

Summary
Objective
Studies examining associations between movement behaviours (i.e. physical activity, sedentary behaviour and sleep duration) and obesity focus on average values of these movement behaviours, despite important within‐country and between‐country variability. A better understanding of movement behaviour inequalities is important for developing public health policies and behaviour‐change interventions. The objective of this ecologic analysis at the country level was to determine if inequality in movement behaviours is a better correlate of obesity than average movement behaviour volume in children from all inhabited continents of the world.
Methods
This multinational, cross‐sectional study included 6,128 children 9–11 years of age. Moderate‐to‐vigorous physical activity (MVPA), total sedentary time (SED) and sleep period time were monitored over 7 consecutive days using waist‐worn accelerometry. Screen time was self‐reported. Inequality in movement behaviours was determined using Gini coefficients (ranging from 0 [complete equality] to 1 [complete inequality]).
Results
The largest inequality in movement behaviours was observed for screen time (Gini of 0.32; medium inequality), followed by MVPA (Gini of 0.21; low inequality), SED (Gini of 0.07; low inequality) and sleep period time (Gini of 0.05; low inequality). Average MVPA (h d−1) was a better correlate of obesity than MVPA inequality (r = −0.77 vs. r = 0.00, p = 0.03). Average SED (h d−1) was also a better correlate of obesity than SED inequality (r = 0.52 vs. r = −0.32, p = 0.05). Differences in associations for screen time and sleep period time were not statistically significant. MVPA in girls was found to be disproportionally lower in countries with more MVPA inequality.
Conclusions
Findings from this study show that average MVPA and SED should continue to be used in population health studies of children as they are better correlates of obesity than inequality in these behaviours. Moreover, the findings suggest that MVPA inequality could be greatly reduced through increases in girls' MVPA alone.
Keywords: Disparity, Gini coefficient, movement behaviours, paediatric population
Introduction
Low levels of physical activity, excess sedentary behaviour (especially screen time) and insufficient sleep duration have all been associated with obesity in children 1, 2, 3. Previous studies have focused on associations between average values of these movement behaviours and various health outcomes, despite surveillance and population studies suggesting important variability in physical activity, sedentary behaviour and sleep duration within and between countries 1, 4, 5. Moving beyond average values of movement behaviours and examining how levels of movement behaviours vary within countries is a critical next step, while also testing the relationships between movement behaviour inequality and health outcomes such as obesity. This analytical approach can provide useful information, because recent findings by Althoff et al. 6 showed that inequality in physical activity was a stronger correlate of obesity than with the use of mean values.
Althoff et al. 6 recently measured physical activity in 111 countries across the globe with the use of smartphones with built‐in accelerometry. They found inequality in how physical activity was distributed within countries and that this inequality was a better correlate of obesity prevalence (among 46 countries) in the population than average physical activity volume (steps per day). Lower physical activity levels in women contributed to a large portion of the observed physical activity inequality in their study (43%). However, whether inequalities in sedentary behaviour and sleep duration are also more predictive of obesity than average volume is currently unknown. Althoff et al. 6 also relied on self‐reported height and weight to measure obesity, and their study was mainly conducted in adults. The International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE) 7 provides a unique opportunity to address this issue and the limitations of Althoff's study. ISCOLE is a collaboration among scientists from 12 countries representing every inhabited continent, with children spanning a wide range of socioeconomic and human development, as well as geographic and cultural diversity. ISCOLE also collected high‐quality, objective measures of movement behaviours and adiposity across all sites using a standardized measurement protocol and rigorous quality control program.
The objective of this ecologic analysis at the country level was to quantify inequalities in the cumulative distribution of objectively measured physical activity, sedentary behaviour and sleep duration in 12 countries from six continents around the globe and examine the relationships between movement behaviour inequality and objective measures of adiposity among children. Whether movement behaviour inequality is a better correlate of obesity prevalence than average movement behaviour volume was also examined. As recently reported 6, it was hypothesized that movement behaviour inequality, as assessed by Gini coefficients, would be more predictive of obesity than average movement behaviour volume in this multinational study of children. The Gini coefficient is a common measure of statistical dispersion and ranges from 0 (perfect equality, where all movement behaviour values are the same in the population) to 1 (maximal inequality).
Methods
Study design and setting
International Study of Childhood Obesity, Lifestyle and the Environment is a cross‐sectional, multinational study designed to examine the relationships between lifestyle behaviours and obesity in 12 study sites located in Australia, Brazil, Canada, China, Colombia, Finland, India, Kenya, Portugal, South Africa, the United Kingdom and the United States. The rationale, design and methods of ISCOLE have previously been published in detail elsewhere 7. The primary sampling frame was schools, which were typically stratified by an indicator of socioeconomic status to maximize variability within sites. A standardized protocol was used to collect data across all sites, and all study personnel underwent rigorous training and certification to ensure high‐quality data. The Pennington Biomedical Research Center Institutional Review Board as well as Institutional/Ethical Review Boards at each site approved the study. Written informed consent was obtained from parents/legal guardians, and child assent was also obtained as required by local ethics review boards. Data were collected during the school year at each study site and occurred between September 2011 and December 2013.
Participants
International Study of Childhood Obesity, Lifestyle and the Environment recruitment targeted grade levels likely to ensure minimal variability around a mean age of 10 years. All children within the targeted grade level in a sampled school were eligible to participate; hence, the sample included 9–11‐year‐old children. Based on a priori sample size and power calculations 7, each site aimed to recruit a sex‐balanced sample of at least 500 children. Of the 7,372 children who participated in ISCOLE, a total of 6,128 remained in the analytical sample after excluding participants without valid accelerometry data (n = 1,214), information on screen time (n = 25) and body mass index (BMI) z‐scores (n = 5). Except for significantly higher BMI z‐scores, children who were excluded for missing data did not significantly differ from those who were included in the present analysis.
Measurements
Physical activity, sedentary time and sleep duration
Moderate‐to‐vigorous physical activity (MVPA), total sedentary time and nocturnal sleep period time were all objectively assessed using 24‐h, waist‐worn accelerometry 8. An ActiGraph GT3X+ accelerometer (ActiGraph LLC, Pensacola, FL, USA) was worn at the waist on an elasticized belt at the right mid‐axillary line. Participants were encouraged to wear the accelerometer 24 h d−1 (removing only for water‐based activities) for at least 7 d, including 2 weekend days. Overall, mean 24‐h wear time and wake wear time were 22.6 and 14.9 h d−1 in ISCOLE, respectively. The minimal amount of daytime data that was considered acceptable for inclusion was at least 4 d with at least 10 h of wake wear time per day, including at least 1 weekend day. Data were collected at a sampling rate of 80 Hz, downloaded in 1‐s epochs with the low‐frequency extension filter using the ActiLife software version 5.6 or higher (ActiGraph LLC), and reintegrated to 15‐ and 60‐s epochs for analysis.
Sleep period time (hours per night) was first estimated from the accelerometry data using 60‐s epochs and a fully automated algorithm for 24‐h waist‐worn accelerometers that was developed and validated for ISCOLE 9, 10. This algorithm produces more precise estimates of sleep period time than previous algorithms and captures total sleep period time from sleep onset to sleep offset, including all epochs and wakefulness after onset 9, 10. The weekly total sleep time averages were calculated using only days where valid sleep was accumulated (i.e. total sleep period time ≥160 min per night and >90% estimated wear time) and only for participants with at least 3 nights of valid sleep, including 1 weekend night (Friday or Saturday). After exclusion of total sleep period time and awake non‐wear time (any sequence of ≥20 consecutive minutes of 0 activity counts), MVPA was defined as all activity ≥574 counts/15 s and total sedentary time as all movement ≤25 counts/15 s, consistent with the widely used Evenson cut‐offs 11.
Finally, child‐reported screen time was assessed using questions from the US Youth Risk Behavior Surveillance System 12. Children were asked to report how many hours they typically watched TV, and how many hours they played video games and/or used the computer per weekday, and per weekend day. As previously reported 13, a daily average screen time score was calculated by weighting the responses for each question (2/7 for weekend and 5/7 for weekday). Self‐report methods of quantifying screen time have been reported to have acceptable reliability and validity in children 14, 15.
Inequality in physical activity, sedentary behaviour and sleep duration
Inequality in movement behaviours was assessed using the Gini coefficient 16, 17, as it is the most commonly used measure with which to quantify inequality and statistical dispersion 18. The Gini coefficient is based on the Lorenz curve, which plots the share of the sample's total average movement behaviours that is cumulatively recorded by the bottom X% of the sample. The Gini coefficient is the ratio of the area that lies between the line of equality and the Lorenz curve to the total area under the line of equality. Scores for the Gini coefficient range from 0 (complete equality) to 1 (complete inequality). A Gini coefficient of ≥0.5 is generally considered ‘high’, between 0.3 and 0.5 is considered ‘medium’ and <0.3 is considered low.
Measurement of obesity
Body mass was measured with a Tanita SC‐240 scale (Arlington Heights, IL, USA), after all outer clothing, heavy pocket items and shoes were removed. Body height was measured without shoes using a Seca 213 portable stadiometer (Hamburg, Germany), with the participant's head in the Frankfort horizontal plane. Each measurement was repeated, and the average was used for analysis (a third measurement was obtained if the first two measurements were greater than 0.5 kg or 0.5 cm apart for body mass and body height, respectively, and the average of the two closest measurements was used for analysis). BMI (kg m−2) was calculated, and BMI z‐scores were computed using age‐specific and sex‐specific reference data from the World Health Organization 19. Participants were classified as obese if the BMI z‐score was greater than +2 standard deviations 19. BMI (kg m‑2), per cent body fat (bioelectrical impedance) and waist circumference (cm) were also assessed in ISCOLE 7, and these continuous variables were used for sensitivity analyses.
Statistical analysis
Statistical analyses were performed using R version 3.4.1 (The R Foundation for Statistical Computing, Vienna, Austria) and JMP version 13 (SAS Institute, Cary, NC, USA) for this ecologic study performed at the country level. Descriptive characteristics of participants were computed by study site. Pearson correlation coefficients between movement behaviour inequality (Gini coefficients) and obesity prevalence were calculated. Average daily movement behaviours (h d−1) were also correlated with obesity prevalence for each site, and the correlation coefficients between both methods were compared using a Steiger's Z‐test 20. Analyses were conducted for the full study sample and were also stratified by sex (boys vs. girls) and income level (high‐income vs. low/middle‐income countries). Finally, the proportion of variability explained by the sex gap in the different movement behaviours was computed using the r 2 measure, i.e. by regressing movement behaviour inequality (Gini coefficients; y‐axis) on the sex gap in average daily movement behaviour ([boys–girls/boys]) (h d−1; x‐axis). Effect sizes of correlation coefficients were considered small (r = 0.1), medium (r = 0.3) or large (r = 0.5) 21.
Results
Table 1 presents descriptive characteristics of the sample stratified by study site. Obesity prevalence was lowest in Finland (5.4%) and highest in China (24.5%). Kenya (1.20 h d−1) and Finland (1.17 h d−1) had the highest levels of MVPA among ISCOLE sites. Total sedentary time was highest in China (9.5 h d−1), while screen time was highest in Brazil (~4 h d−1). Sleep period time was shortest in Portugal (8.3 h per night) and longest in the UK (9.5 h per night). Inequality for MVPA was highest in Brazil (Gini coefficient of 0.24) and lowest in Canada (Gini coefficient of 0.19). Inequality in screen time was highest in China (Gini coefficient of 0.37) and lowest in Colombia (Gini coefficient of 0.28). There was little inequality in total sedentary time and sleep period time. In the full study sample (all sites combined), the largest inequality in movement behaviours was observed for screen time (Gini coefficient of 0.32; medium inequality), followed by MVPA time (Gini coefficient of 0.21; low inequality), total sedentary time (Gini coefficient of 0.07; low inequality) and sleep period time (Gini coefficient of 0.05; low inequality).
Table 1.
Descriptive characteristics of participants stratified by study site
| Country (site) | Participants (N, % boys) | Obesity* (%) | MVPA (h d−1) | Gini coefficient for MVPA | SED (h d−1) | Gini coefficient for SED | Screen time score (h d−1) | Gini coefficient for screen time | Sleep period time (hours per night) | Gini coefficient for sleep period time |
|---|---|---|---|---|---|---|---|---|---|---|
| Australia (Adelaide) | 451 (46.3) | 10.4 | 1.09 (0.39) | 0.1983 | 8.0 (1.0) | 0.0706 | 3.0 (1.6) | 0.2978 | 9.4 (0.7) | 0.0412 |
| Brazil (Sao Paulo) | 469 (48.6) | 21.5 | 0.99 (0.44) | 0.2422 | 8.4 (1.1) | 0.0759 | 3.9 (2.2) | 0.3155 | 8.6 (0.8) | 0.0545 |
| Canada (Ottawa) | 507 (41.0) | 12.0 | 0.97 (0.32) | 0.1855 | 8.5 (1.0) | 0.0671 | 2.8 (1.8) | 0.3402 | 9.1 (0.8) | 0.0514 |
| China (Tianjin) | 465 (51.4) | 24.5 | 0.74 (0.26) | 0.1962 | 9.5 (1.1) | 0.0641 | 2.2 (1.5) | 0.3727 | 8.8 (0.6) | 0.0409 |
| Colombia (Bogotá) | 822 (49.0) | 5.6 | 1.14 (0.41) | 0.2069 | 8.4 (1.1) | 0.0747 | 3.0 (1.5) | 0.2751 | 8.8 (0.8) | 0.0520 |
| Finland (Helsinki, Espoo, Vantaa) | 461 (45.3) | 5.4 | 1.17 (0.45) | 0.2099 | 8.9 (1.1) | 0.0696 | 3.0 (1.5) | 0.2835 | 8.5 (0.9) | 0.0619 |
| India (Bangalore) | 532 (45.3) | 10.7 | 0.82 (0.35) | 0.2373 | 8.6 (1.1) | 0.0706 | 2.0 (1.2) | 0.3111 | 8.6 (0.7) | 0.0473 |
| Kenya (Nairobi) | 459 (45.3) | 6.8 | 1.20 (0.52) | 0.2395 | 8.3 (1.1) | 0.0737 | 2.5 (1.7) | 0.3714 | 8.6 (0.9) | 0.0551 |
| Portugal (Porto) | 639 (42.9) | 16.4 | 0.93 (0.36) | 0.2113 | 9.3 (1.0) | 0.0598 | 2.5 (1.4) | 0.3022 | 8.3 (0.9) | 0.0576 |
| South Africa (Cape Town) | 453 (39.1) | 10.8 | 1.08 (0.42) | 0.2204 | 8.1 (1.1) | 0.0744 | 3.3 (2.0) | 0.3402 | 9.2 (0.7) | 0.0449 |
| UK (Bath and North East Somerset) | 414 (43.7) | 8.9 | 1.06 (0.38) | 0.1951 | 8.4 (0.9) | 0.0633 | 3.2 (1.6) | 0.2808 | 9.5 (0.7) | 0.0429 |
| USA (Baton Rouge) | 456 (40.2) | 17.5 | 0.83 (0.31) | 0.2093 | 8.7 (1.0) | 0.0665 | 3.4 (2.2) | 0.3471 | 8.9 (0.9) | 0.0545 |
| All sites | 6128 (45.1) | 12.3 | 1.01 (0.41) | 0.2127 | 8.6 (1.1) | 0.0692 | 2.9 (1.8) | 0.3198 | 8.8 (0.9) | 0.0504 |
Obesity defined according to the World Health Organization criteria.
MVPA, moderate‐to‐vigorous physical activity; SED, sedentary time. Data are shown as mean (standard deviation) unless otherwise indicated.
Figure 1a shows the association between average MVPA (h d−1) and obesity prevalence, while Figure 1b shows the association between MVPA inequality (Gini index) and obesity prevalence. Boys and girls have been combined for all analyses because the patterns of associations were very similar and we wanted to improve clarity. Figure 1 clearly shows that average MVPA in hours per day was a better correlate of obesity than MVPA inequality (r = −0.77 vs. r = 0.00, respectively). The difference between correlation coefficients was also significant according to Steiger's Z‐test (p = 0.03). Figure 2 also shows that average total sedentary time (h d−1) was a better correlate of obesity than total sedentary time inequality (r = 0.52 vs. r = −0.32, respectively, and p = 0.05 for the difference according to Steiger's Z‐test). In contrast, Figure 3 shows that the association is stronger for screen time inequality (r = 0.47) compared with average screen time (r = 0.05) for predicting obesity; however, the difference was not significant (p = 0.33). Finally, there was no difference between average sleep period time (r = −0.17) and sleep period time inequality (r = −0.19) for predicting obesity (p = 0.96 with the Steiger's Z‐test) (Figure 4).
Figure 1.
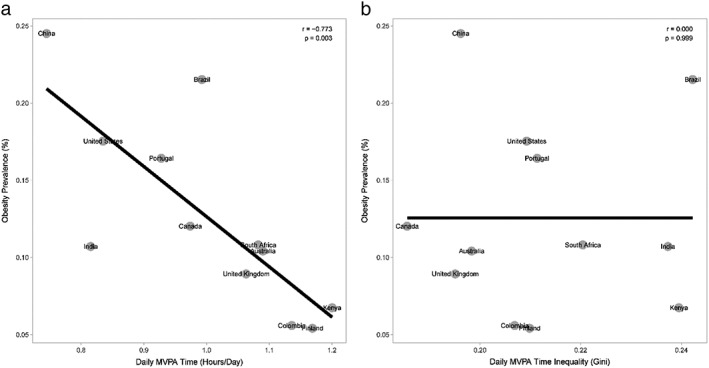
Association between moderate‐to‐vigorous physical activity (MVPA) and obesity. Figure 1a (left panel) shows the correlation between average MVPA and obesity, while Figure 1b (right panel) shows the correlation between MVPA inequality (Gini index) and obesity. Boys and girls are combined for analysis. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.029).
Figure 2.
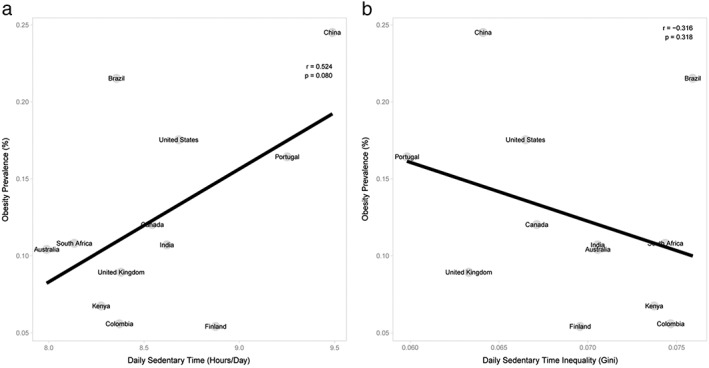
Association between total sedentary time and obesity. Figure 2a (left panel) shows the correlation between average sedentary time and obesity, while Figure 2b (right panel) shows the correlation between sedentary time inequality (Gini index) and obesity. Boys and girls are combined for analysis. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.054).
Figure 3.
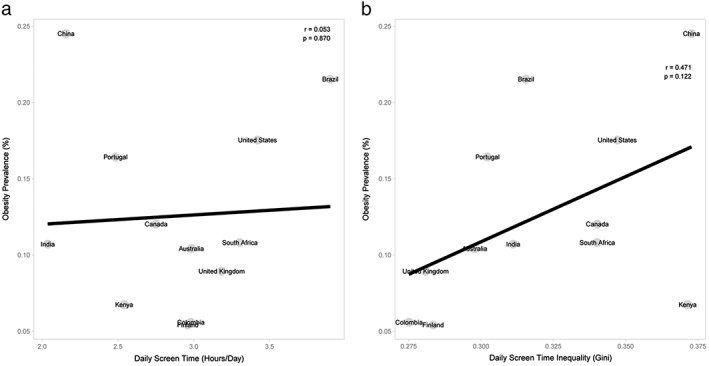
Association between screen time and obesity. Figure 3a (left panel) shows the correlation between average screen time and obesity, while Figure 3b (right panel) shows the correlation between screen time inequality (Gini index) and obesity. Boys and girls are combined for analysis. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.331).
Figure 4.
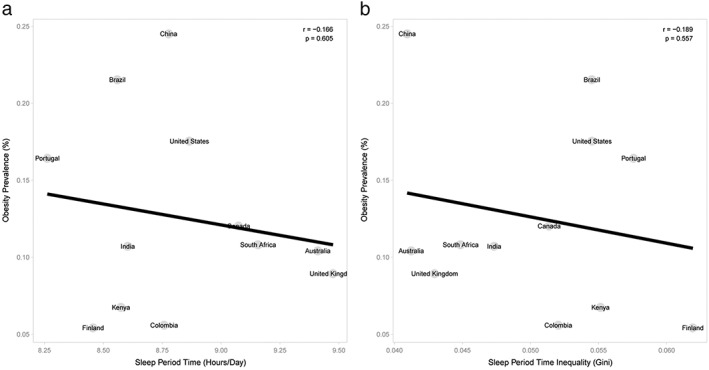
Association between sleep period time and obesity. Figure 4a (left panel) shows the correlation between average sleep period time and obesity, while Figure 4b (right panel) shows the correlation between sleep period time inequality (Gini index) and obesity. Boys and girls are combined for analysis. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.965).
The associations between movement behaviours and obesity were also examined by country‐level World Bank classification of economic development (high‐income countries [Australia, United States, Canada, Finland, United Kingdom, Portugal] vs. low/middle‐income countries [Kenya, India, South Africa, China, Colombia, Brazil]) (Figures S1–S4). Figure S1 (right panel) shows that obesity was associated with greater MVPA inequality in high‐income countries while it was associated with lower MVPA inequality in low/middle‐income countries (although not to a significant extent due to the small sample size in each group) (p = 0.007 with the Steiger's Z‐test for the r comparison in the high‐income country group). Figure S2 shows inverse associations for average sedentary time and sedentary time inequality; longer average sedentary time (h d−1) was associated with obesity, while greater sedentary time inequality was associated with lower obesity prevalence in both groups (p = 0.09 with the Steiger's Z‐test for the r comparison in low/middle‐income country group). No differences were observed for screen time (Figure S3) or sleep period time (Figure S4).
The proportion of variability explained by the sex gap in the different movement behaviours was calculated using the r 2 measure (as described previously). It was observed that 29% (MVPA), 0.4% (sedentary time), 0.2% (screen time) and 11% (sleep period time) of inequality were explained by the sex gap. This means that MVPA in girls is disproportionally lower in countries with higher MVPA inequality (Figure S5). The relative sex gap ranges from 0.18 (Canada) to 0.38 (India).
Sensitivity analyses revealed that using total physical activity time (light, moderate and vigorous combined) or steps per day resulted in similar results as MVPA; hence, only MVPA was used for the present paper. Likewise, using average BMI, per cent body fat or waist circumference (continuous measures) resulted in similar findings to using obesity prevalence (data not shown). Finally, using the MVPA threshold of Treuth et al. 22 rather than the Evenson et al. 11 threshold, or the Centers for Disease Control and Prevention 23 or the International Obesity Task Force 24 cut‐points for obesity instead of the WHO threshold 19, resulted in similar patterns of associations (data not shown).
Discussion
To our knowledge, the present study was the first to examine whether inequality in different movement behaviours was a better correlate of obesity prevalence than average movement behaviour volume in children. Several key findings emerged from this study. First, it was found that the largest inequality in movement behaviours was observed for screen time (Gini coefficient of 0.32; medium inequality), followed by MVPA time (Gini coefficient of 0.21; low inequality), total sedentary time (Gini coefficient of 0.07; low inequality) and sleep period time (Gini coefficient of 0.05; low inequality). Second, and in contrast to our hypothesis, it was found that average MVPA and sedentary time (h d−1) were better correlates of obesity than MVPA and sedentary time inequality (Gini index). Third, differences in patterns of associations between MVPA/sedentary time and obesity were observed according to country‐level World Bank classifications of economic development (high‐income countries vs. low/middle‐income countries). Finally, associations were similar for boys and girls and with the use of other measures of adiposity; however, MVPA in girls was found to be disproportionally lower in countries with higher MVPA inequality.
The observation that average MVPA time and sedentary time were more predictive of obesity than inequality in these movement behaviours is in contrast to our hypothesis that was based on a recent paper by Althoff et al. 6 involving mainly adults. Although they only used steps per day as the measure of physical activity in their study, they reported that inequality in activity (assessed using smartphones) was a better correlate of obesity than average activity volume. The relationships with steps per day were also explored in the present study (sensitivity analysis), and results were similar to those reported for MVPA. Several aspects can explain these discrepant findings. For example, ISCOLE only included 12 countries (smaller sample size) and included children from urban/suburban areas that were not necessarily representative of the whole country. Furthermore, the variability in Gini coefficients was larger in the Althoff et al. study (the Gini coefficients for step count ranged from 0.22 to 0.32 in their study compared with 0.11 to 0.17 in the present study). However, the findings are not directly comparable because their study was mainly composed of adults who were smartphone owners. Additionally, the present study adds important knowledge by adding other movement behaviours (not only step count) and by having several objective measures of adiposity (not only self‐reported height and weight).
Moderate‐to‐vigorous physical activity is associated with improved health outcomes in children, including adiposity 25. Global physical activity guidelines call for a minimum of 60 min d−1 in MVPA for health benefits in school‐aged children 26. The present data show that daily MVPA time is strongly and inversely associated with obesity prevalence (r = −0.77). However, while more inequality in screen time was associated with obesity (r = 0.47), less inequality in total sedentary time was associated with obesity (r = −0.32). This inverse pattern could be explained by the low Gini coefficients for total sedentary behaviour that limit extrapolations to be drawn.
The largest inequality in movement behaviours in ISCOLE was observed for screen time (Gini coefficient of 0.32; medium inequality), followed by MVPA (Gini coefficient of 0.21; low inequality), total sedentary time (Gini coefficient of 0.07; low inequality) and sleep period time (Gini coefficient of 0.05; low inequality). This means that there is less variability in sleep and sedentary time than screen time and MVPA. While sleep and non‐screen sedentary behaviour (e.g. homework) are obligatory daily activities, screen‐based sedentary behaviour and MVPA are discretionary activities that can greatly vary between individuals. From a public health standpoint, intervention strategies that aim to increase MVPA and decrease screen time by reducing the inequality gap are thus important to achieve.
Differences in patterns of associations between MVPA and/or sedentary time and obesity by country‐level World Bank classifications of economic development remind us that public health policies and interventions aimed at improving movement behaviours and health outcomes should be context‐specific and setting‐specific. Intervention strategies aimed at improving movement behaviours in high‐income countries may not necessarily work well in low/middle‐income countries.
Although our findings revealed similar patterns of associations for boys and girls, MVPA in girls was found to be disproportionally lower in countries with higher MVPA inequality; 29% of inequality in MVPA was explained by the sex gap in the present study (compared with 43% in the Althoff et al. study). Part of this difference is likely due to the fact that the Althoff et al. study was based on smartphones while the present study used waist‐worn accelerometers. Many women carry their phone in their handbag, not on their body, so steps per day as measured by smartphones can be systematically undercounted in many women. While lower MVPA levels in girls compared with boys have been reported in several countries 1, 27, the sex gap in MVPA is amplified in countries with low MVPA levels and higher MVPA inequality. This suggests that MVPA inequality could be greatly reduced through increases in girls' MVPA alone, or alternatively that girls' MVPA might be increased differentially by population‐level strategies.
This study has several strengths and limitations. An important strength is the multinational sample of children from low‐income to high‐income countries across several regions of the world. A highly standardized measurement protocol and a rigorous quality control program were also used to ensure high‐quality data across all sites 7. Movement behaviours were accelerometer‐determined using an established 24‐h waist‐worn protocol 8, and objective indicators of adiposity were used. However, the present results need to be interpreted in light of the following limitations. First, the cross‐sectional nature of the data precludes inferences about causality. Second, a larger number of countries for this ecologic study performed at the country level would have provided more statistical power for some of the associations reported. Third, self‐reported measures of screen time were used, which are prone to social desirability responding and recall bias. Fourth, ISCOLE was not designed to provide nationally representative data, thereby limiting generalizability. Fifth, the narrow age range limits extrapolation of results to other age groups. Finally, the possibility that the observed associations are confounded by unmeasured variables is always a possibility in epidemiology.
In conclusion, findings from this study show that the largest inequality in movement behaviours was observed for screen time and MVPA in this multinational study of children. Still, obesity was better predicted by average MVPA and average total sedentary time than by inequality in these movement behaviours. Finally, some differences in patterns of associations were observed between MVPA/sedentary time and obesity when stratified by country‐level of economic development, and MVPA in girls was found to be disproportionally lower in countries with higher MVPA inequality.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Author Contributions
J.‐P. C. conceptualized and designed the study, carried out the statistical analyses and drafted the manuscript. J. D. B. carried out the statistical analyses and produced the figures. M. S. T., M. F., G. H., E. V. L., C. M., J. M., T. O., V. O., O. L. S., M. S. and C. T.‐L. conceptualized and designed the study. P. T. K. obtained funding and conceptualized and designed the study. All authors critically revised the manuscript, approved the final manuscript as submitted and agree to be accountable for all aspects of the work. J.‐P. C., J. D. B. and P. T. K. had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Supporting information
Figure S1. Association between moderate‐to‐vigorous physical activity (MVPA) and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average MVPA and obesity while the right panel shows the correlation between MVPA inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.007 for the comparison in high‐income countries and p = 0.418 for the comparison in low/middle‐income countries).
Figure S2. Association between total sedentary behavior and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average sedentary behavior and obesity while the right panel shows the correlation between sedentary behavior inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.273 for the comparison in high‐income countries and p = 0.086 for the comparison in low/middle‐income countries).
Figure S3. Association between screen time and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average screen time and obesity while the right panel shows the correlation between screen time inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.272 for the comparison in high‐income countries and p = 0.738 for the comparison in low/middle‐income countries).
Figure S4. Association between sleep period time and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average sleep period time and obesity while the right panel shows the correlation between sleep period time inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.686 for the comparison in high‐income countries and p = 0.661 for the comparison in low/middle‐income countries).
Figure S5. Association between the sex gap in average moderate‐to‐vigorous physical activity (MVPA) and MVPA inequality. The proportion of variability explained by the sex gap in average MVPA was 29%, indicating that MVPA in girls is disproportionally lower in countries with high MVPA inequality (such as Brazil, India, Kenya and South Africa).
Acknowledgements
We wish to thank the ISCOLE External Advisory Board, ISCOLE participants and their families, and the ISCOLE Research Group. ISCOLE was funded by The Coca‐Cola Company. With the exception of requiring that the study be global in nature, the funder had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and decision to submit the manuscript for publication.
Chaput, J.‐P. , Barnes, J. D. , Tremblay, M. S. , Fogelholm, M. , Hu, G. , Lambert, E. V. , Maher, C. , Maia, J. , Olds, T. , Onywera, V. , Sarmiento, O. L. , Standage, M. , Tudor‐Locke, C. , and Katzmarzyk, P. T. (2018) Inequality in physical activity, sedentary behaviour, sleep duration and risk of obesity in children: a 12‐country study. Obesity Science & Practice, 4: 229–237. doi: 10.1002/osp4.271.
References
- 1. Hallal PC, Andersen LB, Bull FC, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet 2012; 380: 247–257. [DOI] [PubMed] [Google Scholar]
- 2. Carson V, Hunter S, Kuzik N, et al. Systematic review of sedentary behaviour and health indicators in school‐aged children and youth: an update. Appl Physiol Nutr Metab 2016; 41: S240–S265. [DOI] [PubMed] [Google Scholar]
- 3. Chaput JP, Gray CE, Poitras VJ, et al. Systematic review of the relationships between sleep duration and health indicators in school‐aged children and youth. Appl Physiol Nutr Metab 2016; 41: S266–S282. [DOI] [PubMed] [Google Scholar]
- 4. Tremblay MS, Barnes JD, González SA, et al. Global Matrix 2.0: report card grades on the physical activity of children and youth comparing 38 countries. J Phys Act Health 2016; 13: S343–S366. [DOI] [PubMed] [Google Scholar]
- 5. Galland BC, Taylor BJ, Elder DE, Herbison P. Normal sleep patterns in infants and children: a systematic review of observational studies. Sleep Med Rev 2012; 16: 213–222. [DOI] [PubMed] [Google Scholar]
- 6. Althoff T, Sosič R, Hicks JL, King AC, Delp SL, Leskovec J. Large‐scale physical activity data reveal worldwide activity inequality. Nature 2017; 547: 336–339. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Katzmarzyk PT, Barreira TV, Broyles ST, et al. The International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE): design and methods. BMC Public Health 2013; 13: 900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Tudor‐Locke C, Barreira TV, Schuna JM Jr, et al. Improving wear time compliance with a 24‐hour waist‐worn accelerometer protocol in the International Study of Childhood Obesity, Lifestyle and the Environment (ISCOLE). Int J Behav Nutr Phys Act 2015; 12: 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Tudor‐Locke C, Barreira TV, Schuna JM Jr, Mire EF, Katzmarzyk PT. Fully automated waist‐worn accelerometer algorithm for detecting children's sleep‐period time separate from 24‐h physical activity or sedentary behaviors. Appl Physiol Nutr Metab 2014; 39: 53–57. [DOI] [PubMed] [Google Scholar]
- 10. Barreira TV, Schuna JM Jr, Mire EF, et al. Identifying children's nocturnal sleep using a 24‐h waist accelerometry. Med Sci Sports Exerc 2015; 47: 937–943. [DOI] [PubMed] [Google Scholar]
- 11. Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci 2008; 26: 1557–1565. [DOI] [PubMed] [Google Scholar]
- 12. U.S. Centers for Disease Control and Prevention . Youth Risk Behavior Surveillance System (YRBSS). 2012. Available at http://www.cdc.gov/HealthyYouth/yrbs/. Accessed March 28, 2018.
- 13. Chaput JP, Katzmarzyk PT, LeBlanc AG, et al. Associations between sleep patterns and lifestyle behaviors in children: an international comparison. Int J Obes Suppl 2015; 5: S59–S65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lubans DR, Hesketh K, Cliff DP, et al. A systematic review of the validity and reliability of sedentary behaviour measures used with children and adolescents. Obes Rev 2011; 12: 781–799. [DOI] [PubMed] [Google Scholar]
- 15. Schmitz KH, Harnack L, Fulton JE, et al. Reliability and validity of a brief questionnaire to assess television viewing and computer use by middle school children. J Sch Health 2004; 74: 370–377. [DOI] [PubMed] [Google Scholar]
- 16. Atkinson AB. On the measurement of inequality. J Econ Theory 1970; 2: 244–263. [Google Scholar]
- 17. Allison PD. Measures of inequality. Am Sociol Rev 1978; 43: 865–880. [Google Scholar]
- 18. De Maio FG. Income inequality measures. J Epidemiol Community Health 2007; 61: 849–852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. de Onis M, Onyanga AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school‐aged children and adolescents. Bull World Health Organ 2007; 85: 660–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Steiger JH. Tests for comparing elements of a correlation matrix. Psychol Bull 1980; 87: 245–251. [Google Scholar]
- 21. Cohen J. Statistical Power Analysis for the Behavioral Sciences, 2nd edn. Lawrence Earlbaum Associates: Hillsdale, NJ, 1988. [Google Scholar]
- 22. Treuth MS, Schmitz K, Catellier DJ, et al. Defining accelerometer thresholds for activity intensities in adolescent girls. Med Sci Sports Exerc 2004; 36: 1259–1266. [PMC free article] [PubMed] [Google Scholar]
- 23. Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC growth charts for the United States: methods and development. National Center for Health Statistics. Vital Health Stat 2002; 11: 1–190. [PubMed] [Google Scholar]
- 24. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ 2000; 320: 1240–1243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Poitras VJ, Gray CE, Borghese MM, et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school‐aged children and youth. Appl Physiol Nutr Metab 2016; 41: S197–S239. [DOI] [PubMed] [Google Scholar]
- 26. World Health Organization . Global Recommendations on Physical Activity for Health. World Health Organization: Geneva, Switzerland, 2010, p. 58. [PubMed] [Google Scholar]
- 27. Brown WJ, Mielke GI, Kolbe‐Alexander TL. Gender equality in sport for improved public health. Lancet 2016; 388: 1257–1258. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1. Association between moderate‐to‐vigorous physical activity (MVPA) and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average MVPA and obesity while the right panel shows the correlation between MVPA inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.007 for the comparison in high‐income countries and p = 0.418 for the comparison in low/middle‐income countries).
Figure S2. Association between total sedentary behavior and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average sedentary behavior and obesity while the right panel shows the correlation between sedentary behavior inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.273 for the comparison in high‐income countries and p = 0.086 for the comparison in low/middle‐income countries).
Figure S3. Association between screen time and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average screen time and obesity while the right panel shows the correlation between screen time inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.272 for the comparison in high‐income countries and p = 0.738 for the comparison in low/middle‐income countries).
Figure S4. Association between sleep period time and obesity stratified by country‐level World Bank classification of economic development. The left panel shows the correlation between average sleep period time and obesity while the right panel shows the correlation between sleep period time inequality (Gini index) and obesity. Boys and girls are combined for analysis. High‐income countries include Australia, United States, Canada, Finland, United Kingdom and Portugal while low/middle‐income countries include Kenya, India, South Africa, China, Colombia and Brazil. Correlation coefficients were compared using a Steiger's Z‐test (p = 0.686 for the comparison in high‐income countries and p = 0.661 for the comparison in low/middle‐income countries).
Figure S5. Association between the sex gap in average moderate‐to‐vigorous physical activity (MVPA) and MVPA inequality. The proportion of variability explained by the sex gap in average MVPA was 29%, indicating that MVPA in girls is disproportionally lower in countries with high MVPA inequality (such as Brazil, India, Kenya and South Africa).