

Abstract
In adult patients with severe class II division 2 malocclusion, the ideal treatment option is the orthognathic surgery. However, camouflage therapy is also an acceptable treatment option due to its less traumatic and acceptable esthetic and functional results. In this case report, the camouflage treatment with two maxillary premolar extractions in a 21-year-old female patient who did not accept orthognathic surgery is presented. Acceptable esthetic and functional results were obtained at the end of the treatment.
Keywords: Camouflage treatment, en masse retraction, angle class II malocclusion, orthognathic surgery
INTRODUCTION
Skeletal and/or dental class II malocclusions are one of the most common orthodontic malocclusions. The reason for the skeletal class II malocclusion could be maxillary prognathism, mandibular retrognathia, or a combination of both (1).
With the recent advances in techniques, contemporary orthodontics, which makes function and esthetics the main target, provides different treatment approaches to each patient of any age group.
In skeletal class II anomalies, there are three different treatment approaches: functional treatment, orthodontic camouflage, and orthognathic surgery. Functional therapy provides an ideal outcome for the patients who are in the growing period, and camouflage treatment can be applied for patients whose growth and development have been completed. Orthodontic camouflage treatment can be described as masking of the dental or skeletal problem with orthodontic tooth movement and obtaining an acceptable occlusion and facial esthetics. However, for an adult patient with severe skeletal anomaly, the ideal treatment option is the orthognathic surgery. Today, owing to contemporary and less traumatic surgery techniques, orthognathic surgery has become a good option for orthodontists (2, 3). However, it is often not possible to convince patients and their parents for an operation to be performed under general anesthesia (4).
In this case report, camouflage treatment of a severe deep-bite and orthognathic surgery-required case with en masse retraction is presented. Informed consent was obtained from the patient for publication purposes.
CASE REPORT
In an intraoral examination, severe class II part 2 malocclusion was observed in a 21-year-old female patient who had applied to Cumhuriyet University, School of Dentistry, Orthodontics Department, with a complaint of the anterior teeth. It was determined that the midline was normal, the overjet was reduced, and the overbite was 7 mm. A convex profile related to mandibular retrognathia was observed in an extraoral examination.
According to Hayce Nance analysis, on mandible 2.5 mm and on maxilla 3.3 mm space are required; in the Bolton analysis, a 0.4 mm discrepancy on the maxilla for 6 anterior teeth and 1.3 mm discrepancy on the mandible for 12 teeth were found.
The panoramic evaluation revealed that all third molar teeth were present, and no pathology was found on the teeth and surrounding tissues.
On cephalometric evaluation, an ANB of 80 (SNA: 820, SNB: 740) was measured, skeletal class II malocclusion due to mandibular retrognathia was detected, and retroclination of the maxillary incisors (U1-SN: 830, U1-PP: 890) and slight proclination of the mandibular incisors (IMPA: 940) were observed. Additionally, the convexity angle (NA-APo: 150) was high, and the vertical growth angle (SN-GoMe: 300) was normal. An increase was observed in the nasolabial angle (nasolabial angle: 1120). The upper lip was located in the forward position according to the E line (upper lip-E plane [mm]: 2), and the lower lip was within normal limits according to E line (lower lip-E plane [mm]:-1). The parameters for the cephalometric evaluation are provided in Table 1.
Table 1.
Initial and final cephalometric values
| Parameters | Initial | Final | Normal |
|---|---|---|---|
| SNA (°) | 82 | 81 | 82±3.5 |
| SNB (°) | 74 | 76 | 80.9±3.4 |
| ANB (°) | 8 | 5 | 1.6±1.5 |
| Wits (mm) | 7 | 7 | −1±1 |
| Convexity (NA-APo) (°) | 15 | 10 | 4.9±3 |
| SN-GoGn (°) | 30 | 31 | 32.9±5.2 |
| FMA (°) | 25 | 25 | 23.9±4.5 |
| Y Angle (°) | 71 | 73 | 67±5.5 |
| PP-MP (°) | 28 | 27 | 25±6 |
| U1-SN (°) | 83 | 97 | 102.8±5.5 |
| U1-PP (°) | 89 | 103 | 110±5.0 |
| U1-NA (mm) | −4 | −1 | 4.3±2.7 |
| IMPA (°) | 94 | 96 | 95±7 |
| L1-NB (mm) | 3 | 4 | 4±1.8 |
| Interincisor angle (°) | 148 | 131 | 130±6 |
| Nasolabial angle (°) | 112 | 113 | 102±8 |
| Upper lip-E plane (mm) | −2 | −3 | −6±2 |
| Lower lip-E plane (mm) | −1 | −0.5 | −2±2 |
| Overjet (mm) | 3 | 2 | 2.5±2.5 |
| Overbite (mm) | 7 | 2 | 2.5±2 |
It was explained to the patient that because the profile was convex, mandibular retrognathia and orthognathic surgery were the ideal treatments to correct both profile convexity and intraoral malocclusion. The surgical treatment option was not accepted by the patient; therefore, we decided to use camouflage treatment by premolar extraction of two maxillary teeth.
Process of Treatment
The levelling process lasted for 4 months, and in this step, the Roth .018 bracket system and archwires were used in the order of 0.014 nickel-titanium (Niti; 1 month), 0.016 Niti (1 month), .016×.022 Niti (1 month), .and 017×.025 Niti (1 month). Simultaneously, the lower dental arch was leveled with the same bracket system. After the leveling step, two miniscrews (Neo Anchor Plus, Myungsung, Korea) with a diameter of 1.6 mm and a length of 10 mm were placed bilaterally between the roots of the upper second premolar and first molar. Subsequently, the en masse retraction of six anterior teeth was started by using TAD springs (C3 medium, G & H Wire Comp., USA), which are located on 017×.025 SS archwire with a slightly accentuated curve of Spee. During the en masse retraction, 200 g forces were applied bilaterally. After a total of 8 months of retraction, the canines were brought into class I relationship and the miniscrews were removed. The remaining spaces were closed in 2 months with mesialization of the posterior teeth, and the treatment was completed in 14 months.
Treatment Results
At the end of treatment, the ideal overjet, overbite, and class I canine and class II molar relationships were obtained. The upper incisor angles were brought to normal limits (U1-SN: 970, U1-PP: 1030), and there was no significant change at the lower incisor angles (IMPA: 940). While there was no significant change in the nasolabial angle (nasolabial angle: 112 to 1130), an increase in the distance between the upper lip and E line (upper lip-E plane [mm]: -2 to -3) and a decrease in the distance between the lower lip and E line (lower lip-E plane [mm]:-1 to -0.5) were observed. The post-treatment cephalometric evaluation is provided in Table 1.
DISCUSSION
Only cephalometric evaluation and clinical observations are not always sufficient during treatment planning of borderline cases for orthognathic surgery. External factors, such as the environment, family, friends, and business life, should be considered while planning the treatment (5). Patients and their relatives who see the post-treatment profile simulation created by the orthodontic software before the operation might not consider the profile, which the orthodontists accept as ideal satisfactory. For patients who are not satisfied with facial esthetics, orthognathic surgery is offered as an option, whereas for those who do not complain about facial appearance, camouflage therapy is offered when skeletal problem can be masked by the rearrangement of dentoalveolar structure (6–8). In this case report, a miniscrew-assisted camouflage treatment was presented about the case in which the patient complained about the appearance of the anterior teeth but not the facial esthetics.
According to literature, class II dental camouflage can be treated by extracting two premolars from the upper jaw and two from the lower jaw, and it can also be performed by extracting only the upper two premolar when there is no crowding on the lower dental arch (9, 10). Anterior retraction can be done in two ways: “progressive retraction” in which canine and incisors are retracted in two stages or “en masse retraction” in which the anterior 6 teeth are retracted in one stage. In the progressive retraction, the canines are first distalized and then incisor retraction is performed with different mechanics. The purpose of this technique is to reduce the load on the posterior anchorage unit by retracting the canine and incisors in two separate steps (11). In this method, the extraction spaces are closed with minimum anchorage loss, but because of two separate stages, the treatment time is longer. In addition, the anterior movement of the extraction space and its long-term existence cause esthetic and social anxiety, particularly in adult patients. Besides, more tipping and rotation of the canines are observed because they are distalized alone (12).
When compared with progressive retraction, the en masse retraction shortens the duration of treatment and provides early correction on the profile; thereby, it positively influences the treatment of the patient. In addition, force application can be finished at the point where it is decided that the desired target for the profile and occlusion have been obtained. The mechanics are simpler and allow closing of the extraction spaces without changing the leveling and alignment of the teeth (13). However, in this technique, the load on the posterior teeth that are taken as an anchorage unit is greater. To eliminate this disadvantage of the en masse retraction technique, miniscrews were placed in the posterior region for enhancing anchorages, and the anterior six teeth were retracted as one unit.
Anchorage loss can be seen in conventional retraction techniques in which molar anchorage is used but not miniscrew. Storey and Smith used conventional molar anchors during canine retraction and found an anchorage loss ranging from 5% to 50% (14). Badri et al. used molar teeth and miniscrews as anchorage units in the canine retraction procedure. In the group for which the molar teeth were used as anchorage, anchorage loss was 1.6 mm on the upper jaw and 1.7 mm on the lower jaw, but no anchorage loss was observed in the group for which miniscrews were used.
Miniscrew-assisted retraction also has some advantages, such as maximum anchorage and the opportunity of applying intrusion and retraction forces together (15). There are two components of the forces that were applied to the power arms from the miniscrew: horizontal and vertical. Retraction is achieved by the horizontal component, while the vertical component applies intrusion forces to the anterior teeth. However, since the force vector is below the resistance center of the anterior teeth, the moment caused by this force vector causes the lingual movement of incisors. In this case, both retraction and intrusion movements of the anterior teeth were performed in desired amounts by using miniscrew (Figure 4).
Figure 4.
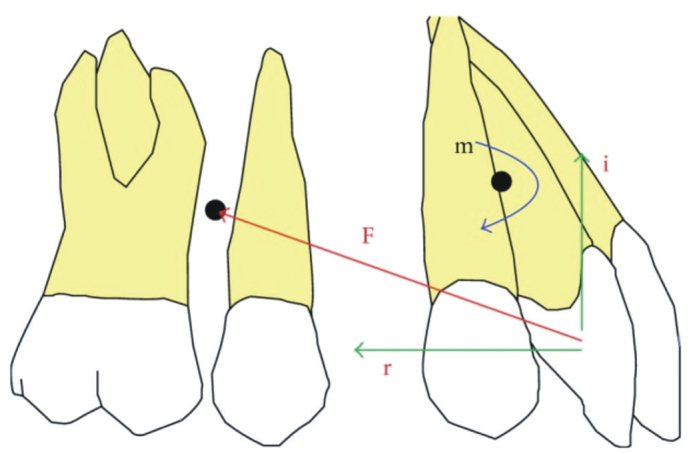
F: Applied force; I: intrusive effect; R: retraction effect; M: moment generated in the anterior teeth
Due to the retraction of the upper anterior teeth, the upper lip went slightly backwards; hence, an increase was observed in the distance between upper lip and E line. However, a decrease was observed in the distance between lower lip and E line because of lower anterior teeth protrusion. Because of these changes in the upper and lower lips, better facial profile was obtained at the end of the treatment.
If we had treated our patient with orthognatic surgery, we could have achieved ideal results in soft tissues. Since the patient had not accepted the surgical treatment option, and had no complaint regarding her profile, she was treated with extraction of teeth to camouflage the skeletal problem. At the end of treatment, not ideal but acceptable soft tissue values were obtained.
CONCLUSION
A severe Class II division 2 malocclusion case was treated without orthognatic surgery, with two maxillary premolars extraction in 14 months. At the end of the treatment, better occlusion and facial esthetics were obtained. In borderline Class II cases, en masse retraction of the maxillary incisors can be an alternative when miniscrews are used as anchorage, for both horizontal and vertical control, in suitable cases. This treatment protocol might also shorten the duration of treatment.
Figure 1. a–j.

Initial intraoral and extraoral pictures and panoramic cephalometric radiograph. Initial extraoral frontal rest image (a). Initial extraoral frontal smile image (b). Initial extraoral profile image (c). Initial intraoral upper occlusal image (d). Initial intraoral lower occlusal image (e). Initial intraoral right lateral image (f). Initial intraoral frontal image (g). Initial intraoral left lateral image (h). Initial cephalometric image (i). Initial panoramic radiograph image (j).
Figure 2. a–d.

In progress intraoral pictures. Progress intraoral right lateral image (a). Progress intraoral frontal image (b). Progress intraoral left lateral image (c). Progress intraoral occlusal image (d)
Figure 3. a–j.

Final intraoral and extraoral pictures and panoramic cephalometric radiograph. Final, extraoral frontal rest image (a). Final, extraoral frontal smile image (b). Final extraoral profile image (c). Final intraoral upper occlusal image (d). Final intraoral lower occlusal image (e). Final intraoral right lateral image (f). Final intraoral frontal image (g). Final intraoral left lateral image (h). Final cephalometric image (i). Final panoramic radiograph image (j).
Figure 5.
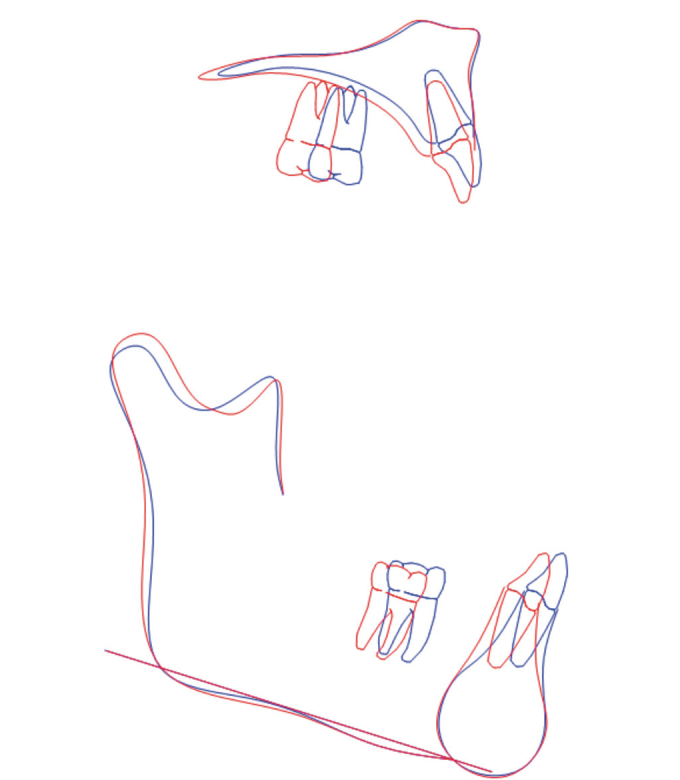
Local cephalometric superimposition of both the maxilla and mandible
Figure 6.
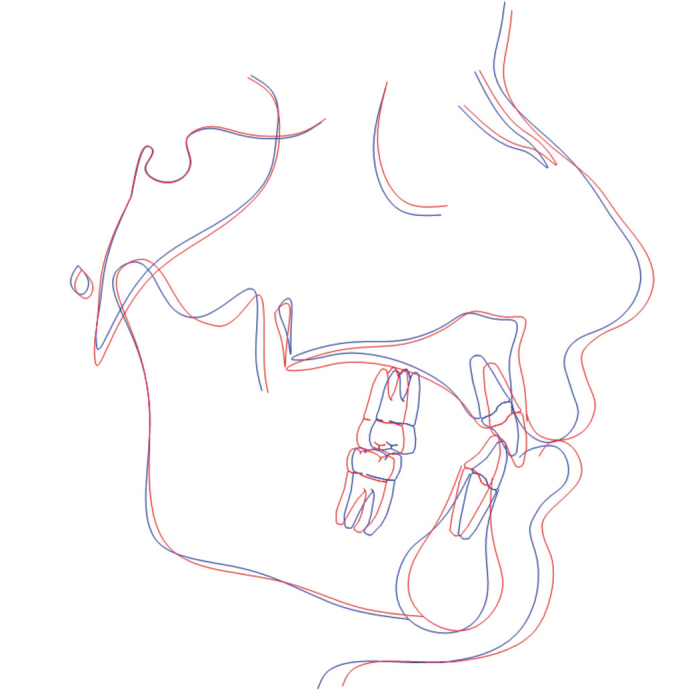
Total cephalometric superimposition (based on S-N plane)
Footnotes
Informed Consent: Written informed consent was obtained from the patient.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - Z.Ç.B.; Design - H.C.; Supervision - C.D.; Resources - H.C.; Materials Z.Ç.B.; Data Collection and/or Processing - Z.Ç.B.; Analysis and/or Interpretation - H.C., C.D.; Literature Search - Z.Ç.B.; Writing Manuscript - H.C.; Critical Review - H.C., C.D.; Other - Z.Ç.B.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Acar Güngör A. Molar distalization in the treatment of class II malocclusions. EÜ Dişhek Fak Derg. 2006;27:97–105. [Google Scholar]
- 2.Sarver DM. Esthetic Orthodontics and Orthognathic Surgery. St Louis: Mosby Inc; 1998. pp. 2–7. [Google Scholar]
- 3.Kuhlberg AJ, Glynn E. Treatment planning considerations for adult patients. Dent Clin North Am. 1997;41:17–27. [PubMed] [Google Scholar]
- 4.Kubein-Meesenburg D, Ihlow D. The problems of borderline cases: an aid for the analysis of orthodontic therapies. J Orofac Orthop. 2006;67:207–14. doi: 10.1007/s00056-006-0548-2. https://doi.org/10.1007/s00056-006-0548-2. [DOI] [PubMed] [Google Scholar]
- 5.Ackerman JL, Proffit WR. Soft tissue limitations in orthodontics: treatment planning guidelines. Angle Orthod. 1997;67:327–36. doi: 10.1043/0003-3219(1997)067<0327:STLIOT>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Ruf S, Pancherz H. Orthognathic surgery and dentofacial orthopedics in adult Class II Division 1 treatment: mandibular sagittal split osteotomy versus Herbst appliance. Am J Orthod Dentofacial Orthop. 2004;126:140–52. doi: 10.1016/j.ajodo.2004.02.011. https://doi.org/10.1016/j.ajodo.2004.02.011. [DOI] [PubMed] [Google Scholar]
- 7.Bell R, Kiyak HA, Joondeph DR, McNeill RW, Wallen TR. Perceptions of facial profile and their influence on the decision to undergo orthognathic surgery. Am J Orthod. 1985;88:323–32. doi: 10.1016/0002-9416(85)90132-0. https://doi.org/10.1016/0002-9416(85)90132-0. [DOI] [PubMed] [Google Scholar]
- 8.Mihalik CA, Proffit WR, Phillips C. Long-term follow-up of Class II adults treated with orthodontic camouflage: a comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2003;123:266–78. doi: 10.1067/mod.2003.43. https://doi.org/10.1067/mod.2003.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Upadhyay M, Yadav S, Nagaraj K, Nanda R. Dentoskeletal and soft tissue effects of mini-implants in class II division 1 patients. Angle Orthod. 2008;79:240247. doi: 10.2319/013008-52.1. [DOI] [PubMed] [Google Scholar]
- 10.Bishara SE, Cummins DM, Jakobsen JR, Zaher AR. Dentofacial and soft tissue changes in class II, Division 1 cases treated with and without extractions. Am J Orthod Dentofacial Orthop. 1995;107:28–37. doi: 10.1016/s0889-5406(95)70154-0. https://doi.org/10.1016/S0889-5406(95)70154-0. [DOI] [PubMed] [Google Scholar]
- 11.Proffit WR, Fields H. The biologic basis of orthodontic therapy. Contemporary orthodontics. 2000:4. [Google Scholar]
- 12.Xu TM, Zang X, Oh HS, Boyd RL, Korn EL, Baumrind S. Randomized clinical trial comparing control of maxillary anchorage with 2 retraction techniques. Am J Orthod Dentofacial Orthop. 2010;138:544.e1–9. doi: 10.1016/j.ajodo.2009.12.027. discussion 544–5. [DOI] [PubMed] [Google Scholar]
- 13.Park HS, Kwon TG. Sliding mechanics with microscrew implant anchorage. Angle Orthod. 2004;74:703–10. doi: 10.1043/0003-3219(2004)074<0703:SMWMIA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 14.Qamruddin I, Shahid F, Alam MK, Zehra Jamal W. Camouflage of Severe Skeletal Class II Gummy Smile Patient Treated Nonsurgically with Mini Implants. Case Rep Dent. 2014;2014:382367. doi: 10.1155/2014/382367. https://doi.org/10.1155/2014/382367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Badri T, Pavithranand A, Rajasigamani K, Kyung HM. Comparison and measurement of the amount of anchorage loss of the molars with and without the use of implant anchorage during canine retraction. Am J Orthod Dentofacial Orthop. 2006;129:551–54. doi: 10.1016/j.ajodo.2005.12.014. https://doi.org/10.1016/j.ajodo.2005.12.014. [DOI] [PubMed] [Google Scholar]