

Abstract
Introduction:
The updated American Geriatrics Society (AGS) 2015 Beers Criteria include the following antidepressant classes as potentially inappropriate medications to be used with caution in older adults: selective serotonin reuptake inhibitors, serotonin norepinephrine reuptake inhibitors, tricyclic antidepressants, and mirtazapine.
Methods:
A search of the medical literature using PubMed and references included in the AGS 2015 Beers Criteria.
Results:
The treatment of depression in the older adult can additionally be complicated by comorbid conditions, as 80% of older adults have at least 1 comorbid condition and 50% have at least 2. These considerations limit the pharmacologic treatment options for depression in older adults. However, the treatment of major depression should not be overlooked, as it is quite common, with estimates of up to 5% of older adults in the community and up to 13.5% in older adults who receive home health care.
Discussion:
This article reviews treatment considerations of depression in the older adult, including both available screening tools and a discussion balancing the need for treatment of depression in this population with the concerns addressed in the 2015 Beers Criteria.
Keywords: depression, geriatric, Beers Criteria
Background
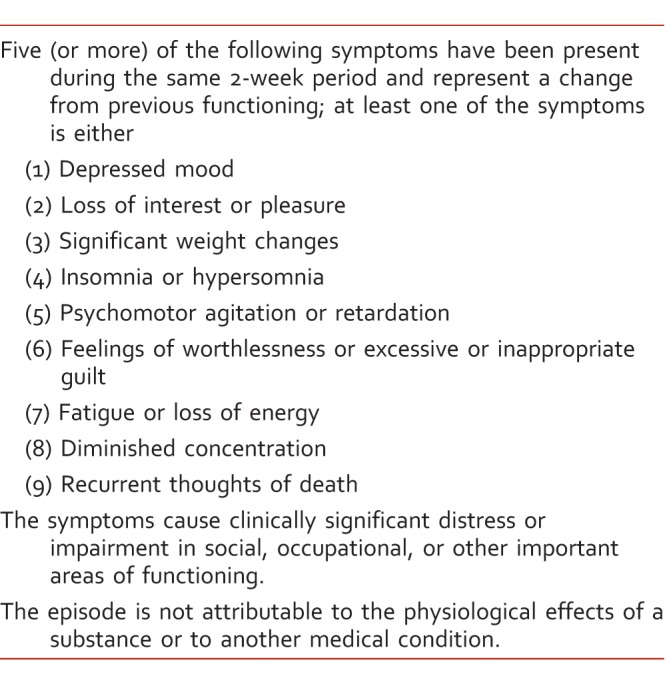
The Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM-5) provides the diagnostic criteria (Table 1) for major depressive disorder (MDD).1 Risk factors for depression include female gender, comorbid psychiatric disorders, family history of MDD, chronic medical diseases, unemployment, and lower socioeconomic status.2,3 The 12-month prevalence of MDD in older adults is lower compared with the general population, approximately 1% to 5% versus 7%, respectively.2 When providing care to the older adult, it is important to remember that depression occurs across the life-span, and it is not a normal part of aging.4 Another consideration when treating the older adult is that this age group is more likely to carry out lethal suicidal behavior.2 It should be a high priority to identify and treat the older adult with MDD, as adequate treatment of depression may help reduce future functional decline.3
TABLE 1: .
Diagnostic and Statistical Manual of Mental Disorders Fifth Edition1 major depressive disorder criteria
Major Depression in the Older Adult
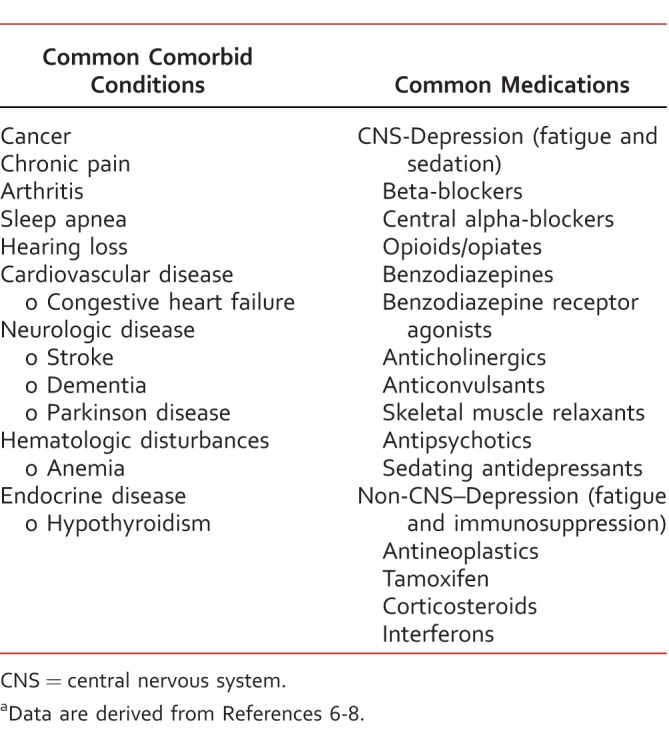
The evaluation and diagnosis of MDD in the older adult can be complicated by comorbid conditions or medications predisposing the patient toward development of depression, contributing to depression, or masking the symptoms of depression.5 These comorbid conditions and medications should be screened for initially, as treatment or optimization of these could improve outcomes without contributing to polypharmacy (Table 2).6-8 Treatment of underlying conditions can ensure the best possible response to the treatment of MDD with an antidepressant.
TABLE 2: .
Non-depression causes of depression symptomsa
Symptoms of depression such as weight loss, appetite change, psychomotor retardation, loss of energy, fatigue, sleep changes, and decreased concentration may be difficult to identify in the older adult owing to comorbid conditions or decreased activity level. The older adult with MDD may have more somatic complaints such as pain or fatigue compared with a younger adult.2-3 These differences in presentation can lead to misdiagnosis or underdiagnosis of MDD in the older adult.9
The general pharmacotherapeutic approach for older adults with MDD is to start low (50% of the adult starting dose) and go slow, titrating slowly to an effective dose.3,10 The goals of treatment for the older adult with depression are the same as for the general population: (1) achieve remission; (2) reduce relapse and recurrence; and (3) improve quality of life and functioning.3,5,6,11 Treatment of depression is usually divided into 3 treatment phases referred to as acute, continuation, and maintenance. The acute treatment phase occurs during the first 6 to 12 weeks of treatment with the goal of remission.11 The continuation phase follows the achievement of remission with the goal of preventing relapse typically lasts 4 to 12 months.5,11 If a patient requires further treatment after the continuation phase, they progress to the maintenance phase, with the goal of avoiding recurrence of depression.11 An older adult with a first episode of depression after the age of 60 may be a candidate for maintenance treatment.11 Other patients that may benefit from maintenance treatment include patients with 3 or more previous episodes of MDD, those with 2 episodes of MDD with rapid recurrence of episodes, and patients with severe episodes of MDD.11
When considering pharmacologic treatment duration in the older adult, a major consideration is the issue of polypharmacy, as 80% of older adults have at least 1 comorbid condition and 50% have at least 2.3 After the older adult has been treated for the appropriate duration, treatment discontinuation should be considered to minimize drug-drug interactions, adverse drug events, and contributions to polypharmacy and the prescribing cascade. Screening tools can be utilized to monitor treatment response and continued remission, aiding with determination of appropriate antidepressant dosage and duration of therapy.
Screening the Older Adult for Depression
The Geriatric Depression Scale (GDS) and the Patient Health Questionnaire (PHQ-9) are 2 of the most commonly used screening tools to measure depressive symptoms in the older adult population (Table 3).12-14 The GDS was created specifically for community-dwelling older adult populations and has been used for older adults hospitalized for MDD. In contrast, the PHQ-9 was created for the general population, aged 13 and older.13,14 In comparison with the PHQ-9, the GDS may have added benefit for the older population owing to ease of use. The GDS utilizes a “yes” or “no” rating scale and requires the patient to recall symptoms from the past week. In contrast, the PHQ-9 uses a more complex 4-point scale and requires a 2-week recall period, which may be difficult for a patient with cognitive impairment.13 The content of the GDS has been modified to more closely capture symptoms of depression common in older adults, such as sadness, apathy, crying, and thoughts of hopelessness, helplessness, guilt, and worthlessness.13 The PHQ-9 and other depression scales created for the general population may overemphasize vegetative symptoms reflective of the activity level of many older adults.15
TABLE 3: .
Comparison of Geriatric Depression Scale and Patient Health Questionnaire-9a

The American Geriatrics Society (AGS) recommends screening for MDD in the elderly with the PHQ-2, a 2-item questionnaire utilizing the first 2 questions from the PHQ-9; an answer of yes to either question indicates a positive test. If an older adult has a positive PHQ-2, the AGS recommends a follow-up test using either the PHQ-9, found to possess 88% sensitivity and 92% specificity in elderly primary-care patients, or the 15-item GDS, found to have 92% sensitivity and 81% specificity in elderly primary-care patients.16-18 A diagnosis of depression should be confirmed by the DSM-5 criteria.12 Both the PHQ-9 and GDS can be used during therapy to monitor for continued treatment response.
Antidepressants Listed in the AGS 2015 Beers Criteria
The Beers Criteria highlight potentially inappropriate medications (PIMs) that are best avoided in the general older adult population and in those older adults with certain diseases or syndromes. If PIMs cannot be avoided, the older adult would likely benefit from prescribing with caution by using reduced doses with careful monitoring. For specific patients, a PIM mentioned in the Beers Criteria may be the best treatment option. As all antidepressants are represented within at least one Beers Criteria section, it is important to understand why these agents are considered PIMs and how to use them in the safest manner possible.
The AGS 2015 Beers Criteria Update Expert Panel released an update in October. Table 4 summarizes the concerns and recommendations from the Panel regarding the use of antidepressants in the general older adult population, and Table 5 summarizes these concerns and recommendations for older adult patients with specific disease states or syndromes.19,20 Although this update was not as extensive as the previous 2012 update, the AGS 2015 Beers Criteria included 2 new lists. The first is a list of chronic medications to avoid or dose-reduce based on renal function that could be overlooked. This list includes the serotonin norepinephrine reuptake inhibitor duloxetine, recommending avoidance if creatinine clearance is <30 mL/min because of the potential for increased gastrointestinal adverse effects, such as nausea and diarrhea.
TABLE 4: .
Potentially inappropriate antidepressants for older adults listed in the American Geriatrics Society 2015 Beers Criteriaa

TABLE 5: .
Potentially inappropriate antidepressants for older adults with specific disease states or syndromes as listed in the American Geriatrics Society 2015 Beers Criteriaa

The second new list is a selection of non–anti-infective drug-drug interactions to be avoided in the older adult owing to a high association with negative outcomes. This list includes antidepressants, antipsychotics, benzodiazepines, and benzodiazepine receptor agonists when used in combination with 2 or more other central nervous system active drugs, because of the increased risk of falls and fractures.19 The remainder of this article discusses methods for increasing the safety of older adults treated with antidepressants.
Monitoring Antidepressant Therapy for Older Adults
Considering the commonality of depression and the need for treatment with antidepressants on the Beers Criteria, it is likely that an older adult patient will be prescribed a PIM that is the best pharmacotherapeutic option.19 It is important to note that the monitoring of antidepressant therapy is more extensive for older adults than younger adults. Compared with younger adults, older adults on antidepressant therapy have an increased risk of adverse effects such as falls, hyponatremia, and gastrointestinal upset resulting from comorbid conditions and pharmacokinetic and pharmacodynamic changes. The risk for drug-drug interactions is also increased owing to an increased occurrence of polypharmacy.9
The older adult may be at an increased risk of adverse effects due to pharmacokinetic or pharmacodynamic changes. In the older adult, elimination of the drug may be decreased due to changes in hepatic metabolism and renal elimination, resulting in accumulation of the drug and increasing the potential for adverse effects. The impact of these elimination changes should be carefully considered when determining dose initiation, dose titration interval, and maximum dose. These decisions should be based on the individual patient and specific medication, with consideration of maximum recommended dosages. For example, the maximum recommended dose of citalopram for a patient over the age of 60 is 20 mg daily because of the increased risk of QTc prolongation. Older adults have increased pharmacodynamic sensitivity to centrally acting medications than younger adults, resulting in efficacy at lower doses of centrally acting medications population-wide.9 The older adult may also be more sensitive to the anticholinergic actions of medications such as tricyclic antidepressants (TCAs) and the selective serotonin reuptake inhibitor (SSRI) paroxetine, increasing the risk for confusion, dry mouth, and constipation.9,19
The older adult may be at an increased risk of falls for a variety of reasons, including poor vision, hypotension, and comorbid conditions.9 Selective serotonin reuptake inhibitors and TCAs further increase the risk of falls, particularly in patients with a history of falls or fractures and should be used cautiously in these patients. Antidepressants increase fall risk owing to sedative effects, anticholinergic properties, and orthostatic hypotension, with TCAs and paroxetine receiving the most attention in the 2015 Beers Criteria.19 It is well known that initiation of antidepressants can cause dizziness, especially in older adults, but the precise mechanism for increased fall risk associated with long-term SSRI use remains unclear. It is possible that older adults with SSRI-induced hyponatremia could be at an increased risk of falls, as mild chronic hyponatremia has been associated with falls, unsteadiness, and inattentiveness.21 Depression, anxiety, and the fear of falling have all been linked to an increased risk of falls, which is a major confounder toward analyzing the relationship between taking antidepressants and having an increased risk of falls.22 Selective serotonin reuptake inhibitors and other serotonergic antidepressants have been theorized to increase fracture risk because of a serotonergic suppression of osteoblast proliferation, and the clinical relevance of this mechanism is a current avenue for research. One study utilized Medicare data and propensity score–matched cohorts to compare fracture rates among patients taking different antidepressants. The study found that in comparison with patients on secondary amine TCAs, the fracture rate was higher among patients taking highly serotonergic antidepressants, including SSRIs or venlafaxine (hazard ration [HR], 1.30; 95% confidence interval [CI], 1.12-1.52). This was in contrast to the comparatively similar fracture rate seen with atypical antidepressants, including duloxetine, mirtazapine, nefazodone, or trazodone (HR, 1.12; 95% CI, 0.96-1.31), and tertiary amine TCAs (HR, 1.01; 95% CI, 0.87-1.18).23 When attempting to reduce the risk of falls for patients taking antidepressants, the provider should review the medication list and limit the use of other medications that can also contribute to falls.19 A number of fall-risk assessments are available online and include lists of medications besides antidepressants that contribute to falls, such as analgesics, antipsychotics, anticonvulsants, benzodiazepines, antihypertensives, cardiac drugs, antiarrhythmics, and diuretics.24
The risk of hyponatremia, syndrome of inappropriate antidiuretic hormone, or both is increased in the older adult patient on antidepressant therapy. The risk is further increased if the patient is on another medication that can cause hyponatremia, such as a diuretic.9 Routine monitoring of serum sodium is not current standard practice for antidepressant therapy. In the older adult, the provider should consider obtaining a baseline serum sodium, repeating 1 month after initiation of therapy, or anytime during therapy if a patient presents with symptoms suggestive of low sodium (fatigue, dizziness, confusion).19,25 If hyponatremia is discovered, the offending agent should be discontinued. In the case of SSRI-induced hyponatremia, the hyponatremia is usually reversible, with most cases resolving 2 weeks after discontination.26
Escitalopram, citalopram, and sertraline are often considered first-line agents for treatment of depression in the elderly. However, diarrhea is a commonly reported side effect of these medications and can lead to therapy discontinuation.10,27,28 Diarrhea is a population-wide adverse effect of these agents, likely resulting from serotonergic actions on the gastrointestinal system.27 The elderly patient could be particularly affected by this adverse effect owing to decreased mobility, increased rates of incontinence, decreased ability to compensate for dehydration, and taking additional medications that cause diarrhea.
Although not mentioned in the Beers Criteria, the older adult treated with SSRI or serotonin norepinephrine reuptake inhibitor therapy may also be at an increased risk of gastrointestinal bleeding as a result of decreased platelet aggregation, especially if taken in combination with nonsteroidal anti-inflammatory drugs, corticosteroids, anticoagulants, or antiplatelet agents such as aspirin or clopidogrel.9,10 Similar to hyponatremia monitoring, it is not standard practice to monitor a complete blood count in patients initiating SSRI therapy. The older adult should be monitored for any signs or symptoms of bleeding throughout the duration of therapy.
Conclusion
Major depressive disorder is not a normal part of aging and can occur across the life-span. Older adults should be screened for depression with the PHQ-2; if positive, either the PHQ-9 or GDS can be used for further screening. Comorbid medical conditions, other medications, and recommendations included in the AGS 2015 Beers Criteria should be considered when making pharmacotherapy treatment decisions. Although antidepressants are included in the 2015 Beers Criteria as PIMs, an antidepressant agent may be the most effective pharmacotherapeutic option for the patient. When the benefits of therapy outweigh the risks, these agents can be used safely as long as the patient is monitored appropriately.
Footnotes
Disclosures: The authors have nothing to disclose.
References
- 1. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Arlington (VA): American Psychiatric Association; 2013. [Google Scholar]
- 2. Fiske A, Wetherell JL, Gatz M. . Depression in older adults. Annu Rev Clin Psychol. 2009; 5 1: 363- 89. DOI: 10.1146/annurev.clinpsy.032408.153621. PubMed PMID: 19327033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. O'Connor EA, Whitlock EP, Gaynes BN, Beil TL. . Screening for depression in adults and older adults in primary care: an updated systematic review . Evidence Synthesis No. 75. AHRQ Publication No. 10-05143-EF-1. Rockville (MD): Agency for Health Care Research and Quality; 2009. [PubMed]
- 4. Centers for Disease Control and Prevention. Depression is not a normal part of growing older [Internet]. Atlanta: Centers for Disease Control and Prevention [cited; 2015. Nov 6]. Available from: http://www.cdc.gov/aging/mentalhealth/depression.htm [Google Scholar]
- 5. Alexopoulos GS, Katz IR, Reynolds CF, Carpenter D, Docherty JP, Ross RW. . Pharmacotherapy of depression in older patients: a summary of the expert consensus guidelines. J Psychiatr Pract. 2001; 7 6: 361- 76. PubMed PMID: 15990550. [DOI] [PubMed] [Google Scholar]
- 6. American Psychiatric Association. Practice guidelines for the treatment of patients with major depressive disorder . 3rd ed. Arlington (VA): American Psychiatric Association; 2010. DOI: 10.1176/appi.books.9780890423387.654001.
- 7. Patten SB, Lavorato DH. . Medication use and major depressive syndrome in a community population. Compr Psychiatry. 2001; 42 2: 124- 31. DOI: 10.1053/comp.2001.21218. PubMed PMID: 11244148. [DOI] [PubMed] [Google Scholar]
- 8. Saito H, Nishiwaki Y, Michikawa T, Kikuchi Y, Mizutari K, Takebayashi T, et al. Hearing handicap predicts the development of depressive symptoms after 3 years in older community-dwelling Japanese. J Am Geriatr Soc. 2010; 58 1: 93- 7. DOI: 10.1111/j.1532-5415.2009.02615.x. PubMed PMID: 20002512. [DOI] [PubMed] [Google Scholar]
- 9. Sultana J, Spina E, Trifirò G. . Antidepressant use in the elderly: the role of pharmacodynamics and pharmacokinetics in drug safety. Expert Opin Drug Metab Toxicol. 2015; 11 6: 883- 92. DOI: 10.1517/17425255.2015.1021684. PubMed PMID: 25736834. [DOI] [PubMed] [Google Scholar]
- 10. Kovich H, DeJong A. . Common questions about the pharmacologic management of depression in adults. Am Fam Physician. 2015; 92 2: 94- 100. PubMed PMID: 26176368. [PubMed] [Google Scholar]
- 11. Trangle M, Gursky J, Haight R, Hardwig J, Hinnenkamp T, Kessler D, et al. Adult depression in primary care [Internet]. Institute for Clinical Systems Improvement. c2016 [cited 2016. March]. Available from: http://www.icsi.org/guidelines__more/catalog_guidelines_and_more/catalog_guidelines/catalog_behavioral_health_guidelines/depression/.
- 12. Gradishar WJ, Vokes EE, Kies MS. . Phase II trial of etoposide and doxorubicin in advanced head and neck cancer. Med Pediatr Oncol. 1990; 18 6: 487- 90. PubMed PMID: 2233521. [DOI] [PubMed] [Google Scholar]
- 13. Smarr KL, Keefer AL. . Measures of depression and depressive symptoms: Beck Depression Inventory-II (BDI-II), Center for Epidemiologic Studies Depression Scale (CES-D), Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and Patient Health Questionnaire. Arthritis Care Res (Hoboken). 2011; 63 Suppl 11: S454- 66. DOI: 10.1002/acr.20556. PubMed PMID: 22588766. [DOI] [PubMed] [Google Scholar]
- 14. Lakkis NA, Mahmassani DM. . Screening instruments for depression in primary care: a concise review for clinicians. Postgrad Med. 2015; 127 1: 99- 106. PubMed PMID: 25526224. [DOI] [PubMed] [Google Scholar]
- 15. Burke WJ, Nitcher RL, Roccaforte WH, Wengel SP. . A prospective evaluation of the Geriatric Depression Scale in an outpatient geriatric assessment center. J Am Geriatr Soc. 1992; 40 12: 1227- 30. PubMed PMID: 1447439. [DOI] [PubMed] [Google Scholar]
- 16. Watson LC, Pignone MP. . Screening accuracy for late-life depression in primary care: a systematic review. J Fam Pract. 2003; 52 12: 956- 64. PubMed PMID: 14653982. [PubMed] [Google Scholar]
- 17. Lyness JM, Noel TK, Cox C, King DA, Conwell Y, Caine ED. . Screening for depression in elderly primary care patients: a comparison of the Center for Epidemiologic Studies-Depression Scale and the Geriatric Depression Scale. Arch Intern Med. 1997; 157 4: 449- 54. PubMed PMID: 9046897. [PubMed] [Google Scholar]
- 18. Phelan E, Williams B, Meeker K, Bonn K, Frederick J, Logerfo J, et al. A study of the diagnostic accuracy of the PHQ-9 in primary care elderly. BMC Fam Pract. 2010; 11: 63 DOI: 10.1186/1471-2296-11-63. PubMed PMID: 20807445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. American Geriatrics Society 2015. Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015; 63 11: 2227- 46. DOI: 10.1111/jgs.13702. PubMed PMID: 26446832. [DOI] [PubMed] [Google Scholar]
- 20. Hanlon JT, Semla TP, Schmader KE. . Alternative medications for medications in the use of high-risk medications in the elderly and potentially harmful drug-disease interactions in the elderly quality measures. J Am Geriatr Soc. 2015; 63 12: e8- 18. DOI: 10.1111/jgs.13807. PubMed PMID: 26447889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Renneboog B, Musch W, Vandemergel X, Manto MU, Decaux G. . Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am J Med. 2006; 119 1: 71.e1- 8. DOI: 10.1016/j.amjmed.2005.09.026. PubMed PMID: 16431193. [DOI] [PubMed] [Google Scholar]
- 22. Iaboni A, Flint AJ. . The complex interplay of depression and falls in older adults: a clinical review. Am J Geriatr Psychiatry. 2013; 21 5: 484- 92. DOI: 10.1016/j.jagp.2013.01.008. PubMed PMID: 23570891. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Gagne JJ, Patrick AR, Mogun H, Solomon DH. . Antidepressants and fracture risk in older adults: a comparative safety analysis. Clin Pharmacol Ther. 2011; 89 6: 880- 7. DOI: 10.1038/clpt.2011.54. PubMed PMID: 21508938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Agency for Healthcare Research and Quality. Tool 3I: medication fall risk score and evaluation tools [Internet]. Rockville (MD): Agency for Healthcare Research and Quality [cited; 2016. Jan 10]. Available from: http://www.ahrq.gov/professionals/systems/hospital/fallpxtoolkit/fallpxtk-tool3i.htm [Google Scholar]
- 25. Frank C. . Pharmacologic treatment of depression in the elderly. Can Fam Physician. 2014; 60 2: 121- 6. PubMed PMID: 24522673. [PMC free article] [PubMed] [Google Scholar]
- 26. Jacob S, Spinler SA. . Hyponatremia associated with selective serotonin-reuptake inhibitors in older adults. Ann Pharmacother. 2006; 40 9: 1618- 22. DOI: 10.1345/aph.1G293. PubMed PMID: 16896026. [DOI] [PubMed] [Google Scholar]
- 27. Garfield LD, Dixon D, Nowotny P, Lotrich FE, Pollock BG, Kristjansson SD, et al. Common selective serotonin reuptake inhibitor side effects in older adults associated with genetic polymorphisms in the serotonin transporter and receptors: data from a randomized controlled trial. Am J Geriatr Psychiatry. 2014; 22 10: 971- 9. DOI: 10.1016/j.jagp.2013.07.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Cipriani A, La Ferla T, Furukawa TA, Signoretti A, Nakagawa A, Churchill R, et al. Sertraline versus other antidepressive agents for depression. Cochrane Database Syst Rev. 2010; (4):CD006117. DOI: 10.1002/14651858.CD006117.pub4. PubMed PMID: 20393946. [DOI] [PMC free article] [PubMed]