

Abstract
A 15-year-old female presented with the chief complaint of crowding. Extraoral examination revealed little facial asymmetry, which was related with mandibular deviation caused by constriction of the maxilla. Upon intraoral examination, Class III molar and Class II canine relationships were seen on the right side, and Class III molar and Class III canine relationships were seen on the left side. A morphological lower midline shift was detected (4 mm to the right). After the start of treatment with rapid maxillary expansion, miniscrews were inserted into the buccal shelf and canine-premolar areas in order to solve the morphological deviation without extractions. Because there was a need to shift the lower midline to the right side, miniscrews were inserted into the left buccal shelf at the right canine-premolar area. The miniscrews were placed vertically so that the angle between the long axes of the teeth and the long axes of the screws were approximately 20 degrees. Acceptable correction of the midline deviation lasted for four months. At the end of the treatment, a good occlusal relationship was obtained.
Keywords: Dento-alveolar asymmetries, diagnosis, midline deviation, treatment strategies, mini-screw
INTRODUCTION
Midline deviation is one of the more difficult problems that orthodontists encounter. This problem is most commonly found in Class II cases, but it might be seen in all types of malocclusions (1). In order to correct midline deviation, it is necessary to make correct differential diagnosis in order to determine the correct etiology and to evaluate the effects on the occlusion. General causes of midline deviation are (1):
Lateral mandibular deviation that might be related with posterior cross-bite or not.
Tipping and/or drifting on the upper and/or lower incisors.
Asymmetries of the upper and/or lower arch.
Any combination of these factors.
Miniscrews are orthodontic anchorage units fixed into the bone that strengthen the orthodontic anchorage and minimize the loss of anchorage by supporting the teeth in the anchorage unit. Various extraoral appliances have been designed to provide anchorage control in routine orthodontic practices. Although these extraoral appliances are effective methods for anchorage control, the requirement for the patient’s cooperation is their biggest disadvantage. Therefore, a number of intraoral anchors (miniscrews, onplants, miniplates, Graz implants, etc.) have been developed in recent years that eliminate the need for patient cooperation. Miniscrews can be used in extraction cases, for example, instead of headgear (2,3). Miniscrews can also be an aid in the orthodontic mechanics and are used for mesialization, distalization, intrusion of posterior teeth, or extrusion of impacted canines (4,5).
CASE PRESENTATION
A 15-year-old female patient presented to our clinic with the complaint of upper left lateral crowding. On extraoral examination, facial asymmetry was observed, which was thought to be related with maxillary constriction. On the right side, Class III molar and Class II canine relationships were seen, and on the left side Class III molar and canine relationships were seen. Additionally, there was a lower midline shift (4 mm to the right), a unilateral posterior crossbite on the right side, and an anterior edge-to-edge relationship of the anterior teeth. In panoramic radiograph, all four wisdom teeth were absent (Figure 1).
Figure 1. a–i.

Initial intraoral and extraoral photographs and panoramic radiograph: initial, extraoral frontal rest image (a); initial, extraoral frontal smile image (b); initial, extraoral profile image (c); initial, intraoral frontal image (d); initial, intraoral right lateral image (e); initial, intraoral left lateral image (f); initial, intraoral upper occlusal image (g); initial, intraoral lower occlusal image (h); initial, panoramic radiograph image (i)
Cephalometric measurements revealed a skeletal Class III relationship–SNA:83°, SNB:85°, ANB: −2° with a slightly prognathic mandible–but it was not prominent on the facial profile clinically, and the patient did not desire any change in her facial profile. The patient only wanted to correct the incisor irregularity and relationship.
Our treatment objectives were:
to correct the posterior transversal relationship and the mandibular midline deviation
to align the upper and lower crowding
to obtain a normal overjet and overbite
to establish a Class I molar and canine relationship
Ankylosis of the maxillary first molar was noted; however, the treatment of this phenomenon was not planned.
In order to correct the cross-bite, rapid maxillary expansion (RME) was applied in the initial stages of treatment, and there was no change in midline deviation after expansion. This finding was in line with our initial clinical examination that the midline deviation was not functional.
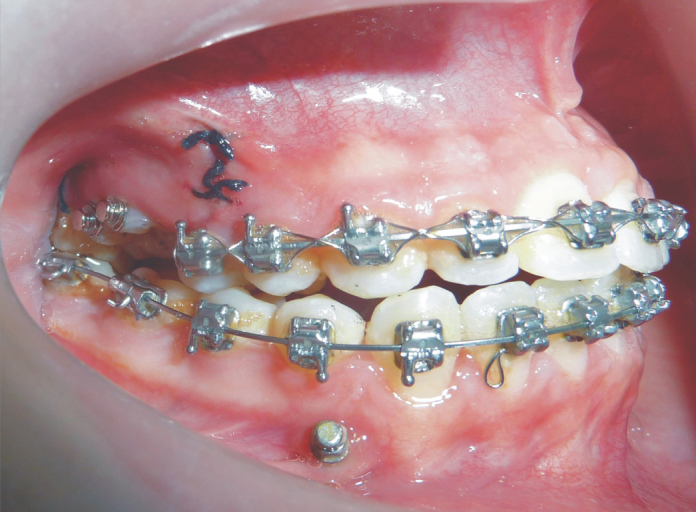
After six months of leveling and alignment, two 1.6 mm-diameter and 10 mm-long miniscrews (Jeil Med. Corp.; Seoul, Korea) were inserted into the left buccal shelf at the right canine-premolar area. This area was selected due to the fact that the lower midline was shifted to the right. After the insertions, a second panoramic radiograph was taken to evaluate the position of the miniscrews (Figure 2). On the right side, a 300 g force was applied from the screw located between the canine and first premolar to the surgical hook that was located at mesial to the right first molar. In the same way, a 300 g force was also applied on the left side from the screw located on the buccal shelf area to the surgical hook that was located mesial of the canine. These forces were applied on a .019 × .025″ SS arch wire until midline shift was corrected. Correction of the midline deviation lasted for four months. At the end of the treatment, a good occlusal relationship was obtained, but there was still a small but acceptable midline deviation and some facial asymmetry. And maxillary right first molar could not be extruded because of the ankylosis (Figure 3). After segmental osteotomy, extrusive force was applied from buttons. But no extrusion movement was observed. Second surgical requirement was explained to patient. But the patient did not want to undergo to surgery for the second time. Informed consent was obtained from the patient for this publication.
Figure 2. a–d.

In-progress intraoral and extraoral photographs and panoramic radiograph: intraoral frontal image (a); intraoral right lateral image (b); intraoral left lateral image (c); panoramic radiograph image (d)
Figure 3.
Extrusion of the maxillary right first molar
DISCUSSION
Clinically, the nasal tip, nasal base, philtrum, and midpoint of the chin are the reference points for detection of the facial midline (6). Photographs or videos might also be used for this purpose, but the clinical examination for determination of the midline deviation gives more reliable results (7). Midline deviation can be related to skeletal, dentoalveolar, or soft-tissue asymmetries or some combination of these (8). General reasons for the existence of midline deviations are early loss of primary teeth, abnormal tooth eruption, and extraction of permanent teeth (7).
Narrowed maxillary arches also can cause a deviation of the mandible, which is called functional mandibular deviation. Our patient also had a narrowed maxilla; however, the maxillary constriction did not cause a functional deviation. In our case, only a morphological lower midline deviation was present. After RPE, the deviation remained. Usually morphological dental midline deviation can be corrected through asymmetric tooth extraction, stripping, or a combination of intraoral elastics. However, as an unwanted effect asymmetric extraction might cause an asymmetrical molar relationship and an asymmetry of the arch form at the end of the treatment (9). Furthermore, intraoral elastics require full cooperation of the patient for the success of this kind of therapy (10,11). Our patient initially had a Class III molar relationship on the right side. In order to correct the midline deviation, the lower left premolar might have been extracted; however, this could cause a number of problems as listed above. Therefore, we distalized the mandibular posterior teeth on the left side, and this helped to correct both the molar relationship and the midline deviation without extraction.
This technique can be thought to negatively affect the angulation of the teeth, but no angulation problem was seen on the final panoramic radiograph, probably because of the use of the .019×.025″ SS arch wire. Class I canine and molar relations were obtained at the end of the treatment (Figure 4).
Figure 4. a–i.

Final intraoral and extraoral photographs and panoramic radiograph: final, extraoral frontal rest image (a); final, extraoral frontal smile image (b); final, extraoral profile image (c); final, intraoral frontal image (d); final, intraoral right lateral image (e); final, intraoral left lateral image (f); final, intraoral upper occlusal image (g); final, intraoral lower occlusal image (h); final, panoramic radiograph image (i)
Use of miniscrews might help to correct a severely deviated midline without the use of intermaxillary elastics that requires the patient’s cooperation. The greatest advantage of this technique is that there is no need for patient cooperation. In order to correct midline deviation, the screws might be placed either unilaterally or bilaterally, in one or both of the arches, depending on the side where the midline deviation exists (12,13). Poggio et al. (14) reported that in the mesiodistal dimension, the greatest amount of bone was found between the first and second premolars, and the least amount of bone was seen between the first premolar and the canine in the mandibula. Therefore, it may seem more appropriate to insert one of the screws between the first and second premolars; however, the interpremolar region might be risky because of the existence of mental foramen for vertically positioned miniscrews. As a result, we preferred to insert one of the miniscrews between the canine and premolar, and for the second miniscrew the buccal shelf area was selected because Chang et al. reported that a high success rate (93%) was seen for miniscrews that were inserted in the buccal shelf area (9). In this region, large-diameter screws might be inserted parallel to the long axes of the molars thanks to sufficient thickness of the bone. Adequate bone thickness allows insertion of miniscrews without interfering with tooth roots (15). This technique should be monitored for long-term stability and may require overcorrection and long-term retention, especially when the midline deviations are severe.
CONCLUSION
In order to achieve successful and stable results at the end of the treatment, correction of midline deviations requires an attentive diagnosis, a well thought out treatment plan, and case-specific selection of suitable mechanics. We think that using miniscrews for anchorage is an effective method for the correction of midline deviation. Furthermore, the biggest advantage of this technique is that patient cooperation is not required. However, long-term evaluation of the stability of results that are obtained at the end of the treatment is required.
Footnotes
Ethics Committee Approval: N/A.
Informed Consent: Written informed consent was obtained from the parents of the patient who participated in this study.
Peer-review: Externally peer-reviewed.
Author Contributions: Concept - H.C., C.D.; Design - H.C., C.D.; Supervision - H.C., B.T.; Resources - H.C., B.T.; Materials - H.C., B.T.; Data Collection and/or Processing - H.C., B.T.; Analysis and/or Interpretation - H.C., C.D.; Literature Search - H.C., B.T.; Writing Manuscript - H.C., C.D.; Critical Review - H.C., C.D.; Other - H.C., B.T.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Lewis PD. The deviated midline. Am J Orthod. 1976;70:601–16. doi: 10.1016/0002-9416(76)90223-2. https://doi.org/10.1016/0002-9416(76)90223-2. [DOI] [PubMed] [Google Scholar]
- 2.Creekmore TD, Eklund MK. The possibility of skeletal anchorage. J Clin Orthod. 1983;17:266–9. [PubMed] [Google Scholar]
- 3.Herman R, Cope J. Temporary anchorage devices in orthodontics: Mini implants. Semin Orthod. 2005;11:32–9. https://doi.org/10.1053/j.sodo.2004.11.006. [Google Scholar]
- 4.Dalstra M, Cattaneo PM, Melsen B. Load transfer of miniscrews for orthodontic anchorage. Orthodontics. 2004;1:53–62. [Google Scholar]
- 5.Kuroda S, Yamada K, Deguchi T, Hashimoto T, Kyung HM, Yamamoto TT. Root proximity is a major factor for screw failure in orthodontic anchorage. Am J Orthod Dentofacial Orthop. 2007;131:68–73. doi: 10.1016/j.ajodo.2006.06.017. https://doi.org/10.1016/j.ajodo.2006.06.017. [DOI] [PubMed] [Google Scholar]
- 6.Arnett GW, Bergman RT. Facial keys to orthodontic diagnosis and treatment planning. Part I. Am J Orthodontics Dentofacial Orthop. 1993;103:299–312. doi: 10.1016/0889-5406(93)70010-L. https://doi.org/10.1016/0889-5406(93)70010-L. [DOI] [PubMed] [Google Scholar]
- 7.Nanda R, Margolis MJ. Treatment strategies for midline discrepancies. Semin Orthod. 1996;2:84–9. doi: 10.1016/s1073-8746(96)80046-6. https://doi.org/10.1016/S1073-8746(96)80046-6. [DOI] [PubMed] [Google Scholar]
- 8.Jerrold L, Lowenstein LJ. The midline: diagnosis and treatment. Am J Orthod Dentofacial Orthop. 1990;97:453–62. doi: 10.1016/S0889-5406(05)80025-3. https://doi.org/10.1016/S0889-5406(05)80025-3. [DOI] [PubMed] [Google Scholar]
- 9.Chang C, Liu SS, Roberts WE. Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. Angle Orthod. 2015;85:905–10. doi: 10.2319/092714.695.1. https://doi.org/10.2319/092714.695.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rebellato J. Asymmetric extractions used in the treatment of patients with asymmetries. Semin Orthod. 1998;4:180–8. doi: 10.1016/s1073-8746(98)80019-4. https://doi.org/10.1016/S1073-8746(98)80019-4. [DOI] [PubMed] [Google Scholar]
- 11.Vaden J, Dale JG, Klontz HA. Tweed-Merrifield edgewise appliance: philosophy, diagnosis and treatment. In: Graber TM, Vanarsdall RL Jr, editors. Orthodontics Current principles and techniques. 3rd ed. St. Louis: Mosby; 2000. pp. 647–707. [Google Scholar]
- 12.Chung KR, Kim SH, Kook YA, Kang YG, Sinclair PM. Dental midline correction using two component C-orthodontic mini-implant. Prog Orthod. 2008;10:76–86. [PubMed] [Google Scholar]
- 13.Feng X, Yang Z, Dai J, Li R. Miniscrew anchorage for the correction of midline discrepancies. J Clin Orthod. 2014;48:169–79. [PubMed] [Google Scholar]
- 14.Poggio PM, Incorvati C, Velo S, Carano A. ‘Safe zones’: a guide for miniscrew positioning in the maxillary and mandibular arch. Angle Orthod. 2006;76:191–7. doi: 10.1043/0003-3219(2006)076[0191:SZAGFM]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 15.Lin S-Y, Chang C, Roberts EW. Simple mechanics to upright horizontally impacted molars with ramus screws. OJN. 2016;5:42–7. https://doi.org/10.3126/ojn.v5i2.15231. [Google Scholar]