

Summary
Women’s decision-making autonomy has been poorly studied in most developing countries. The few existing studies suggest that it is closely linked to women’s socio-demographic characteristics and the social settings in which they live. This study examined Nigerian women’s perceived decision-making autonomy about their own health care using nationally representative data from the 2013 Nigerian Demographic and Health Survey. The study sample consisted of 27,135 women aged 15–49 years who lived with their husbands/partners. Responses to questions about who usually makes decisions about the respondent’s health care were analysed. Factors associated with women’s health care decision-making were investigated using logistic regression models. Only 6.2% of the women reported making their own decisions about health care. For most women (61.1%), this decision was made by their husband/partner alone and 32.7% reported joint decision-making with their husband/partner. Factors independently associated with decision-making by the woman included: geographical region, rural/urban residence, age, education, religion, wealth index, occupation, home ownership and husband’s occupation. A strong association between women making their own health care decision was seen with region of residence (χ2 = 3221.48, p < 0.0001), even after controlling for other factors. Notably, women from the South West region were 8.3 times more likely to make their own health care decisions than women from the North West region. Factors that were significantly associated with joint health care decision-making were also significantly associated with decision-making by the woman alone. The study found that individual-level factors were significantly associated with Nigerian women’s decision-making autonomy, as well as other factors, in particular geographic region. The findings provide an important perspective on women’s health care decision-making autonomy in a developing country.
Introduction
Women’s autonomy – their opportunity to make choices that affect their lives – is an important factor in demographic, economic and health-related outcomes (Fikree & Pasha, 2004). Studies of women’s autonomy related to health care decision-making report definitions and measures of autonomy that encompass similar dimensions: the ability to obtain information and make decisions about one’s own concerns, have some control over finances and have some freedom of movement. A woman who can exercise personal autonomy to make decisions is able to improve and maintain her health and seek necessary health-related resources (Fikree & Pasha, 2004). In studies on reproductive behaviour, women’s active participation in decision-making indicates their power within the household. It increases their adoption of modern contraceptives and reduces their desired fertility (Mason, 1987; Balk, 1994).
The few studies of women’s decision-making autonomy in developing countries suggest a close link to women’s socio-demographic characteristics and the social settings in which they live. For instance, highly educated women are more likely to be knowledgeable about their own health, have more self-confidence and be more assertive than those with less or no education (Singh et al., 2014). These authors concluded that without education and at least a certain amount of wealth, it is difficult for an individual woman to make choices. Age and family structure are strong determinants of women’s authority in rural Pakistan – older women and women in nuclear households were more likely to participate in family decisions (Sathar & Kazi, 1997). The older a woman is, the more likely she is to have negotiating skills and self-confidence leading to decision-making autonomy (Kritz & Makinwa-Adebusoye, 1999). According to Nigatu and colleagues (Nigatu et al., 2014), women in south-east Ethiopia with higher household monthly income were more likely to be autonomous. Similarly, poverty, distance to health care services and lack of education exacerbated low levels of women’s autonomy in northern Kenya (Brunson et al., 2009). Women with more children tend to have greater decision-making autonomy (Gage, 1995; Morgan & Niraula, 1995; Kritz & Makinwa-Adebusoye, 1999). Similarly, employed women are more likely to participate in decision-making than unemployed women (Bloom et al., 2001; Acharya et al., 2010). Couples living in urban areas were more likely to jointly make reproductive decisions than rural residents (Feyisetan, 2000). Being a Muslim woman in Nigeria is associated with lower decision-making power (Kritz & Makinwa-Adebusoye, 1999), and religion represents an important aspect of Nigerian family life (Ojo, 1997). Little is known about other socio-demographic characteristics associated with women’s autonomous decision-making in Nigeria.
Nigeria is the most populous country in sub-Saharan Africa and the tenth most populated country in the world. Its estimated population of 162 million (National Population Commission, 2007) is spread across more than 250 ethnic groups. Given the association of women’s autonomy with several health outcomes, it is essential to have a better understanding of the perceived decision-making autonomy of Nigerian women and the factors associated with their decision-making autonomy. Nigeria is particularly desirable for studying factors that affect women’s autonomous decision-making because its great diversity provides an opportunity to disentangle various factors. For example, Nigeria has multiple religions with Christianity and Islam being the dominant religions, it is divided into six regions reflecting geo-political groupings and has a wide range of education and income levels. How these factors influence women’s decision-making autonomy for their own health care is poorly studied in Nigeria. Furthermore, a study of Nigeria may serve as a case study for similar diverse countries in sub-Saharan Africa. This study aimed to utilize empirical evidence from nationally representative data to systematically describe women’s self-reported health care decision-making autonomy and associated socio-demographic factors. Specifically, it describes Nigerian women’s responses to the Nigerian Demographic and Health Survey (NDHS) question ‘Who usually makes decisions about health care for yourself?’ as an indicator of decision-making autonomy about their own health care and the factors independently associated with their responses.
The study hypotheses were that: i) there are regional differences in Nigerian women’s decision-making autonomy about their own health care, as indicated by the NDHS question; ii) socio-demographic and other factors (including region of country, urban/rural residence, respondent’s age, education, religion, wealth index, employment status, occupation, type of marriage, husband/partner’s education, husband/partner’s occupation) are independently associated with Nigerian women’s decision-making autonomy about their own health care.
Methods
Data
Data were from the 2013 NDHS, a nationally representative study of socioeconomic characteristics, reproductive patterns and health behaviours of reproductive-age women (aged 15–49 years) in Nigeria. The survey was locally implemented by the Nigerian National Population Commission (NPC) but funded by various international bodies including the US Agency for International Development (USAID), the UK Department for International Development (DFID) and the United Nations Population Fund (UNFPA). The relevant data for this project, including individual characteristics, husband/partner’s characteristics and measures of women’s autonomy, were captured in the 2013 NDHS women’s individual dataset.
A total of 38,948 women aged 15–49 years were surveyed in the 2013 NDHS. Eligible participants for this analysis included women who: (1) were married or had a partner; (2) were living with their husband/partner at the time of interview; and (3) answered the question about who usually decides about respondent’s health care. Overall, 27,217 women met these criteria. Respondents who answered ‘other’ (n = 64) or ‘someone else’ (n = 18) to the decision-making question were excluded, leaving a final unweighted sample size of 27,135.
Outcome variable
The outcome variable was ‘women’s decision-making for their own health care’. This was the response to the question: ‘Who usually makes decisions about health care for yourself?’ Possible responses were: ‘[respondent] alone’; ‘husband/partner alone’; ‘[respondent] and husband/partner jointly.’ Women who answered ‘husband/partner alone’ were considered to have the least autonomy of the three groups. This group of women was contrasted with those whose response was ‘respondent alone’ and, in a separate comparison, with women whose response was ‘respondent and husband/partner jointly’, since the dynamics of autonomy represented by women reporting sole decision-making may differ from those reporting joint decision-making with husband/partner.
Variables associated with women’s health care decision-making autonomy
Variables investigated for association with women’s response to the question about health care decision-making included: region of country, rural/urban residence, respondent’s age, education, religion, exposure to the mass media (print and electronic), ownership of house, ownership of land, wealth index, currently working, occupation, type of marriage, number of children and age gap between respondent and husband/partner. Certain socio-demographic characteristics of the husband/partner were also examined, including husband/partner’s education and occupation. The NDHS wealth index was a composite derived measure of a household’s cumulative living standard and relative wealth, calculated using data on a household’s ownership of selected assets, including televisions and bicycles; materials for housing construction; and types of water access and sanitation facilities. The resulting index was then presented in ordered categories: ‘poorest’, ‘poorer’, ‘middle’, ‘richer’ and ‘richest’.
For the purpose of statistical modelling, several variables were re-coded into two groups, including: (1) respondent’s age: 15–34 years (coded as 0) and 35–49 years (coded as 1); (2) type of marriage: monogamy (coded as 1) and polygamy (one or more co-wives) (coded as 0); (3) house or land ownership: 1 for women who owned such property and 0 for those who did not; (4) place of residence: rural (coded as 0) or urban (coded as 1). Other variables were indexed as follows. Education was represented by three indicator variables, with women with no education as the reference group and primary, secondary and higher education as the other categories. Respondent’s religion was coded with Islam as the reference category and Catholic, Other Christian and Traditional/other religion as the other categories. Occupation was categorized as unemployed, non-professional (clerical, sales, agriculture, manual jobs) and professional (professional, technical, managerial), with unemployment as the reference category. Wealth index was represented by four indicator variables with ‘poorest’ as the reference group. Region was encoded into five categorical variables with the North West region as the reference group. Exposure to the media (newspaper, radio and television) variables were each re-coded into two indicator variables with ‘not at all’ as the reference category and ‘less than once a week’ and ‘at least once a week’ as the other categories.
Data management and statistical analysis
Data management and analysis were done using SPSS version 14. The NDHS sample weights were applied in all analyses. The distribution of responses to the autonomy question was explored using univariate statistics and association with socio-demographic variables using bivariate statistics. Multivariate logistic models were used to identify factors independently associated with women’s decision-making autonomy about health care. The first multivariate model evaluated the woman’s sole decision-making about her health care compared with sole decision-making by the husband/partner as the outcome variable and included the following independent variables: region of country, place of residence (rural versus urban), respondent’s age, education, religion, exposure to the mass media (print and electronic), ownership of house, ownership of land, wealth index, currently working, occupation, type of marriage, number of children, age gap with husband/partner, husband/partner’s education and husband/partner’s occupation. The second model had joint decision-making with the respondent’s husband/partner versus sole decision-making by the husband/partner as the outcome variable and the same independent variables as the first model.
Results
Characteristics of respondents
The characteristics of the women included in the study are shown in Table 1. The largest proportions of women (36.2%) were in the North West region. Nearly two-thirds (63.6%) resided in rural areas, only 7.3% had above secondary education, while 48.5% of the women had no formal education and nearly 40% of respondents’ husband/partners had no formal education. The distribution of the women by religion was: 60.5% Muslim, 37.9 % Catholic and other Christian, with only 1.6% of women reporting ‘other religious traditions’. Nearly a quarter (23.1%) of the women belonged to the poorest wealth index.
Table 1.
Distribution of survey respondents by who makes the decision on the respondent’s health care and by socio-demographic characteristics, N = 27,135, NDHS 2013
| Respondent’s characteristic | Percentage of total sample | Percentage by who makes decision on health care
|
||
|---|---|---|---|---|
| Respondent alone | Respondent & husband/partner | Husband/partner alone | ||
| Region | ||||
| North Central | 13.9 | 5.9 | 36.6 | 57.5 |
| North East | 16.8 | 1.7 | 24.8 | 73.5 |
| North West | 36.2 | 1.5 | 14.7 | 83.8 |
| South East | 8.3 | 11.7 | 52.3 | 36.0 |
| South South | 9.7 | 11.1 | 55.0 | 33.9 |
| South West | 15.0 | 16.6 | 56.2 | 27.2 |
| Place of residence | ||||
| Urban | 36.4 | 10.3 | 44.2 | 45.4 |
| Rural | 63.6 | 3.8 | 26.2 | 70.0 |
| Age group | ||||
| 15–34 years | 62.5 | 4.5 | 30.5 | 65.0 |
| 35–49 years | 37.5 | 9.1 | 36.4 | 54.6 |
| Highest educational level | ||||
| No education | 48.5 | 2.0 | 17.1 | 80.9 |
| Primary | 19.2 | 9.3 | 40.2 | 50.4 |
| Secondary | 25.0 | 11.0 | 48.7 | 40.3 |
| Higher | 7.3 | 9.2 | 62.0 | 28.9 |
| Religion | ||||
| Catholic | 8.5 | 9.8 | 51.8 | 38.5 |
| Other Christian | 29.4 | 12.1 | 54.4 | 33.5 |
| Islam | 60.5 | 2.9 | 19.5 | 77.7 |
| Traditionalist/other | 1.6 | 7.9 | 34.6 | 57.5 |
| Exposure to print media | ||||
| No | 84.7 | 5.6 | 28.6 | 65.8 |
| Yes | 15.3 | 9.7 | 55.7 | 34.6 |
| Exposure to radio | ||||
| No | 37.9 | 4.0 | 22.1 | 74.0 |
| Yes | 62.1 | 7.6 | 39.2 | 53.2 |
| Exposure to TV | ||||
| No | 52.4 | 3.1 | 21.8 | 75.1 |
| Yes | 47.6 | 9.7 | 44.7 | 45.7 |
| Owns house | ||||
| No | 79.0 | 6.3 | 31.9 | 61.8 |
| Yes | 21.0 | 5.9 | 35.9 | 58.2 |
| Owns land | ||||
| No | 82.7 | 6.1 | 30.1 | 63.8 |
| Yes | 17.3 | 6.8 | 45.2 | 48.1 |
| Wealth index | ||||
| Poorest | 23.1 | 1.1 | 14.5 | 84.5 |
| Poorer | 21.5 | 3.2 | 22.9 | 73.9 |
| Middle | 17.9 | 7.2 | 33.7 | 59.1 |
| Richer | 18.1 | 9.8 | 41.1 | 49.1 |
| Richest | 19.4 | 11.4 | 56.6 | 32.0 |
| Currently working | ||||
| No | 30.3 | 2.0 | 18.5 | 79.5 |
| Yes | 69.7 | 8.1 | 38.9 | 53.1 |
| Occupation | ||||
| None | 29.1 | 1.8 | 17.8 | 80.4 |
| Professional | 4.6 | 12.1 | 60.9 | 27.0 |
| Non-professional | 66.3 | 7.7 | 37.2 | 55.1 |
| Polygamous marriage | ||||
| No | 66.8 | 6.0 | 38.1 | 55.9 |
| Yes | 33.2 | 6.6 | 21.5 | 71.9 |
More than half of the women (57.8%) said they could not read at all and 28.7% of the women reported not working at the time of the survey. Regarding husband/partner’s occupation, 31.6% were agricultural employees, 19.5% were clerical sales persons and another 19.7% had skilled manual jobs. One-third (33.2%) of women were in polygamous relationships, i.e. had spouses who were concurrently married to other women. Media exposure variables showed that 84.7% reported not reading newspapers or magazines at all, 37.9% did not listen to the radio at all, 52.4% reported not watching television at all while 30.3% said they watched television at least once a week. Among respondents currently working, 60% of the women said they earned less than their husbands. A large proportion (79.0% and 82.7%) of the women in the survey reported that they did not own a house or land, while 21.0% and 17.3% reported owning a house and land, respectively.
Decision-making about health care
Only 6.2% of women reported making their own decisions about health care, while 61.1% reported that health care decisions were made by husbands/partners alone and 32.7% that health care decisions were made jointly. The distribution of responses for who makes decisions about the respondent’s health care by socio-demographic characteristics is shown in Table 1. There were considerable and significant differences in who makes the decision about the woman’s health care by region (Fig. 1) (χ2 = 6253.01, df = 10, p < 0.001). Only 1.5% of women in the North West region made their own health care decisions, and 16.6% in the South West region, while the proportion of women for whom husbands/partners made the decision alone ranged from 27.2% in the South West to 83.8% in the North West.
Fig. 1.
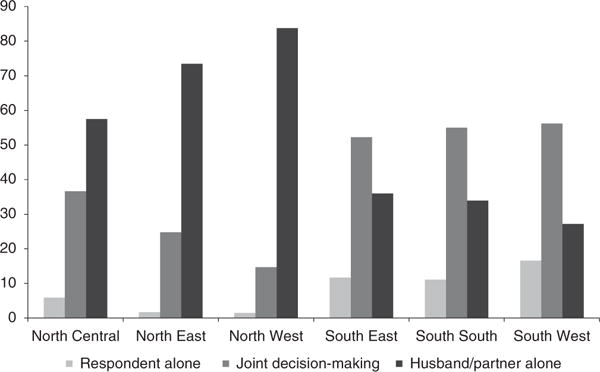
Who usually decides on respondent’s health care by geographical region, NDHS 2013.
Factors associated with women making decisions alone about their health care
The results of the logistic models used to identify factors associated with the question ‘Who usually makes decisions about health care for yourself?’ are shown in Table 2. Factors that were independently and significantly associated with woman making the decision alone included: region, rural/urban residence, respondent’s age, education, religion, wealth index and occupation, as well as ownership of home and husband’s occupation. The latter two variables were negatively associated with women making health care decisions alone. On the other hand, factors that were not independently associated included the respondent’s exposure to print media, radio or television, whether currently working, land ownership, number of children, age gap between husband/partner and husband/partner’s education.
Table 2.
Factors associated with respondent making decisions alone and jointly with her husband/partner on her own health care compared with husband/partner making the decision alone, NDHS 2013
| Variable | Decision-making by woman alone
|
Joint decision-making
|
||||||
|---|---|---|---|---|---|---|---|---|
| Coeff. | p-value | OR | 95%CI | Coeff. | p-value | OR | 95%CI | |
| Region | ||||||||
| North West (Ref.) | ||||||||
| North East | 0.25 | ns | 1.28 | 0.96–1.71 | 0.8.0 | <0.001 | 2.22 | 2.02–2.45 |
| North Central | 1.08 | <0.001 | 2.93 | 2.29–3.75 | 0.69 | <0.001 | 1.99 | 1.79–2.22 |
| South East | 1.34 | <0.001 | 3.81 | 2.9–5.01 | 0.72 | <0.001 | 2.05 | 1.78–2.37 |
| South South | 1.40 | <0.001 | 4.06 | 3.1–5.33 | 0.84 | <0.001 | 2.31 | 2.02–2.65 |
| South West | 2.12 | <0.001 | 8.30 | 6.6–10.44 | 1.27 | <0.001 | 3.56 | 3.18–3.99 |
| Place of residence (urban vs rural) | 0.43 | <0.001 | 1.54 | 1.33–1.78 | 0.00 | ns | 1.00 | 0.92–1.09 |
| Age ≥35 years | 0.61 | <0.001 | 1.83 | 1.59–2.11 | 0.21 | <0.001 | 1.23 | 1.14–1.33 |
| Education | ||||||||
| No education (Ref.) | ||||||||
| Primary | 0.53 | <0.001 | 1.70 | 1.38–2.09 | 0.22 | <0.001 | 1.25 | 1.13–1.38 |
| Secondary | 0.66 | <0.001 | 1.94 | 1.54–2.43 | 0.27 | <0.001 | 1.31 | 1.16–1.47 |
| Higher | 0.45 | 0.01 | 1.57 | 1.12–2.22 | 0.46 | <0.001 | 1.58 | 1.31–1.90 |
| Religion | ||||||||
| Islam (Ref.) | ||||||||
| Catholic | 0.95 | <0.001 | 2.58 | 2.05–3.25 | 0.91 | <0.001 | 2.49 | 2.19–2.82 |
| Other Christian | 0.85 | <0.001 | 2.35 | 1.98–2.77 | 0.85 | <0.001 | 2.33 | 2.13–2.55 |
| Traditional/other | 0.92 | 0.001 | 2.50 | 1.48–4.22 | 0.75 | <0.001 | 2.12 | 1.60–2.80 |
| Exposure to print media | 0.06 | ns | 1.06 | 0.9–1.25 | 0.16 | 0.002 | 1.17 | 1.06–1.30 |
| Exposure to radio | −0.11 | ns | 0.90 | 0.77–1.05 | 0.37 | <0.001 | 1.45 | 1.34–1.56 |
| Exposure to TV | 0.05 | ns | 1.05 | 0.89–1.25 | −0.24 | <0.001 | 0.78 | 0.72–0.86 |
| Ownership of house | −0.53 | <0.001 | 0.59 | 0.5–0.69 | −0.52 | <0.001 | 0.60 | 0.55–0.65 |
| Ownership of land | −0.08 | ns | 0.93 | 0.78–1.1 | 0.39 | <0.001 | 1.48 | 1.35–1.63 |
| Wealth index | ||||||||
| Poorest (Ref.) | ||||||||
| Poorer | 0.45 | 0.003 | 1.57 | 1.16–2.12 | 0.21 | <0.001 | 1.24 | 1.12–1.37 |
| Middle | 0.79 | <0.001 | 2.20 | 1.62–2.97 | 0.43 | <0.001 | 1.54 | 1.37–1.73 |
| Richer | 0.79 | <0.001 | 2.21 | 1.6–3.06 | 0.50 | <0.001 | 1.65 | 1.44–1.89 |
| Richest | 0.88 | <0.001 | 2.42 | 1.71–3.43 | 0.86 | <0.001 | 2.36 | 2.01–2.76 |
| Currently working | 0.07 | ns | 1.08 | 0.7–1.66 | 0.16 | ns | 1.18 | 0.95–1.46 |
| Occupation | ||||||||
| Unemployed (Ref.) | ||||||||
| Professional | 1.35 | <0.001 | 3.84 | 2.28–6.49 | 0.70 | <0.001 | 2.02 | 1.54–2.63 |
| Non-professional | 1.04 | <0.001 | 2.83 | 1.8–4.45 | 0.64 | <0.001 | 1.89 | 1.52–2.34 |
| Polygamous marriage | 0.60 | <0.001 | 1.82 | 1.58–2.09 | −0.19 | <0.001 | 0.83 | 0.77–0.89 |
| Number of children | 0.01 | ns | 1.01 | 0.98–1.05 | −0.01 | ns | 0.99 | 0.97–1.00 |
| Age gap between respondent and husband/partner | <0.01 | ns | 1.00 | 0.99–1.01 | <0.01 | ns | 1.00 | 0.99–1.00 |
| Husband/partner’s education | ||||||||
| No education (Ref.) | ||||||||
| Primary | 0.15 | ns | 1.17 | 0.94–1.45 | 0.17 | 0.001 | 1.19 | 1.07–1.31 |
| Secondary | 0.15 | ns | 1.17 | 0.93–1.46 | 0.09 | ns | 1.10 | 0.99–1.22 |
| Higher | −0.13 | ns | 0.87 | 0.66–1.15 | −0.07 | ns | 0.93 | 0.81–1.07 |
| Husband/partner’s occupation | ||||||||
| Unemployed (Ref.) | ||||||||
| Professional | −0.72 | <0.001 | 0.48 | 0.33–0.72 | −0.35 | 0.006 | 0.71 | 0.55–0.90 |
| Non-professional | −0.80 | <0.001 | 0.45 | 0.31–0.65 | −0.41 | 0.001 | 0.67 | 0.53–0.84 |
ns, not significant at p<0.05.
The region of the country was significantly associated with the outcome variable (χ2 = 3221.48, p < 0.0001). While women in the North East region did not differ substantially from those in the North West region, women from the South South region were four times more likely than those from the North West, while those from the South West region were 8.3 times more likely, to make their own health care decisions than women in the North West. Older women (above 35 years) were significantly more likely (OR 1.83; 95%CI 1.59–2.11) to make decisions alone compared with younger women. Women’s place of residence also had a strong association; rural women were less likely to make their own decisions (p < 0.001) compared with their urban counterparts (OR 1.54; 95%CI 1.33–1.78).
Education also affected women’s decision-making. Women who had attended secondary school were twice as likely to make their own decisions compared with those with no education, while those with higher and primary education were 1.57 and 1.70 times more likely, respectively, to make decisions alone. Regarding religion, Catholic women and other Christians were more than 2.5 times more likely to make their own health care decisions than Islamic women. Women in polygamous marriages were 1.82 times more likely to be autonomous in decisions-making compared with women in monogamous relationships (OR 1.82; 95%CI 1.58–2.09). The likelihood of women making decisions alone increased monotonically with wealth index. Richer and richest women were 2.21 and 2.42 times, respectively, more likely than the poorest women to make decisions alone. Compared with women with unemployed husbands/partners, women whose husbands/partners were professionals or non-professionals were significantly less likely to make health care decisions alone (OR 0.48, p < 0.001, and OR 0.45, p < 0.001, respectively).
Factors associated with joint decision-making by the woman and her husband/partner on her health care
Table 2 also shows the result of logistic regression done to identify independent variables associated with joint decision-making between the respondent and her husband/partner versus sole decision-making by the husband/partner. Factors significantly associated with joint decision-making included: region, woman’s age, education, religion, exposure to print media, radio or television, ownership of land and house, wealth index, marriage type and husband’s occupation. Unlike significant factors for women who make their own decisions, the coefficient on place of residence (rural vs urban) was not significant, whereas exposure to media and ownership of a house and land were significant. Neither age gap between husband/partner nor number of children was statistically significant for either comparison (Table 2).
Older women were more likely to participate in joint decision-making on their own health care than younger women (OR 1.23; 95%CI 1.14–1.33). Women in the South West region were four times more likely to take part in joint decision-making than women from the North West region. Similarly, women of the Catholic faith and other Christians had higher odds (OR 2.49 and 2.33, respectively) of participating in joint decision-making with their husband/partner compared with women of the Islamic faith.
Listening to radio (OR 1.45; 95%CI 1.34–1.56) and exposure to print media (OR 1.17; 95%CI 1.0) were positive predictors of joint decision-making, while watching television (OR 0.78; 95%CI 0.72–0.86) was negatively associated. Notably, compared with women whose husbands/partners were unemployed, women whose husbands/partners were professionals or non-professionals were significantly less likely to make health care decisions jointly (OR 0.71, p = 0.006, and OR 0.67, p = 0.001, respectively). As wealth index increased, respondents were more likely to make joint decisions with their husband/partner about health care. Women who were in the richest category were 2.36 times more likely to be part of joint decision-making than those in the poorest category. Interestingly, women whose husband/partner had primary education were more likely to participate in joint decision-making (OR 1.19; 95%CI 1.07–1.31) than those whose husbands/partners had no education, while secondary or higher education showed no significant association (Table 2).
Discussion
Women’s decision-making autonomy is constrained in many societies, especially in low-and middle-income countries. Studies of women’s autonomy in developing countries first emerged in the context of reproductive health, women’s nutritional status and child health outcomes (immunization and nutrition) (Gage, 1995; Al Riyami et al., 2004; Becker et al., 2006; Acharya et al., 2010; Thapa & Neihof, 2013). In contrast, few studies (Kritz & Makinwa-Adebusoye, 1999; Enabudoso & Igbarumah, 2012) have focused on women’s decision-making autonomy in the context of their own health care needs that are unrelated to reproductive health.
Three important findings emerged from the present study: (1) health care decisions for women in Nigeria are most often made by their husbands/partners without women’s involvement; (2) many socio-demographic factors were found to be independently associated with Nigerian women’s decision-making autonomy, the strongest of which was region of the country; and (3) socio-demographic factors suggest that joint decision-making between a women and her husband or partner is more similar to a woman making her own decisions about health care, thus suggesting some level of decision-making autonomy.
A low level of women’s decision-making autonomy in Nigeria is vividly illustrated by the observation that only 6% of women in the study sample made their own decisions about health care and one-third (32.7%) made decisions jointly with their husband/partner. For the majority of Nigerian women (61.1%), health care decisions were made by their husband/partner alone. This finding is consistent with studies of nationally representative samples in Asia, which found only a small minority of women (13.4% in Nepal, 17.6% in Bangladesh and 28.1% in India) made decisions alone for their own health care (Senarath & Gunawardena, 2009). In that survey, in the majority of households (72.7%, 54.3% and 48.5% in Nepal, Bangladesh and India, respectively) women’s health care decisions were made without women’s participation, much like what was found in this study in Nigeria. Other studies found a similar pattern. For example, Mistry et al. (2009), in a study in rural India, found that more than half (55.6%) of the women were not involved in decision-making about their own health care. Similarly, Rahman et al. (2014) found that more than one-third (37.3%) of women in a Bangladeshi study were not involved in decision-making about their own health care. Overall, despite differences in study sites, study design and analytic methods, these data are consistent with those of other studies that show that very few women in multiple low- and middle-income countries make their own decisions about health, indicating a prevalent low level of women’s decision-making autonomy regarding their own health care.
Several factors were found to be independently associated with women’s decision-making autonomy in Nigeria, including: region of the country, rural/urban residence, respondent’s age, education, religion, wealth index and occupation, as well as home ownership and husband/partner’s occupation. A recent review of studies of women’s autonomy in low- and middle-income countries found that many of these factors are common correlates of women’s autonomy across multiple societies in Asia and Africa. Reasons for the association of factors such as age, education, occupation, wealth and income with women’s autonomy have been reviewed (Gage, 1995; Meekers & Oladosu, 1996; Oyediran, 1998; Al Riyami et al., 2004; Saleem & Bobak, 2005; Becker et al., 2006; Acharya et al., 2010; Nigatu et al., 2014). The present data found positive associations between decision-making autonomy and wealth index, urban residence and education, as has been reported elsewhere (Acharya et al., 2010; Haque et al., 2012; Nigatu et al., 2014; Lamidi, 2016), and women with no education have less autonomy than those with secondary and higher education. Of note, no relationship was found between decision-making about a woman’s own health care and the woman’s employment status or the number of children she had, once other factors had been controlled for. This is in contrast to previous findings that working women are more likely to participate in decision-making, and the more children women have, the more likely they are to participate in decision-making (Bloom et al., 2001; Acharya et al., 2010).
The strongest association with women’s decision-making autonomy was the region of the country in which they lived. As hypothesized, region was an important determinant of a woman’s decision-making autonomy, even after controlling for individual and household factors. Notably, other studies (Kritz & Makinwa-Adebusoye, 1999; Jejeebhoy & Sathar, 2001; Mistry et al., 2009) have also found that geographic region was significantly and independently associated with women’s autonomy after controlling for other variables. These findings suggest that there are factors associated with geographical region that are not captured by many surveys. For example, a study in India found that women in the southern region of India have more exposure to the outside world, a greater voice in family life and more freedom of movement than do those in the north (Basu, 1992; Jejeebhoy & Sathar, 2001). Such factors were not captured in the DHS instrument used in the present study. In Nigeria, family life is guided by normative principles, institutions and belief systems that derive from ethnicity and culture. Such factors as cultural beliefs and ethnic group are important components of regional variation, and may explain (at least in part) the independent influence of region on women’s autonomy.
A previous study of Nigerian women that specifically set out to study the effects of this noted that ethnicity is a major determinant of whether Nigerian women receive formal education, have a say in selecting their spouses, live with a mother-in-law, work outside the home and control income (Kritz & Makinwa-Adebusoye, 1999). Regions of Nigeria also represent geo-political zones that exhibit differences in history, length of contact with Western education, unequal access to education, the prevalence of Islam and ethnic composition. Indeed, it was recently shown that women’s participation in household decision-making was lower in Nigerian states that introduced Sharia law into secular life (Lamidi, 2016). Thus, there are important community-level factors that shape women’s decision-making autonomy beyond the usual individual-level factors (such as age, education, income and occupation).
Joint decision-making with a husband/partner was examined separately from decisions made by a woman alone about health care. While it is apparent that health care decisions made by the husband/partner alone without the participation of the woman represents the lowest level of decision-making autonomy for the woman, joint decision-making may represent a level of partnership or equality within the couple that is harder to explain in terms of decision-making autonomy. Indeed, it was found that similar factors (age, education, occupation, wealth, religion) were associated with decision-making by the woman alone and jointly with her husband/partner (Figure 2). Secondly, the associated effect sizes were usually in the same direction (and in many cases, similar in magnitude) for decision-making by the woman alone and jointly with husbands/partners. These observations support the notion that joint decision-making by the woman and her husband/partner may not represent a lower level of autonomy for women than decision-making by the woman alone. Joint decision-making deserves further study.
Fig. 2.
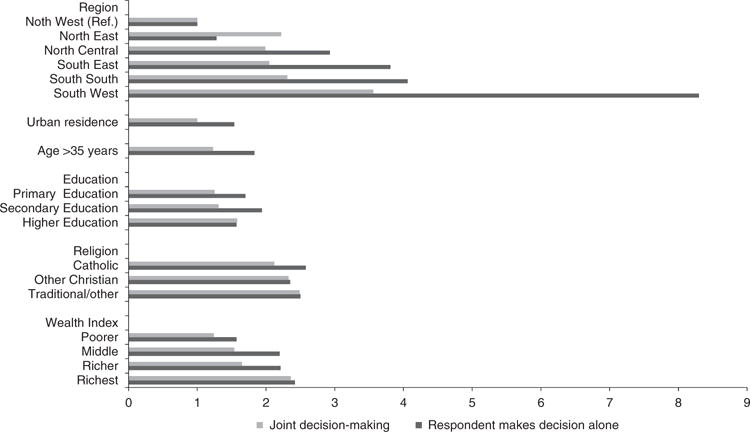
Odds ratios for selected variables independently associated with women making decisions alone about her health care and joint decision-making with her husband/partner.
The study has a number of limitations. This was a secondary analysis of survey data with responses obtained by self-report. This means the responses were subject to recall and reporting bias. Survey questions (especially closed-ended and semi-open-ended items) have limited ability to capture the nuance and context of responses, and preclude clarification of responses through open-ended follow-up questions. For instance, when a woman reports making health care decisions jointly with her husband/partner, it could indicate equity in the relationship or could be an indicator of lower autonomy for the woman because she is not allowed to make such decisions alone. Similarly, although making decisions alone by the woman was interpreted as representing more autonomy, it could indicate lack of support from the husband/partner who would rather not be involved. Without follow-up questions/prompts or qualitative data, it is uncertain which interpretation is appropriate. Further, in common with other surveys, the questions may not have been understood the same way by all participants. While a large number of potential explanatory variables were captured in the survey, some other variables (e.g. woman’s freedom of movement) were not directly captured. Some of these issues could affect the internal validity and/or generalizability of these findings, but a study based on secondary data (such as the present study) has limited ability to control for issues in study design, instruments and/or implementation. Therefore, the data were compared with previous regional or national data from Nigeria (Kritz & Makinwa-Adebusoye, 1999; Lamidi, 2016) and broadly similar findings were found. The responses to another question asking the woman if her need to obtain permission constituted a barrier to seeking health care were also examined, and broadly similar consistency were found with the findings of this study with regards to association with geographical region, income, education and occupation (data not shown). These observations provide confidence for the validity of the findings. At the same time, these data were derived from a nationally representative sample of a large number of women.
A better understanding of factors affecting women’s decision-making autonomy can inform the design and implementation of health programmes and policy. For example, if men wield such power in decision-making for their wives/partner’s health care, the target of health education programmes has to include men. On the other hand, targeting modifiable factors that increase women’s decision-making autonomy (such as education and income) in a community would not only enhance women’s autonomy, but could also lead to better health care outcomes as women gain more control over their lives and health. Factors that are not individual-level factors (such as regional variation) should be taken into account when designing and implementing health programmes. Using this study as an example, a national one-size-fits-all approach is likely to encounter varying degrees of success because of regional variation. Tailoring some health interventions to specific regions may be essential to account for the unique dynamics of health care decision-making of each region.
In conclusion, using data from a large, recent nationally representative survey of Nigerian women, more than half of the women reported that they have no say in decision-making about their own health care. Factors associated with women’s decision-making autonomy included individual-level factors as well as other factors, in particular geographic region. Decision-making varied dramatically between regions in Nigeria even after controlling for other factors, indicating other unmeasured factors that influence decision-making about health care. Future studies are needed to provide context to these findings using qualitative methods, to examine the issue of joint decision-making and evaluate decision-making for different components of health care (such as clinic visits, hospital admissions, surgical procedures or blood transfusions), for which decision-making may differ.
Acknowledgments
The first author is a post-doctoral fellow in the Department of Bioethics, NIH Clinical Center, Bethesda, US. The authors are grateful to the Demographic and Health Surveys (DHS) Program (http://dhsprogram.com/) for providing access to the data. Adebowale Adeyemo provided expertise in data management and analysis, for which the authors are grateful. The authors appreciate the helpful comments and suggestions of Scott Kim on the draft of the manuscript. The opinions expressed are the authors’ alone and do not necessarily reflect the positions or policies of the National Institutes of Health or the US Department of Health and Human Services.
Footnotes
The authors have no conflicts of interest to declare.
References
- Acharya DR, Bell JS, Simkhada P, van Teijlingen ER, Regmi PR. Women’s autonomy in household decision-making: a demographic study in Nepal. Reproductive Health. 2010;7:15. doi: 10.1186/1742-4755-7-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al Riyami A, Afifi M, Mabry RM. Women’s autonomy, education and employment in Oman and their influence on contraceptive use. Reproductive Health Matters. 2004;12:144–154. doi: 10.1016/s0968-8080(04)23113-5. [DOI] [PubMed] [Google Scholar]
- Balk D. Individual and community aspects of women’s status and fertility in rural Bangladesh. Population Studies. 1994;48(1):21–45. [Google Scholar]
- Basu AM. Culture, the Status of Women, and Demographic Behaviour: Illustrated with the Case of India. Clarendon Press; Oxford: 1992. [Google Scholar]
- Becker S, Fonseca-Becker F, Schenck-Yglesias C. Husbands’ and wives’ reports of women’s decision-making power in Western Guatemala and their effects on preventive health behaviours. Social Science & Medicine. 2006;62:2313–2326. doi: 10.1016/j.socscimed.2005.10.006. [DOI] [PubMed] [Google Scholar]
- Bloom SS, Wypij D, Das Gupta M. Dimensions of women’s autonomy and the influence on maternal health care utilization in a north Indian city. Demography. 2001;38:67–78. doi: 10.1353/dem.2001.0001. [DOI] [PubMed] [Google Scholar]
- Brunson EK, Shell-Duncan B, Steele M. Women’s autonomy and its relationship to children’s nutrition among the Rendille of northern Kenya. American Journal of Human Biology. 2009;21:55–64. doi: 10.1002/ajhb.20815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enabudoso E, Igbarumah S. Maternal autonomy on health in a community as assessed by signing of consent for caesarean section and its sociodemographic correlates. Journal of Maternal–Fetal & Neonatal Medicine. 2012;25:1980–1982. doi: 10.3109/14767058.2012.668588. [DOI] [PubMed] [Google Scholar]
- Feyisetan BJ. Spousal communication and contraceptive use among the Yoruba of Nigeria. Population Research and Policy Review. 2000;19:29–45. [Google Scholar]
- Fikree FF, Pasha O. Role of gender in health disparity: the South Asian context. British Medical Journal. 2004;328:823–826. doi: 10.1136/bmj.328.7443.823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gage AJ. Women’s socioeconomic position and contraceptive behaviour in Togo. Studies in Family Planning. 1995;26(5):264–277. [PubMed] [Google Scholar]
- Haque SE, Rahman M, Mostofa MG, Zahan MS. Reproductive health care utilization among young mothers in Bangladesh: does autonomy matter? Womens Health Issues. 2012;22:e171–e180. doi: 10.1016/j.whi.2011.08.004. [DOI] [PubMed] [Google Scholar]
- Jejeebhoy SJ, Sathar ZA. Women’s autonomy in India and Pakistan: the influence of religion and region. Population and Development Review. 2001;27:687–712. [Google Scholar]
- Kritz MM, Makinwa-Adebusoye P. Determinants of women’s decision-making authority in Nigeria: the ethnic dimension. Sociological Forum. 1999;14:399. [Google Scholar]
- Lamidi EO. Multilevel analysis of state variations in women’s participation in household decision-making in Nigeria. Journal of International Women’s Studies. 2016;17:186–201. [Google Scholar]
- Mason KO. The impact of women’s social position on fertility in developing countries. Paper presented at the Sociological Forum. 1987;2(4):718–745. [Google Scholar]
- Meekers D, Oladosu M. Spousal communication and family planning decision-making in Nigeria. Population Research Institute. 1996;3:33. [Google Scholar]
- Mistry R, Galal O, Lu M. Women’s autonomy and pregnancy care in rural India: a contextual analysis. Social Science & Medicine. 2009;69:926–933. doi: 10.1016/j.socscimed.2009.07.008. [DOI] [PubMed] [Google Scholar]
- Morgan SP, Niraula BB. Gender inequality and fertility in two Nepali villages. Population and Development Review. 1995;21(3):541–561. [Google Scholar]
- National Population Commission. The 2006 National Census Report. National Population Commission; Abuja, Nigeria: 2007. [Google Scholar]
- Nigatu D, Gebremariam A, Abera M, Setegn T, Deribe K. Factors associated with women’s autonomy regarding maternal and child health care utilization in Bale Zone: a community based cross-sectional study. BioMed Central Women’s Health. 2014;14:79. doi: 10.1186/1472-6874-14-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ojo MA. Sexuality, marriage and piety among charismatics in Nigeria. Religion. 1997;27:65–79. [Google Scholar]
- Oyediran KA. Changes in womens reproductive health and male involvement in Nigeria: post evaluation findings: 1996-1998. Association for Reproductive and Family Health; Ibadan: 1998. (ARFH Monograph Series No. 2). [Google Scholar]
- Rahman MM, Mostofa MG, Hoque MA. Women’s household decision-making autonomy and contraceptive behaviour among Bangladeshi women. Sexual and Reprod Health. 2014;5:9–15. doi: 10.1016/j.srhc.2013.12.003. [DOI] [PubMed] [Google Scholar]
- Saleem S, Bobak M. Women’s autonomy, education and contraception use in Pakistan: a national study. Reproductive Health. 2005;2:1–8. doi: 10.1186/1742-4755-2-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sathar ZA, Kazi S. Women’s autonomy, livelihood and fertility: a study of rural Punjab. Pakistan Institute of Development Economics [PIDE]; Islamabad, Pakistan: 1997. [Google Scholar]
- Senarath U, Gunawardena NS. Women’s autonomy in decision making for health care in South Asia. Asia Pacific Journal of Public Health. 2009;2:137–143. doi: 10.1177/1010539509331590. [DOI] [PubMed] [Google Scholar]
- Singh K, Singh K, Singh B, Pathak A. Impact of education and autonomy on fertility of women in eastern Uttar Pradesh. Demography India. 2014;31:223–233. [Google Scholar]
- Thapa DK, Niehof A. Women’s autonomy and husbands’ involvement in maternal health care in Nepal. Social Science & Medicine. 2013;93:1–10. doi: 10.1016/j.socscimed.2013.06.003. [DOI] [PubMed] [Google Scholar]