

Abstract
Silicone implant incompatibility syndrome (SIIS) has been identified as a cause of systemic symptoms such as lymphadenopathy, myalgia, and dyspnea in patients with silicone implants. We present a case of 76-year-old female patient, treated for carcinoma left breast with mastectomy and silicone breast implant, chemotherapy, and radiotherapy 42 years ago. There was a history of implant rupture and removal 2 years ago. The patient presented with right axillary swelling and dyspnea. 18-fluorine fluoro-deoxy-glucose positron emission tomography/computed tomography (F-18 FDG PET-CT) showed mildly FDG-avid left anterior chest wall and right rectus abdominis deposits, multiple lymph nodes, and low-grade FDG-avid pneumonitis changes in both lungs. Biopsy from the chest wall and rectus abdominis deposit was negative for malignancy and revealed foamy histiocytes and foreign-body giant cell reaction, indicative of SIIS. SIIS is a mimic for metastases and should be considered as a differential diagnosis in FDG PET-CT interpretation in patients with silicone breast implant.
Keywords: Autoimmune/inflammatory syndrome induced by adjuvants, breast implant rupture, fluorodeoxyglucose positron emission tomography-computed tomography, intramuscular deposit, silicone implant incompatibility syndrome
Introduction
Silicone Implant Incompatibility Syndrome (SIIS) is known to produce the autoimmune/inflammatory syndrome induced by adjuvants (ASIA) including systemic symptoms such as lymphadenopathy, myalgia, arthralgia, dyspnea, sicca syndrome, and others.[1] It was first described five decades ago as adjuvant breast disease in patients with breast implant and unexplained systemic symptoms.[2] We report a case of breast cancer with silicone implant rupture, who developed similar symptoms and had subcutaneous and intramuscular deposits mimicking metastases.
Case Report
A 76-year-old female patient, a known case of carcinoma left breast, was treated 42 years ago by performing left mastectomy and silicone breast implantation, followed by systemic chemotherapy and radiotherapy. There was a history of implant rupture and removal 2 years ago. Four months ago, patient had presented with palpable lymph nodes in the right axilla. On evaluation with mammography of the right breast and ultrasonography, right breast was normal, there were multiple enlarged the right axillary and left supraclavicular nodes. Fine-needle aspiration cytology (FNAC) of the right axillary nodes showed reactive lymphadenitis. Aspirate was negative for fungal, acid-fast bacilli, Gram-stain, culture, and Mycobacterium tuberculosis complex. Now, patient had presented with dyspnea on exertion, not associated with chest pain. There was no history of a cough or fever. On evaluation with contrast-enhanced computed tomography (CT) of chest, there were well-defined enhancing subcutaneous nodular deposits with soft-tissue attenuation in the anterior chest wall to the left of sternum, enlarged right axillary, left cervical, supraclavicular and mediastinal lymph nodes, suggestive of recurrence in the surgical bed with multi-nodal involvement. Ground-glass opacities, centrilobular nodules, and fibrotic changes were noted in both lungs suggestive of pneumonitis. 18-Fluorine Fluoro-deoxy-glucose positron emission tomography with CT (F-18 FDG PET-CT) [Figure 1] showed mildly FDG-avid enhancing nodular soft tissue deposits in the anterior chest wall to the left of sternum (maximum standardized uptake value [SUV max] 3.8) [Figure 1b], a similar enhancing intramuscular deposit in right rectus abdominis (SUV max 3.8) [Figure 1c], left supraclavicular (SUV max 3.2), level V cervical (SUV max 3.4), right axillary (SUV max 4.0), subpectoral (SUV max 4.3) [Figure 1d], left internal mammary (SUV max 3.4), mediastinal (SUV max 4.0), retroperitoneal (SUV max 3.9), pelvic (SUV max 4.7) [Figure 1c] and inguinal (SUV max 4.5) nodes. Low-grade FDG-avid pneumonitis changes were also noted in both lungs.
Figure 1.
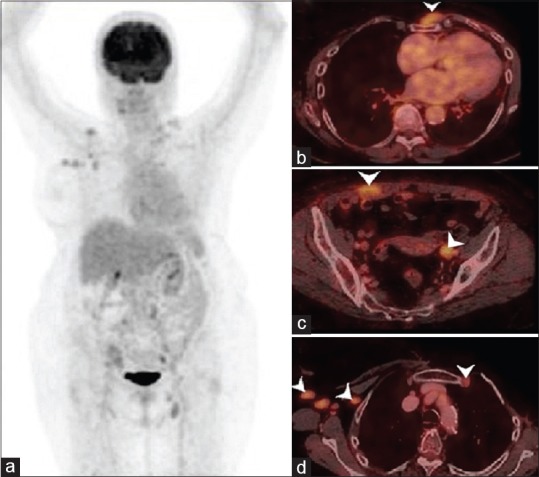
(a) 18-fluorine fluoro-deoxy-glucose positron emission tomography/computed tomography maximum intensity projection image showing tracer uptake in the right axillary, left supraclavicular, left common iliac and left inguinal regions. Focal tracer uptake in right shoulder corresponds to degenerative changes in the acromioclavicular joint. (b-d) Axial fused positron emission tomography/computed tomography images showing mild 18-fluorine fluoro-deoxy-glucose uptake in subcutaneous nodule in the anterior chest wall, deposit in right rectus abdominis muscle, left external iliac, right axillary, subpectoral, and left internal mammary nodes (arrow heads)
Biopsy from subcutaneous deposit in the chest wall, intramuscular deposit in right rectus abdominis muscle [Figure 2a and b], and right common iliac node showed foamy histiocytes, lymphocytes and foreign-body giant cell reaction indicative of SIIS and was negative for granuloma, atypia, or malignancy.
Figure 2.
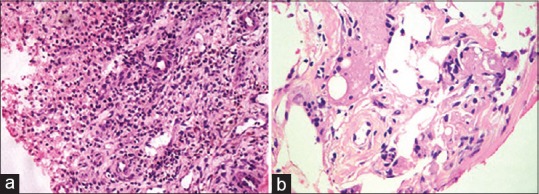
(a) Histopathological examination of chest wall nodule showing fibrocollagenous stroma, histiocytes, lymphocytes, and proliferating blood vessels (H and E, ×20). (b) Histopathological examination of rectus abdominis deposit showing fibroadipose tissue, foamy histiocytes, and giant cells (H and E, ×40)
Discussion
Maijers et al. reported symptoms of dyspnea and lymphadenopathy as a part of ASIA due to SIIS in about 35% and 45% of women with silicone breast implants, respectively.[1] Silicone breast implants develop a connective tissue capsule around them after implantation. Contracture of this capsule causes silicone from the implant to “bleed” through the capsule even in the absence of rupture, which reaches the regional lymph nodes causing silicone lymphadenopathy[3,4,5] and may form subcutaneous nodules known as silicone granulomas or siliconomas.[3,4] This may mimic metastasis in a known case of breast cancer.
The silicone released is engulfed by macrophages and gets trapped in lysosomes. This causes activation of macrophages, production of cytokines and reactive oxygen species which in turn lead to apoptosis of the macrophages. As a result, there is the release of silicone which is further engulfed by other macrophages and the cycle continues.[6] The FNAC picture of silicone lymphadenopathy has been reported to show foamy macrophages and multinucleated giant cells and may have cytoplasmic vacuolation with lymphoid cells in the background.[7] The presence of FDG-avid intramuscular deposit at a distant site has not yet been reported in SIIS or ASIA in the literature to the best of our knowledge and forms a great mimic for disease recurrence or metastases on follow-up evaluation with CT or FDG PET-CT even after decades of treatment in a known case of primary breast malignancy. Few cases reported in the literature with false-positive finding on FDG PET-CT due to SIIS are summarized in Table 1.[8,9,10,11,12,13]
Table 1.
Summary of studies reporting false positive findings due to SIIS on FDG PET-CT

ASIA describes a spectrum of immune-mediated diseases as a result of acute or chronic exposure to adjuvants such as silicone, vaccines, and others.[1,2,3] There have been case reports on patients with silicone breast implants presenting with type IV delayed hypersensitivity reaction.[14] Histologically, there is chronic inflammation showing granulation tissue and foreign-body reaction[15] which in this case, has been revealed on biopsy of the lymph node, subcutaneous, and intramuscular deposits.
This case highlights the importance of the knowledge that F-18 FDG-avid intramuscular deposit at a distant site, apart from lymphadenopathy and subcutaneous chest wall deposits can be caused by SIIS which may mimic metastases. Furthermore, worth noting is that the latent period for presentation with symptoms of SIIS is long and patient rarely may present years after removal of the ruptured implant as in this case. Hence, detailed surgical history, history of implant placement, and rupture or removal of the implant are important in cases of carcinoma breast.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Maijers MC, de Blok CJ, Niessen FB, van der Veldt AA, Ritt MJ, Winters HA, et al. Women with silicone breast implants and unexplained systemic symptoms: A descriptive cohort study. Neth J Med. 2013;71:534–40. [PubMed] [Google Scholar]
- 2.Colaris MJL, de Boer M, van der Hulst RR, Cohen Tervaert JW. Two hundreds cases of ASIA syndrome following silicone implants: A comparative study of 30 years and a review of current literature. Immunol Res. 2017;65:120–8. doi: 10.1007/s12026-016-8821-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Perricone C, Colafrancesco S, Mazor RD, Soriano A, Agmon-Levin N, Shoenfeld Y, et al. Autoimmune/inflammatory syndrome induced by adjuvants (ASIA) 2013: Unveiling the pathogenic, clinical and diagnostic aspects. J Autoimmun. 2013;47:1–6. doi: 10.1016/j.jaut.2013.10.004. [DOI] [PubMed] [Google Scholar]
- 4.Guerrissi JO. Asia syndrom: Diagnosis and surgical approach. Austin J Surg. 2017;4:1093. [Google Scholar]
- 5.De Backer H, Darquennes K, Dooms C, Yserbyt J, Coolen J, Verschakelen J, et al. The inner and outer of our thorax: Silicone breast implants and pulmonary alveolar proteinosis. Acta Clin Belg. 2015;70:384–6. doi: 10.1179/2295333715Y.0000000035. [DOI] [PubMed] [Google Scholar]
- 6.Cohen Tervaert JW, Kappel RM. Silicone implant incompatibility syndrome (SIIS): A frequent cause of ASIA (Shoenfeld's syndrome) Immunol Res. 2013;56:293–8. doi: 10.1007/s12026-013-8401-3. [DOI] [PubMed] [Google Scholar]
- 7.Zardawi I, Pickering A. Fine needle aspiration appearances of silicone lymphadenopathy. Med Sci Case Rep. 2014;1:36–8. [Google Scholar]
- 8.D’hulst L, Nicolaij D, Beels L, Gheysens O, Alaerts H, Van de Wiele C, et al. False-positive axillary lymph nodes due to silicone adenitis on (18) F-FDG PET/CT in an oncological setting. J Thorac Oncol. 2016;11:e73–5. doi: 10.1016/j.jtho.2016.01.001. [DOI] [PubMed] [Google Scholar]
- 9.Sutton EJ, Watson EJ, Gibbons G, Goldman DA, Moskowitz CS, Jochelson MS, et al. Incidence of internal mammary lymph nodes with silicone breast implants at MR imaging after oncoplastic surgery. Radiology. 2015;277:381–7. doi: 10.1148/radiol.2015142717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Soudack M, Yelin A, Simansky D, Ben-Nun A. Fluorodeoxyglucose – Positive internal mammary lymph node in breast cancer patients with silicone implants: Is it always metastatic cancer? Eur J Cardiothorac Surg. 2013;44:79–82. doi: 10.1093/ejcts/ezs625. [DOI] [PubMed] [Google Scholar]
- 11.Adejolu M, Huo L, Rohren E, Santiago L, Yang WT. False-positive lesions mimicking breast cancer on FDG PET and PET/CT. AJR Am J Roentgenol. 2012;198:W304–14. doi: 10.2214/AJR.11.7130. [DOI] [PubMed] [Google Scholar]
- 12.Bauer RP, Krajicek JB, Daniels EC, Shah SS, Ryu HJ. Silicone breast implant-induced lymphadenopathy: 18 cases. Respir Med CME. 2011;4:126–30. [Google Scholar]
- 13.Chen CJ, Lee BF, Yao WJ, Wu PS, Chen WC, Peng SL, et al. A false positive F-FDG PET/CT scan caused by breast silicone injection. Korean J Radiol. 2009;10:194–6. doi: 10.3348/kjr.2009.10.2.194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rider K, Kaya H, Gutierrez G. Dyspnea associated with silicone breast implant rupture. Eurasian J Pulmonol. 2015;17:117–8. [Google Scholar]
- 15.Mendes PR, Bins-Ely J, Lima EA, Vasconcellos ZA, d’Acampora AJ, Neves RD, et al. Histological study on acute inflammatory reaction to polyurethane-coated silicone implants in rats. Acta Cir Bras. 2008;23:93–101. doi: 10.1590/s0102-86502008000100015. [DOI] [PubMed] [Google Scholar]