

Abstract
IMPORTANCE
Clinical practice guidelines state there is insufficient evidence to support advising patients with peripheral artery disease (PAD) to participate in a home-based walking exercise program.
OBJECTIVE
To determine whether a home-based walking exercise program that uses a group-mediated cognitive behavioral intervention, incorporating both group support and self-regulatory skills, can improve functional performance compared with a health education control group in patients with PAD with and without intermittent claudication.
DESIGN, SETTING, AND PATIENTS
Randomized controlled clinical trial of 194 patients with PAD, including 72.2% without classic symptoms of intermittent claudication, performed in Chicago, Illinois between July 22, 2008, and December 14, 2012.
INTERVENTIONS
Participants were randomized to 1 of 2 parallel groups: a home-based group-mediated cognitive behavioral walking intervention or an attention control condition.
MAIN OUTCOMES AND MEASURES
The primary outcome was 6-month change in 6-minute walk performance. Secondary outcomes included 6-month change in treadmill walking, physical activity, the Walking Impairment Questionnaire (WIQ), and Physical and Mental Health Composite Scores from the 12-item Short-Form Health Survey.
RESULTS
Participants randomized to the intervention group significantly increased their 6-minute walk distance ([reported in meters] 357.4 to 399.8 vs 353.3 to 342.2 for those in the control group; mean difference, 53.5 [95% CI, 33.2 to 73.8]; P < .001), maximal treadmill walking time (intervention, 7.91 to 9.44 minutes vs control, 7.56 to 8.09; mean difference, 1.01 minutes [95% CI, 0.07 to 1.95]; P = .04), accelerometer-measured physical activity over 7 days (intervention, 778.0 to 866.1 vs control, 671.6 to 645.0; mean difference, 114.7 activity units [95% CI, 12.82 to 216.5]; P = .03), WIQ distance score (intervention, 35.3 to 47.4 vs control, 33.3 to 34.4; mean difference, 11.1 [95% CI, 3.9 to 18.1]; P = .003), and WIQ speed score (intervention, 36.1 to 47.7 vs control, 35.3–36.6; mean difference, 10.4 [95% CI, 3.4 to 17.4]; P = .004).
CONCLUSION AND RELEVANCE
A home-based walking exercise program significantly improved walking endurance, physical activity, and patient-perceived walking endurance and speed in PAD participants with and without classic claudication symptoms. These findings have implications for the large number of patients with PAD who are unable or unwilling to participate in supervised exercise programs.
TRIAL REGISTRATION
clinicaltrials.gov Identifier: NCT00693940
Few medical therapies improve the functional impairment associated with lower extremity peripheral artery disease (PAD).1–3 Supervised treadmill exercise increases maximal treadmill walking distance by 50% to 200% in individuals with PAD.4–6 However, supervised exercise is typically not covered by medical insurance and requires regular transportation to the exercise center. Thus, few patients with PAD participate in supervised treadmill exercise therapy.7
Home-based walking exercise is a promising alternative to supervised exercise. However, several clinical trials of home-based exercise in people with PAD have been small and inconclusive.8–10 Recent, larger randomized trials have yielded mixed results.11,12 Current clinical practice guidelines state that there is insufficient evidence to recommend home-based walking exercise for people with PAD.13,14 Most physicians do not recommend home-based walking exercise to patients with PAD.7,15,16
We conducted a randomized controlled clinical trial, the Group Oriented Arterial Leg Study (GOALS), to determine whether an intervention designed to increase home-based walking exercise improved walking performance at 6-month follow-up in people with PAD. GOALS used a group-mediated cognitive behavioral intervention that incorporated group support and self-regulatory skills to help participants adhere to home-based walking exercise.17 We hypothesized that the intervention group would have greater improvement in objective and subjective measures of walking performance and physical activity, compared with a health-education control group.
Methods
The institutional review board of Northwestern University approved the protocol. Participants provided written informed consent and methods have been reported.17 The study was a parallel-design randomized controlled clinical trial. Participants were randomized to 1 of 2 groups: a home-based group-mediated cognitive behavioral exercise intervention or an attention control condition. The study was performed in Chicago, Illinois between July 22, 2008, and December 14, 2012.
Participant Identification
Participants were recruited through newspaper or radio advertisements or from postcards mailed to individuals aged 65 years and older in the Chicago area. Practicing physicians at Northwestern Memorial Hospital were invited to refer potentially eligible patients with PAD. People with PAD who had previously participated in research with the principal investigator (M.M.M.) at Northwestern and expressed interest in future research participation were contacted.
Inclusion and Exclusion Criteria
The inclusion criterion was an ankle-brachial index (ABI) of 0.90 or less in either leg. Individuals with a resting ABI of 0.91 or greater to 1.00 or less at baseline were eligible if their ABI dropped by at least 20% after a heel-rise test.18 Individuals with a resting ABI greater than 0.90 were eligible if they provided medical record documentation of lower extremity revascularization or evidence of PAD from an accredited vascular laboratory.
Criteria for exclusion included potential participants with a below- or above-knee amputation; wheelchair confinement; inability to walk at least 50 feet without stopping; use of a walking aid other than a cane; inability to attend weekly sessions; walking impairment for a reason other than PAD, foot ulcer or critical limb ischemia; significant visual or hearing impairment; noncompletion of the study run-in (attendance at 2 weekly health education sessions over a 3-week period); major surgery or lower extremity revascularization during the previous 3 months or planned during the next 12 months; major medical illness including cancer treatment during the prior 12 months; current participation in another clinical trial or in another exercise trial within the past 3 months; completion of cardiac rehabilitation during the past 3 months; Parkinson disease; requirement of oxygen with activity or exercise; determination that exercise may be unsafe including having more than a class II New York Heart Association level of heart failure or angina; an increase in angina pectoris during the prior 6 months; an abnormal baseline exercise stress test; an exercise level similar to that targeted in the intervention at the time of recruitment; and having a Mini-Mental State Examination score of less than 23 at baseline.19
ABI Measurement
A handheld Doppler probe (Pocket Dop II; Nicolet Biomedical Inc) was used to obtain systolic blood pressure twice in the right and left brachial, dorsalis pedis, and posterior tibial arteries using established methods.1–3,5 The ABI was calculated by dividing the mean of the dorsalis pedis and posterior tibial pressure levels in each leg by the mean of the 4 brachial blood pressures. Systolic blood pressure levels of zero were excluded from ABI calculations. Mean blood pressure levels in the arm with the higher pressure were used when one brachial pressure was higher than the opposite brachial pressure in both measurement sets and the 2 brachial pressures differed by 10 mm Hg or more in a single measurement set.20
Participant Characteristics
Medical History
Medical history, race/ethnicity, and other demographics were obtained using patient report.5 Other measures included height and weight, which were measured at baseline. Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared.
Leg Symptoms
Leg symptoms were characterized using the San Diego claudication questionnaire.21 Intermittent claudication was defined as exertional calf pain that does not begin at rest, causes the participant to stop walking, and resolves within 10 minutes of rest.21 Participants without intermittent claudication were either asymptomatic (ie, reported no exertional leg symptoms) or had leg symptoms not meeting all criteria for intermittent claudication.21
Outcomes
All outcomes were measured before randomization and at 6-month follow-up by assessors unaware of participants’ group assignment.
Primary Outcome: the 6-Minute Walk Test
Change in 6-minute walk performance between baseline and 6-month follow-up was our primary outcome. The 6-minute walk was selected as the primary outcome measure for several reasons. First, 6-minute walk performance is more closely correlated with physical activity during daily life than treadmill walking performance in people with PAD.22 Second, in older patients, treadmill walking is associated with balance problems and greater anxiety when compared with corridor walking (ie, the 6-minute walk).23,24 Third, treadmill walking performance, but not the 6-minute walk, is associated with a learning effect.5,25 Fourth, the 6-minute walk is well validated and predicts mortality and mobility loss in people with PAD.26–28 Following a standardized protocol,1–3,5,22 participants walked up and down a 100-foot hallway for 6 minutes after instructions to cover as much distance as possible. The distance completed after 6 minutes was recorded.
Secondary Outcomes
Secondary outcomes were changes in maximal treadmill walking time, pain-free treadmill walking time, physical activity, the Walking Impairment Questionnaire (WIQ) scores, and the Physical Health Composite Score (PCS) and Mental Health Composite Score (MCS) scales from the 12-item Medical Outcomes Study Short-Form Health Survey (SF-12).
Maximal treadmill walking time and time to onset of is-chemic leg symptoms were measured using the Gardner-Skinner protocol.5,25
Physical activity was measured over 7 days using a vertical accelerometer (Caltrac, Muscle Dynamics Fitness Network Inc) according to established, validated methods.29–31 Because accelerometers were programmed using identical age, weight, and sex for each participant, the measurement yielded activity units.29–31
Walking distance, walking speed, and stair climbing were reported as 3 domains using the WIQ, a PAD-specific measure of self-reported limitations.32 Each domain is scored on a 0- to 100-point scale in which 0 represents extreme limitation and 100 represents no difficulty walking long distances, walking rapidly, or climbing 3 flights of stairs, respectively.32
The PCS and MCS were used to assess global dimensions of health-related quality of life.33
Randomization and Study Interventions
Eligible participants were randomized by computer using a randomly permuted block method, stratifying by baseline 6-minute walk performance.
Group-Mediated Cognitive Behavioral Intervention
Our intervention applied principles from social cognitive theory, the group dynamics literature, and research on self-regulation to motivate participants to adhere to home-based walking exercise.34–36 Participants met once weekly for 90 minutes in a group with other PAD participants for the entire 6 months of the intervention. Groups were led by a trained facilitator. Forty-five minutes was devoted to facilitator-led discussions and 45 minutes to walking around an indoor track. The facilitator led discussion on a different topic each week, including benefits of walking exercise for PAD, goal-setting, self-monitoring, and managing pain during exercise.17 Participants were instructed to engage in over-ground (rather than treadmill) walking exercise at least 5 days per week, working up to 50 minutes per exercise session. We emphasized over-ground walking because it is more directly relevant to walking during daily life than treadmill walking.22,23 Participants were advised to walk to severe leg discomfort (a severity of 4 or 5 on a scale of 0–5) and rest until the discomfort subsided sufficiently to resume walking. Participants without leg symptoms were asked to walk to an intensity of 12 to 14 on the Borg Rating of Perceived Exertion scale (a validated estimate of workload that correlates with heart rate and oxygen consumption).37 After each weekly session, participants completed a questionnaire listing walking goals for the coming week. Participants recorded their actual time walked on this questionnaire each day during the week. The facilitator reviewed completed questionnaires and provided brief individualized feedback each week.
Control Group
The health education control group attended weekly 60-minute group sessions with other PAD participants. Physicians and other health care professionals provided lectures on topics including managing hypertension, cancer screening, and vaccinations.
Statistical Analyses
Power calculations assumed that 100 people completing 6-month follow-up testing in each group would provide 80% power to detect a difference of 0.40 standard deviations of the pooled 6-month change in 6-minute walk distance between the exercise and control groups. This difference corresponded with 21.6 m in the 6-minute walk in a prior study of supervised exercise in PAD participants. It represents a small meaningful difference in the 6-minute walk test.5,38
One-way analyses of variance and χ2 tests were used to compare categorical and continuous characteristics of participants across the 2 groups at baseline, respectively. Two-sample, 2-sided t tests were used to compare changes in outcomes between baseline and 6-month follow-up between the intervention and the control groups without adjustment for baseline data. A priori, the P value considered statistically significant was a P value of less than .05. Intention-to-treat analyses were performed.
All participants were asked to return for follow-up measurements, regardless of their adherence to their assigned group. Decedents were excluded from analyses. Several sensitivity analyses were performed. First, multivariate linear regression models were performed to adjust for potential imbalances in baseline characteristics between the 2 groups. Additionally, a recently developed method was used that adjusts for all relevant baseline characteristics.39 Second, multiple imputation was used to account for missing data at 6-month follow-up40 including additional analyses in which a value of zero was assigned for missing 6-month follow-up data for decedents.
In post hoc analyses, the effect of the intervention on change in 6-minute walk was evaluated in subsets of participants defined by age (greater than vs less than median), sex, race/ethnicity (African American vs non–African American), baseline 6-minute walk performance (greater than vs less than median), PAD severity (ABI ≤0.50 vs ABI >0.50), presence vs absence of diabetes mellitus, and presence vs absence of classic claudication symptoms. Logistic regression and χ2 analyses were used to compare differences in rates of small (20 m) and large (50 m) meaningful improvements in the 6-minute walk between the intervention and control groups.38 Analyses were performed using SAS statistical software version 9.2.
Results
Of 1322 participants with a scheduled baseline visit, 194 met eligibility criteria and were randomized (Figure 1). Twelve participants were eligible because they had a resting ABI of 0.91 to 0.99 with a 20% ABI drop after the heel-rise test. Of 3 additional participants with an ABI of 0.91 or greater, 2 had prior lower extremity revascularization and 1 had evidence of PAD in an accredited vascular laboratory. Overall, 27.8% of participants had classic intermittent claudication symptoms.
Figure 1.
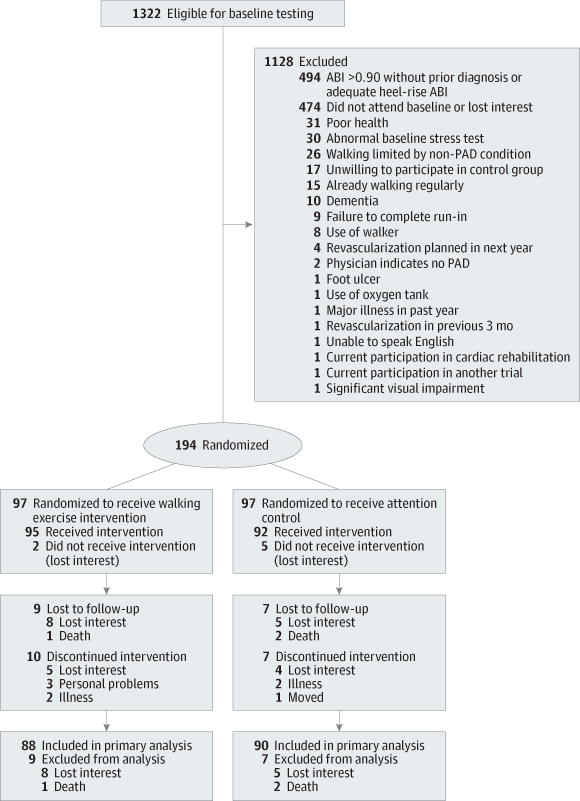
Study Participation and Follow-up for the Group-Oriented Arterial Leg Study (GOALS)
Participants randomized to the intervention group had higher physical activity levels at baseline compared with participants randomized to the control group (Table 1). There were no other significant baseline differences between the 2 groups (Table 1).
Table 1.
Characteristics of Peripheral Artery Disease Participants Randomized to Home-Based Exercise vs Attention Control
| Baseline Measures | No. (%) | |
|---|---|---|
| Home-Based Exercise Group (n = 97) | Attention Control Group (n = 97) | |
| Age, mean (SD), y | 69.3 (9.5) | 71.0 (9.6) |
| Men | 49 (50.5) | 48 (49.5) |
| White | 42 (43.3) | 51 (52.6) |
| African American | 53 (54.6) | 43 (44.3) |
| Ankle-brachial index, mean (SD) | 0.67 (0.16) | 0.67 (0.18) |
| BMI, mean (SD)a | 29.1 (7.0) | 29.0 (6.5) |
| Current smoker | 26 (26.8) | 22 (22.7) |
| Angina | 15 (15.5) | 15 (15.6) |
| Antiplatelet medication | 45 (46.4) | 46 (47.4) |
| Cancer | 16 (16.5) | 15 (15.6) |
| Continuance of walking even with pain | 8 (8.3) | 6 (6.2) |
| Diabetes mellitus | 28 (28.9) | 36 (37.1) |
| Disc disease | 21 (21.7) | 25 (26.0) |
| Heart failure | 10 (10.3) | 12 (12.4) |
| Hip arthritis | 13 (13.4) | 18 (18.6) |
| History of myocardial infarction | 13 (13.4) | 14 (14.4) |
| Intermittent claudication | 31 (32.0) | 23 (23.7) |
| Knee arthritis | 34 (35.1) | 22 (22.9) |
| No pain when walking | 8 (8.3) | 8 (8.3) |
| Other atypical leg pain | 24 (24.7) | 29 (29.9) |
| Pain when walking and when at rest | 26 (26.8) | 31 (32.0) |
| Pulmonary disease | 13 (13.4) | 13 (13.4) |
| Spinal stenosis | 12 (12.4) | 8 (8.3) |
| Stroke | 9 (9.3) | 15 (15.5) |
| Using ACE inhibitors or ARBs | 31 (32.0) | 29 (29.9) |
| Using cilostazol | 3 (3.1) | 10 (10.3) |
| Using statin medications | 42 (43.3) | 48 (49.5) |
| Outcome measures, mean (SD) | ||
| 6-Minute walk distance, m | 354.6 (98.4) | 352.2 (91.8) |
| Maximalt readmill walking time, min | 7.9 (4.7) | 7.4 (4.6) |
| Treadmill time to onset of leg symptoms, min | 2.9 (2.1) | 3.3 (3.0) |
| 7-Day physical activity level, activity units | 783 (402.0) | 656 (332.0) |
| WIQ distance scoreb | 34.1 (27.2) | 32.4 (26.0) |
| WIQspeed scoreb | 35.1 (23.7) | 33.8 (22.7) |
| WIQ stair-climbing scoreb | 48.4 (25.9) | 46.5 (25.4) |
| PCSc | 40.6 (6.2) | 40.0 (5.3) |
| MCSc | 39.2 (5.9) | 38.6 (6.0) |
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin II receptor blocker; BMI, body mass index; MCS, Mental Composite Score; PCS, Physical Composite Score; SF-12, Medical Outcomes Study Short-Form Health Survey; WIQ, Walking Impairment Questionnaire.
BMI is calculated as weight in kilograms divided by height in meters squared.
The WIQ is scored on a 0- to 100-point scale in which 0 indicates extreme difficulty and 100 indicates no difficulty with the walking distance, walking speed, and stair-climbing elements.
PCS and MCS are both from the SF-12, which is used to assess global dimensions of health-related quality of life. The SF-12 is scored on a 0- to 100-point scale in which 0 indicates the most severe limitation and 100 indicates no limitation.
Median attendance was 84% in the home-based exercise intervention group and 81% in the control group. During months 1, 3, and 6 of the intervention, participants walked a mean of 153, 193, and 212 minutes per week, respectively. Follow-up rates were 90.7% and 92.8% in the intervention and control groups. After excluding 3 participants who died before follow-up testing, follow-up rates were 91.7% and 94.7%.
Primary Outcome
At 6-month follow-up, participants in the intervention group improved their 6-minute walking distance compared with the control group ([reported in meters] 357.4 to 399.8 vs 353.3 to 342.2 for those in the control group; mean difference, 53.5 [95% CI, 33.2 to 73.8]; P < .001; Table 2). These results were not substantially changed when analyses were repeated, adjusting for baseline physical activity and other baseline characteristics (45.7 m; 95% CI, 24.6 to 66.7; P < .001).
Table 2.
6-Month Change in Study Outcomes in the GOALS Trial
| Outcome Measures | No. | Mean (SD) | Change (95% CI) | P Value | ||
|---|---|---|---|---|---|---|
| Baseline | 6-Month Change | Within-Group Change | With-Control Comparison | |||
| Primary outcome | ||||||
| 6-min walk distance, meter | ||||||
| Control | 90 | 353.3 (91.9) | 342.2 (110.8) | −11.4 (−25.4 to 3.2) | 0 [Reference] | <.001 |
| Intervention | 88 | 357.4 (97.6) | 399.8 (101.6) | 42.4 (27.9 to 56.8) | 53.5 (33.2 to 73.8) | |
| Secondary outcomes | ||||||
| Total treadmill walk time, min | ||||||
| Control | 87 | 7.56 (4.69) | 8.09 (5.14) | 0.53 (−0.14 to 1.19) | 0 [Reference] | .04 |
| Intervention | 86 | 7.91 (4.72) | 9.44 (5.95) | 1.54 (0.87 to 2.20) | 1.01 (0.07 to 1.95) | |
| Pain-free treadmill walking time, min | ||||||
| Control | 68 | 3.12 (2.79) | 3.54 (2.76) | 0.42 (−0.18 to 1.02) | 0 [Reference] | .02 |
| Intervention | 77 | 2.72 (1.89) | 4.15 (3.06) | 1.43 (0.87 to 2.00) | 1.02 (0.19 to 1.84) | |
| Change in physical activity measured over 7 d, activity units | ||||||
| Control | 88 | 671.6 (337.6) | 645.0 (333.5) | −26.6 (−98.4 to 45.2) | 0 [Reference] | .03 |
| Intervention | 87 | 778.0 (410.7) | 866.1 (405.4) | 88.1 (15.9 to 160.3) | 114.7 (12.8 to 216.5) | |
| WIQdistance scorea | ||||||
| Control | 88 | 33.3 (25.5) | 34.4 (27.2) | 1.1 (−3.9 to 6.2) | 0 [Reference] | .003 |
| Intervention | 88 | 35.3 (27.6) | 47.4 (29.7) | 12.1 (7.1 to 17.1) | 11.1 (3.9 to 18.1) | |
| WIQspeed scorea | ||||||
| Control | 90 | 35.3 (22.8) | 36.6 (24.6) | 1.1 (−3.4 to 5.6) | 0 [Reference] | .004 |
| Intervention | 88 | 36.1 (23.8) | 47.7 (26.0) | 11.7 (6.7 to 16.6) | 10.4 (3.4 to 17.4) | |
| WIQstair-climbing scorea | ||||||
| Control | 90 | 47.9 (25.6) | 48.5 (27.8) | 0.60 (−4.9 to 6.1) | 0 [Reference] | .05 |
| Intervention | 88 | 48.9 (26.0) | 57.3 (24.5) | 8.5 (2.9 to 14.0) | 7.9 (0 to 15.8) | |
| PCSb | ||||||
| Control | 90 | 40.1 (5.1) | 39.7 (5.5) | −0.3 (−1.7 to 1.0) | 0 [Reference] | .38 |
| Intervention | 88 | 40.5 (6.3) | 41.0 (5.9) | 0.63 (−0.5 to 1.7) | 0.83 (−1.0 to 2.7) | |
| MCSb | ||||||
| Control | 90 | 38.2 (5.7) | 38.8 (6.0) | 0.6 (−0.8 to 2.0) | 0 [Reference] | .72 |
| Intervention | 88 | 39.4 (5.9) | 39.6 (5.7) | 0.2 (−1.2 to 1.6) | −0.36 (−2.3 to 1.6) | |
Abbreviations: GOALS, Group Oriented Arterial Leg Study; MCS, Mental Composite Score; PCS, Physical Composite Score; SF-12, Medical Outcomes Study Short-Form Health Survey; WIQ, Walking Impairment Questionnaire.
The WIQ is scored on a 0- to 100-point scale in which 0 indicates extreme difficulty and 100 indicates no difficulty with the walking distance, walking speed, and stair-climbing elements.
PCS and MCS are both from the SF-12, which is used to assess global dimensions of health-related quality of life. The SF-12 is scored on a 0- to 100-point scale in which 0 indicates the most severe limitation and 100 indicates no limitation.
Secondary Outcomes
At 6-month follow-up, participants in the intervention group significantly improved their maximal treadmill walking time compared with the control group (7.91 to 9.44 minutes vs 7.56 to 8.09 minutes; mean difference, 1.01 minutes [95% CI, 0.07 to 1.95]; P = .04). Participants in the intervention group improved their pain-free walking time compared with the control group (2.72 to 4.15 minutes vs 3.12 to 3.54 minutes; mean difference, 1.02 minutes [95% CI, 0.19 to 1.84]; P = .02). Participants in the intervention group increased their physical activity compared with the control group (778.0 to 866.1 activity units vs 671.6 to 645.0 activity units; mean difference, 114.7 activity units [95% CI, 12.8 to 216.5]; P = .03). Participants in the intervention group, when compared with those in the control group, improved their WIQ distance score (35.3 to 47.4 vs 33.3 to 34.4; mean difference, 11.1 [95% CI, 3.9 to 18.1]; P = .003) and their WIQ speed score (36.1 to 47.7 vs 35.3 to 36.6; mean difference, 10.4 [95% CI, 3.4 to 17.4]; P = .004) but not their WIQ stair-climbing score (48.9 to 57.3 vs 47.9 to 48.5; mean difference, 7.9 [95% CI, 0.00 to 15.8]; P = .05). There were no between-group differences in change in the SF-12 PCS or MCS subscales (Table 2). Results were not meaningfully changed when analyses were repeated, adjusting for baseline differences in physical activity and other characteristics between the intervention and control groups.
In sensitivity analyses, missing data were imputed for participants who dropped out and were set to zero for participants who died before follow-up testing. In these analyses, results for change in treadmill walking performance were no longer statistically significant (mean difference for maximal treadmill walking time was 0.93 minutes [95% CI, −0.04 to 1.89]; P = .06) and mean difference for pain-free treadmill walking time was 0.86 minutes (95% CI, −0.07 to 1.78; P = .07). Results for remaining primary and secondary outcomes were not substantially changed.
Participants randomized to the intervention group were more likely to achieve a small meaningful improvement in the 6-minute walk (59.1% vs 31.1%; odds ratio [OR], 3.20 [95% CI, 1.73 to 5.92]; P < .001) and a large meaningful improvement in the 6-minute walk (44.3% vs 11.1%; OR, 6.37 [95% CI, 2.92 to 13.89]; P < .001), compared with the control group.
Subgroup Analyses
Significant improvement in the 6-minute walk was observed for participants randomized to the intervention compared with the control group within each defined subgroup except among participants with intermittent claudication (Figure 2).
Figure 2.
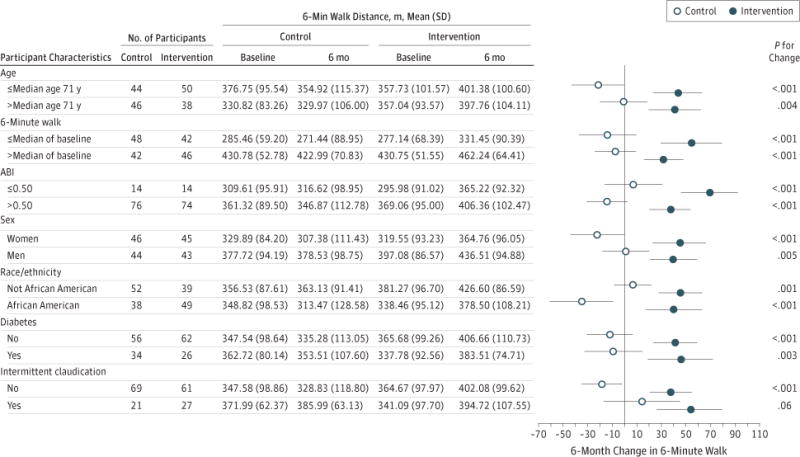
Association Between Home-Based Walking Exercise Intervention and Change in 6-Minute Walk at 6-Month Follow-up Within Subsets of GOALS Participants.
Change in 6-minute walk is shown for specific subsets of participants within the Group-Oriented Arterial Leg Study (GOALS) according to whether they were randomized to the intervention vs control group. P values represent the change in 6-minute walk between the intervention vs control group for each study characteristic. Error bars indicate 95% CIs.
Serious Adverse Events
One participant randomized to the home-based exercise intervention developed dyspnea on exertion during exercise. Subsequent work-up revealed coronary atherosclerosis requiring coronary artery bypass grafting. This participant completed the study. One death occurred due to cancer in the intervention group and 2 deaths occurred in the control group due to hypertensive cardiovascular disease and cardiovascular disease combined with pneumonia, respectively. Deaths were determined unrelated to study participation.
Discussion
In this randomized controlled trial of 194 participants with PAD, 6 months of a home-based group-mediated cognitive behavioral exercise intervention significantly improved the 6-minute walk performance by 53.5 meters when compared with a control group. A 50-meter improvement in the 6-minute walk is consistent with a large meaningful change in the 6-minute walk based on prior study.38 Participants in the intervention group were significantly more likely to achieve a large meaningful improvement in the 6-minute walk than the control group. The intervention also improved treadmill walking performance, WIQ distance and speed scores, and physical activity levels when compared with the control group. The home-based walking exercise program did not require physician supervision and was safe for patients with PAD meeting inclusion criteria including passing a baseline exercise stress test.
The functional limitations experienced by patients with PAD are associated with poor quality of life, high hospitalization rates, increased mortality, and high medical care costs.41–43 However, only 2 medications are US Food and Drug Administration approved for treating intermittent claudication. Of these, pentoxifylline is not better than placebo and cilostazol is associated with an approximate 25% improvement in walking performance.44 Supervised treadmill exercise is associated with a 50% to 200% improvement in maximal treadmill walking performance in PAD.4–6 However, most patients with PAD do not participate in supervised exercise. Medical insurance typically does not pay for supervised exercise for patients with PAD and traveling to exercise sessions is burdensome. Home-based exercise could provide a feasible therapeutic option that is accessible to most patients with PAD.
PAD clinical practice guidelines, published in 2006 and updated in 2011,13,45 concluded that there is insufficient evidence to recommend home-based walking exercise for PAD. Two recent randomized trials of home-based exercise in PAD showed conflicting results.11,12 Collins et al11 randomized 145 participants with PAD and diabetes to a home-based exercise program vs a control group. The intervention consisted of a 1-hour instruction session at baseline and 2 exercise sessions that included feedback on walking exercise and group interaction. Participants were subsequently encouraged to attend 1 group exercise session per week and to walk for exercise at home at least 3 times weekly using pedometers to self-monitor. Participants also received biweekly telephone calls. After 6 months, the intervention and control groups did not differ in change in maximum treadmill walking distance. Gardner et al12 randomized 119 participants with PAD and intermittent claudication to home-based walking exercise, supervised treadmill exercise, or a control group. Participants in the home-based intervention were instructed to walk 3 times weekly for 45 minutes per session, were provided with a motion sensor to track their progress, and met with an investigator every 2 weeks to receive feedback. At 12-week follow-up, participants in the home-based intervention group increased their maximal treadmill walking time by 31%. Those in the supervised treadmill exercise intervention increased their maximal treadmill walking time by 66%. Each exercise group significantly increased their treadmill walking time when compared with the control group. However, loss to follow-up was 25% and study duration was only 12 weeks. To our knowledge, GOALS is the only randomized trial of a 6-month home-based exercise that included PAD participants with and without intermittent claudication, with and without diabetes mellitus, and included the 6-minute walk as an outcome. Selection of the 6-minute walk as a primary outcome is important because 6-minute walk performance more closely approximates physical activity levels in daily life than treadmill walking performance and predicts mortality and mobility loss in patients with PAD.22,23,26–28 Clinically meaningful change has been defined for the 6-minute walk38 but not for treadmill walking performance. Additional study is needed to determine why the home-based intervention by Collins et al11 was not successful, while the GOALS trial and the study by Gardner et al12 demonstrated significant benefit.
The GOALS trial has limitations. First, results are only generalizable to patients with PAD meeting our inclusion criteria. Second, the GOALS trial was not designed to determine whether the gains in the home-based exercise program are comparable to those achievable in a supervised treadmill exercise intervention. Third, the attention control condition sessions were 60 minutes, compared with 90 minutes for the intervention condition.
In summary, a home-based exercise intervention with a group-mediated cognitive behavioral intervention component improved walking performance and physical activity in patients with PAD, including individuals with and without intermittent claudication. Based on these findings, clinical practice guidelines should advise clinicians to recommend home-based walking programs with a weekly group-mediated cognitive behavioral intervention component for patients with PAD who do not have access to supervised exercise.
Acknowledgments
Funding/Support
Supported by R01-HL088589 and RO1-HL107510 from the National Heart, Lung, and Blood Institute. Supported in part by the Intramural Research Program, National Institutes on Aging (NIA), National Institutes of Health. No other funding was used to carry out the study or complete the manuscript.
Role of the Sponsor
The funding agencies played no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation of the manuscript; and decision to submit the manuscript for publication.
Footnotes
Author Contributions
Dr McDermott (principal investigator) had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Liu, Guralnik, Spring, Rejeski, McDermott.
Acquisition of data: Domanchuk, Ferrucci, Lloyd-Jones, McDermott.
Analysis and interpretation of data: Liu, Guralnik, Criqui, Spring, Tian, Ferrucci, Lloyd-Jones, Kibbe, Tao, Zhao, Liao, McDermott.
Drafting of the manuscript: Rejeski, McDermott.
Critical revision of the manuscript for important intellectual content: Liu, Guralnik, Criqui, Spring, Tian, Domanchuk, Ferrucci, Lloyd-Jones, Kibbe, Tao, Zhao, Liao, Rejeski, McDermott.
Statistical analysis: Liu, Guralnik, Spring, Tian, Kibbe, Tao, Liao, McDermott.
Obtained funding: Guralnik, Criqui, Rejeski, McDermott.
Administrative, technical, or material support: Domanchuk, Kibbe, McDermott.
Study supervision: Spring, Domanchuk, Ferrucci, Zhao, Rejeski, McDermott.
Conflict of Interest Disclosures
All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr McDermott reports being a medical editor for the Foundation for Informed Medical Decision Making, consulting for Ironwood Pharmaceuticals, and receipt of travel expenses from the American Heart Association as an SACC member. Dr Spring reports board membership with Actigraph. No other disclosures were reported.
Disclaimer
Dr McDermott, an Associate Editor for JAMA, was not involved in the evaluation of or decision to publish this article.
Contributor Information
Mary M. McDermott, Northwestern University Feinberg School of Medicine Department of Medicine, Chicago, Illinois; Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
Kiang Liu, Northwestern University Feinberg School of Medicine Department of Medicine, Chicago, Illinois; Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
Jack M. Guralnik, University of Maryland Department of Epidemiology, Baltimore.
Michael H. Criqui, University of California at San Diego.
Bonnie Spring, Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
Lu Tian, Stanford University Department of Health Research and Policy, Stanford, California.
Kathryn Domanchuk, Northwestern University Feinberg School of Medicine Department of Medicine, Chicago, Illinois.
Luigi Ferrucci, National Institute on Aging Division of Intramural Research, Baltimore, Maryland.
Donald Lloyd-Jones, Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
Melina Kibbe, Northwestern University Department of Surgery, Chicago, Illinois.
Huimin Tao, Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
Lihui Zhao, Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
Yihua Liao, Northwestern University Feinberg School of Medicine, Department of Preventive Medicine, Chicago, Illinois.
W. Jack Rejeski, Wake Forest University, Departments of Health and Exercise Science and Geriatric Medicine, Winston-Salem, North Carolina.
References
- 1.McDermott MM, Greenland P, Liu K, et al. Leg symptoms in peripheral arterial disease: associated clinical characteristics and functional impairment. JAMA. 2001;286(13):1599–1606. doi: 10.1001/jama.286.13.1599. [DOI] [PubMed] [Google Scholar]
- 2.McDermott MM, Liu K, Greenland P, et al. Functional decline in peripheral arterial disease: associations with the ankle brachial index and leg symptoms. JAMA. 2004;292(4):453–461. doi: 10.1001/jama.292.4.453. [DOI] [PubMed] [Google Scholar]
- 3.McDermott MM, Greenland P, Liu K, et al. The ankle brachial index is associated with leg function and physical activity: the Walking and Leg Circulation Study. Ann Intern Med. 2002;136(12):873–883. doi: 10.7326/0003-4819-136-12-200206180-00008. [DOI] [PubMed] [Google Scholar]
- 4.Fakhry F, van de Luijtgaarden KM, Bax L, et al. Supervised walking therapy in patients with intermittent claudication. J Vasc Surg. 2012;56(4):1132–1142. doi: 10.1016/j.jvs.2012.04.046. [DOI] [PubMed] [Google Scholar]
- 5.McDermott MM, Ades P, Guralnik JM, et al. Treadmill exercise and resistance training in patients with peripheral arterial disease with and without intermittent claudication: a randomized controlled trial. JAMA. 2009;301(2):165–174. doi: 10.1001/jama.2008.962. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Watson L, Ellis B, Leng GC. Exercise for intermittent claudication. Cochrane Database Syst Rev. 2008;4:CD000990. doi: 10.1002/14651858.CD000990.pub2. [DOI] [PubMed] [Google Scholar]
- 7.Regensteiner JG. Exercise rehabilitation for the patient with intermittent claudication: a highly effective yet underutilized treatment. Curr Drug Targets Cardiovasc Haematol Disord. 2004;4(3):233–239. doi: 10.2174/1568006043336195. [DOI] [PubMed] [Google Scholar]
- 8.Regensteiner JG, Meyer TJ, Krupski WC, Cranford LS, Hiatt WR. Hospital vs home-based exercise rehabilitation for patients with peripheral arterial occlusive disease. Angiology. 1997;48(4):291–300. doi: 10.1177/000331979704800402. [DOI] [PubMed] [Google Scholar]
- 9.Savage P, Ricci MA, Lynn M, et al. Effects of home versus supervised exercise for patients with intermittent claudication. J Cardiopulm Rehabil. 2001;21(3):152–157. doi: 10.1097/00008483-200105000-00006. [DOI] [PubMed] [Google Scholar]
- 10.Menard JR, Smith HE, Riebe D, Braun CM, Blissmer B, Patterson RB. Long-term results of peripheral arterial disease rehabilitation. J Vasc Surg. 2004;39(6):1186–1192. doi: 10.1016/j.jvs.2004.01.034. [DOI] [PubMed] [Google Scholar]
- 11.Collins TC, Lunos S, Carlson T, et al. Effects of a home-based walking intervention on mobility and quality of life in people with diabetes and peripheral arterial disease: a randomized controlled trial. Diabetes Care. 2011;34(10):2174–2179. doi: 10.2337/dc10-2399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gardner AW, Parker DE, Montgomery PS, Scott KJ, Blevins SM. Efficacy of quantified home-based exercise and supervised exercise in patients with intermittent claudication: a randomized controlled trial. Circulation. 2011;123(5):491–498. doi: 10.1161/CIRCULATIONAHA.110.963066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hirsch AT, Haskal ZJ, Hertzer NR, et al. ACC/AHA 2005 Practice Guidelines for the management of patients with arterial disease (lower extremity, renal, mesenteric, and abdominal aortic) Circulation. 2006;113(11):e463–e654. doi: 10.1161/CIRCULATIONAHA.106.174526. [DOI] [PubMed] [Google Scholar]
- 14.Dormandy JA, Rutherford RB. Management of peripheral arterial disease (PAD): TASC Working Group: TransAtlantic Inter-Society Consensus (TASC) J Vasc Surg. 2000;31(1 pt 2):S1–S296. [PubMed] [Google Scholar]
- 15.Hirsch AT, Halverson SL, Treat-Jacobson D, et al. The Minnesota Regional Peripheral Arterial Disease Screening Program: toward a definition of community standards of care. Vasc Med. 2001;6(2):87–96. doi: 10.1177/1358836X0100600204. [DOI] [PubMed] [Google Scholar]
- 16.McDermott MM, Hahn EA, Greenland P, et al. Atherosclerotic risk factor reduction in peripheral arterial diseasea: results of a national physician survey. J Gen Intern Med. 2002;17(12):895–904. doi: 10.1046/j.1525-1497.2002.20307.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McDermott MM, Domanchuk K, Liu K, et al. The Group Oriented Arterial Leg Circulation Study to improve walking performance in peripheral arterial disease. Contemp Clin Trials. 2012;33:1311–1320. doi: 10.1016/j.cct.2012.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Amirhamzeh MM, Chant HJ, Rees JL, Hands LJ, Powell RJ, Campbell WB. A comparative study of treadmill tests and heel raising exercise for peripheral arterial disease. Eur J Vasc Endovasc Surg. 1997;13(3):301–305. doi: 10.1016/s1078-5884(97)80102-5. [DOI] [PubMed] [Google Scholar]
- 19.Heun R, Papassotiropoulos A, Jennssen F. The validity of psychometric instruments for detection of dementia in the elderly general population. Int J Geriatr Psychiatry. 1998;13(6):368–380. doi: 10.1002/(sici)1099-1166(199806)13:6<368::aid-gps775>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 20.Shadman R, Criqui MH, Bundens WP, et al. Subclavian artery stenosis: prevalence, risk factors, and association with cardiovascular diseases. J Am Coll Cardiol. 2004;44(3):618–623. doi: 10.1016/j.jacc.2004.04.044. [DOI] [PubMed] [Google Scholar]
- 21.Criqui MH, Denenberg JO, Bird CE, Fronek A, Klauber MR, Langer RD. The correlation between symptoms and non-invasive test results in patients referred for peripheral arterial disease testing. Vasc Med. 1996;1(1):65–71. doi: 10.1177/1358863X9600100112. [DOI] [PubMed] [Google Scholar]
- 22.McDermott MM, Ades PA, Dyer A, Guralnik JM, Kibbe M, Criqui MH. Corridor-based functional performance measures correlate better with physical activity during daily life than treadmill measures in persons with peripheral arterial disease. J Vasc Surg. 2008;48(5):1231–1237; e1. doi: 10.1016/j.jvs.2008.06.050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Greig C, Butler F, Skelton D, Mahmud S, Young A. Treadmill walking in old age may not reproduce the real life situation. J Am Geriatr Soc. 1993;41(1):15–18. doi: 10.1111/j.1532-5415.1993.tb05941.x. [DOI] [PubMed] [Google Scholar]
- 24.Swerts PMJ, Mostert R, Wouters EFM. Comparison of corridor and treadmill walking in patients with severe chronic obstructive pulmonary disease. Phys Ther. 1990;70(7):439–442. doi: 10.1093/ptj/70.7.439. [DOI] [PubMed] [Google Scholar]
- 25.Gardner AW, Skinner JS, Cantwell BW, Smith LK. Progressive vs single-stage treadmill tests for evaluation of claudication. Med Sci Sports Exerc. 1991;23(4):402–408. [PubMed] [Google Scholar]
- 26.McDermott MM, Guralnik JM, Tian L, et al. Baseline functional performance predicts the rate of mobility loss in persons with peripheral arterial disease. J Am Coll Cardiol. 2007;50(10):974–982. doi: 10.1016/j.jacc.2007.05.030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.McDermott MM, Tian L, Liu K, et al. Prognostic value of functional performance for mortality in patients with peripheral artery disease. J Am Coll Cardiol. 2008;51(15):1482–1489. doi: 10.1016/j.jacc.2007.12.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.McDermott MM, Tian L, Liu K, et al. Prognostic value of functional performance for mortality in patients with peripheral artery disease. J Am Coll Cardiol. 2008;51(15):1482–1489. doi: 10.1016/j.jacc.2007.12.034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Richardson MT, Leon AS, Jacobs DR, Jr, Ainsworth BE, Serfass R. Ability of the Caltrac accelerometer to assess daily physical activity levels. J Cardiopulm Rehabil. 1995;15(2):107–113. doi: 10.1097/00008483-199503000-00003. [DOI] [PubMed] [Google Scholar]
- 30.McDermott MM, Ohlmiller SM, Liu K, et al. Gait alterations associated with walking impairment in people with peripheral arterial disease with and without intermittent claudication. J Am Geriatr Soc. 2001;49(6):747–754. doi: 10.1046/j.1532-5415.2001.49151.x. [DOI] [PubMed] [Google Scholar]
- 31.Garg PK, Liu K, Tian L, et al. Physical activity during daily life and functional decline in peripheral arterial disease. Circulation. 2009;119(2):251–260. doi: 10.1161/CIRCULATIONAHA.108.791491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Regensteiner JG, Steiner JF, Panzer RJ, et al. Evaluation of walking impairment by questionnaire in patients with peripheral arterial disease. J Vasc Med Biol. 1990;2:142–152. [Google Scholar]
- 33.Ware J, Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- 34.Bandura A. Health promotion from the perspective of social cognitive theory. Psychol Health. 1998;13:623–650. doi: 10.1080/08870449808407422. [DOI] [Google Scholar]
- 35.Cartwright DC. Group Dynamics: Research and Theory. New York, NY: Harper and Row; 1953. [Google Scholar]
- 36.Baumeister RF, Heatherton TF, Tice DM. Losing Control: How and Why People Fail at Self-Regulation. San Diego, CA: Academic Press; 1994. [Google Scholar]
- 37.Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc. 1982;14(5):377–381. [PubMed] [Google Scholar]
- 38.Perera S, Mody SH, Woodman RC, Studenski SA. Meaningful change and responsiveness in common physical performance measures in older adults. J Am Geriatr Soc. 2006;54(5):743–749. doi: 10.1111/j.1532-5415.2006.00701.x. [DOI] [PubMed] [Google Scholar]
- 39.Tian L, Cai T, Zhao L, Wei LJ. On the covariate-adjusted estimation for an overall treatment difference with data from a randomized comparative clinical trial. Biostatistics. 2012;13(2):256–273. doi: 10.1093/biostatistics/kxr050. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York, NY: Wiley; 1987. [Google Scholar]
- 41.Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–M94. doi: 10.1093/geronj/49.2.m85. [DOI] [PubMed] [Google Scholar]
- 42.Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332(9):556–561. doi: 10.1056/NEJM199503023320902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.McDermott MM, Liu K, Ferrucci L, et al. Decline in functional performance predicts later increased mobility loss and mortality in peripheral artery disease. J Am Coll Cardiol. 2011;57(8):962–970. doi: 10.1016/j.jacc.2010.09.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Stevens JW, Simpson E, Harnan S, et al. Systematic review of the efficacy of cilostazol, naftidrofuryl oxalate and pentoxifylline for the treatment of intermittent claudication. Br J Surg. 2012;99(12):1630–1638. doi: 10.1002/bjs.8895. [DOI] [PubMed] [Google Scholar]
- 45.2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline) J Am Coll Cardiol. 2011;58(19):2020–2045. doi: 10.1016/j.jacc.2011.08.023. [DOI] [PMC free article] [PubMed] [Google Scholar]