, and transmission by providing artificial chromophores. Criteria for artificial chromophore were that it should be safe, biocompatible, provide deep red color, and palatable to the patient. Hence, we shortlisted three agents (1) extract of hibiscus flower, (2) beetroot juice, and (3) erythrosine dye 3% (commonly used as plaque disclosing agent).
Thus, the aim of the current study was to assess the efficacy and influence of tissue staining by external chromophores on cutting efficacy of 940 nm diode laser.
Materials and Methods
Eight porcine meat samples of dimensions approximately 2” ×1.5” ×0.5” were divided into four groups of two pieces each. Group I was stained with beetroot extract, Group II stained with erythrosine dye, Group III stained with hibiscus extract, and Group IV left unstained (saline).
The 940 nm diode laser was used at 1.2 watts in interrupted wave mode. A continuous incision of 1-inch distance was performed in 25 s using initiated tip for each sample [Figure 1]. For stained sample, a cotton ball was used to apply respective stains on the tissue surface along the line of incision planned and then the incision was taken. For unstained sample, saline was applied using the same technique which acted as control. One sample in each group was used for video profilometer to check surface characteristics under video profilometer, and the other sample was transferred to 10% formalin and sent for histopathological examination to evaluate extent of lateral thermal damage.
Figure 1.
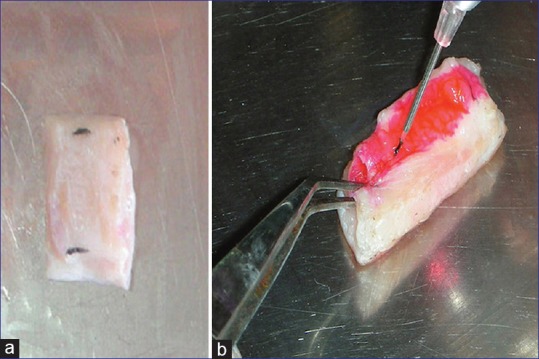
(a) Marking to standardize the length of the incision (b) Shows incision by diode laser into externally stained tissue
Profilometer (Novacam Technologies Inc. Quebec, Canada) systems are used as scanners for three dimensional metrology, roughness, measurements, and cross-sectional imaging in high prevention industries. This system was used to analyze the charring of the tissue and the continuity of the incision. The optical profilometer scan speed is dictated by the light reflected from the surface and the speed of the acquisition electronics [Figure 2].
Figure 2.
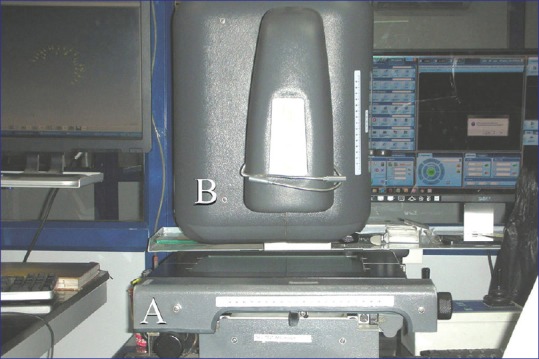
(A) Base on which meat samples are kept (B) Sensor enabling scanning of surface of meat sample used in noncontact mode
For histopathological analysis, the tissue samples are first sliced and sectioned into thin cross sections with a microtome. The tissue was fixed to prevent degradation using 4% formaldehyde in phosphate-buffered saline. The samples were later transferred through baths of progressively more concentrated ethanol to remove the water. This is followed by a hydrophobic clearing agent, xylene for removing alcohol. Finally, paraffin wax was used as an infiltrating agent and epoxy resins as an embedding media.
Results
Incision width
With the use of video profilometer, incision width at two most prominent points across the incision line was recorded as point A and point B for all stained and unstained tissue samples. Results showed maximum incision width with the 3% erythrosine stain, followed by beetroot and hibiscus stains, and least with the unstained (saline) tissue samples. Erythrosine stain showed a significant difference (<0.0001) in the tissue width as opposed to the unstained tissue [Table 1].
Table 1.
Incision width at two prominent points A and B along the incision line, as measured by video profilometer

Continuity of line
The incision line is consistent in case of the erythrosine-stained tissue samples with no breakpoints as opposed to unstained tissue samples that was a discontinuous line. The incision line for beetroot- and hibiscus-stained tissue samples had 1 and 2 breakpoints, respectively [Figure 3].
Figure 3.
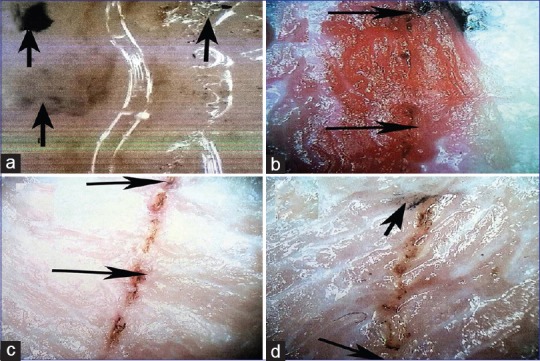
(a) Saline, (b) erythrosine, (c) beetroot, and (d) hibiscus. The area marked with the arrow show charring of the tissue
Charring of tissue
The charring of tissue is limited along the incision for erythrosine, beetroot, and hibiscus unlike the unstained tissue sample. Charring of adjacent tissue was noted with the unstained tissue sample [Figure 3].
Histopathological examination
The incision walls in case of erythrosine were sharper and better delineated as compared to beetroot and hibiscus whereas control group samples had ragged borders [Figure 4].
Figure 4.
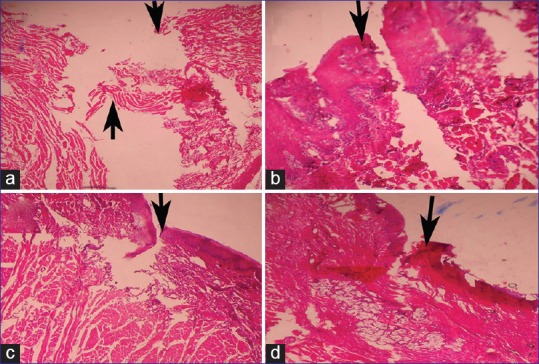
(a) Saline, (b) erythrosine, (c) beetroot, and (d) hibiscus. With arrows showing incision line
Discussion
Porcine meat samples were used to carry out this study because of its known similarity with the human beings. Domestic pigs (Sus scrofa domesticus) are closely related to humans in terms of anatomy, genetics, and physiology and represent an excellent animal model for various scientific studies.[11] Meat samples from this animal are easily accessible from the butcher shop, and hence, we do not need to sacrifice any just for the sake of study purpose.
Chromophore is a material, present either endogenous in the tissues or exogenous, i.e. brought from outside, which absorbs particular wavelengths depending on its absorption coefficient. Examples of endogenous chromophores are melanin, hemoglobin, (oxyhemoglobin, deoxyhemoglobin, and methemoglobin), water, protein, peptide bonds, aromatic amino acids, nucleic acid, urocanic acid, and bilirubin. Exogenous compounds such as different colors of tattoo ink also act as chromophores. When concentration C (g/l) of a chromophore in a given material is known, the corresponding partial absorption coefficient can be calculated from the molar extinction coefficient: (AC = 2.303). E = C/M, where E is extinction coefficient, C is concentration [g/l], M is the molecular weight [g/mole] of the chromophore.[8,12] Since noninflamed or thick fibrous tissue lacks the benefits of natural/internal chromophores, we hypothesized that the absorption of photons can be increased by providing external chromophores to the site of action.
External chromophores/dyes used in the present study were 3% erythrosine dye, beetroot, and hibiscus extracts. Among all these biocompatible materials, erythrosine dye, also known as Red No. 3, is present in Plaksee® in concentration of 3% which is a commercially available product used routinely in dentistry as a measure of plaque disclosure. Beetroot and hibiscus stains were obtained by grating beetroot and hibiscus and squeezing out the extract. In addition to providing a source of external chromophores, all these liquids also moisten the area of incision. To prevent bias, control sample was incised with similar quantity/frequency of saline as required for all other test sites.
As can be interpreted from the results of this study, the cutting efficiency of the stained tissue samples was greater (P < 0.0001) as compared to the unstained control. Furthermore, there was a significant difference in the surface characteristics including the cut surface, charring, and the continuity of the line maintained, wherein samples stained with 3% erythrosine showed the best results. Even in histopathological analysis, it was noted that the tissue samples stained with erythrosine had sharper and well-defined margins.
Based on the advantages of erythrosine dye observed in this in vitro study, it could be hypothesized that intermittent use of 3% erythrosine dye during laser surgery may produce cleaner and faster cutting which needs to be evaluated in further studies. Future studies can also incorporate different wavelength and parameters of diode lasers or different concentrations of erythrosine dye to further enhance the cutting efficiency of diode lasers. The resultant decrease in lateral thermal damage should provide for better healing outcomes. Furthermore, the faster cutting will reduce the overall surgical time, especially in cases such as drug-induced gingival enlargement and hereditary gingival fibromatosis.
Conclusion
On the basis of this study it can be stated that intermittent use of 3% erythrosine dye during laser surgery produces cleaner and faster cutting.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
I Am indebted to Mr Pravin Nikam (Test Engineer) and Deepak Shrivas (Laboratory Incharge) for allowing us to use the “Video Profilometer” available at Nasik Engineering Cluster.
References
- 1.Liboon J, Funkhouser W, Terris DJ. A comparison of mucosal incisions made by scalpel, CO2 laser, electrocautery, and constant-voltage electrocautery. Otolaryngol Head Neck Surg. 1997;116:379–85. doi: 10.1016/S0194-59989770277-8. [DOI] [PubMed] [Google Scholar]
- 2.Walsh LJ. The current status of laser applications in dentistry. Aust Dent J. 2003;48:146–55. doi: 10.1111/j.1834-7819.2003.tb00025.x. [DOI] [PubMed] [Google Scholar]
- 3.Rechman P, Hennig T. Lasers in periodontology. New trends. J Oral Laser Appl. 2002;2:7–14. [Google Scholar]
- 4.Pick RM, Colvard MD. Current status of lasers in soft tissue dental surgery. J Periodontol. 1993;64:589–602. doi: 10.1902/jop.1993.64.7.589. [DOI] [PubMed] [Google Scholar]
- 5.Gold SI, Vilardi MA. Pulsed laser beam effects on gingiva. J Clin Periodontol. 1994;21:391–6. doi: 10.1111/j.1600-051x.1994.tb00735.x. [DOI] [PubMed] [Google Scholar]
- 6.White JM, Goodis HE, Rose CL. Use of the pulsed Nd: YAG laser for intraoral soft tissue surgery. Lasers Surg Med. 1991;11:455–61. doi: 10.1002/lsm.1900110511. [DOI] [PubMed] [Google Scholar]
- 7.Uddhav A, Patil Lakshyajit D. Dhami. Overview of lasers. Indian J Plast Surg. 2008;41(Suppl):S101–S113. [PMC free article] [PubMed] [Google Scholar]
- 8.Douven L, Lucassen GW. Retrieval of optical properties of skin from measurement and modelling the diffuse reflectance. Proc SPIE. 2000;14:312–23. [Google Scholar]
- 9.Welch AJ, Gemert MJ. Optical-Thermal Response of Laser-Irradiated Tissue. New York: Plenum Press; 1995. [Google Scholar]
- 10.Yaroslavsky AN, Priezzhev AV, Rodriguez J, Yaroslavsky IV, Battarbee H. Handbook of Optical Biomedical Diagnostics. 2nd ed. Bellingham, WA: SPIE Press; 2002. Optics of blood; pp. 169–218. [Google Scholar]
- 11.Meurens F, Summerfield A, Nauwynck H, Saif L, Gerdts V. The pig: A model for human infectious diseases. Trends Microbiol. 2012;20:50–7. doi: 10.1016/j.tim.2011.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Dover, Jeffrey S, Kenneth A. Arndt. Illustrated cutaneous laser surgery: A practitioner's guide. Appleton and Lange; 1990. [Google Scholar]