

Abstract
Objective Adherence to antiretroviral therapy (ART) is paramount to successful long-term suppression of human immunodeficiency virus (HIV). For poorly adherent patients with HIV, barriers to remaining adherent may be overcome by the implementation of targeted interventions delivered via mobile devices. This systematic review is focused specifically on mobile phone technologies to deliver adherence interventions in HIV/acquired immunodeficiency syndrome (AIDS) populations.
Methods This review (PROSPERO #CRD42017065131) systematically extracted data from published literature from five databases on mobile phone interventions to improve adherence to ART for HIV. The reported studies had been conducted between 2007 and 2017. Risk of bias was assessed using the Cochrane method ranking each criterion as low, high, or unclear risk of bias.
Results Of the 835 articles returned, we identified 26 randomized controlled trials (RCTs), retrospective and prospective cohort trials, or mixed method studies with a comparison group that fit criteria for inclusion. No standard measure of adherence was consistent throughout the examined studies, and assessments by self-report, pill counting, and medication event monitoring system (MEMS) were utilized. The studies reported mixed results, with 17 reporting significant improvements to adherence, 3 reporting improvements without supplying p -values, and 6 reporting no significant change or a reduction in adherence.
Conclusion The mixed nature of the results exemplifies the need for more comprehensive approaches and larger scale trials to confirm results observed in limited cohort sizes. To better retain satisfactory adherence within the HIV population, and especially in low-resource settings, we recommend that future interventions incorporate multiple strategies: mobile-based reminders, social support structures, and personalized content.
Keywords: HIV, acquired immunodeficiency syndrome, medication adherence, antiretroviral therapy, highly active, mHealth
Background and Significance
A key concern for optimizing treatment of human immunodeficiency virus (HIV) is the adherence to antiretroviral therapy (ART). This paper presents a systematic review of mobile phone technologies to improve HIV medication adherence. There were an estimated 36.7 million people living with HIV (PLWHIV) worldwide in 2015. 1 The impact of HIV/acquired immunodeficiency virus (AIDS) has been particularly hard on countries with limited resources. ART can help people with HIV infection to live longer, healthier lives, but adherence to treatment can be challenging, especially in low-resource settings.
Non-adherence to HIV/AIDS treatment is a significant public health issue. 2 Patients who remain adherent to ART are significantly less likely to transmit an infection to sexual partners; 3 however, the population affected by HIV/AIDS demonstrates a lack of knowledge about the disease, treatment approaches and the importance of strict adherence. 4 Various HIV programs have noted the importance of improving adherence to attain better outcomes. 5 6 7 8
Mobile phone technologies have the potential to promote adherence in these patients. Wireless telecommunications networks have spread rapidly worldwide, and sending text messages on wireless mobile telephones has become an extremely popular means of communication. 5 Mobile phone text messaging, also called short messaging service (SMS), has been explored as an approach to enhancing patient adherence to ART regimens.
Recent systematic reviews have focused on mobile health (mHealth) and adherence not specific to HIV; 9 10 mHealth in low-resource settings, but not specific to HIV adherence; 11 12 13 HIV adherence in low-resource settings, but not with mHealth; 14 treatment for HIV but not specifically adherence; 15 16 and mHealth and disease management. 17 18 Two earlier review studies examined ART adherence, but were not focused on mobile technologies. 19 20 Other systematic reviews have focused on adolescent and young adult populations using mHealth interventions for adherence, which have seen HIV diagnoses growing at a disproportionately high rate. 21 22 23 A review 5 in 2012 analyzed two randomized control trials (RCT) using mobile phones for HIV adherence, but there have been many studies since then. This paper presents a comprehensive review focused on mobile text messaging to deliver adherence interventions in HIV/AIDS populations.
Objective
Our research focus was to determine whether using mobile phone text-based reminder systems are efficacious in enhancing adherence to ART in patients with HIV infection.
Methods
Search Strategy
We conducted a systematic review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews and the Cochrane review standards for classification of quality assessment and data extraction. 24 Systematic computerized literature searches were performed in PubMed/MEDLINE (NCBI), Embase (Elsevier), Cumulative Index to Nursing and Allied Health Literature-CINAHL (EBSCO), Cochrane Central Register of Controlled Clinical Trials (EBSCO), and Web of Science (Thomson Reuters). The search was designed to identify studies that evaluated the effectiveness of mobile phone technologies for enhancing adherence to ART in PLWHIV. Controlled vocabulary terms were included when available. No date or language limits were applied, but meeting abstracts were excluded when possible. We examined the bibliographies of relevant studies for additional material. Neither study authors were contacted nor were gray literature sources examined. The literature search was completed on December 12, 2017. The search terms are listed in Appendix A .
Study Selection and Eligibility Criteria
Three of this study's authors (Y.Q., D.F., and E.A.G.M.) independently screened and reviewed the titles and abstracts of each article identified by the search. The authors were unblinded because blinding has little effect on systematic review results. 25 The authors used inclusion and exclusion criteria to assess the full eligibility of the screened abstracts. Study date was not a criterion for inclusion or exclusion. Only peer-reviewed journal articles written in English were included in the review. Selection of English-only articles was decided because of our language limitations. Additional inclusion criteria were as follows: any experimental or observational intervention evaluations with a control group or single cohort group with a before and after comparison, where the intervention was delivered digitally, not by voice alone, via mobile phone, or smart phone in any setting. The types of evaluations included were as follows: retrospective cohort study, prospective cohort study, randomized controlled trial (RCT), cohort study, mixed retrospective/prospective cohort study, or before-and-after study. The exclusion criteria were applied in the order shown in Fig. 1 . Any study selection disputes were settled by a consensus of the authors.
Fig. 1.
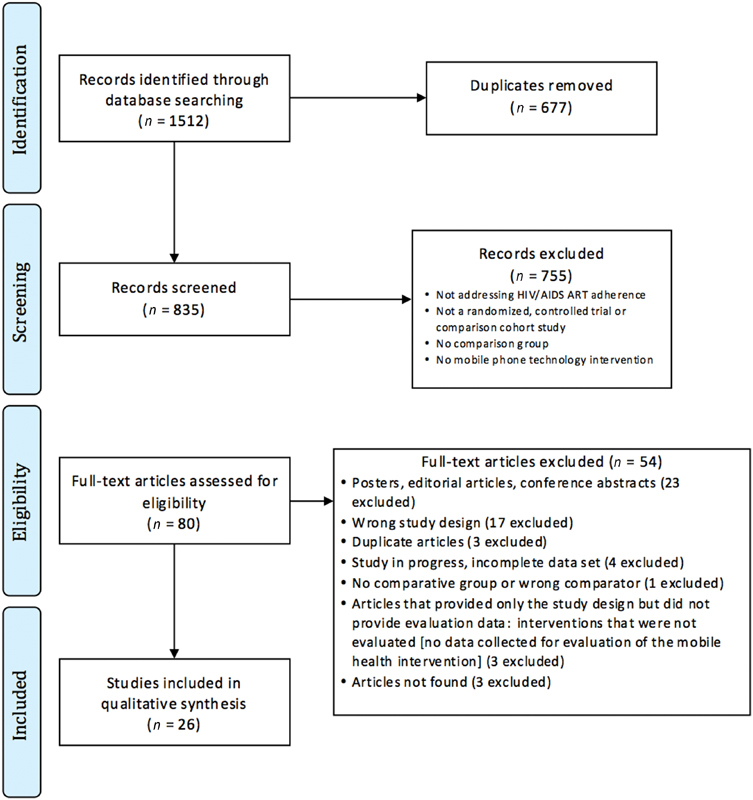
PRISMA flow chart of study selection. 24 AIDS, acquired immunodeficiency virus; HIV, human immunodeficiency virus; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Extraction and Analysis of the Data
Two blinded authors (D.F. and E.A.G.M.) independently conducted the quality assessment and data extraction. The Covidence ( http://www.covidence.org ) screening and data extraction tool for authors were used. The quality assessment was conducted based on the recommendations of the Cochrane Risk of Bias Comparison: sequence generation, allocation concealment, blinding of participants, blinding of outcome assessors, incomplete outcome data, selective outcome, and other sources of bias. The following data were extracted: study identification, methods, population, intervention, and outcome variables. p -Values <0.05 were considered significant. Disagreements between the two blinded authors (D.F. and E.A.G.M.) were adjudicated by a third author (Y.Q.), who was not involved in the data extraction. Four authors (C.S., Y.Q., D.F., and E.A.G.M.) reviewed the results and participated in the analysis and write-up.
Results
After examining the search results for inclusion and exclusion criteria, described in Fig. 1 , 26 articles for the qualitative synthesis remained: one short report, 26 and 25 peer-reviewed journal articles. 8 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 Of these 26 studies, 23 studies used SMS alone for reminders, and 3 used SMS plus counseling as noted in Table 1 . Six reports were from the United States; 35 36 37 42 43 44 three each from Kenya 8 31 40 and South Africa; 28 39 48 two each from Uganda, 38 45 China, 34 47 and Cameroon; 30 41 and one each from Italy, 26 Brazil, 29 Nigeria, 32 New Zealand, 27 India, 33 Argentina, 46 Canada, 49 and Malaysia. 50 The types of studies included 19 RCTs, 8 27 29 30 31 32 34 35 36 38 39 41 42 43 44 45 47 50 three prospective cohort studies, 26 37 46 two ambidirectional studies (retrospective/prospective cohort study), 28 49 one cluster RCT, 40 one quasi-experimental cohort study, 33 and one retrospective cohort. 48 The studies had been performed between 2007 and 2015 and published between 2010 and 2016 ( Table 1 ). For the RCTs, the number of participants ranged from 11 to 401 in the control groups and from 14 to 314 in the intervention groups. The intervention period plus follow-up ranged from 1 to 24 months, with a median of 10 months (quartiles 5–12). The primary outcomes addressed in the studies included one ART usage among study participants, 40 one adherence measured through prescription refills, 48 two viral load adherences, 37 46 six adherences over time, 31 33 34 38 39 43 and 16 self-reported adherences ( Table 2 ). 8 26 27 28 29 30 32 35 36 41 42 44 45 47 49 50 Adherence interventions were measured as self-report, ART usage, adherence over time using a medication event monitoring system (MEMS) or an electronic adherence monitoring device, such as Wisepill, pharmacy refills, pill count, and clinical outcomes (viral load, HIV-ribonucleic acid [RNA] suppression, and cluster of differentiation 4 [CD4] count). Additionally, a summary of the outcome data, adherence assessment, metrics, relative effect (risk and odds ratios [OR]), and a measure of precision (95% confidence interval [CI]) for each study are shown in Table 2 . Details on the types and levels of bias inherent in the individual studies are summarized in Fig. 2 .
Table 1. Summary of studies.
| Authors | Study year | Country | Type of study | Reminder method | Target population | n (Control group) | n (Intervention group) | Inclusion/Exclusion criteria reported | Adherence measure reported |
|---|---|---|---|---|---|---|---|---|---|
| Abdulrahman et al 50 | 2014 | Malaysia | RCT | SMS | Adult HIV positive patients who had completed four weeks of vitamin training and were newly initiating ART | 121 | 121 | Yes/Yes | Yes |
| Ammassari et al 26 | NR | Italy | PC | SMS | Patients reporting any degree of suboptimal adherence | 0 | 145 | Yes/Yes | Yes |
| da Costa et al 29 | 2009–2010 | Brazil | RCT | SMS | Patients with viral load below 400 copies/mL for at least 3 months and patients with CD4+ cell counts greater than 200/mm 3 | 15 | 14 | Yes/Yes | Yes |
| Evans et al 28 | 2011–2014 | South Africa | RC/PC | SMS | Patients receiving a second-line ART regimen containing lopinavir/ritonavir or atazanavir/ritonavir and experienced a single elevated viral load (≥400 copies/mL) on second-line ART intervention | 401 | 49 and 314 | Yes/No | Yes |
| Garofalo et al 35 | 2010–2014 | USA | RCT | SMS | HIV+ patients on ART for ≥1 month with adherence problems | 54 | 52 | Yes/Yes | Yes |
| Georgette et al 48 | 2012–2014 | South Africa | RC | SMS | Patients with pre-program prescription coverage <100% and patients who initiated ART within 2 years of the start of the SMS program | 2,255 | 2,255 | Yes/No | Yes |
| Haberer et al 38 | 2013–2014 | Uganda | RCT | SMS | This study involved two types of participants: individuals taking ART (‘study participants’) and their ‘social supporters’ | 21 | 21 and 20 | Yes/Yes | Yes |
| Hardy et al 36 | 2008 | USA | RCT | SMS | HIV-infected men and women receiving HIV primary care on a stable regimen of antiretroviral therapy for at least 3 months and reporting less than 85% adherence to ART over the prior 7 days | Not reported | 23: 12 and 11 | Yes/No | Yes |
| Kalichman et al 42 | 2011–2015 | USA | RCT | SMS | Patients receiving ART and self-reported less than 95% adherence in the past month as per a validated visual analog adherence scale | 149 and 151 | 150 and 150 | Yes/No | Yes |
| Kassaye et al 40 | 2012–2013 | Kenya | Cluster RCT | SMS | Pregnant women were eligible to enroll in the study if they were less than 32 weeks of gestational age, were not currently receiving ART, were planning to remain in the area for the duration of the study period, and agreed to follow-up of their infants until 6 weeks following delivery. Male partners of women were also permitted to enroll in the study. | 270 | 280 | Yes/No | No: improve PMTCT |
| King et al 49 | 2013–2014 | Canada | RC/PC | SMS | Patients attending the clinic for at least 1 year prior to study entry, with an indication for cART (at time of study development, CD4 <500 cells/mm 3 ), detectable VL (≥200 copies/mL), with high risk for disengagement in treatment | 80 | 80 | Yes/Yes | Yes |
| Lester et al 8 | 2007–2008 | Kenya | RCT | SMS | Patients who were initiating ART for the first time | 265 | 273 | Yes/No | Yes |
| Lewis et al 37 | 2010 | USA | PC | SMS | HIV-positive men having sex with men | 0 | 52 | Yes/No | Yes |
| Linnemayr et al 45 | 2014–2015 | Uganda | RCT | SMS | Patients on ART or cotrimoxazole prophylaxis against common opportunistic infections, 15–22 years of age | 112 | 110 | Yes/Yes | Yes |
| Mbuagbaw et al 41 | 2010 | Cameroon | RCT | SMS | Patients who had been on ART for at least 1 month | 99 | 101 | Yes/Yes | Yes |
| Moore et al 44 | NR | USA | RCT | SMS | Documented HIV infection, diagnosis of bipolar disorder I or II via the composite international diagnostic interview, and currently taking at least one ARV and one PSY medication to treat HIV and BD, respectively. Medication non-adherence was not a study entry requirement | 28 | 30 | Yes/Yes | Yes |
| Nsagha et al 30 | 2011 | Cameroon | RCT | SMS | People living with HIV and AIDS and who had been on ARVs for at least 1 month | 45 | 45 | Yes/Yes | Yes |
| Orrell et al 39 | 2012–2014 | South Africa | RCT | SMS | Participants who were ART-naive adults and adolescents (≥15 years old) commencing treatment at the Hannan Crusaid Treatment Centre | 115 | 115 | Yes/No | Yes |
| Perera et al 27 | 2012–2013 | New Zealand | RCT | Mobile App | Individuals who had been on ART for at least 6 months | 11 | 17 | Yes/No | Yes |
| Rodrigues et al 33 | 2010–2011 | India | Quasi-experimental cohort study | SMS | HIV-infected adults who followed up at the clinic as outpatients and who were on ART for at least a month prior to enrollment | 0 | 150 | Yes/Yes | Yes |
| Ruan et al 47 | 2013–2014 | China | RCT | SMS | HIV-positive patients on ART for no more than 3 months | 50 | 50 | Yes/No | Yes |
| Sabin et al 34 | 2012–2013 | China | RCT | SMS | Patients who were receiving or initiating ART and were deemed at risk for poor adherence by clinicians or themselves | 21 and 35 | 23 and 40 | Yes/No | Yes |
| Stankievich et al 46 | 2014 | Argentina | PC | SMS | Patients who were receiving ART and who had suboptimal adherence (incomplete viral suppression determined by VL ≥ 1000 copies/mL) | 22 | 22 | Yes/Yes | Yes |
| Studies with SMS reminder and additional counseling | |||||||||
| Ingersoll et al 43 | 2012 | USA | RCT | SMS | Patients who had an active prescription for ART and reported less than 95% ART adherence in the past 2 weeks | 30 | 33 | Yes/no | Yes |
| Maduka and Tobin 32 | 2011 | Nigeria | RCT | SMS | HIV-positive patients who had been HAART experienced for at least 3 months and had a history of non-adherence (adherence below 95%) to HAART at the time of the study | 52 | 52 | Yes/yes | Yes |
| Pop-Elecheset al. 31 | 2007–2008 | Kenya | RCT | SMS | Patients who had initiated ART less than 3 months prior to enrollment | 139 | 70 and 72 and 73 and 74 | Yes/yes | Yes |
Abbreviations: AIDS, acquired immunodeficiency syndrome; ART, antiretroviral therapy; ARV, antiretroviral; BD, bipolar disorder; cART, combination antiretroviral therapy; HAART, highly active antiretroviral therapy; HIV, human immunodeficiency virus; NR, not reported; PC, prospective cohort; PMTCT, prevention of mother-to-child transmission; PSY, psychiatric; RC, retrospective cohort; RCT, randomized controlled trial; SMS, short messaging service; VL, viral load.
Table 2. Summary of outcomes, outcome variables, and statistical significance.
| Author | Year | Study focus | Metric | Outcome variable | Relative effect | Outcome | Notes | Positive outcome | Non-positive outcome | p < 0.05 | p ≥ 0.05 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kassaye et al 40 | 2016 | Antiretroviral usage among study participants | N , % | Any missed dose past week | Risk ratio (95%) for both outcomes (ART usage and missed dose) | Antiretroviral usage among study participants | Slightly higher % in control group than in intervention group; no p -value reported | X | – | – | |
| Any missed dose during past week | Slightly lower % in control group than in intervention group; no p -value reported | X | – | – | |||||||
| Lewis et al 37 | 2013 | VL | Median, high, and low, Improved, remained adherent, non-adherent | CD4 count, Medication adherence - VL (HIV-1 RNA copies per mL); medication adherence - CD4 count (absolute count per mm 3 ) | – | VL | Significant improvement in VL from baseline to follow-up, p < 0.012 | X | X | ||
| CD4 count | Significant increase in CD4 counts, p < 0.037 | X | X | ||||||||
| Medication adherence- VL (HIV-1 RNA copies/mL) | Participants who improved their medication adherence during the study or remained adherent had significant improvements in VLs, p = 0.013 | X | X | ||||||||
| Medication adherence – CD4 count (absolute count per mm 3 ) | Participants who improved their medication adherence during the study or remained adherent had a general trend of improvements in CD4 counts, p = 0.051 | X | X | ||||||||
| Pop-Eleches et al 31 | 2011 | Adherence ITT over time (MEMS) | % | – | – | Adherence ITT over time (MEMS) | Weekly SMS reminders increased the percentage of participants achieving 90% adherence to ART by ∼13% to 16% compared with those with no reminder; no p -value reported | X | – | – | |
| Rodrigues et al 33 | 2012 | Adherence over time (IVR) | N, % | – | – | Adherence over time (IVR) | Significant improvement in proportion of participants adherent over time, p = 0.016 | X | X | ||
| Sabin et al 34 | 2015 | Adherence over time | N , %, mean, SD | CD4+ cell count, undetectable VL over time <50 copies/mL | Risk Ratio (95%) Adherence only | Adherence over time | Adherence was significantly greater in the intervention group than in the controls at the end of the study as well as during the entire intervention period, p < 0.001 | X | X | ||
| Undetectable VL over time <50 copies/mL | Adherence in both the intervention and control groups increased, but proportions were similar between them at month 9, p = 0.218 | X | X | ||||||||
| CD4+ cell count | Mean change in CD4-cell count between baseline and month 9 trended higher, but was not significantly different in intervention subjects versus controls, p = 0.297 | X | X | ||||||||
| Orrell et al- 39 | 2015 | Adherence over time (EAMD) | OR, CI, N, mean TI only | TIs, retention in care, HIV-RNA > 40 copies/mL | Odds ratio (95%) for adherence, odds ratio for HIV-RNA, risk ratio (95%) for TIs | Adherence over time (EAMD) | Median adherence by EAMD was slightly greater in the intervention group than in the controls, but not significant, p = 0.642 | X | X | ||
| HIV-RNA >40 copies/mL | No difference in the odds of virological failure in the intervention arm, p = 0.393 | X | X | ||||||||
| TIs, retention in care | The intervention significantly reduced the frequency of TIs over 72 h, p = 0.393 | X | X | ||||||||
| Ingersoll et al 43 | 2015 | Adherence over time (pharmacy refill) | Mean, %, SD | Alcohol and drug using days, Proportion of missed visits | – | Adherence over time (pharmacy refill) | The intervention improved adherence, p = 0.02 | X | X | ||
| Proportion of missed visits | There was a trend toward improved visit attendance in the intervention group, but it was not significant, p = 0.12 | X | X | ||||||||
| Alcohol and drug using days | There was improvement, but the intervention did not reduce substance- using days compared with the control, p = 0.14 | X | X | ||||||||
| Haberer et al 38 | 2016 | Adherence over time (EAMD) | Median, %, IQR, mean %, SD | HIV-RNA suppression | Risk ratio adherence only | Adherence over time (EAMD) | Percentage adherence was 11.1% higher ( p < 0.02) and >48-h and >96-h lapses were less frequent ( p < 0.02, p < 0.001, respectively) in the scheduled SMS arm compared with the control | X | X | ||
| HIV-RNA suppression | No statistically significant differences in HIV RNA suppression were seen between study arms, p = 0.14 | X | X | ||||||||
| Maduka et al 32 | 2013 | Self-reported adherence over time | N, % | CD4+ cell count | Risk ratio (95%) adherence only | Self-reported adherence over time | Text message reminders significantly improved drug adherence, p = 0.022 | X | X | ||
| CD4+ cell count | Median CD4+ cell count of the intervention group increased, p = 0.007 | X | X | ||||||||
| Lester et al 8 | 2010 | Self-reported adherence over time | N , % | Rate of attrition, HIV-1 VL RNA Suppression <400 copies/mL | Risk ratio (95%) | Self-reported adherence over time | Greater adherence to ART was reported for patients receiving the SMS intervention, p = 0.006 | X | X | ||
| HIV-1 VL RNA suppression <400 copies/mL | Suppressed VLs were reported in more patients in the SMS group, p = 0.04 | X | X | ||||||||
| Ammassari et al 26 | 2011 | Self-reported adherence over time | Mean, %, SD | Undetectable HIV RNA VL <50 copies/mL | – | Self-reported adherence over time | Significant improvement in the proportion of ART doses taken over the preceding month at all study time points, p < 0.001 | X | X | ||
| Undetectable HIV RNA VL <50 copies/mL | Significant improvement in the proportion of subjects with undetectable HIV RNA VL, p < 0.001 | X | X | ||||||||
| da Costa et al 29 | 2012 | Self-reported adherence over time | N , % | MEMS adherence over time, pill counting adherence over time | – | Self-reported adherence over time | Not significant, p = 0.243 | X | X | ||
| Pill counting adherence over time | Not significant, p = 0.6038 | X | X | ||||||||
| MEMS adherence over time | Significant, p = 0.1946 | X | X | ||||||||
| Garofalo et al 35 | 2016 | Self-reported adherence over time | N , mean, SD | Undetectable VL ≤75 copies/mL over time | Odds ratio (95%) | Self-reported adherence over time | The average effect estimate over the 6-month intervention was significant for ≥90% adherence, p < 0.05, and maintained at 12 months | X | X | ||
| Undetectable VL ≤75 copies/mL over time | Improved in intervention group, p < 0.05 | X | X | ||||||||
| Hardy et al 36 | 2011 | Self-reported adherence over time | Mean, range | MEMS adherence over time, CAS adherence over time, pill count adherence over time | Odds ratio (95%) for MEMS only | Self-reported adherence over time | All the samples resulted in a significant difference between the mean adherence in the two intervention groups at both week 3 and week 6 ( p -value ranges 0.004–0.043 at week 3 and 0.004–0.026 at week 6) | X | X | ||
| Pill count adherence over time | All the samples resulted in a significant difference between the mean adherence in the two intervention groups at both week 3 and week 6 ( p -value ranges 0.004–0.043 at week 3 and 0.004–0.026 at week 6) | X | X | ||||||||
| MEMS adherence over time, CAS adherence over time | All the samples resulted in a significant difference between the mean adherence in the two intervention groups at both week 3 and week 6 ( p -value ranges 0.004–0.043 at week 3 and 0.004–0.026 at week 6) | X | X | ||||||||
| Kalichman et al 42 | 2016 | Self-reported adherence over time | N , mean, SD | Medication adherence self-efficacy, HIV RNA VL suppression <100 copies/mL | Odds ratio (95%) for HIV RNA viral suppression only | Self-reported adherence over time | Self-reported adherence improved 90% demonstrating a clinical meaningful improvement, p < 0.01 & p < 0.05 | X | X | ||
| HIV RNA VL suppression <100 copies/mL | Modest but significant effect on the HIV RNA VL suppression, p < 0.05 | X | X | ||||||||
| Medication adherence self-efficacy | Significant effect, p < 0.05 | X | X | ||||||||
| Mbuagbaw et al 41 | 2012 | Self-reported adherence over time | N , %, mean, SD | Pharmacy refill rate, self-reported number of doses missed | Risk ratio (95%) for self-reported adherence and doses missed only | Self-reported adherence over time | No significant effect on adherence | X | X | ||
| Self-reported number of doses missed | p > 0.9 | X | X | ||||||||
| Pharmacy refill rate | No significant effect | X | X | ||||||||
| Moore et al 44 | 2015 | Self-reported adherence over time | %, SD | – | – | Self-reported adherence over time | Adherence for 80% of the participants in the study was > 90% and ART dose timing significantly improved with the intervention compared with the control, no p-value reported | X | – | – | |
| Nsagha et al 30 | 2016 | Self-reported adherence over time | N , % | – | – | Self-reported adherence over time | Self-reported adherence was higher in the intervention group, p = 0.05 | X | X | ||
| Perera et al 27 | 2014 | Self-reported adherence over time | N , mean, SD, 95% CI | Prescribed doses taken, pharmacy dispensing, HIV VL (log 10 copies/mL) | – | Self-reported adherence over time | Self-reported adherence significantly improved, p = 0.03 | X | X | ||
| HIV VL (log 10 copies/mL) | Decreased, p = 0.02 | X | X | ||||||||
| Prescribed doses taken, pharmacy dispensing | Non-adherence decreased, p = 0.18, not significant | X | X | ||||||||
| Evans et al 28 | 2016 | Self-reported adherence over time | N , % | VL suppressed <400 copies/mL | – | Self-reported adherence over time | Only 44.9% of participants in the intervention resuppressed their VL, modest improvement in the primary outcome. It could not be demonstrated that EAMD could significantly improve adherence | X | X | ||
| VL suppressed <400 copies/mL | Modest, but not significant improvement in viral suppression | X | X | ||||||||
| Abdulrahman et al 50 | 2017 | Self-reported adherence over time | N , mean, SD, 95% CI | Adherence, CD4 count (cells/mL), VL (log 10 ), Weight (kg) | – | Adherence | Mean adherence to ART increased from baseline values in the intervention group as compared with the control group after 6 months follow-up ( p = 0.035). The proportion of respondents who had good adherence (>95%) was significantly higher in the intervention group ( n = 107, 92.2%) as compared with control group ( n = 59, 54.6%) ( p = 0.001) after 6 months follow-up. | X | X | ||
| CD4 count | A significantly higher rise in CD4 count ( p = 0.017) was observed in the intervention group after 6 months follow-up. CD4 count increased by 146.01 cells/μL in the intervention group whereas an increase of 93.62 cells/μL was observed in the control group. | X | X | ||||||||
| VL | It was found that 99.1% of the intervention group who achieved optimal/good adherence, >95%, had viral suppression compared with 89.3% in the control group, p = 0.028 | X | X | ||||||||
| Georgette et al 48 | 2017 | ART prescription coverage | N , %, 95% CI, IQR | Program effect: exposed, unexposed, and unknown | Adjusted odds ratio (95%) | Self-reported adherence over time | Self-reported adherence significantly improved, p = 0.03 | X | X | ||
| King et al 49 | 2017 | VL, CD4 count, and self-reported adherence | N , mean, median, % | Geometric mean VL (copies/mL), mean (95% CI); CD4 (cells/mm 3 ), median (IQR); cART regimen, N (%); attendance (%), mean (95% CI) | Odds ratio (95%) | HIV VL (log 10 copies/mL) | Decreased, p = 0.02 | X | X | ||
| Prescribed doses taken, pharmacy dispensing | Non-adherence decreased, p = 0.18, not significant | X | X | ||||||||
| Self-reported adherence over time | Only 44.9% of participants in the intervention resuppressed their VL, modest improvement in the primary outcome. It could not be demonstrated that EAMD could significantly improve adherence | X | X | ||||||||
| Linnemayr et al 45 | 2017 | Self-reported adherence over time | N , mean, 95% CI | MEMS adherence over time for control, SMS only, and SMS + response: ITT and Complete case | – | VL suppressed <400 copies/mL | Modest but not significant improvement in viral suppression | X | X | ||
| Adherence | Mean adherence to ART increased from baseline values in the intervention group as compared with the control group after 6 months follow-up ( p = 0.035). The proportion of respondents who had good adherence (>95%) was significantly higher in the intervention group ( n = 107, 92.2%) as compared with control group ( n = 59, 54.6%) ( p = 0.001) after 6 months follow-up. | X | X | ||||||||
| CD4 count | A significantly higher rise in CD4 count ( p = 0.017) was observed in the intervention group after 6 months follow up. CD4 count increased by 146.01 cells/μL in the intervention group whereas an increase of 93.62 cells/μL was observed in the control group. | X | X | ||||||||
| Ruan et al 47 | 2017 | HIV-related and HIV mediation knowledge and self-reported adherence | N , %, mean, SD, Z -score | VAS, CPCRA Antiretroviral medication self-report, CD4 count | – | VAS | The intervention group had a significantly higher VAS mean score ( Z = 2.735, p = 0.006) and lower suboptimal adherence rate ( Z = 2.208, p = 0.027) at the end of the study. | X | X | ||
| CPCRA antiretroviral medication self-report | The percentage of people with suboptimal adherence in the control group (27%) was significantly higher than that in the intervention group (10.7%) in the post-test ( p = 0.027). | X | X | ||||||||
| Stankievich et al 46 | 2017 | ART adherence, VL | N , % | VL (copies/mL) | – | VL | After the strategy implementation, 20/22 VL results were available. 13/20 (65%) were undetectable, 14/20 (70%) had VL < 1000 copies/mL. 6/20 (30%) VLs had no changes; no p -value reported. | X | – | – |
Abbreviations: AIDS, acquired immunodeficiency syndrome; AOR, adjusted odds ratio; ART, antiretroviral therapy; cART, combination antiretroviral therapy; CAS, composite adherence score; CI, confidence interval; CPCRA, Community Programs for Clinical Research on AIDS; EAMD, electronic adherence monitoring device; HIV, human immunodeficiency virus; IQR, interquartile range; ITT, intention to treat; IVR, interactive voice response; MEMS, medication event monitoring system; OR, odds ratio; SD, standard deviation; SMS, short message service; TI, treatment interruption; VAS, visual analog scale; VL, viral load.
Fig. 2.
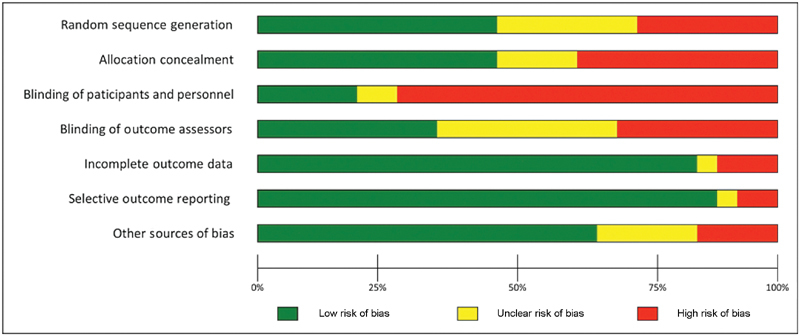
Types and levels of bias inherent in the individual studies.
The Cochrane method was used to evaluate bias and is summarized in Fig. 2 . Most of the studies we reviewed fall under the high-risk category for performance bias. For protocols that call for large numbers of subjects, it may not be economically feasible to supply each study participant with a mobile phone to ensure proper blinding. The alternative—either using a subject's phone or providing phones only to the interventional cohort—introduces the risk of performance bias. Nine of the 19 RCTs were deemed to be at low risk for detection bias, 4 at high risk, and 6 at unclear risk. All the studies were deemed to be at low risk for attrition bias, with two exceptions. Two studies—one by Evans et al 28 and another by Lewis et al 37 —had a high risk of reporting bias because of missing data, but in the Evans et al study, the authors noted the missing data and addressed the issue by including a sensitivity analysis. A major factor in determining the risk of bias was the inadequate reasoning for missing data with low attrition rates. Similarly, reporting bias was low across all studies, with all but one RCT deemed as low risk. One prospective cohort trial was evaluated as high risk and one as unclear. We determined a high risk of bias in one study due to non-reporting of HIV laboratory data, 43 which were not consistently gathered.
Four studies contained other potential sources of bias. One study noted that 37% of screened participants were excluded because of lack of mobile phone access. 38 We determined that this met the criteria for a high risk of bias owing to the study design and problems with the recruitment of participants with mobile phone access. Another study was evaluated as having a high risk of bias due to the lack of information listed regarding sources of funding or conflicts of interest. 43 Two studies 48 49 declared authors with a material interest in the development of adherence promoting tools or procedures.
Small sample sizes and missed recruitment goals were other concerning issues in some studies. Recruitment ranged from 28 to 715 subjects, and only 11 (55%) studies had more than 100 enrolled. Two studies had low recruitment numbers—28 and 29—limiting the generalizability of the reported results. 27 29 Additionally, although 200 patients were recruited, the sample size was insufficient to adequately statistically power the study. 41 The study by Lewis et al had limited enrollment criteria because of a second, concurrently running study at the same site. 37
Nineteen studies reported statistically significant adherence outcomes ( Table 2 ). One study found that text messages significantly increased the proportion of those achieving adherence (76.9% versus 55.8%, p = 0.02). 32 Another reported that even though adherence increased significantly with weekly reminders, daily SMS reminders did not have a significantly different effect on study subjects versus the control group, which the authors attributed to the possibility of habituation. 31 One study showed that increased adherence, from 85% to 91%, had been maintained 6 months after the intervention was discontinued ( p = 0.016). 33 One study using real-time reminders significantly improved adherence. 34 Another study concluded that mobile phone SMS interventions might be effective tools for improving patient outcomes in resource-limited settings. 8 One study found a higher proportion of adherent subjects through the use of pill counting and MEMS methods. 28 An additional study estimated that the average effect over the 6-month intervention period was significant for ≥90% adherence (OR = 2.12, 95% CI 1.01–4.45, p < 0.05) and was maintained at 12 months. 35 One study showed significant adherence when it was measured by MEMS (mean difference ± standard deviation [SD]: 33.4 ± 9.1, p = 0.002) and composite adherence score (27.1 ± 9.2, p = 0.009). 36 In contrast, significance was not attained while assessing adherence measured by pill count (13.7 ± 9.1, p = 0.153) or self-report (20.2 ± 10.3, p = 0.069). One study showed that SMS improved adherence and that the key constraints affecting adherence to antiretroviral medication can be addressed by using SMS. 30 Another study showed that greater usage of the extra components of an augmented phone application was associated with a greater perceived understanding of HIV infection and increased perceived necessity for ART. 27 In addition to significant adherence improvement, some authors reported improvement in clinical outcomes. One study observed a significant reduction in viral load, 37 and in another study, the proportion of subjects with undetectable viral load increased. 26 One study reported that scheduled SMS reminders significantly improved adherence in the context of real-time monitoring ( p = 0.02), and HIV RNA suppression was seen, although it was not statistically significant ( p = 0.14). 38
The remaining seven studies described non-significant outcomes ( Table 2 ). Six yielded no significant difference in adherence over the course of their studies. 39 40 41 42 45 46 One study observed that in patients with an elevated viral load on a second-line ART, electronic adherence monitoring was associated with a modest, but not significant, improvement in viral suppression. 28 Those authors concluded that adherence strategies increase the durability of second-line ART, decrease the need for costly third-line regimens, and prevent unnecessary genotyping tests.
Discussion
Our review shows that using mobile phone text-based reminder systems are efficacious in enhancing adherence to ART in patients with HIV infection in a wide variety of global settings. Of the 23 studies that used text messaging, 21 had positive outcomes, and of the 3 studies that used text-messaging with counseling, all 3 had positive outcomes. While a majority of studies had positive outcomes, the sample sizes will need to be larger to evaluate effect size and variations in delivery methods. All the studies contributed to a better understanding of how to deliver these interventions via mobile devices.
Several studies showed that wireless devices could provide real-time behavior data 28 34 38 that allow messages to be tailored to the patient and promote faster behavior correction. Four studies monitored the patients' ART adherence electronically in real time by providing them with a medication dispenser device. 28 34 38 39 Three of those studies would trigger an SMS reminder if the monitoring device were not activated within 30 minutes to 2 hours of a scheduled dose. 34 38 39 One study achieved high outcomes (optimal adherence ≥95%) and showed this technology to be feasible and acceptable in China, with reliable monitoring of adherence over time. 34 Combined, these findings suggest that wireless technologies can be an aid to adherence programs.
Three studies combined the strategies of adherence counseling and text-message reminders. The first evaluated the differences between the lengths of ‘short’ and ‘long’ messages and the difference in daily and weekly frequencies. 31 The second used a similar strategy, sending up to four text messages to those in the intervention cohort regarding whether a medication was taken, the subject's mood, and if any substance use had taken place. 43 The third, in Nigeria, evaluated subjects receiving adherence counseling monthly for 4 months in addition to receiving adherence text-message reminders. 32 Text messages were crafted to address behavioral barriers and adherence support and to serve as a reminder to continue the ART. All three reported positive outcomes as increases in adherence in the intervention cohorts. The optimal frequency of reminders is debatable, as two of the studies sent messages daily, 31 43 while the third called for reminders twice a week on weekdays only. 32 The results were mixed, with one study finding no difference between the control group and those who received daily messages, 31 while the other study found clinically relevant differences. 43 This difference could be explained by the bidirectional nature of the intervention, which could account for increased subject participation and engagement. Subjects receiving daily texts may become accustomed to the content of the messages, thus diminishing the effect through habituation. In studies with combined strategies, it may be impossible to distinguish the isolated effect of the SMS intervention alone, and for future work, examining the efficacy of mobile reminders, the research methodology of combined interventions should be tailored to differentiate the effects via multiple cohorts.
Studies that included both adherence and clinical outcomes could provide a more comprehensive view of their outcomes than those that relied on self-report alone. One study that had both self-report and clinical outcomes found that self-reported ART adherence was >95% of prescribed doses in the past 30 days at both 6- and 12-month follow-up visits, and plasma HIV-1 viral RNA load suppression was <400 copies/mL at 12 months. 8 In all, 11 studies collected self-reports in addition to clinical metrics. 8 26 27 28 32 34 35 37 38 39 42
Several studies used self-adherence reporting to measure adherence without clinical measures. Six of the studies reviewed had ‘self-reported adherence’ as the primary outcome measure, and lacked any clinical measure. 29 30 31 32 44 While patient-reported non-adherence has been found to be an accurate predictor of virologic outcomes, 51 52 53 it is not a replacement for clinically derived measures such as HIV RNA viral load. Self-reported adherence is subject to inherent cognitive bias, such as response bias and recall bias. Subjects may not recall whether they have taken their medication, especially in cases of cognitive dysfunction or decline 54 55 and may incorrectly report as adherent. Another study discusses the challenges and discrepancies due to measurement methods. 56
Illiteracy is a barrier to ART adherence. 42 Of the papers reviewed, only one had inclusion criteria that clearly addressed illiteracy and owning or sharing a mobile phone. 8 Six studies stated illiteracy and/or inability to read as specific exclusion criteria, while the remaining authors did not mention these criteria. 8 26 29 30 41 43 Five studies required the participants to be able to speak, read, and write English at the fourth-grade level. 28 35 38 43 44
In most resource-limited settings, access to the second-line treatment is scarce and has a significantly higher cost compared with the first-line therapy, and access to third-line ART is non-existent. 19 Of the reviewed studies, only one assessed the effectiveness of an electronic adherence monitoring device among patients failing the second-line ART, as measured by viral load suppression (<400 copies/mL). 28 The results of this study are encouraging since patients who re-suppress viral load at the first follow-up are more likely to remain virally suppressed.
According to the International Telecommunications Union, 57 in 2016, per 100 people mobile cellular subscriptions, for developing countries had a mobile cellular subscription rate of 60 and for middle-income countries had a rate of 101. Sub-Saharan Africa, for example, had a rate of 74. Middle-income countries were further subdivided into upper middle and lower middle, with rates of 108 and 95, respectively. 57 This data suggest that cell phone health interventions could be scaled to large numbers of people even in low- and middle-income countries.
One of the limitations of this review is that our search included only articles written in English. However, we feel that the papers in this review represent a global perspective on these approaches. Additionally, completing a meta-analysis of the reviewed studies is not possible due to the wide range of research study designs, and included papers were not all RCTs. Given that many of the published works on this subject are not RCTs speaks to the continual evolution of the field and is a reflection that the body of evidence is in development. Future studies could include more reported data and sensitivity analysis.
Privacy concerns are an opportunity for an investigation to understand differences in adherence according to age, sex, socioeconomic level, and geographical differences. Although most of the studies we reviewed developed methods for ensuring the privacy of the text reminders 8 31 32 33 34 35 36 37 38 39 41 42 43 44 that ranged from omitting references to HIV or ART to common message greetings, there was no examination of whether privacy concerns affected the viewing of the reminder and maintenance of adherence.
Based on this review, it appears that studies that combine multiple delivery methods (SMS and counseling) and measure both adherence and clinical outcomes show particular promise in improving care. Future mHealth ART studies should consider people who access mobile phones via a partner or family member, include both self-report and clinically measurable outcomes, evaluate the training for both patients and health professionals, and pay more careful attention to randomization and blinding of participants to reduce possible effects of bias. The mental health of patients could be part of future study designs. Interventions should be individualized in real time to promote faster behavior correction by adjusting the content, frequency, and length of messages. Studies should consider the use of devices that can track medication pill dispensing. A cost analysis would be useful for policymakers. The definition of adherence needs to be more clearly defined and reported to allow comparison of approaches. Future investigations could examine the role of personalized messages and cultural differences in approaches.
Conclusion
This review shows that text message in low-cost cell phones can be effective for promoting adherence, and this is particularly useful to low- and middle-income countries. While the majority of studies reviewed had positive outcomes in many diverse global settings, there needs to be larger scale studies to evaluate effect sizes. The analysis of potential bias showed that the main potential source of bias was in the lack of blinding of participants and personnel. While our search criteria did not exclude apps, only one study used a mobile app as a supplementary tool. 27 All the studies that had text messaging combined with additional support mechanisms had positive outcomes. There is a need for more comprehensive approaches and larger scale trials to confirm results observed in limited cohort sizes and evaluate the impact of complimentary services, such as counseling. The feasibility of such interventions is increasingly possible even within low-resource settings due to the expanding prevalence of mobile phone availability. 57 To better retain satisfactory adherence within the HIV population, and especially in low-resource settings, we recommend that future interventions incorporate multiple strategies: mobile-based reminders, social support structures, and personalized content. Further work needs to be done to determine the optimal frequency of reminders, content length, and tailoring to local customs and user preferences.
Clinical Relevance Statement
Phone text-based reminder systems are efficacious in enhancing HIV ART adherence. Mobile reminder systems have been successfully implemented in low-resource settings. Content and length should be tailored to local customs and user preferences.
Multiple Choice Question
Which of the following should be considered while tailoring text messaging-based adherence reminders for patients living with HIV/AIDS?
Privacy
Length of message
Local customs and preferences
All of the above
Correct Answer: The correct answer is option d, all of the above.
Acknowledgments
The searches were conducted by Paul Pain, Reference and Education Librarian, Countway Library of Medicine, Harvard Medical School. We appreciate comments by Patricia Stephens, PhD; Brian Haynes, MD; and Roger Davis, ScD, on earlier versions of this paper.
Funding Statement
Funding None.
Conflict of Interest None.
Protection of Human and Animal Subjects
Human or animal subjects were not included in this project.
Appendix A: PubMed Search Strategy.
PubMed
2017–12–11
371 Records
(“HIV Infections”[mesh] OR “Antiretroviral Therapy, Highly Active”[mesh] OR “Anti-HIV Agents”[mesh] OR human immunodeficiency virus[tiab] OR immunodeficiency syndrome[tiab] OR HIV[tiab] OR aids[tiab] OR antiretroviral[tiab] OR antiretroviral[tiab] OR haart[tiab])
AND
(“Cell Phone”[mesh] OR “Smartphone”[mesh] OR “Mobile Applications”[mesh] OR cellular phone*[tiab] OR cellular telephone*[tiab] OR cellular device*[tiab] OR cell phone*[tiab] OR cellphone*[tiab] OR mobile telephone*[tiab] OR mobile phone*[tiab] OR smartphone*[tiab] OR smart phone*[tiab] OR wireless phone*[tiab] OR wireless telephone*[tiab] OR mobile app*[tiab] OR text messag*[tiab] OR text reminder*[tiab] OR short message service*[tiab] OR short messaging service*[tiab] OR short message system[tiab] OR short messaging system[tiab] OR sms[tiab] OR texting[tiab])
AND
(“Patient Compliance”[mesh] OR compliance[tiab] OR adherence[tiab] OR noncompliance[tiab] OR nonadherence[tiab] OR attendance[tiab] OR retention[tiab] OR return to clinic[tiab])
References
- 1.WHO. 2017.Number of people (all ages) living with HIV Estimates by WHO region. Global Health Observatory data repositoryWorld Health Organization. Available at:http://apps.who.int/gho/data/view.main.22100WHO?lang=en. Accessed January 3, 2018
- 2.Dryden-Peterson S, Bennett K, Hughes M D et al. An augmented SMS intervention to improve access to antenatal CD4 testing and ART initiation in HIV-infected pregnant women: a cluster randomized trial. PLoS One. 2015;10(02):e0117181. doi: 10.1371/journal.pone.0117181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Anglemyer A, Rutherford G W, Horvath T, Baggaley R C, Egger M, Siegfried N. Antiretroviral therapy for prevention of HIV transmission in HIV-discordant couples. Cochrane Database Syst Rev. 2013;4(04):CD009153. doi: 10.1002/14651858.CD009153.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dyrehave C, Rasmussen D N, Hønge B L et al. Nonadherence is associated with lack of HIV-related knowledge: a cross-sectional study among HIV-infected individuals in Guinea-Bissau. J Int Assoc Provid AIDS Care. 2016;15(04):350–358. doi: 10.1177/2325957415599211. [DOI] [PubMed] [Google Scholar]
- 5.Horvath T, Azman H, Kennedy G E, Rutherford G W. Mobile phone text messaging for promoting adherence to antiretroviral therapy in patients with HIV infection. Cochrane Database Syst Rev. 2012;3(03):CD009756. doi: 10.1002/14651858.CD009756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Joint United Nations Programme on HIV/AIDS (UNAIDS).Global AIDS Update 2016. May 31, 2016Available at:http://www.unaids.org/sites/default/files/media_asset/global-AIDS-update-2016_en.pdf. Accessed January 3, 2018
- 7.U.S. Central Intelligence Agency (CIA). 2016.The World Factbook: Country comparison: hiv/aids–adult prevalence ratEAvailable at:https://www.cia.gov/library/publications/the-world-factbook/rankorder/2155rank.html. Accessed January 3, 2018
- 8.Lester R T, Ritvo P, Mills E Jet al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial Lancet 2010376(9755):1838–1845. [DOI] [PubMed] [Google Scholar]
- 9.Anglada-Martinez H, Riu-Viladoms G, Martin-Conde M, Rovira-Illamola M, Sotoca-Momblona J M, Codina-Jane C. Does mHealth increase adherence to medication? Results of a systematic review. Int J Clin Pract. 2015;69(01):9–32. doi: 10.1111/ijcp.12582. [DOI] [PubMed] [Google Scholar]
- 10.Checchi K D, Huybrechts K F, Avorn J, Kesselheim A S. Electronic medication packaging devices and medication adherence: a systematic review. JAMA. 2014;312(12):1237–1247. doi: 10.1001/jama.2014.10059. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Aranda-Jan C B, Mohutsiwa-Dibe N, Loukanova S. Systematic review on what works, what does not work and why of implementation of mobile health (mHealth) projects in Africa. BMC Public Health. 2014;14:188. doi: 10.1186/1471-2458-14-188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Déglise C, Suggs L S, Odermatt P. SMS for disease control in developing countries: a systematic review of mobile health applications. J Telemed Telecare. 2012;18(05):273–281. doi: 10.1258/jtt.2012.110810. [DOI] [PubMed] [Google Scholar]
- 13.James D C, Harville C, II, Sears C, Efunbumi O, Bondoc I. Participation of African Americans in e-Health and m-Health studies: a systematic review. Telemed J E Health. 2017;23(05):351–364. doi: 10.1089/tmj.2016.0067. [DOI] [PubMed] [Google Scholar]
- 14.Bärnighausen T, Chaiyachati K, Chimbindi N, Peoples A, Haberer J, Newell M-L. Interventions to increase antiretroviral adherence in sub-Saharan Africa: a systematic review of evaluation studies. Lancet Infect Dis. 2011;11(12):942–951. doi: 10.1016/S1473-3099(11)70181-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Catalani C, Philbrick W, Fraser H, Mechael P, Israelski D M. mHealth for HIV treatment & prevention: a systematic review of the literature. Open AIDS J. 2013;7:17–41. doi: 10.2174/1874613620130812003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Devi B R, Syed-Abdul S, Kumar A et al. mHealth: An updated systematic review with a focus on HIV/AIDS and tuberculosis long term management using mobile phones. Comput Methods Programs Biomed. 2015;122(02):257–265. doi: 10.1016/j.cmpb.2015.08.003. [DOI] [PubMed] [Google Scholar]
- 17.Hall A K, Cole-Lewis H, Bernhardt J M. Mobile text messaging for health: a systematic review of reviews. Annu Rev Public Health. 2015;36:393–415. doi: 10.1146/annurev-publhealth-031914-122855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Burns K, Keating P, Free C. A systematic review of randomised control trials of sexual health interventions delivered by mobile technologies. BMC Public Health. 2016;16(01):778. doi: 10.1186/s12889-016-3408-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jeffery R A, Navarro T, Wilczynski N L et al. Adherence measurement and patient recruitment methods are poor in intervention trials to improve patient adherence. J Clin Epidemiol. 2014;67(10):1076–1082. doi: 10.1016/j.jclinepi.2014.06.008. [DOI] [PubMed] [Google Scholar]
- 20.Chaiyachati K H, Ogbuoji O, Price M, Suthar A B, Negussie E K, Bärnighausen T. Interventions to improve adherence to antiretroviral therapy: a rapid systematic review. AIDS. 2014;28 02:S187–S204. doi: 10.1097/QAD.0000000000000252. [DOI] [PubMed] [Google Scholar]
- 21.Belzer M E, MacDonell K K, Clark L F et al. Acceptability and feasibility of a cell phone support intervention for youth living with HIV with nonadherence to antiretroviral therapy. AIDS Patient Care STDS. 2014;6(29):338–345. doi: 10.1089/apc.2014.0282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hightow-Weidman L B, Muessig K E, Bauermeister J, Zhang C, LeGrand S. Youth, technology, and HIV: recent advances and future directions. Curr HIV/AIDS Rep. 2015;12(04):500–515. doi: 10.1007/s11904-015-0280-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Navarra A D, Gwadz M V, Whittemore R et al. Health technology-enabled interventions for adherence support and retention in care among US HIV-infected adolescents and young adults: an integrative review. AIDS Behav. 2017;21(11):3154–3171. doi: 10.1007/s10461-017-1867-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Moher D, Liberati A, Tetzlaff J, Altman D G; PRISMA Group.Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement PLoS Med 2009607e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Berlin J A; University of Pennsylvania Meta-analysis Blinding Study Group.Does blinding of readers affect the results of meta-analyses? Lancet 1997350(9072):185–186. [DOI] [PubMed] [Google Scholar]
- 26.Ammassari A, Trotta M P, Shalev N et al. Timed short messaging service improves adherence and virological outcomes in HIV-1-infected patients with suboptimal adherence to antiretroviral therapy. J Acquir Immune Defic Syndr. 2011;58(04):e113–e115. doi: 10.1097/QAI.0b013e3182359d2a. [DOI] [PubMed] [Google Scholar]
- 27.Perera A I, Thomas M G, Moore J O, Faasse K, Petrie K J. Effect of a smartphone application incorporating personalized health-related imagery on adherence to antiretroviral therapy: a randomized clinical trial. AIDS Patient Care STDS. 2014;28(11):579–586. doi: 10.1089/apc.2014.0156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Evans D, Berhanu R, Moyo F, Nguweneza A, Long L, Fox M P. Can short-term use of electronic patient adherence monitoring devices improve adherence in patients failing second-line antiretroviral therapy? Evidence from a pilot study in Johannesburg, South Africa. AIDS Behav. 2016;20(11):2717–2728. doi: 10.1007/s10461-016-1417-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.da Costa T M, Barbosa B J, Gomes e Costa D A et al. Results of a randomized controlled trial to assess the effects of a mobile SMS-based intervention on treatment adherence in HIV/AIDS-infected Brazilian women and impressions and satisfaction with respect to incoming messages. Int J Med Inform. 2012;81(04):257–269. doi: 10.1016/j.ijmedinf.2011.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Nsagha D S, Lange I, Fon P N, Nguedia Assob J C, Tanue E A. A randomized controlled trial on the usefulness of mobile text phone messages to improve the quality of care of HIV and AIDS patients in Cameroon. Open AIDS J. 2016;10:93–103. doi: 10.2174/1874613601610010093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Pop-Eleches C, Thirumurthy H, Habyarimana J P et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011;25(06):825–834. doi: 10.1097/QAD.0b013e32834380c1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Maduka O, Tobin-West C I. Adherence counseling and reminder text messages improve uptake of antiretroviral therapy in a tertiary hospital in Nigeria. Niger J Clin Pract. 2013;16(03):302–308. doi: 10.4103/1119-3077.113451. [DOI] [PubMed] [Google Scholar]
- 33.Rodrigues R, Shet A, Antony J et al. Supporting adherence to antiretroviral therapy with mobile phone reminders: results from a cohort in South India. PLoS One. 2012;7(08):e40723. doi: 10.1371/journal.pone.0040723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sabin L L, Bachman DeSilva M, Gill C J et al. Improving adherence to antiretroviral therapy with triggered real-time text message reminders: the China adherence through technology study. J Acquir Immune Defic Syndr. 2015;69(05):551–559. doi: 10.1097/QAI.0000000000000651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Garofalo R, Kuhns L M, Hotton A, Johnson A, Muldoon A, Rice D. A randomized controlled trial of personalized text message reminders to promote medication adherence among HIV-positive adolescents and young adults. AIDS Behav. 2016;20(05):1049–1059. doi: 10.1007/s10461-015-1192-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Hardy H, Kumar V, Doros G et al. Randomized controlled trial of a personalized cellular phone reminder system to enhance adherence to antiretroviral therapy. AIDS Patient Care STDS. 2011;25(03):153–161. doi: 10.1089/apc.2010.0006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lewis M A, Uhrig J D, Bann C M et al. Tailored text messaging intervention for HIV adherence: a proof-of-concept study. Health Psychol. 2013;32(03):248–253. doi: 10.1037/a0028109. [DOI] [PubMed] [Google Scholar]
- 38.Haberer J E, Musiimenta A, Atukunda E C et al. Short message service (SMS) reminders and real-time adherence monitoring improve antiretroviral therapy adherence in rural Uganda. AIDS. 2016;30(08):1295–1300. doi: 10.1097/QAD.0000000000001021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Orrell C, Cohen K, Mauff K, Bangsberg D R, Maartens G, Wood R. A randomized controlled trial of real-time electronic adherence monitoring with text message dosing reminders in people starting first-line antiretroviral therapy. AIDS. 2015;70(05):495–502. doi: 10.1097/QAI.0000000000000770. [DOI] [PubMed] [Google Scholar]
- 40.Kassaye S G, Ong'ech J, Sirengo M et al. Cluster-randomized controlled study of SMS text messages for prevention of mother-to-child transmission of HIV in rural Kenya. Aids Res Treat. 2016;2016:1.289328E6. doi: 10.1155/2016/1289328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mbuagbaw L, Thabane L, Ongolo-Zogo P et al. The Cameroon Mobile Phone SMS (CAMPS) trial: a randomized trial of text messaging versus usual care for adherence to antiretroviral therapy. PLoS One. 2012;7(12):e46909. doi: 10.1371/journal.pone.0046909. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Kalichman S C, Kalichman M O, Cherry C, Eaton L A, Cruess D, Schinazi R F. Randomized factorial trial of phone-delivered support counseling and daily text message reminders for HIV treatment adherence. J Acquir Immune Defic Syndr. 2016;73(01):47–54. doi: 10.1097/QAI.0000000000001020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ingersoll K S, Dillingham R A, Hettema J E et al. Pilot RCT of bidirectional text messaging for ART adherence among nonurban substance users with HIV. Health Psychol. 2015;34S:1305–1315. doi: 10.1037/hea0000295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Moore D J, Poquette A, Casaletto K B et al. Individualized texting for adherence building (iTAB): improving antiretroviral dose timing among HIV-infected persons with co-occurring bipolar disorder. AIDS Behav. 2015;19(03):459–471. doi: 10.1007/s10461-014-0971-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Linnemayr S, Huang H, Luoto J et al. Text messaging for improving antiretroviral adherence: no effect after 1 year in a randomized controlled trial among adolescents and young adults. Am J Public Health. 2017;107(12):1944–1950. doi: 10.2105/AJPH.2017.304089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Stankievich E, Malanca A, Foradori I, Ivalo S, Losso M. Utility of mobile communication devices as a tool to improve adherence to antiretroviral treatment in HIV-infected children and young adults in Argentina. Pediatr Infect Dis J. 2018;37(04):345–348. doi: 10.1097/INF.0000000000001807. [DOI] [PubMed] [Google Scholar]
- 47.Ruan Y, Xiao X, Chen J, Li X, Williams A B, Wang H. Acceptability and efficacy of interactive short message service intervention in improving HIV medication adherence in Chinese antiretroviral treatment-naïve individuals. Patient Prefer Adherence. 2017;11:221–228. doi: 10.2147/PPA.S120003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Georgette N, Siedner M J, Petty C R, Zanoni B C, Carpenter S, Haberer J E. Impact of a clinical program using weekly Short Message Service (SMS) on antiretroviral therapy adherence support in South Africa: a retrospective cohort study. BMC Med Inform Decis Mak. 2017;17(01):18. doi: 10.1186/s12911-017-0413-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.King E, Kinvig K, Steif J et al. Mobile text messaging to improve medication adherence and viral load in a vulnerable Canadian population living with human immunodeficiency virus: a repeated measures study. J Med Internet Res. 2017;19(06):e190. doi: 10.2196/jmir.6631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Abdulrahman S A, Rampal L, Ibrahim F, Radhakrishnan A P, Kadir Shahar H, Othman N. Mobile phone reminders and peer counseling improve adherence and treatment outcomes of patients on ART in Malaysia: a randomized clinical trial. PLoS One. 2017;12(05):e0177698. doi: 10.1371/journal.pone.0177698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Haubrich R H, Little S J, Currier J S et al. The value of patient-reported adherence to antiretroviral therapy in predicting virologic and immunologic response. AIDS. 1999;13(09):1099–1107. doi: 10.1097/00002030-199906180-00014. [DOI] [PubMed] [Google Scholar]
- 52.Nieuwkerk P T, Oort F J. Self-reported adherence to antiretroviral therapy for HIV-1 infection and virologic treatment response: a meta-analysis. J Acquir Immune Defic Syndr. 2005;38(04):445–448. doi: 10.1097/01.qai.0000147522.34369.12. [DOI] [PubMed] [Google Scholar]
- 53.Simoni J M, Kurth A E, Pearson C R, Pantalone D W, Merrill J O, Frick P A. Self-report measures of antiretroviral therapy adherence: a review with recommendations for HIV research and clinical management. AIDS Behav. 2006;10(03):227–245. doi: 10.1007/s10461-006-9078-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Hinkin C H, Hardy D J, Mason K I et al. Medication adherence in HIV-infected adults: effect of patient age, cognitive status, and substance abuse. AIDS. 2004;18 01:S19–S25. doi: 10.1097/00002030-200418001-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Bonnet F, Amieva H, Marquant F et al. Cognitive disorders in HIV-infected patients: are they HIV-related? AIDS. 2013;27(03):391–400. doi: 10.1097/QAD.0b013e32835b1019. [DOI] [PubMed] [Google Scholar]
- 56.Ajose O, Mookerjee S, Mills E J, Boulle A, Ford N. Treatment outcomes of patients on second-line antiretroviral therapy in resource-limited settings: a systematic review and meta-analysis. AIDS. 2012;26(08):929–938. doi: 10.1097/QAD.0b013e328351f5b2. [DOI] [PubMed] [Google Scholar]
- 57.Telecommunication Union World Telecommunication/ ICT Indicators database; World Development Indicators database (IT.CEL. SETS.P2, IT.MLT.MAIN.P2). Available at:https://data.worldbank.org/indicator/IT.CEL.SETS.P2. Accessed January 3, 2018