

Abstract
The aim of the present study was to evaluate the effects of the miniscrew-supported, modified Hyrax appliance on bilateral distalization of posterior teeth. A 15-year-old girl with Class II malocclusion (end-to-end molar relationships, space deficiency for maxillary canine) underwent orthodontic treatment. The patient rejected tooth extraction. Then, she was treated with the miniscrew-supported, modified Hyrax appliance. An activation of 1 mm per month was planned. Lateral cephalometric views were used to evaluate distal movement. Distalization was successfully achieved at 4 months. No anchorage loss and incisor protrusion were noted. It would be beneficial to choose this appliance for the distalization of maxillary molars in patients with maxillary incisor protrusion, as this appliance does not cause anchorage loss in the upper jaw.
Keywords: Mini distalization, mini screw, anchorage
INTRODUCTION
Class II malocclusion is the most common type of malocclusion encountered in the practice of orthodontics. Class II malocclusion characterized by proclination of the maxilla and/or upper dental arch or retroclination of the mandible and/or lower dental arch or combination of these is a type of malocclusion in which accurate diagnosis and appropriate treatment can yield successful outcomes (1). Distalization of the upper buccal segment is one of the treatment options in cases with dental Class II and skeletal Class I or II malocclusion in which lower dental arch is aligned properly (2). In addition to, when space deficiency is combined with missing or previous extracted teeth and a tendency toward molar Class II relationship, the first choice for providing space and solve the problem is distal movement of posterior teeth.
Extraoral traction, one of the traditional techniques for molar distalization, is often a method to distalize maxillary molar teeth (3). The application of various maxillary distalization appliances has recently shown clinical success. Classical intraoral molar distalization techniques such as Schwartz plaque-type appliances, Wilson distalization arches, coil spring appliances, distal jet, repelling magnets, and pendulum appliances are commonly used (4–7). Herein, we report a female case with class II malocclusion in whom orthodontic treatment was applied and distalization was successfully achieved at 4 months.
CASE PRESENTATION
A 15-year-old female patient presented to our clinic complaining of crowded anterior teeth. Her past medical history was unremarkable. She had facial symmetry and balanced appearance with a slightly convex profile. During intraoral examination, maxillary canine teeth were localized in the vestibule due to space deficiency in the dental arch, and with the exception of these teeth, all teeth including second molar teeth erupted. The wisdom teeth were unable to be visualized on panoramic view. There was space deficiency in the maxillary arch and mildly crowded teeth in the mandibular arch (Figure 1). The patient had dental class II relationship. Cephalometric examination revealed no skeletal problems.
Figure 1. a–h.

Pretreatment-intraoral and extraoral photographs, lateral cephalometry, and panoramic radiograph; pretreatment photograpghs of the patients (a); intraoral frontal image (b); intraoral right image (c); intraoral left image (d); intraoral photographs of the patients (e); intraoral photographs of the patients (f); pretreatment panoramic film (g); pretreatment lateral cephalometric film (h)
The patient was offered two treatment options. The first option involved the extraction of premolar teeth, and the second option involved distalization of maxillary posterior teeth, and the patient accepted the second option.
Treatment Progress
The appliance was designed to produce a distalization force in the upper molar teeth. The placement of two palatal miniscrews (1.7’8 mm2) (Tomas Anchorage System, Dentaurum, Ispringen, Germany) under local anesthesia was planned to be used as an anchor unit of the appliance. The miniscrews were placed 6 to 8 mm distal to the incisive papilla and 3 mm distant to the midpalatal suture, and orthodontic bands were applied on the first molar teeth.
Laboratory Process
A silicon impression was then taken after application of transfer caps. Laboratory analogues were placed on the transfer caps, the bands were positioned in the impression, and a plaster model was made. Afterward, two standard abutments were screwed on top of the laboratory analogues. Posterior legs of Hyrax were welded to first maxillary molar bands. Anterior legs of Hyrax and two screws were connected by welding anteriorly onto the two abutments. The expansion vector was set anteroposteriorly.
After the maxillary molar teeth are temporarily inserted, the modified Hyrax appliance (Forestadent memory screw, Pforzheim, Germany) was fixed on the mini-implants followed by the final seating on the molars. While screwing the abutment screws, the modified Hyrax was gently pressed onto the mini-implants to facilitate the fixation. This distalization unit, with its two miniscrews and two molar bands, provided stable and 4-point support for the appliance when placed parallel to occlusal plane (Figure 2).
Figure 2.

The appliance used in the study
The modified Hyrax appliance (Forestadent memory screw, Pforzheim, Germany) was used for the distalization of maxillary molar teeth. According to the manufacturer, the memory screw delivers a total force of 800 grams in activation of every 1 millimeter. The Hyrax opening rate was 1.0 mm per month.
Lateral cephalometry was used to determine the amount of distal movements. The stability of the appliance, miniscrews, and oral hygiene were evaluated at each one of the monthly appointments. After 4 months, the molars had distalized by 3–4 mm, and class I relationship in molars and premolars was obtained. Post-distal driving extra-intraoral views were seen in Figure 3. Cephalometric analysis was used to evaluate changes of molar position, inclination, and mandibular plane angle (Figure 4). Orthodontic treatment was completed in a 13-month period. Molar teeth were distalized, arch-length was increased at buccal position, and malpositioned canine teeth were placed in the dental arch. Dental class I relationship was established. Cephalometric parameters before and after distalization and after treatment are shown in Table 1. Written informed consent was obtained from patients’ parents for the publication of treatment results.
Figure 3. a–h.

Posttreatment-intraoral and extraoral photographs, lateral cephalometry, and panoramic radiograph; posttreatment photographs of the patients (a); intraoral frontal image (b); intraoral right image (c); intraoral left image (d); intraoral photographs of the patients (e); intraoral photographs of the patient (f); posttreatment panoramic film (g); posttreatment lateral cephalometric film (h)
Figure 4.
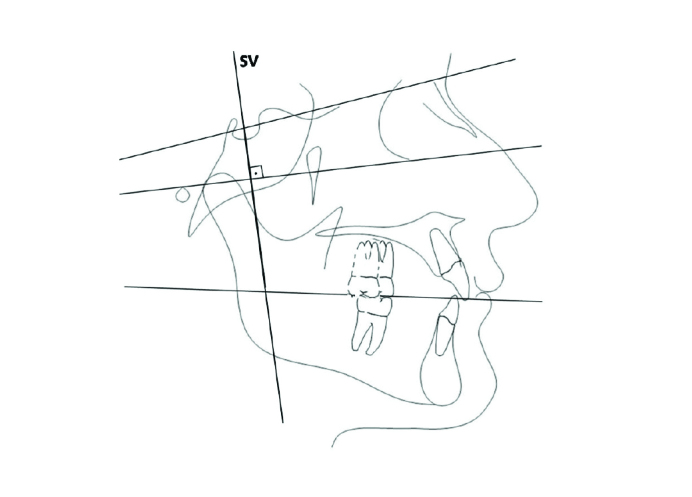
Vertical reference plane perpendicular from S to FH (SV)
Table 1.
Cephalometric variables at pretreatment (TO) and posttreatment (T1)
| Measurement | Pre treatment (T0) | Post treatment (T1) |
|---|---|---|
| SNA(°) | 82 | 82.2 |
| SNB(°) | 78.9 | 80.4 |
| SN-MP (°) | 30 | 30.7 |
| FMA (°) | 26.1 | 27.8 |
| Y angle (°) | 59.5 | 60.9 |
| SV-U1(mm) | 70.3 | 68.7 |
| SV-U6(mm) | 42 | 39.3 |
| SV-U7(mm) | 32 | 28 |
| Over-jet (mm) | 3.8 | 3.4 |
| Over-bite (mm) | 1.6 | 2.2 |
| UL-E (mm) | −6.2 | −6.2 |
SNA: angle between S-N and N-A; SNB: angle between S-N an N-B; SN-MP: angle between SN and mandibular planes; FMA: angle between FH and mandibular planes; Y angle (°): angle between SN to SGn; SV-U1(mm): SV (from sella, perpendicular to Frankfort Horizontal Plane); SV-U6(mm): distance from SV (from sella, perpendicular to Frankfort Horizontal Plane) to U6; SV-U7(mm): distance from SV (from sella, perpendicular to Frankfort Horizontal Plane) to U7v
DISCUSSION
In the present case, we evaluated the effects of the miniscrew-supported, modified Hyrax appliance on bilateral distalization of posterior teeth. The aim of the case was to remind clinicians and update information about miniscrew-assisted memory screw unit for distalization of maxillary molars as a noncompliance therapy.
Extraoral appliances such as headgear appliances offer the advantage of stabilizing the anterior teeth, whereas these appliances are associated with patient complaints and distal tipping and extrusion of molar teeth. Furthermore, these appliances may cause psychological problems and neck pain in the patients (2, 8).
The most significant disadvantage associated with classical intraoral distalization techniques is the anchorage loss. These appliances use anterior teeth or palate as the anchorage unit similar to Schwartz plaque-type appliances, Wilson distalization arches and distal jet (3, 4, 6). This results in protrusion of incisors and anchorage loss. The reason is that teeth move in response to the repelling forces (9). To prevent undesired tooth movement, additional measures are often required during to support anchorage teeth when maximum anchorage is needed during orthodontic treatment (10). Thus, many interventions have been performed for the use of tooth implants as an anchorage unit for orthodontic appliances (11). According to many authors, hard palate is an appropriate and temporary anatomic location for the placement of implants (12).
The use of miniscrew-supported appliance in the present study avoided these complications. The rigid arms of the screw did not allow a spontaneous upright position of the molars during the distalization period. The distal tipping of the molar crowns may be disadvantageous for anchorage but, as shown in the present study, the distalization appliance can be used as a retention appliance, and thus any possible anchorage loss can be prevented by leaving the appliance. In this case, the treatment corrected molar class I relationship with distalization of molar teeth in a short period of 4 months and provided space for normal positioning of canine teeth in the dental arch that are thought to erupt in the vestibule without need for further intervention. There are different views regarding distalization speed and therefore treatment time in the presence of second molar teeth. Some authors suggested that distaliziation speed was not affected by the presence of second molar teeth, whereas others reported decreased distalization speed (13, 14). Many studies on distalization of upper molar teeth reported upper molar distalization between 2.5 and 6.4 mm within an approximate duration of 1.5 to 13 months depending in the requirements of the individuals (15). As distalization of molar teeth was achieved in a parallel manner avoiding deviation in our case and second molar teeth had already erupted, the mean distalization time in our case was longer than those reported in the aforementioned studies. Although deviation of molar teeth during distalization seems to be reducing the treatment time, correcting deviated molar teeth would be time consuming and would also cause anchorage loss as mentioned previously.
No complication occurred related to the miniscrews during the distalization process. The most important advantage of the distalization system used in the present study is the lack of need for patient cooperation during the treatment and lack of anchorage loss due to minimum protrusion of the incisors. It would be beneficial to choose this appliance for the distalization of maxillary molars in patients with maxillary incisor protrusion, as this appliance does not cause anchorage loss in the upper jaw.
CONCLUSION
In conclusion, miniscrew-supported, modified Hyrax appliances provide distalization of posterior teeth by reducing the treatment time and avoiding undesired anterior teeth movement. Therefore, as in our case, we suggest that miniscrew-supported intraoral distalization appliances can be used in patients of all ages with angle class II malocclusion in whom the upper first molar teeth have erupted.
Footnotes
Informed Consent: Written informed consent was obtained from the patient who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - M.A.; Design - F.A.; Supervision - M.A.; Materials - F.A.; Writing Manuscript - M.A.; Other - U.O.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Altuğ A. DoktoraTezi. Ankara Üniversitesi Sağlık Bilimleri Enstitüsü; Ankara: 2002. 3D bimetrik maksiller distalizasyon arkı ileservikal headgear te- davisinin dentofasiyal yapılara olan etkilerinin karşılaştırmalı olarak incelenmesi. [Google Scholar]
- 2.Sabri R. Treatment of a severe arch-length deficiency with anteroposterior and transverse expansion: long-term stability. Am J Orthod Dentofacial Orthop. 2010;137:401–11. doi: 10.1016/j.ajodo.2007.08.040. [DOI] [PubMed] [Google Scholar]
- 3.Haas AJ. Headgear therapy: the most efficient way to distalize molars. Semin Orthod. 2000;6:79–90. doi: 10.1053/od.2000.5900. [DOI] [Google Scholar]
- 4.Schwarz AM. Gebissregelungmit platten. 5th ed. Wien Innsbruck: Urban & Schwarzenbeg; 1947. [Google Scholar]
- 5.Muse DS, Fillman MJ, Emmerson WL, Mitchell RD. Molar and incisor changes with Wilson rapid molar distalization. Am J Orthod Dentofacial Orthop. 1993;104:556–65. doi: 10.1016/S0889-5406(05)80439-1. [DOI] [PubMed] [Google Scholar]
- 6.Locatelli R, Bednar J, Dietz VS, Gianelly AA. Molar distalization with superelastic NiTi wire. J Clin Orthod. 1992;26:277–9. [PubMed] [Google Scholar]
- 7.Hilgers JJ. The pendulum appliances for Class II non- compliance therapy. Clin Orthod. 1992;26:706–14. [PubMed] [Google Scholar]
- 8.Papadopoulos MA. Orthodontic treatment of Class II malocclusion with miniscrew implants. Am J Orthod Dentofacial Orthop. 2008;134:604. doi: 10.1016/j.ajodo.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 9.Arman A, Gökçelik A. Ağıziçi molar distalizasyon yöntemleri. Cumhuriyet Univ Dis Hek Fak Derg. 2005;8:48–55. [Google Scholar]
- 10.Bernhart T, Vollgruber A, Gahleitner A, Dörtbudak O, Haas R. Alternative to the median region of the palate for placement of an orthodontic implant. Clin Oral Impl Res. 2000;11:595–601. doi: 10.1034/j.1600-0501.2000.011006595.x. [DOI] [PubMed] [Google Scholar]
- 11.Roberts WE, Helm FR, Marshall KJ, Gangloff RK. Rigid endosseous implants for orthodontic and orthopedic anchorage. Angle Orthod. 1989;59:247–56. doi: 10.1043/0003-3219(1989)059<0247:REIFOA>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Wehrbein H, Merz BR, Diedrich P. Palatal bone support for orthodontic implant anchorage-a clinical and radiological study. Eur J Orthod. 1999;21:65–70. doi: 10.1093/ejo/21.1.65. [DOI] [PubMed] [Google Scholar]
- 13.Ghosh J, Nanda RS. Evaluation of an intraoral maxillary molar distalization technique. Am J Orthod Dentofac Orthop. 1996;110:639–46. doi: 10.1016/S0889-5406(96)80041-2. [DOI] [PubMed] [Google Scholar]
- 14.Hilgers JJ. The pendulum appliance for Class II noncompliance therapy. J Clin Orthod. 1992;26:706–14. [PubMed] [Google Scholar]
- 15.Fortini A, Lupoli M, Gıuntoli F, Franchi L. Dentoskeletal effects induced by rapid molar distalization with the first class appliance. Am J Orthod Dentofacial Orthop. 2004;125:697–705. doi: 10.1016/j.ajodo.2003.06.006. [DOI] [PubMed] [Google Scholar]