

Abstract
Objective
To test the hypotheses that (i) there is a significant correlation between the curve of Spee (COS), basal arch (WALA ridge) to dental arch distance (WALA-FA distance) and curve of Wilson (CW) and that (ii) the deepening of the COS is affected by the CW and the WALA-FA distance.
Methods
Mandibular models of 50 patients aged between 20 and 35 years were scanned with TRIOS. The xyz coordinate system was determined, and a reference occlusal plane was generated. The depth of the COS, the CW, and WALA-FA distance were measured using an engineering software.
Results
The greatest difference in the measurement of the depth of the COS between the right and left was found to be 0.41±0.50 mm in the first molar teeth. On the basis of the results of Pearson correlation analysis, there was no strong correlation between the depth of the COS, the CW, and the WALA-FA distance.
Conclusion
It was shown that there was no strong correlation between the depth of COS, CW, and WALA-FA distance. The CW and WALA-FA distance could not be effective in the deepening of the COS.
Keywords: Curve of Spee, curve of Wilson, WALA-FA distance
INTRODUCTION
Orthodontic treatment planning starts with attaining acceptable aesthetic changes in facial soft tissues. Additionally, it is important to position the teeth at the accurate position and proper angulation and inclination within the basal bone to obtain physiological static and dynamic occlusal relationships. Orthodontic tooth movements that exceed the basal border result in periodontal problems in teeth, damaging the post-treatment stability (1). It is vital to determine the dental arch form of the individual prior to treatment and to use the mechanics that comply with the form of the arch throughout the treatment for preventing periodontal problems, ensuring stability, and obtaining aesthetic results (2).
WALA (the initials of Will Andrews and Larry Andrews) is the most prominent point in the keratinized gingiva close to the mucogingival junction (3). Where the WALA points unite, they create a ridge in the keratinized gingiva. The ridge, which is also clinically observable, is important because it indicates the bone base and the physiological border within which the teeth can move (4). The facial axis point (FA point) is the most prominent point of the clinical crown. The union of the FA points determines the dental arch form (5). The relationship between the dental arch and basal arch that is described as WALA to FA, abbreviated as WALA-FA in this study, has been assessed in several malocclusions (6–8). On the frontal plane, the occlusal table passing the cusp tips of the posterior teeth does not follow the same plane. Wilson described this as a compensational curve to prevent balancing interferences (9). This curve, specified by Andrews as the fourth key of the ideal occlusion, is given form by the buccolingual inclinations of the posterior teeth (10).
The curve of Spee (COS) was first described in 1890 by F. Graf von Spee (11) as the line on a cylinder tangent to the anterior border of the condyle, the occlusal surface of the second molar, and the incisal edges of the mandibular incisors. COS is one of the factors specified in the six keys of occlusion defined by Andrews. According to Andrews, COS ranges from flat to mild in subjects with proper occlusion (10).
Several hypotheses have been proposed to explain the functional significance of these morphological curves. Among them are biomechanical considerations concerning the resistance against the forces developed during occlusion and chewing and thus about the stability of the dental arches and an increase of the crush/shear ratio during chewing in the molar region (12). COS provides posterior teeth disclusion and anterior tooth guidance with forward movement of the mandible (11), whereas the curve of Wilson (CW) prevents premature contacts in lateral movements of the mandible (9).
There is no significant relationship between COS and gender, age, and facial skeletal morphology (13, 14). However, there are some studies suggesting that the deep-bite cases are associated with the increased depth of the COS (15). On the other hand, when the intra-arch factors that may be effective in the formation of the COS were evaluated, anterior teeth extrusion was reported to be effective in Class I anomalies, and no significant difference was detected between class I, II, and III malocclusions (16). Although the morphological relationship between the COS and the CW has been the subject of several researches, the effect of CW on the deepening of the COS has not been evaluated. Although it is possible to obtain reduction in the depth of the COS with archwires used in orthodontic treatments, it may simultaneously be necessary to attain transverse expansion with increased posterior tooth torque as required by the abnormality. To date, no available study has investigated the relationship between the COS and the basal arch-dental arch distance that creates the transverse border of the dental movement.
In the past, the natural dental arch curves have been analyzed in plaster models using analogue or digital calipers or other modified tools (6,14,17–19). Because it is almost impossible to perform certain linear measurements with these methods, the fact that records cannot be kept on the model during the study is a crucial shortcoming. One cannot obtain sufficient information because a three-dimensional structure is examined after being minimized into a single section by two-dimensional techniques (20). The measurements performed on stone models in the past have been replaced by digital models recently. Numerous studies indicated that different digital modeling methods were accurate and reliable (21). The use of digital models together with different advanced software makes it possible to obtain faster, more effective, and more detailed information than from these plaster models. The COS, CW, and the relationship between WALA and FA have been measured for various purposes in different studies. However, at present, no study has investigated the relationship between those variables that may be changed by virtue of orthodontic treatments. The changes in depth of the COS during the treatment are mostly described with intra-arch anteroposterior changes. Patients may also need transverse movements as required by the treatment. Knowledge of the potential relationship between the increased depth of the COS and those parameters is important for prediction of the changes during the treatment. In light of this information, the objective of the present study was to investigate the effect of CW and dental-basal bone arch distance on the deepening of COS and to demonstrate the potential relationship between these variables using three-dimensional models and advanced engineering software programs. We hypothesize that there is a significant relationship between COS, CW, and the dental arch-basal arch distance and that CW and dental arch-basal arch distance are effective on the deepening of the COS.
METHODS
The ethical committee approval for this retrospective study was obtained from the Sağlık Bilimleri University Gülhane School of Dentistry (1648.4–763). Pretreatment mandibular plaster models of 50 patients (24 females, 26 males; mean age: 26.4 years) aged between 20 and 35 years from the archives of Ege University Department of Orthodontics were scanned and digitized using Trios (3Shape; Copenhagen Denmark). All patients signed a form before treatment, granting permission for their models to be used in scientific researches. Measurements in the digital mandibular models were performed by an advanced engineering software (Rapidform; Inus Technology Inc., Seoul, South Korea). The excessive parts under the dento-alveolar region were trimmed, and the models were made ready for the measurement. The inclusion criteria for the patients were: skeletal class I (1°<ANB<4°)relationship, no previous orthodontic treatment, no crowding or diastema greater than 3 mm, lower and upper dental midline coincidence, Angle class I canine and molar relationship; no clinically observable attrition or fracture noted in the models, and no prominent dental shape and congenital abnormality (Figure 1).
Figure 1.
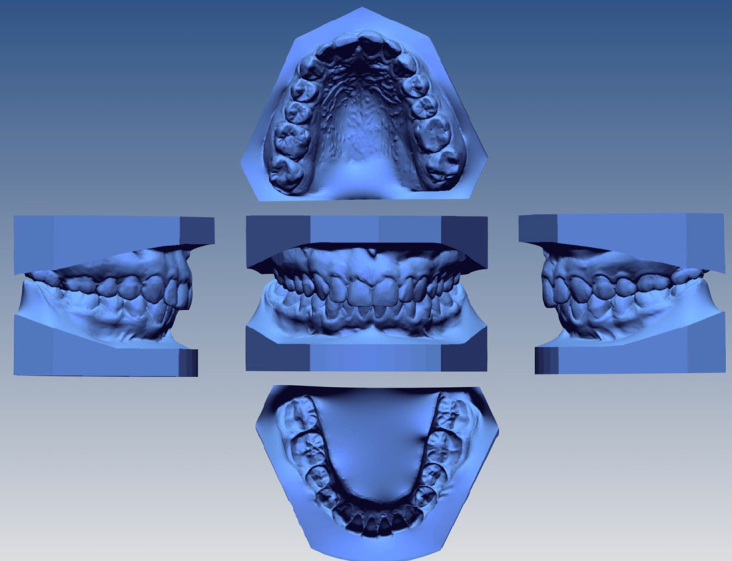
Views from different angles of the model of a patient enrolled in the study
A reference occlusal plane (ROP) was established in such a manner to pass the distobuccal cusp tips of bilateral second molars and cusp tips of the canines to measure the CW and COS in the digital models (Figure 2). In determining the depth of the COS, the perpendicular distances from the buccal cusp tips of the first premolar and second premolar teeth and mesiobuccal cusps of the first molar tooth to the ROP were measured in mm units (Figure 3). To determine the CW, lines were drawn in such a way to pass the mesiobuccal and lingual cusp tips of the first and second premolar teeth and the first molar tooth. The angles made by these lines with the ROP were measured. The angle is positive in the case of teeth inclined to the lingual surface (Figure 4).
Figure 2.
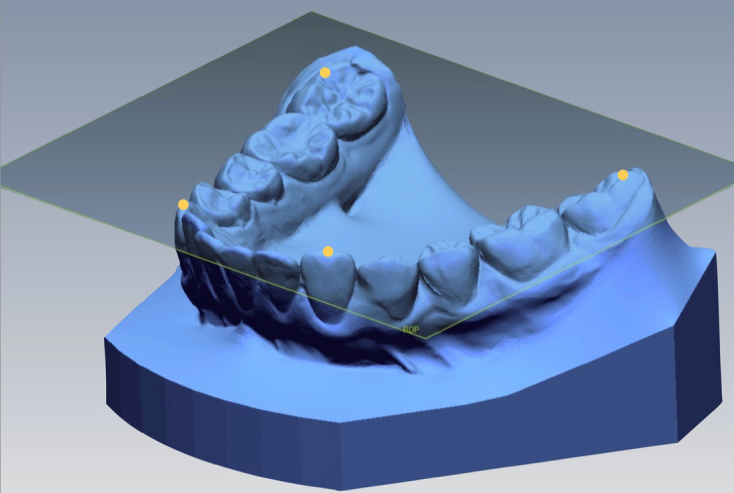
Reference occlusal plane
Figure 3.
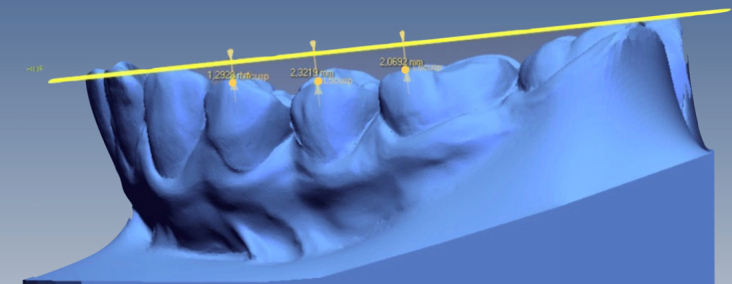
Measurement of the COS in the first, second premolar and first molar teeth
COS: curve of Spee
Figure 4.
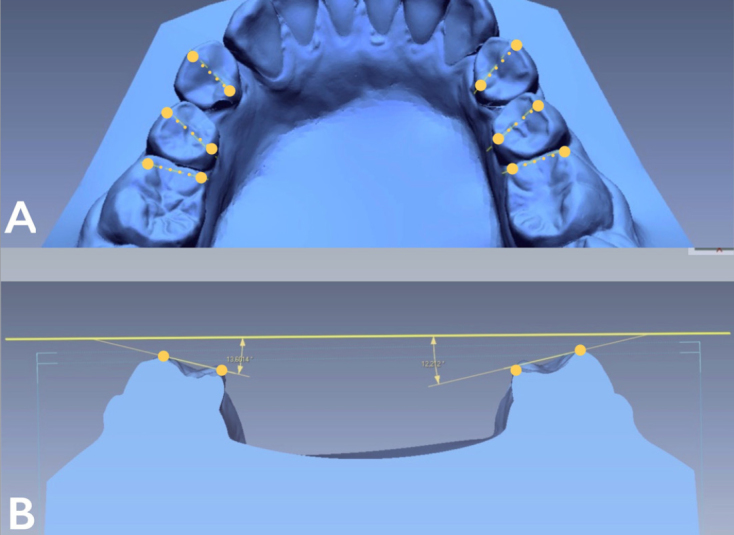
Points creating the lines determined on the occlusal surfaces of the teeth to measure the CW (a); angle made by the line determined on the occlusal surfaces of the teeth with the ROP (b)
CW: curve of Wilson; ROP: reference occlusal plane
The localization of the x (transversal), y (sagittal), and z (vertical) coordinates was determined on the digital models. The FA points of all teeth were marked by the same investigator. The WALA point was measured directly below the FA point of each tooth perpendicular to the occlusal plane at mucogingival junction. The distances in the specified x-, y-, and z-axes between these points were calculated using the software. For the transverse distance, the distance between the WALA and FA points on the x-axis in the right and left first molar, first premolar, and second premolar teeth was noted in mm units (Figure 5).
Figure 5.
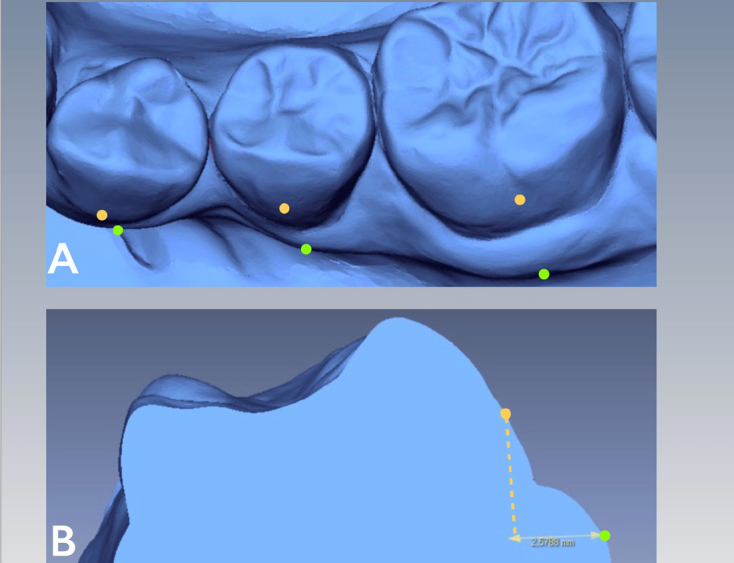
Image of the WALA (green) and FA (yellow) points on the first and second premolar teeth and the first molar tooth (a); display of the transverse distance measured between the WALA and FA points (b)
WALA: basal arch point FA: facial axis point
Statistical Analysis
The statistical analysis of the data was performed using Statistical Packages for the Social Sciences version 20 (IBM Corp.; Armonk, NY, USA). The statistical significance level was determined to be p<0.05. The normal distribution of the data was evaluated using the Shapiro-Wilk test. The paired sample t test was used for side comparisons. Pearson correlation coefficients were calculated to determine the linear associations among WALA-FA distance, CW, and depth of the COS for each tooth. To assess the contribution of these two variables to the depth of the COS, linear multiple regression analysis was carried out. The measurements were repeated 1 month later on 20 randomly selected digital models. Intra-observer repeatability was measured by the intraclass correlation coefficient (ICC).
RESULTS
The descriptive statistics and analysis results of the depth of the COS, CW, and WALA-FA distance measurements in the first premolar, second premolar, and first molar teeth are shown in Tables 1 to 3. Intra-observer reliability values observed in the measurements repeated 1 month later by the same investigator ranged between ICC 0.89 and 0.95.
Table 1.
Comparison of measurements between right and left sides of the arch
| Tooth | Side | COS | WALA-FA distance | CW | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
||||||||||||||
| Mean | SD | Mean difference (95% CI) | t | p | Mean | SD | Mean difference (95% CI) | t | p | Mean | SD | Mean difference (95% CI) | t | p | ||
| 1. Premolar | ||||||||||||||||
| Left (mm) | 1.09 | 0.78 | −0.33 (−0.086, −0.59) | −2.712 | 0.010 | 1.04 | 0.61 | 0.02 (−0.16, 0.2) | 0.207 | 0.837 | 25.22 | 7.91 | 0.57 (−1.70, 2.83) | 0.505 | 0.616 | |
| Right (mm) | 1.42 | 0.70 | 1.02 | 0.46 | 24.65 | 6.16 | ||||||||||
| 2. Premolar | ||||||||||||||||
| Left (mm) | 1.40 | 0.48 | −0.26 (−0.10, −0.42) | −3.287 | 0.002 | 1.86 | 0.63 | 0.14 (−0.04, 0.32) | 1.602 | 0.117 | 21.50 | 6.98 | −0.03 (−1.93, 1.88) | −0.031 | 0.976 | |
| Right (mm) | 1.66 | 0.59 | 1.72 | 0.52 | 21.53 | 6.58 | ||||||||||
| 1. Molar | ||||||||||||||||
| Left (mm) | 1.33 | 0.55 | −0.41 (−0.25, −0.56) | −5.341 | <0.001 | 2.72 | 0.62 | −0.01 (−0.19, 0.18) | −0.038 | 0.970 | 9.95 | 3.75 | −0.41 (−0.70, 1.87) | −0.645 | 0.523 | |
| Right (mm) | 1.74 | 0.53 | 2.73 | 0.70 | 10.36 | 4.73 | ||||||||||
SD: standard deviation; COS: curve of Spee; CW: curve of Wilson; WALA-FA distance: basal arch-dental arch distance
Table 2.
Pearson correlation values for the variables
| Tooth | Side | WALA-FA | CW | |
|---|---|---|---|---|
| 1. Premolar | Left | COS | −0.215 | −0.302 |
| WALA-FA | 1 | 0.270 | ||
| Right | COS | 0.032 | −0.050 | |
| WALA-FA | 1 | 0.173 | ||
| 2. Premolar | Left | COS | 0.177 | 0.264 |
| WALA-FA | 1 | 0.386 | ||
| Right | COS | 0.000 | 0.156 | |
| WALA-FA | 1 | 0.157 | ||
| 1. Molar | Left | COS | 0.264 | −0.218 |
| WALA-FA | 1 | 0.289 | ||
| Right | COS | −0.107 | −0.175 | |
| WALA-FA | 1 | 0.064 |
CW: curve of Wilson; WALA-FA distance: basal arch-dental arch distance; COS: curve of Spee
Table 3.
Results of linear multiple regression analysis to determine the contribution of CW and WALA-FA distance to the depth of the COS
| Tooth | Side | Variables | B | Std E | β | t | r2 | p |
|---|---|---|---|---|---|---|---|---|
| 1. Premolar | ||||||||
| Left | WALA-FA | 0.151 | 0.212 | 0.120 | 0.715 | 0.277 | 0.479 | |
| CW | −0.058 | 0.016 | −0.185 | −1.03 | 0.277 | 0.205 | ||
| Right | WALA-FA | 0.063 | 0.248 | 0.041 | 0.255 | 0.004 | 0.800 | |
| CW | −0.006 | 0.018 | −0.057 | −0.351 | 0.004 | 0.728 | ||
| 2. Premolar | ||||||||
| Left | WALA-FA | 0.029 | 0.143 | 0.038 | 0.203 | 0.071 | 0.840 | |
| CW | 0.017 | 0.013 | 0.243 | 1.290 | 0.071 | 0.205 | ||
| Right | WALA-FA | −0.028 | 0.181 | −0.25 | −0.154 | 0.025 | 0.879 | |
| CW | 0.014 | 0.014 | 0.159 | 0.996 | 0.004 | 0.325 | ||
| 1. Molar | ||||||||
| Left | WALA-FA | 0.317 | 0.136 | 0.357 | 1.334 | 0.164 | 0.095 | |
| CW | −0.047 | 0.023 | −0.321 | −1.102 | 0.164 | 0.102 | ||
| Right | WALA-FA | −0.074 | 0.121 | −0.097 | −0.614 | 0.040 | 0.543 | |
| CW | −0.019 | 0.018 | −0.168 | −1.071 | 0.040 | 0.291 | ||
B: unstandardized regression coefficient; β: standardized regression coefficient; r2: coefficient of determination; Std E: standard error; CW: curve of Wilson; WALA-FA distance: basal arch-dental arch distance
In the WALA-FA distance and CW measurements, no statistically significant difference was found between the right and left first premolar, second premolar, and first molar teeth, whereas the depth of the COS created a significant difference in the right and left teeth (p=0.010, p=0.002, and p<0.001, respectively). The greatest difference in the measurement of the depth of the COS between the right and left was found to be 0.41±0.50 mm in the first molar teeth (Table 1).
The Pearson correlation coefficient was calculated separately for the right and left segments in the evaluation of the relationship between the WALA-FA distance, depth of the COS, and the CW. There was no strong correlation between the depth of the COS, the CW, and the WALA-FA distance (Table 2). On the basis of the results of the multiple linear regression analysis performed to investigate the effect of the WALA-FA distance and CW on the deepening of the COS, it was found that the deepening of the COS was not affected by the WALA-FA distance or the CW (Table 3).
DISCUSSION
The present study examined the correlation between the depth of the COS, the CW, and WALA-FA distance and the effect of the buccolingual inclination (CW) of the teeth and the WALA-FA distance on the deepening of the COS. It is important to specify the pretreatment characteristics of these three variables with respect to predicting potential changes resulting from the orthodontic mechanics applied during the treatment and to provide information about the effect of these changes on the orthodontic treatment success and failure. It has been demonstrated that there is no significant correlation between the depth of COS-CW and WALA-FA distance and that neither the CW nor the WALA-FA distance has a clinically meaningful effect on the deepening of the COS.
Farella et al. (13) reported that the craniofacial morphology had a small effect on the depth of COS. Given the limited number of studies with a high level of evidence in this respect, individuals with craniofacial abnormalities, including facial asymmetry, syndrome, and other issues, were not included in the study to prevent any potential interaction. Gender was reported to be ineffective on the depth of the COS (14). It has been reported that the depth of the COS increased with the second molar tooth eruption and that the depth of COS decreased slightly during the adolescent dentition stage and then remained relatively stable into early adulthood (14). It is not possible that the occlusal attritions which may occur through aging affect the variables included in the present study in a consistent manner. For example, whereas the COS and CW may be changed by the occlusal attritions, the attrition is unlikely to affect the WALA-FA distance in the same way. Although the change in the CW is more significant, even in the event that the attrition is not similar in the cusps, it is likely that the depth of COS remains constant. Therefore, the present study enrolled adult patients aged 18 to 26 years with erupted second molar tooth, without clinically significant occlusal attritions, or without history of bruxism that may cause attrition in the teeth.
In the present study, the ROP was specified as the line passing the distal cusp tips of the second molar tooth and the cusp tips of the canine, and the depth of the COS and axial inclination of the teeth were measured using this line as reference. Several studies used the incisor sides of the incisor teeth, the distobuccal cusp of the second molar tooth, and the distal cusp of the last molar tooth as reference to determine the guide line (16, 22, 23).
The measurements performed on plaster models and photographs in the past have been replaced by three-dimensional digital models and advanced software that ensure collecting more comprehensive and detailed data from the models in this study. It was stated that the thickness of soft tissue may be effective during the determination of the WALA points on the model, thus these points may be specified more accurately by CBCT (24). Use of CBCT is recommended in limited indications, rather than using it routinely in orthodontic diagnosis and treatment planning (25). Additionally, it is not deemed realistic to subject the patient to radiation just to determine the form of the basal arch. It has been indicated that the WALA points can be determined at a highly reliable level on the models, and many studies have investigated the relationship between the basal arch and dental arch on digital models. In the literature, COS has been measured in different ways and included in the studies. In some studies, the deepest point of the curve was measured, whereas some of the investigators measured the perpendicular distance from the cusp tips of each tooth (14, 16, 18, 19). Two different studies reported that the deepest point corresponded to the mesiobuccal cusp of the first molar or was located in the second premolar tooth (26, 27). On the other hand, Bishara et al. (28) used the average of the sum of the perpendicular distances to each cusp tip. In the present study, the depth of COS was obtained for each tooth and by measuring the perpendicular distance from the cusp tips to the ROP. In the literature, apart from the investigations that measure CW by directly determining the axial inclination of the teeth in CBCT images (9), there were also measurements published in which the investigators create lines passing the buccal and lingual cusps of the teeth on the models, thereby removing the need for radiation. Similarly, the angle made by the line passing the cusp tips with the reference plane was measured in this study.
The present study compared the depth of the COS, the CW, and the WALA-FA distance measured in the right and left first premolar teeth and found a significant difference only in the depth of the COS. The studies in which the depth of the COS was analyzed as the maximum depth in the right and left arches did not demonstrate any significant difference between the right and left sides in the depth of the COS (14, 16). Shannon and Nanda (18) measured the depth of the COS individually in the posterior teeth and reported no significant difference between the right and left depth of the COS. The greatest difference detected for each of the three tooth groups was in the first molar teeth and was determined to be 0.41 mm on average [95% confidence interval (CI), −0.25 to −0.56]. Many studies have provided evidence that the measurements made on the digital models are reliable and accurate. The confidence limit was found to be 0.4 to 0.6 mm in the study measuring the depth of the COS (16). The difference which might be considered clinically insignificant may occur because of the measurement error. Likewise, in another study, Kim et al. (5) performed three-dimensional measurements for the WALA-FA distance at specified points on different planes and indicated that the ICC values were greater than 0.8 for the reliability of measurement. Although there are limited studies regarding the CW, the reliability was indicated to be 0.9 in a study that measured the CW in a way similar to that used in our study (19). The method used in the present study found ICC values to be greater than 0.9 in all of the measurements performed.
The literature indicates that the growth of orofacial structures, the eruption of the teeth, and the neuromuscular development affect the formation of the COS (14). According to Veli et al. (16), anterior teeth extrusion is effective on the deepening of the COS in class I and III malocclusions, whereas the posterior teeth extrusion is effective on the deepening of the curve in class II division II malocclusions. It is important for the orthodontic treatment planning and stability to evaluate the factors that might be effective in the deepening of the COS. The variables included in the present study are the subject of different studies; however, the correlations between these variables have not been investigated. The increased buccolingual inclinations of the teeth after orthodontic treatment may also induce the reduction in the WALA-FA distance. On the other hand, distal tipping, anterior tipping, or transverse expansion may occur in the molar teeth during the flattening of the COS. It is deemed possible that movements forcing the posterior teeth to buccal tipping on the transverse direction may directly affect the CW and WALA-FA distance. It is also possible that aforementioned changes achieved by orthodontic mechanics may be the result of the natural occlusal changes during the growth and development of the patients. Therefore, the correlation between these three variables was analyzed in this study where no high level of correlation was observed between these variables.
In the literature, there are varying results obtained in studies that compared the correlation between the basal arch and dental arch in various malocclusion groups (7, 8, 24). It has been suggested that the depth of the COS differs between the malocclusion groups (16). Similarly, the mandibular first premolar tooth in class II division I abnormalities have more lingual inclination than class 1 malocclusions, and there was no significant difference between the malocclusion groups in the mandibular second premolar and first molar teeth (6). On the basis of these results, it is possible that the type of malocclusion may cause differences in the measured parameters by the teeth groups. Therefore, it is not appropriate to extrapolate the results of this study to the other malocclusion groups. Therefore, further studies are needed investigating the correlation between the depth of the COS, the CW, and the WALA-FA distance in different malocclusion groups.
CONCLUSION
There was no strong correlation between the depth of the COS, the CW, and the WALA-FA distance. The CW and WALA-FA distances could not be effective on the deepening of the COS. Although there was a difference between the right and left arches in the depth of the COS, it was clinically insignificant. There was no significant difference between the right and left mandibular arches in the CW and WALA-FA distance.
Footnotes
Ethics Committee Approval: Ethics committee approval was received for this study from the ethics committee of Sağlık Bilimleri University Gülhane School of Dentistry.
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - F.D., G.S.D; Design - F.D., G.S.D.; Supervision - F.D., G.S.D.; Resources - F.D., A.T.; Materials - F.D, A.T., S.D.; Data Collection and/or Processing - G.S.D, A.T.; Analysis and/or Interpretation - F.D.; Literature Search - F.D., G.S.D; Writing Manuscript - F.D; Critical Review - F.D., G.S.D., A.T., S.G., S.D.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Little RM, Wallen TR, Riedel RA. Stability and relapse of mandibular anterior alignment-first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1981;80:349–65. doi: 10.1016/0002-9416(81)90171-8. https://doi.org/10.1016/0002-9416(81)90171-8. [DOI] [PubMed] [Google Scholar]
- 2.Raberin M, Laumon B, Martin JL, Brunner F. Dimensions and form of dental arches in subjects with normal occlusions. Am J Orthod Dentofacial Orthop. 1993;104:67–72. doi: 10.1016/0889-5406(93)70029-N. https://doi.org/10.1016/0889-5406(93)70029-N. [DOI] [PubMed] [Google Scholar]
- 3.Andrews LF. The 6-elements orthodontic philosophy: Treatment goals, classification, and rules for treating. Am J Orthod Dentofacial Orthop. 2015;148:883–7. doi: 10.1016/j.ajodo.2015.09.011. https://doi.org/10.1016/j.ajodo.2015.09.011. [DOI] [PubMed] [Google Scholar]
- 4.Lundstrom AF. Malocclusion of the teeth regarded as a problem in connection with the apical base. Int J Orthod Oral Surg. 1925;11:591–612. [Google Scholar]
- 5.Kim KY, Bayome M, Kim K, Han SH, Kim Y, Baek SH, et al. Three-dimensional evaluation of the relationship between dental and basal arch forms in normal occlusion. Korean J Orthod. 2011;41:288–96. https://doi.org/10.4041/kjod.2011.41.4.288. [Google Scholar]
- 6.Shu R, Han X, Wang Y, Xu H, Ai D, Wang L, et al. Comparison of arch width, alveolar width and buccolingual inclination of teeth between Class II division 1 malocclusion and Class I occlusion. Angle Orthod. 2012;83:246–252. doi: 10.2319/052412-427.2. https://doi.org/10.2319/052412-427.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gupta D, Miner RM, Arai K, Will LA. Comparison of the mandibular dental and basal arch forms in adults and children with Class I and Class II malocclusions. Am J Orthod Dentofacial Orthop. 2010;138:10.e11–18. doi: 10.1016/j.ajodo.2010.01.024. discussion 10–11. [DOI] [PubMed] [Google Scholar]
- 8.Zou W, Jiang J, Xu T, Wu J. Relationship between mandibular dental and basal bone arch forms for severe skeletal Class III patients. Am J Orthod Dentofacial Orthop. 2015;147:37–44. doi: 10.1016/j.ajodo.2014.08.019. https://doi.org/10.1016/j.ajodo.2014.08.019. [DOI] [PubMed] [Google Scholar]
- 9.Barrera JM, Llamas JM, Espinar E, Sáenz-Ramírez C, Paredes V, Pérez-Varela JC. Wilson maxillary curve analyzed by CBCT. A study on normocclusion and malocclusion individuals. Med Oral Patol Oral Cir Bucal. 2013;18:e547–52. doi: 10.4317/medoral.18291. https://doi.org/10.4317/medoral.18291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Andrews LF. The six keys to normal occlusion. Am J Orthod. 1972;62:296–309. doi: 10.1016/s0002-9416(72)90268-0. https://doi.org/10.1016/S0002-9416(72)90268-0. [DOI] [PubMed] [Google Scholar]
- 11.The gliding path of the mandible along the skull. Ferdinand Graf Spee (1855–1937), prosector at the Anatomy Institute of Kiel. J Am Dent Assoc. 1980;100:670–5. [PubMed] [Google Scholar]
- 12.Osborn JW. Orientation of the masseter muscle and the curve of Spee in relation to crushing forces on the molar teeth of primates. Am J Phys Anthropol. 1993;92:99–106. doi: 10.1002/ajpa.1330920108. https://doi.org/10.1002/ajpa.1330920108. [DOI] [PubMed] [Google Scholar]
- 13.Farella M, Michelotti A, van Eijden TM, Martina R. The curve of Spee and craniofacial morphology: a multiple regression analysis. Eur J Oral Sci. 2002;110:277–81. doi: 10.1034/j.1600-0722.2002.21255.x. https://doi.org/10.1034/j.1600-0722.2002.21255.x. [DOI] [PubMed] [Google Scholar]
- 14.Marshall SD, Caspersen M, Hardinger RR, Franciscus RG, Aquilino SA, Southard TE. Development of the curve of Spee. Am J Orthod Dentofacial Orthop. 2008;134:344–52. doi: 10.1016/j.ajodo.2006.10.037. https://doi.org/10.1016/j.ajodo.2006.10.037. [DOI] [PubMed] [Google Scholar]
- 15.El-Dawlatly MM, Fayed MMS, Mostafa YA. Deep overbite malocclusion: analysis of the underlying components. Am J Orthod Dentofacial Orthop. 2012;142:473–80. doi: 10.1016/j.ajodo.2012.04.020. https://doi.org/10.1016/j.ajodo.2012.04.020. [DOI] [PubMed] [Google Scholar]
- 16.Veli I, Ozturk MA, Uysal T. Curve of Spee and its relationship to vertical eruption of teeth among different malocclusion groups. Am J Orthod Dentofacial Orthop. 2015;147:305–12. doi: 10.1016/j.ajodo.2014.10.031. https://doi.org/10.1016/j.ajodo.2014.10.031. [DOI] [PubMed] [Google Scholar]
- 17.Warren JJ, Bishara SE. Comparison of dental arch measurements in the primary dentition between contemporary and historic samples. Am J Orthod Dentofacial Orthop. 2001;119:211–5. doi: 10.1067/mod.2001.112260. https://doi.org/10.1067/mod.2001.112260. [DOI] [PubMed] [Google Scholar]
- 18.Shannon KR, Nanda RS. Changes in the curve of Spee with treatment and at 2 years posttreatment. Am J Orthod Dentofacial Orthop. 2004;125:589–96. doi: 10.1016/j.ajodo.2003.09.027. https://doi.org/10.1016/j.ajodo.2003.09.027. [DOI] [PubMed] [Google Scholar]
- 19.Ali IM, Yamada K, Alkhamrah B, Vergara R, Hanada K. Relationship between occlusal curvatures and mandibular deviation in orthodontic patients with temporomandibular disorders. J Oral Rehabil. 2003;30:1095–103. doi: 10.1046/j.1365-2842.2003.01160.x. https://doi.org/10.1046/j.1365-2842.2003.01160.x. [DOI] [PubMed] [Google Scholar]
- 20.Nam SE, Park YS, Lee W, Ahn SJ, Lee SP. Making three-dimensional Monson’s sphere using virtual dental models. J Dent. 2013;41:336–44. doi: 10.1016/j.jdent.2013.01.003. https://doi.org/10.1016/j.jdent.2013.01.003. [DOI] [PubMed] [Google Scholar]
- 21.Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes: A systematic review. Am J Orthod Dentofacial Orthop. 2016;149:161–70. doi: 10.1016/j.ajodo.2015.06.029. https://doi.org/10.1016/j.ajodo.2015.06.029. [DOI] [PubMed] [Google Scholar]
- 22.Xu H, Suzuki T, Muronoi M, Ooya K. An evaluation of the curve of Spee in the maxilla and mandible of human permanent healthy dentitions. J Prosthet Dent. 2004;92:536–9. doi: 10.1016/j.prosdent.2004.08.023. https://doi.org/10.1016/j.prosdent.2004.08.023. [DOI] [PubMed] [Google Scholar]
- 23.Kumar KPS, Tamizharasi S. Significance of curve of Spee: An orthodontic review. J Pharm Bioallied Sci. 2012;4:323–8. doi: 10.4103/0975-7406.100287. https://doi.org/10.4103/0975-7406.100287. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Suk KE, Park JH, Bayome M, Nam YO, Sameshima GT, Kook YA. Comparison between dental and basal arch forms in normal occlusion and Class III malocclusions utilizing cone-beam computed tomography. Korean J Orthod. 2013;43:15–22. doi: 10.4041/kjod.2013.43.1.15. https://doi.org/10.4041/kjod.2013.43.1.15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kapila S, Conley RS, Harrell WE. The current status of cone beam computed tomography imaging in orthodontics. Dentomaxillofac Radiol. 2011;40:24–34. doi: 10.1259/dmfr/12615645. https://doi.org/10.1259/dmfr/12615645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Garcia R. Leveling the curve of Spee: a new prediction formula. J Charles H Tweed Int Found. 1985;13:65–72. [PubMed] [Google Scholar]
- 27.Koyama T. A comparative analysis of the curve of Spee (lateral aspect) before and after orthodontic treatment--with particular reference to overbite patients. J Nihon Univ Sch Dent. 1979;21:25–34. doi: 10.2334/josnusd1959.21.25. https://doi.org/10.2334/josnusd1959.21.25. [DOI] [PubMed] [Google Scholar]
- 28.Bishara SE, Jakobsen JR, Treder JE, Stasi MJ. Changes in the maxillary and mandibular tooth size-arch length relationship from early adolescence to early adulthood. A longitudinal study. Am J Orthod Dentofacial Orthop. 1989;95:46–59. doi: 10.1016/0889-5406(89)90135-2. https://doi.org/10.1016/0889-5406(89)90135-2. [DOI] [PubMed] [Google Scholar]