

ABSTRACT
Because infants are born with small amounts of stored intrathyroidal iodine, they depend on human-milk iodine for normal physical and neurologic growth and development. The mammary gland concentrates iodide; however, there is a lack of consensus on the concentrations of breast-milk iodine necessary to achieve equilibrium in the infant. The objectives of the present review are to consider trends in breast-milk iodine concentrations over the course of lactation, to determine which maternal factors or interventions influence breast-milk iodine concentrations, to examine the association between breast-milk iodine concentrations and infant iodine status, and to identify how newer data contribute to the literature and inform recommendations for achieving optimal breast-milk iodine concentrations. A systematic search of the published literature was undertaken by using the US National Library of Medicine's MEDLINE/PubMed bibliographic search engine. Observational and intervention studies were included if the research was original, the study had not been included in a previous review, and iodine concentration in human milk was measured at ≥1 time point during the first 12 mo of lactation. Results of the systematic review indicate that breast-milk iodine concentrations vary widely between populations but are highest in colostrum and decrease gradually throughout the lactation period. Included studies did not replicate earlier findings of an inverse correlation between breast-milk iodine and perchlorate concentrations. Supplementation with high-dose or daily iodine during lactation was effective in increasing breast-milk iodine concentrations with some evidence of a dose-response relationship, which is consistent with findings of earlier supplementation trials in pregnancy and lactation. Although additional and globally representative research is needed, data suggest that breast-milk iodine concentrations in the range of 150 μg/L during the first 6 mo of lactation would achieve or exceed infant iodine equilibrium and prevent the developmental consequences of iodine deficiency.
Keywords: human milk, lactation, iodine, perchlorate, deficiency, neurologic consequences, developmental consequences
Introduction
Iodine deficiency early in life can irreversibly impair neurodevelopment and increase infant mortality (1). Iodine is needed for the production of thyroid hormone, which is essential for normal physical and neurologic growth and maturation in the first 2 y of life (2–4). Compared with other age groups, infants are more sensitive to iodine deficiency because they have the highest iodine requirements relative to body weight and only small amounts of stored intrathyroidal iodine (∼100 μg in a full-term neonate under conditions of iodine sufficiency) (1, 5). Infant sensitivity is corroborated by a response of thyroid-stimulating hormone and thyroxine concentrations to degrees of iodine deficiency that do not affect thyroid function in the general population (6).
Breastfed infants depend on breast-milk iodine to meet their physiologic needs. It has been speculated that full-term infants need 15 μg ⋅ kg−1 ⋅ d−1 to maintain positive iodine balance (7, 8). Iodide transport and uptake by the mammary gland are mediated by the sodium-iodide symporter (NIS), the expression of which increases during lactation (9). The mammary gland concentrates iodide so that the concentration of iodine in human milk is 20–50 times that of plasma (3). Increased uptake of iodine by the mammary gland compensates for inadequate maternal iodine status at the expense of maternal iodine reserves (10).
Several reviews on iodine concentrations in human milk have been published previously (3, 11, 12). These reviews provided comprehensive summaries of breast-milk iodine concentration (BMIC) in studies published since the 1920s, in lactating women in Europe, Asia, Africa, and North America both before and after the establishment of national salt iodization programs. Given the importance of iodine in early development and evidence of continued maternal and infant inadequacy in the presence of salt iodization, a number of newer studies have measured BMIC. The objectives of the present review were to consider trends in BMIC over the course of lactation, to determine which maternal factors or interventions influence BMIC, to examine the association between BMIC and infant iodine status, and to identify how newer data contribute to the literature and inform recommendations for achieving optimal BMIC.
Methods
A systematic search of the published literature from 1 January 2007 to 15 November 2015 was undertaken by using the US National Library of Medicine's MEDLINE/PubMed (https://www.ncbi.nlm.nih.gov/pubmed/) bibliographic search engine. The date limits were chosen to identify original research articles that were not included in the latest review of iodine nutrition in breastfeeding, which was accepted for publication in 2008 (3). Multiple PubMed searches were conducted by using various combinations of Medical Subject Heading (MeSH) and title/abstract keywords. MeSH keywords included “Milk, Human,” “Lactation,” “Breast Feeding,” and “Colostrum” as well as “iodine.” Title/abstract keywords included “lactation,” “breastfeeding,” “breast feeding,” “breast-feeding,” “breastmilk,” breast milk,” “breast-milk,” “human milk,” “colostrum,” and “iodide” and “iodine.” Filters limited search results to human studies published in English, French, German, Spanish, Hebrew, Danish, Norwegian, or Swedish. Two individuals independently screened unique article titles and abstracts to identify a list of relevant studies for full-text review. When opinions differed, a third individual reviewed the abstracts to resolve the discrepancy by a two-thirds majority. Review and original research articles were examined for references to other relevant studies not identified by the initial search. Studies were included if the research was original and nutrient concentrations in human milk were measured at ≥1 time points during the first 12 mo of lactation. Results from the breast milk of mothers who gave birth prematurely or who had other complicating factors (i.e., malnutrition, disease, inflammation, or smoking) were included. Exclusion criteria were animal studies, case studies, studies that measured nutrient status in serum but not breast milk, and studies referenced in a previous review. By using this strategy, a total of 14 original research studies were identified (Figure 1). Risk of bias was assessed at the individual study level through review of methods, data analysis, and reporting (Table 1). The principal summary measure was median or mean BMIC at various stages of lactation or in intervention and control groups.
FIGURE 1.

Flow diagram of studies considered for inclusion in the systematic review.
TABLE 1.
Description of studies included in the systematic review of breast-milk iodine concentration1
| Study, year (ref) | Country | Presumed iodine adequacy of population | n | Time | Intervention | Salt iodization2 | Taking supplements containing iodine, % | BMIC3, μg/L | Range or IQR, μg/L | Analytical method | Comments | Bias |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Andersen et al., 2014 (13) | Denmark | Yes | 127 | 14–135 d | None | + | 46.9 (postpartum), 83.3 (in pregnancy) | 83 | IQR: 61–125 | Sandell-Kolthoff colorimetry | Weak significant correlation between UIC and BMIC (r = 0.27, P = 0.015), stronger when UIC adjusted for urinary creatinine (fluid intake marker) (r = 0.79, P < 0.001). BMIC significantly higher in women taking supplements (112 vs. 72 μg/L, P < 0.001), with higher BMIC in women taking 150–175 vs. 45 μg/d postpartum (P = 0.05). | Iodine content of fluids unknown; single region of Denmark; no dietary intake data |
| Andersson et al., 2010 (14) | Switzerland | Yes | 181 | 6 or 12 mo | None | + | 3 | 48.9 μg/kg combined, 6 mo: 50.6 μg/kg (n = 149), 12 mo: 42.3 μg/kg (n = 32) | N/A | Sandell-Kolthoff with spectrophotometric detection | No significant difference between 6 and 12 mo in BMIC. BMIC positively correlated with UIC of infants (P < 0.001). | No dietary intake data; cross-sectional comparison between time points |
| Bouhouch et al., 2014 (15) | Morocco | Region of moderate-to-severe iodine deficiency | 239 | <8 wk (baseline) and 3, 6, and 9 mo | 400 mg oral iodine (oil) at ≤8 wk PP (n = 121) | — | — | Baseline: 40.8 (supp) vs. 42.8 (control); 3 mo: 61.4 vs. 33.2; 6 mo: 49.1 vs. 35.7; 9 mo: 39.4 vs. 26.2 | IQR: 35.8–94.8 (supp) vs. 18.4–53.1 (control) at 3 mo | ICP-MS | Significantly higher BMIC in supplementation vs. control group through 9 mo (P < 0.0001). Supplementing mothers more effective at improving infant iodine status (UIC) than supplementing infants with 200 mg I directly (P = 0.015). | No dietary intake data but assumed to be low; no infant control group |
| Chung et al., 2009 (16) | Korea | Yes | 31 | 1, 3, and 6 wk | None | — | N/A | 2529, 1153, and 822 at respective time points | 198–8484 | Sandell-Kolthoff colorimetry | BMIC high due to traditional intake of brown seaweed soup during lactation. Excessive iodine intake (>100 μg ⋅ kg−1 ⋅ d−1) from breast milk associated with subclinical hypothyroidism. | Preterm infants (<34 wk gestation); small sample; no quantitative dietary data |
| Dasgupta et al., 2008 (17) | United States | Yes | 13 | 55–253 d at first collection | None | + | N/A | 110 | 26–630 | ICP-MS | Each subject collected 4 samples/d for 9 consecutive days. All but one infant with inadequate iodine intake from breast milk as defined by IOM (110 μg/d ≤6 mo and 130 μg 6–12 mo). | Wide range in lactational stage; small sample; no dietary data |
| Fernández-Sánchez et al., 2007 (18) | Spain | Yes | 14 | Not reported, casual | None | + | N/A | 144 ± 93.2 μg/kg (mean) | N/A | ICP-MS | Majority of breast-milk iodine (80–90%) in whey, 5–10% in casein, 2% in fat. Methods paper. | Small sample; no dietary data |
| Hannan et al., 2009 (19) | United States | No (low-income) | 31 | 30–45 d (n = 31), 75–90 d (n = 17) | None | + | N/A | 30–45 d: 47.8 ± 17.1; 75–90 d: 42.3 ± 8.71 (P < 0.05) | N/A | Neutron activation analysis | Significantly higher iodine intake (24-h recall) and BMIC at 30–45 d than at 75–90 d. No significant correlation between dietary and BM iodine at either time point or both combined. | Mexican-American women; small sample, especially at 75–90 d |
| Kirk et al., 2012 (20) | United States | Yes | 13 | 1–8 mo (4 times/d for 3 d in each of 3 regimens) | Each subject underwent 3 regimens: 1) no supplement, 2) 150 μg/d in the morning, 3) 150 μg/d in the evening | +/ − (users/nonusers) | N/A | Overall: 56.5 ± 55.2; users of iodized salt (n = 7): 71.3 ± 26.3; nonusers (n = 6): 37.9 ± 14.9 | N/A | ICP-MS | No significant differences were found in BMIC between any of the regimens. Iodized salt users (n = 7) had significantly higher BMIC than non–iodized salt users (P < 0.03). Infant UIC exceeded estimated iodine intake from BMIC. | Short intervention period; small sample; no dietary data |
| Leung et al., 2009 (21) | United States, Boston | Yes | 61 | <60 h | None | + | Not reported | 51.4 | 21.2–304.2 | Colorimetry | Weak but significant inverse correlation between maternal UIC per gram creatinine and colostrum iodine (r2 = 0.12, P = 0.007). | Sufficient colostrum collected from 61 of 97 participants; no dietary data |
| Leung et al., 2012 (22) | United States, Boston | Yes | 16 | Not reported; samples collected at baseline and hourly for 8 h | 600 μg KI (456 μg iodide) | + | 12.5; not taken within 24 h before study supplement | Baseline: 45.5; peak: 354 | Baseline IQR: 34.5–169.0; peak IQR: 315–495 | Colorimetry | Median time to peak: 6 h (IQR: 5–7 h) | Small sample; stage of lactation not reported |
| Mekrungcharas and Kasemsup, 2014 (23) | Thailand | National programs to counter IDD | 100 | Median 31 d (IQR: 14–71 d) | None | +/ − (90% of participants used iodized salt) | 18 (in pregnancy), 7 (in lactation) | 129.7 | IQR: 81.0–205.7 | Spectrophotometer kinetic assay | Significantly higher percentage of women with BMICs ≥150 μg/L in first month (56%) than later in lactation (28%) (P = 0.004). OR of BMIC ≥150 μg/L did not differ by supplementation during pregnancy or lactation or by use of iodized salt or fish sauce but was significantly associated with consumption of iodine-fortified eggs (P = 0.03). | Dietary data limited to food frequency of high-iodine foods |
| Mulrine et al., 2010 (24) | New Zealand | No | 109 (56 placebo, 27 and 26 in respective intervention doses) | 1, 2, 4, 8, 12, 16, 20, and 24 wk | Placebo, 75 μg/d (S1) or 150 μg/d (S2) from delivery until 24 wk postpartum | +(82–92% by treatment groups) | 0 (exclusion criterion) | 25–43 (placebo), 29–50 (S1), 44–78 (S2); geometric mean from delivery–24 wk | N/A | Colorimetry | BMIC in 150- and 75-μg/d groups 1.69 times and 1.31 times higher than in control group, respectively (P < 0.001, P = 0.03), but BMIC in treatment groups did not differ significantly from each other. Infant and maternal UIC was influenced by maternal treatment group (P = 0.006, P < 0.001). Significant decrease of 40% in BMIC in placebo group from 1 to 24 wk (P < 0.001); NS decrease in BMIC in control groups over same time. | No dietary data; maternal and infant UIC measured but correlations with BMIC not determined |
| Wang et al., 2009 (25) | China | Yes | 97 (49 <6 mo, 48 >6 mo) | Not reported | None | + | N/A | Overall: 163; <6 mo: 240; >6 mo: 122 | Overall: 16.48–875; <6 mo: 47.33–875, >6 mo: 16.48–391 | Sandell-Kolthoff method | Percentage of BMIC ≥150 μg/L significantly higher in women lactating <6 mo than in those lactating >6 mo (P < 0.01). Significantly positive correlation between BMIC and UIC of infants but not mothers. | No dietary data |
| Zhao et al., 2014 (26) | China | Yes | 90 | 5 − 11, 12–30, 31–60, 61–120, and 121 − 240 d | None | + | N/A | 292.4 ± 159.1, 226.7 ± 122.0, 230.6 ± 297.5, 222.0 ± 331.0, 184.3 ± 95.7 (mean ± SD, μg/kg) at the respective time points | ICP-MS | 349.9 μg/kg cesarean delivery vs. 237.5 μg/kg vaginal delivery in transitional milk (5–11 d) (P < 0.001). | No dietary data reported (collected per methods) |
1BM, breast-milk; BMIC, breast-milk iodine concentration; ICP-MS, inductively coupled plasma MS; IDD, iodine deficiency disorder; IOM, Institute of Medicine; KI, potassium iodide; N/A, not available; PP, postpartum; ref, reference; supp, supplemented; S1, first supplementation protocol; S2, second supplementation protocol; UIC, urinary iodine concentration; +, yes; −, no.
2Indicates presence of salt iodization, either stated in the text or based on national salt iodization data (27).
3Values are medians or mean ± SDs.
Results
Description of included studies
Of the 14 studies included in the systematic review (Table 1), 5 were conducted in populations of lactating women in the United States (17, 19–22), 4 in Asia (China, South Korea, and Thailand) (16, 23, 25, 26), 3 in Western Europe (Denmark, Spain, and Switzerland) (13, 14, 18), 1 in New Zealand (24), and 1 in Northern Africa (Morocco) (15). In 3 of the studies at least a subset of the subject base was recognized to have a high population prevalence of iodine deficiency or endemic goiter (15, 23, 24), whereas in 1 study maternal excess iodine consumption was a concern (16). Salt iodization policies were in place in most countries during the time of the studies, with the exception of South Korea where dietary iodine intake is high, especially during lactation (16), and Morocco (15). Five studies included in the review collected data on household use of iodized salt (14, 15, 17, 20, 24).
Five of the 14 included studies measured iodine concentrations longitudinally at 2–8 time points spanning periods from colostrum through 9 mo of lactation (15, 16, 19, 24, 26). Among the longitudinal studies 2 were supplementation trials, both involving a control group (15, 24). The remainder of included studies were cross-sectional and measured BMIC either at a specific lactation time or stage or at any point during lactation.
Sample sizes of included studies (with the use of baseline n for longitudinal studies) ranged from 13 to 239 with a median of n = 76 (IQR: 20–107). Although a few studies had strict breast-milk sampling protocols involving multiple collections per day over 3–9 d, alternating between fore- and hindmilk (17, 20), the majority were casually collected samples of 5–120 mL. No study protocols involved full breast expression. Potential sources of bias in individual studies are described in Table 1. These include small sample size, method and timing of breast-milk collection, methodologic limitations leading to over- or underestimation of iodine, and selection bias based on known conditions.
Breast-milk iodine concentrations over the course of lactation
Because of substantial regional variations attributable to intake patterns, soil iodine quality, and uncertainty in measurement accuracy, trends in BMIC over the course of lactation are best interpreted through longitudinal studies in unsupplemented women (Figure 2). Of the 5 longitudinal studies that included, at minimum, a control group without maternal iodine supplementation, 2 were conducted in populations with poor iodine status (15, 24), 2 in populations deemed to be iodine replete (19, 26), and 1 in a South Korean population with a high dietary iodine intake (16). Of 3 studies that measured BMIC in early lactation (≤1 wk postpartum) (16, 24, 26), the 2 with higher initial concentrations showed a sharper decrease in concentration from colostrum to mature milk (16, 26). A gradual decline in mature BMIC at ≤9 mo of lactation was observed across longitudinal studies (15, 16, 19, 24, 26), with one study reporting a 40% decrease in BMIC from 1 to 24 wk of lactation in unsupplemented women (24).
FIGURE 2.
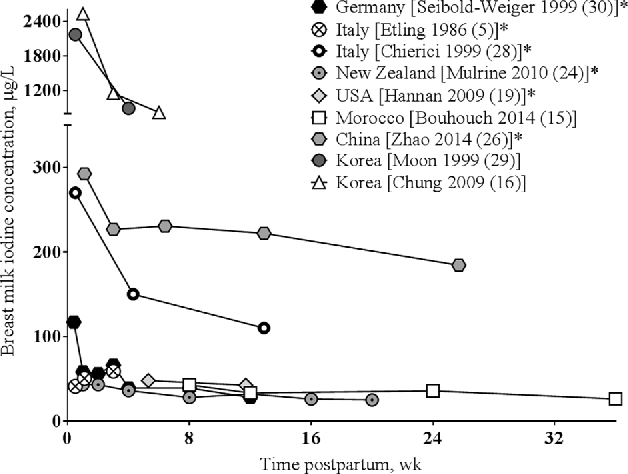
Breast-milk iodine concentrations in longitudinal studies in unsupplemented women. Values are means at each time point within a study. *Indicates presence of salt iodization, either stated in the text or based on national salt iodization data (27).
Cross-sectional data also showed decreases in BMIC during lactation. In Thailand, 56% compared with 28% of women had BMICs ≥150 μg/L in the first month compared with later in lactation (P = 0.004), whereas in China, 64.6% compared with 24.5% of women had BMICs ≥150 μg/L at <6 mo compared with at >6 mo of lactation (P < 0.01) (23, 25). Another cross-sectional study in Switzerland found no significant difference in BMICs measured at 6 and 12 mo of lactation (14).
Factors affecting BMIC
One study found a positive correlation between BMIC and maternal urinary iodine concentration (UIC), which was stronger when adjusted for creatinine (13), whereas another found a weak but significant positive correlation between colostrum iodine concentration and creatinine-adjusted UIC. BMIC was not significantly correlated with maternal UIC, unadjusted for creatinine, in a study conducted in China (25).
In South Korea, lactating mothers with assumed iodine intakes >2000 μg/d had BMICs in the range of 822–2529 μg/L between 1 and 6 wk of lactation (16). In comparison, measured BMICs in a Moroccan population with moderate to severe iodine deficiency were <50 μg/L during a similar period of lactation (15). Two studies failed to find a correlation between BMIC and iodine intake at 1–3 mo of lactation in populations with calculated intakes below recommended levels (19) or with a history of prevalent iodine deficiency disorders (23).
A cross-sectional study in lactating women in the United States found significantly higher BMICs in 7 women who used iodized salt than in 6 women who used noniodized salt at various stages of lactation (P < 0.03) (20). In Thailand, the frequency of iodine-fortified egg consumption but not the use of iodized salt or iodized fish sauce significantly improved the OR of BMICs ≥150 μg/L (23). Despite the presence of salt iodization, the mean BMIC in well-nourished unsupplemented women was <100 μg/L at all time points in 5 studies (13, 14, 20–22).
Perchlorate, a widespread environmental contaminant that has been detected in breast-milk samples, acts as a competitive inhibitor of the NIS in the lactating mammary gland. No correlation was found between colostrum iodine and perchlorate concentrations in the study by Leung et al. (21), nor were daily oral supplements of 150 μg I taken in the morning or the evening effective at altering the perchlorate concentrations of breast milk (20). The results of a small but well-designed study by Dasgupta et al. (17) suggested a much lower selectivity factor of perchlorate over iodine by the NIS than previously reported in the literature; however, the study also found that 21% of maternal iodine intake but 56% of perchlorate intake are excreted in breast milk.
BMICs were significantly lower at 5–11 d of lactation in women who underwent a cesarean delivery than in women who had a vaginal delivery (26). In one study subset of 13 women, a small but significantly higher BMIC was measured in a sample collected before rather than after breastfeeding (13). Another study found a slight inverse correlation between BMIC and maternal age (23).
Effect of supplementation
Of 3 supplementation trials included in the review, 2 were randomized controlled trials (RCTs) conducted in populations with poor iodine status (15, 24), 1 with a placebo control (24). The third was a crossover design in a well-nourished population (20). One RCT involved a single high-dose maternal supplement of 400 mg I delivered orally during early lactation (15), and the second involved daily supplementation with 75 or 100 μg I from delivery through 24 wk of lactation (24). In both studies, BMIC was significantly higher in the treatment than in the control groups at all measured time points through 6–9 mo of lactation. In the third study, no differences in BMIC were found between 3-d periods of no supplementation, 150 μg I in the morning, and 150 μg I in the evening (20).
In 2 studies that evaluated a dose-response relation of postpartum supplementation, BMIC was higher in women taking greater quantities of iodine in daily supplements. In the study by Mulrine et al. (24), BMICs were 1.3 and 1.7 times higher in women supplemented with 75 and 150 μg I/d, respectively, than in controls from delivery through 3 mo of lactation. Twenty-four-hour breast-milk iodine excretion was significantly higher in women taking 150–175 μg I/d from postpartum multivitamin supplements compared with those taking 45 μg/d in an observational study in Denmark (P = 0.048) (13). In another study, BMIC did not differ between women who did or did not use iodine-containing multivitamin supplements in pregnancy or lactation (23). Peak BMIC occurred 6 h after a single oral 456-μg iodide load (as potassium iodide) in lactating mothers (22).
Relation between BMIC and infant UIC
Two studies included in the review found a significant positive correlation between BMIC and infant UIC, the primary indicator of infant iodine status (14, 25). Supplementing lactating mothers with 400 mg I was more effective at improving infant UIC than supplementing infants with 200 mg I directly (15). In the study by Kirk et al. (20), infant UIC exceeded estimated iodine intake from BMIC. The authors suggested that iodine-containing infant care products may have contaminated urine samples or contributed to UIC via transdermal absorption.
Comparison with previous data
The time trends in BMIC shown in the longitudinal studies in the present review agree with data from 3 earlier studies in Italy, South Korea, and Germany (Figure 2) (28–30), although these studies followed women at most through 3 mo of lactation. In a fourth previous study conducted in Italy, BMICs increased significantly from colostrum (2–5 d) to transitional (6–10 d) and mature (11–32 d) milk, but concentrations were low (<60 μg/L) at all time points, the sample size was small (n = 23), and intraindividual variation may have contributed to the observed trend (5).
Few studies have measured iodine intake quantitatively; however, consistent with the results of the present review, higher BMICs have been reported in areas of iodine sufficiency than in regions endemic for goiter (31–34). BMIC in individual mothers with goiter may or may not be depressed, reflecting a compensatory mechanism for iodine uptake by the mammary gland (3, 10). Iodized salt intake has been correlated with BMIC previously (35). Despite some evidence of an inverse association between BMIC and breast-milk perchlorate at perchlorate concentrations >10 μg/L (36), the lack of correlation shown in the present review is corroborated by the finding of a previous study (37).
Other maternal factors that may influence BMIC have been considered in recent as well as in earlier research. A correlation between BMIC and maternal UIC is inconsistent but more likely in regions of iodine sufficiency (3). Several studies, including those in the present review, have found a positive correlation between BMIC and UIC adjusted for creatinine in well-nourished populations (13, 21, 37, 38). Despite considerable diurnal variation in BMIC (39), no consistent trends have been shown by time of day, fore- or hindmilk, left or right breast, or season (3, 14). BMIC does not differ significantly in mothers of preterm or term infants (5). In contrast to the results of the Thai study included in the present review (23), a slight but significant positive correlation of BMIC with maternal age was found in one previous study (37), whereas no correlation was found in a second study (40). The maternal age range of 16–45 y was similar across these studies. Cigarette smoking was found to decrease BMIC in 2 studies (37, 41).
Three iodine supplementation trials in pregnancy, lactation, or both were published before the period of the present review. Two studies in which women were supplemented with 100–200 μg I/d from the second trimester of pregnancy through delivery (42) or lactation (43) found significantly higher colostrum iodine concentrations in supplemented mothers than in unsupplemented controls, which is consistent with results of the 2 lactation supplementation RCTs included in the present review. In the third study, women who received 116 μg potassium iodide daily from delivery through 3 mo of lactation did not have significantly different BMICs than did controls, although the sample size was small (n = 22) and the analytical methods were poorly described (28).
BMICs were higher in women taking daily multivitamin supplements that contained iodine during pregnancy or lactation than in those who did not in several previous studies (13, 30, 44). However, this finding was not corroborated by Bader et al. (45) in a small cohort of German women in early lactation. On the basis of dietary intake data, the authors concluded that women not taking supplements made a greater effort to obtain adequate iodine from dietary sources.
Discussion
According to the findings of the present systematic review as well as previous data, BMICs are widely variable across populations, which is likely influenced by habitual and recent maternal iodine intake and status. BMIC is highest in colostrum and decreases throughout lactation. The rate of concentration decline is most rapid in early lactation, especially in women with a higher initial BMIC. Environmental contaminants such as perchlorate and thiocyanate act as competitive inhibitors of iodine uptake by the mammary gland; however, an inverse correlation between BMIC and perchlorate has been observed previously only at high breast-milk perchlorate concentrations (>10 μg/L) and was not replicated in this review. Aside from smoking, which produces thiocyanate, other maternal factors and breastfeeding practices evaluated are not consistently associated with BMIC. Supplementation with high-dose or daily iodine during lactation is effective at increasing BMIC, with some evidence of a dose-response relation. The correlation between BMIC and infant UIC suggests that interventions to improve BMIC would have a positive impact on infant iodine status.
There is no scientific consensus on the optimal BMIC necessary to meet infant iodine requirements, which are themselves poorly defined. The Adequate Intake levels established by the Food and Nutrition Board of the Institute of Medicine are 110 μg/d for infants aged 0–6 mo and 130 μg/d for infants aged 6–12 mo (46). The basis for these recommendations is a single study published in 1984 that collected 61 samples from 37 US lactating women between 14 d and 3.5 y postpartum and found a wide range of iodine concentrations in breast milk (29–490 μg/L; mean: 178 μg/L) (35). In contrast, a technical consultation of the WHO recommended intakes of 90 μg I/d up to the age of 2 y, although related data on breast milk concentrations were not mentioned (47). Recently, a crossover dose-response metabolic iodine balance study in eleven 2- to 5-mo-old healthy, full-term, euthyroid, formula-fed Swiss infants found that a null balance was achieved at an intake of 70 μg/d, although a buffer would be necessary for the accumulation of thyroidal iodine stores (48). Infants aged 2 and 4 mo with average breast-milk intakes of 0.781 and 0.855 L/d, respectively (49), would need BMICs of 141 μg/L at 2 mo and 129 μg/L at 4 mo to meet the Institute of Medicine recommendations and BMICs of 115 and 105 μg/L at the same time points to meet the WHO recommendations. The data of Dold et al. (48) suggest a BMIC ≥92 μg/L to meet an infant's daily iodine requirement. A BMIC of 150 μg/L would meet the range of estimated needs without nearing intakes of >100 μg ⋅ kg−1 ⋅ d−1, which have been associated with subclinical hypothyroidism in infants (16).
In countries or regions where <90% of households consume iodized salt and the median urinary iodine concentration is <100 μg/L, the technical consultation of the WHO recommends annual supplementation of women of reproductive age with 400 mg I as iodized oil, or a daily supplement of 150 μg for nonpregnant and nonlactating women and 250 μg for pregnant or lactating women (47). The American Thyroid Association recommends that all pregnant and lactating women, regardless of status, take a daily supplement of 150 μg I to reduce the risk of iodine deficiency disorders in infants (50). On the basis of data reported in this review, neither high-dose 400-mg supplemental iodine as iodized oil (15) nor 150 μg I/d during lactation (24) is sufficient to achieve a BMIC of 150 μg/L in regions of iodine deficiency.
The present systematic review identified several limitations in the existing data. It has been shown that the colorimetric assay for iodine in breast milk, which was used in 6 of the included studies (13, 16, 21, 22, 24, 25), is unreliable (51, 52). Inductively coupled plasma MS is considered the gold standard for iodine analysis (53); this method was used in 6 of the studies (14, 15, 17, 18, 20, 26). It is possible that analytical inaccuracy may have contributed to the wide range of BMICs observed. In addition, most studies failed to collect dietary data, which would have contributed to the interpretation of BMIC. Finally, data on BMICs are not globally representative and are unavailable from South America, Australia, and much of North America and Africa.
In conclusion, there exists no consensus on optimal BMIC, in large part because of the debate over iodine requirements of infants. Measured concentrations of iodine in breast milk vary ≤100-fold on the basis of maternal diet, environmental factors enhancing or inhibiting iodine availability in the food supply, salt iodization, maternal supplementation, and measurement inaccuracies. Although the studies included in the review add to the knowledge base with regard to BMIC and support the effectiveness of interventions to achieve a BMIC of ∼150 μg/L, more research is needed to define and attain an ideal BMIC in well-nourished women without risking excess. To better understand iodine balance in lactating mothers and infants, BMIC in exclusively breastfed infants should be measured in parallel with maternal dietary intake and maternal and infant urinary iodine excretion. Thyroid-stimulating hormone is elevated in iodine-deficient infants in the first few weeks of life and may be used as an early indicator of maternal and infant iodine sufficiency. A more thorough understanding of iodine physiology during lactation will better enable the prevention and control of deficiency and its consequences in the mother-infant dyad.
Acknowledgments
Both authors read and approved the final manuscript.
Notes
Published in a supplement to Advances in Nutrition. Supplement funding was provided by the Bill & Melinda Gates Foundation. The Supplement Coordinators for this supplement were Lindsay H Allen and Daphna K Dror. Supplement Coordinator disclosure: Lindsay H Allen has no conflict of interest. Daphna K Dror has no conflict of interest. Publication costs for this supplement were defrayed in part by the payment of page charges. This publication must therefore be hereby marked “advertisement” in accordance with 18 USC section 1734 solely to indicate this fact. The opinions expressed in this publication are those of the author(s) and are not attributable to the sponsors or the publisher, Editor, or Editorial Board of Advances in Nutrition.
Supported by the Bill & Melinda Gates Foundation (OPP1061055) and intramural USDA–Agricultural Research Service projects 5306-51000-003-00D and 5306-51000-004-00D.
Author disclosures: DKD and LHA, no conflicts of interest.
The USDA, Agricultural Research Service, is an equal opportunity provider and employer.
Abbreviations used:
- BMIC
breast-milk iodine concentration
- NIS
sodium-iodide symporter
- RCT
randomized controlled trial
- UIC
urinary iodine concentration.
References
- 1. Zimmermann MB. Are weaning infants at risk of iodine deficiency even in countries with established iodized salt programs? Nestle Nutr Inst Workshop Ser 2012;70:137–46. [DOI] [PubMed] [Google Scholar]
- 2. Zoeller RT, Rovet J. Timing of thyroid hormone action in the developing brain: clinical observations and experimental findings. J Neuroendocrinol 2004;16:809–18. [DOI] [PubMed] [Google Scholar]
- 3. Azizi F, Smyth P. Breastfeeding and maternal and infant iodine nutrition. Clin Endocrinol (Oxf) 2009;70:803–9. [DOI] [PubMed] [Google Scholar]
- 4. Rohner F, Zimmermann M, Jooste P, Pandav C, Caldwell K, Raghavan R, Raiten DJ. Biomarkers of nutrition for development—iodine review. J Nutr 2014;144(Suppl):1322S–42S. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Etling N, Padovani E, Fouque F, Tato L. First-month variations in total iodine content of human breast milks. Early Hum Dev 1986;13:81–5. [DOI] [PubMed] [Google Scholar]
- 6. Delange F. Iodine requirements during pregnancy, lactation and the neonatal period and indicators of optimal iodine nutrition. Public Health Nutr 2007;10(12A):1571–80; discussion 81–3. [DOI] [PubMed] [Google Scholar]
- 7. Delange F. Requirements of iodine in humans. In: Delange F, Dunn JT, Glinoer D, (eds) Iodine Deficiency in Europe: A ContInuing Concern. New York: Plenum Press; 1993,5–15. [Google Scholar]
- 8. Ares S, Quero J, Morreale de Escobar G. Neonatal iodine deficiency: clinical aspects. J Pediatr Endocrinol Metab 2005;18:1257–64. [DOI] [PubMed] [Google Scholar]
- 9. Spitzweg C, Joba W, Eisenmenger W, Heufelder AE. Analysis of human sodium iodide symporter gene expression in extrathyroidal tissues and cloning of its complementary deoxyribonucleic acids from salivary gland, mammary gland, and gastric mucosa. J Clin Endocrinol Metab 1998;83:1746–51. [DOI] [PubMed] [Google Scholar]
- 10. Parr RM, DeMaeyer EM, Iyengar VG, Byrne AR, Kirkbright GF, Schoch G, Niinisto L, Pineda O, Vis HL, Hofvander Y et al. Minor and trace elements in human milk from Guatemala, Hungary, Nigeria, Philippines, Sweden, and Zaire: results from a WHO/IAEA joint project. Biol Trace Elem Res 1991;29:51–75. [DOI] [PubMed] [Google Scholar]
- 11. Semba RD, Delange F. Iodine in human milk: perspectives for infant health. Nutr Rev 2001;59:269–78. [DOI] [PubMed] [Google Scholar]
- 12. Dorea JG. Iodine nutrition and breast feeding. J Trace Elem Med Biol 2002;16:207–20. [DOI] [PubMed] [Google Scholar]
- 13. Andersen SL, Moller M, Laurberg P. Iodine concentrations in milk and in urine during breastfeeding are differently affected by maternal fluid intake. Thyroid 2014;24:764–72. [DOI] [PubMed] [Google Scholar]
- 14. Andersson M, Aeberli I, Wust N, Piacenza AM, Bucher T, Henschen I, Haldimann M, Zimmermann MB. The Swiss iodized salt program provides adequate iodine for school children and pregnant women, but weaning infants not receiving iodine-containing complementary foods as well as their mothers are iodine deficient. J Clin Endocrinol Metab 2010;95:5217–24. [DOI] [PubMed] [Google Scholar]
- 15. Bouhouch RR, Bouhouch S, Cherkaoui M, Aboussad A, Stinca S, Haldimann M, Andersson M, Zimmermann MB. Direct iodine supplementation of infants versus supplementation of their breastfeeding mothers: a double-blind, randomised, placebo-controlled trial. Lancet Diabetes Endocrinol 2014;2:197–209. [DOI] [PubMed] [Google Scholar]
- 16. Chung HR, Shin CH, Yang SW, Choi CW, Kim BI. Subclinical hypothyroidism in Korean preterm infants associated with high levels of iodine in breast milk. J Clin Endocrinol Metab 2009;94:4444–7. [DOI] [PubMed] [Google Scholar]
- 17. Dasgupta PK, Kirk AB, Dyke JV, Ohira S. Intake of iodine and perchlorate and excretion in human milk. Environ Sci Technol 2008;42:8115–21. [DOI] [PubMed] [Google Scholar]
- 18. Fernández-Sánchez LM, Bermejo-Barrera P, Fraga-Bermudez JM, Szpunar J, Lobinski R. Determination of iodine in human milk and infant formulas. J Trace Elem Med Biol 2007;21:10–3. [DOI] [PubMed] [Google Scholar]
- 19. Hannan MA, Faraji B, Tanguma J, Longoria N, Rodriguez R. Maternal milk concentration of zinc, iron, selenium, and iodine and its relationship to dietary intakes. Biol Trace Elem Res 2009;127:6–15. [DOI] [PubMed] [Google Scholar]
- 20. Kirk AB, Kroll M, Dyke JV, Ohira S, Dias RA, Dasgupta PK. Perchlorate, iodine supplements, iodized salt and breast milk iodine content. Sci Total Environ 2012;420:73–8. [DOI] [PubMed] [Google Scholar]
- 21. Leung AM, Pearce EN, Hamilton T, He X, Pino S, Merewood A, Braverman LE. Colostrum iodine and perchlorate concentrations in Boston-area women: a cross-sectional study. Clin Endocrinol (Oxf) 2009;70:326–30. [DOI] [PubMed] [Google Scholar]
- 22. Leung AM, Braverman LE, He X, Heeren T, Pearce EN. Breastmilk iodine concentrations following acute dietary iodine intake. Thyroid 2012;22:1176–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Mekrungcharas T, Kasemsup R. Breast milk iodine concentrations in lactating mothers at Queen Sirikit National Institute of Child Health. J Med Assoc Thai 2014;97:S115–9. [PubMed] [Google Scholar]
- 24. Mulrine HM, Skeaff SA, Ferguson EL, Gray AR, Valeix P. Breast-milk iodine concentration declines over the first 6 mo postpartum in iodine-deficient women. Am J Clin Nutr 2010;92:849–56. [DOI] [PubMed] [Google Scholar]
- 25. Wang Y, Zhang Z, Ge P, Wang Y, Wang S. Iodine status and thyroid function of pregnant, lactating women and infants (0–1 yr) residing in areas with an effective universal salt iodization program. Asia Pac J Clin Nutr 2009;18:34–40. [PubMed] [Google Scholar]
- 26. Zhao A, Ning Y, Zhang Y, Yang X, Wang J, Li W, Wang P. Mineral compositions in breast milk of healthy Chinese lactating women in urban areas and its associated factors. Chin Med J (Engl) 2014;127:2643–8. [PubMed] [Google Scholar]
- 27. Andersson M, de Benoist B, Darnton-Hill I, Delange F. Iodine Deficiency in Europe: A Continuing Public Health Problem. Geneva (Switzerland): WHO, UNICEF; 2007. [Google Scholar]
- 28. Chierici R, Saccomandi D, Vigi V. Dietary supplements for the lactating mother: influence on the trace element content of milk. Acta Paediatr Suppl 1999;88:7–13. [DOI] [PubMed] [Google Scholar]
- 29. Moon S, Kim J. Iodine content of human milk and dietary iodine intake of Korean lactating mothers. Int J Food Sci Nutr 1999;50:165–71. [DOI] [PubMed] [Google Scholar]
- 30. Seibold-Weiger K, Wollmann H, Rendl J, Ranke M, Speer C. Iodine concentration in the breast milk of mothers of premature infants. Z Geburtshilfe Neonatol 1999;203:81–5(in German). [PubMed] [Google Scholar]
- 31. Heidemann PH, Stubbe P, von Reuss K, Schurnbrand P, Larson A, von Petrykowski W. Iodine excretion and dietary iodine supply in newborn infants in iodine-deficient regions of West Germany. Dtsch Med Wochenschr 1984;109:773–8(in German). [DOI] [PubMed] [Google Scholar]
- 32. Vermiglio F, Lo Presti VP, Finocchiaro MD, Battiato S, Grasso L, Ardita FV, Mancuso A, Trimarchi F. Enhanced iodine concentrating capacity by the mammary gland in iodine deficient lactating women of an endemic goiter region in Sicily. J Endocrinol Invest 1992;15:137–42. [DOI] [PubMed] [Google Scholar]
- 33. Aquaron R, Zarrouck K, el Jarari M, Ababou R, Talibi A, Ardissone JP. Endemic goiter in Morocco (Skoura-Toundoute areas in the high Atlas). J Endocrinol Invest 1993;16:9–14. [DOI] [PubMed] [Google Scholar]
- 34. Pongpaew P, Supawan V, Tungtrongchitr R, Phonrat B, Vudhivai N, Chantaranipapong Y, Kitjaroentham A, Jintaridhi P, Intarakhao C, Mahaweerawat U et al. Urinary iodine excretion as a predictor of the iodine content of breast milk. J Med Assoc Thai 1999;82:284–9. [PubMed] [Google Scholar]
- 35. Gushurst CA, Mueller JA, Green JA, Sedor F. Breast milk iodide: reassessment in the 1980s. Pediatrics 1984;73:354–7. [PubMed] [Google Scholar]
- 36. Kirk AB, Martinelango PK, Tian K, Dutta A, Smith EE, Dasgupta PK. Perchlorate and iodide in dairy and breast milk. Environ Sci Technol 2005;39:2011–7. [DOI] [PubMed] [Google Scholar]
- 37. Pearce EN, Leung AM, Blount BC, Bazrafshan HR, He X, Pino S, Valentin-Blasini L, Braverman LE. Breast milk iodine and perchlorate concentrations in lactating Boston-area women. J Clin Endocrinol Metab 2007;92:1673–7. [DOI] [PubMed] [Google Scholar]
- 38. Chan SS, Hams G, Wiley V, Wilcken B, McElduff A. Postpartum maternal iodine status and the relationship to neonatal thyroid function. Thyroid 2003;13:873–6. [DOI] [PubMed] [Google Scholar]
- 39. Kirk AB, Dyke JV, Martin CF, Dasgupta PK. Temporal patterns in perchlorate, thiocyanate, and iodide excretion in human milk. Environ Health Perspect 2007;115:182–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Younes B, Almeshari A, Alhakeem A, Alzamil F, Alsaleh S, Alattas O. Iodine level in breast milk of nursing mothers living in Riyadh City. Med Sci Res 1994;22:675–6. [Google Scholar]
- 41. Laurberg P, Nohr SB, Pedersen KM, Fuglsang E. Iodine nutrition in breast-fed infants is impaired by maternal smoking. J Clin Endocrinol Metab 2004;89:181–7. [DOI] [PubMed] [Google Scholar]
- 42. Glinoer D, De Nayer P, Delange F, Lemone M, Toppet V, Spehl M, Grün J-P, Kinthaert J, Lejeune B. A randomized trial for the treatment of mild iodine deficiency during pregnancy: maternal and neonatal effects. J Clin Endocrinol Metab 1995;80:258–69. [DOI] [PubMed] [Google Scholar]
- 43. Pedersen KM, Laurberg P, Iversen E, Knudsen PR, Gregersen HE, Rasmussen OS, Larsen KR, Eriksen GM, Johannesen PL. Amelioration of some pregnancy-associated variations in thyroid function by iodine supplementation. J Clin Endocrinol Metab 1993;77:1078–83. [DOI] [PubMed] [Google Scholar]
- 44. Nøhr SB, Laurberg P, Børlum K, Pedersen KM, Johannesen PL, Damm P, Fuglsang E, Johansen A. Iodine status in neonates in Denmark: regional variations and dependency on maternal iodine supplementation. Acta Paediatr 1994;83:578–82. [DOI] [PubMed] [Google Scholar]
- 45. Bader N, Moller U, Leiterer M, Franke K, Jahreis G. Pilot study: tendency of increasing iodine content in human milk and cow's milk. Exp Clin Endocrinol Diabetes 2005;113:8–12. [DOI] [PubMed] [Google Scholar]
- 46. Institute of Medicine Dietary Reference Intakes for vitamin A, vitamin K, arsenic, boron, chromium, copper, iodine, iron, manganese, molybdenum, nickel, silicon, vanadium, and zinc. Report of the Panel on Micronutrients. Washington (DC): National Academies Press; 2001. [PubMed] [Google Scholar]
- 47. Andersson M, de Benoist B, Delange F, Zupan J. Prevention and control of iodine deficiency in pregnant and lactating women and in children less than 2-years-old: conclusions and recommendations of the technical consultation. Public Health Nutr 2007;10:1606–11. [DOI] [PubMed] [Google Scholar]
- 48. Dold S, Zimmermann MB, Baumgartner J, Davaz T, Galetti V, Braegger C, Andersson M. A dose-response crossover iodine balance study to determine iodine requirements in early infancy. Am J Clin Nutr 2016;104:620–8. [DOI] [PubMed] [Google Scholar]
- 49. Michaelsen KF, Larsen PS, Thomsen BL, Samuelson G. The Copenhagen Cohort Study on infant nutrition and growth: breast-milk intake, human milk macronutrient content, and influencing factors. Am J Clin Nutr 1994;59:600–11. [DOI] [PubMed] [Google Scholar]
- 50. Public Health Committee of the American Thyroid Association ; Becker DV, Braverman LE, Delange F, Dunn JT, Franklyn JA, Hollowell JG, Lamm SH, Mitchell ML, Pearce E et al. Iodine supplementation for pregnancy and lactation—United States and Canada: recommendations of the American Thyroid Association. Thyroid 2006;16:949–51. [DOI] [PubMed] [Google Scholar]
- 51. Shelor CP, Campbell CA, Kroll M, Dasgupta PK, Smith TL, Abdalla A, Hamilton M, Muhammad TW. Fenton digestion of milk for iodinalysis. Anal Chem 2011;83:8300–7. [DOI] [PubMed] [Google Scholar]
- 52. Dold S, Baumgartner J, Zeder C, Krzystek A, Osei J, Haldimann M, Zimmermann MB, Andersson M. Optimization of a new mass spectrometry method for measurement of breast milk iodine concentrations (BMIC) and an assessment of the effect of analytic method and timing of within-feed sample collection on BMIC. Thyroid 2016;26:287–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Huynh D, Zhou SJ, Gibson R, Palmer L, Muhlhausler B. Validation of an optimized method for the determination of iodine in human breast milk by inductively coupled plasma mass spectrometry (ICPMS) after tetramethylammonium hydroxide extraction. J Trace Elem Med Biol 2015;29:75–82. [DOI] [PubMed] [Google Scholar]