

Abstract
Background
A drug provocation test using a sodium channel blocker (SCB) can unmask a type 1 ECG pattern in patients with Brugada syndrome. However, the prognostic value of the results of an SCB challenge is limited in patients with non–type 1 ECG. We investigated the associations of future risk for ventricular fibrillation with SCB‐induced ECG changes and ventricular tachyarrhythmias (VTAs).
Methods and Results
We administered intravenous pilsicainide to 245 consecutive patients with Brugada syndrome (181 patients with spontaneous type 1 ECG, 64 patients with non–type 1 ECG). ECG parameters before and after the test and occurrence of drug‐induced VTAs were evaluated. During a mean follow‐up period of 113±57 months, fatal VTA events occurred in 31 patients (sudden death: n=3, ventricular tachycardia/ventricular fibrillation: n=28). Symptomatic patients and spontaneous type 1 ECG were associated with future fatal arrhythmic events. Univariable analysis of ECG parameters after the test showed that long PQ and QRS intervals, high ST level, and SCB‐induced VTAs were associated with later VTA events during follow‐up. Multivariable analysis showed that symptomatic patients, high ST level (V1) ≥0.3 mV after the test, and SCB‐induced VTAs were independent predictors for future fatal arrhythmic events (hazard ratios: 3.28, 2.80, and 3.62, 95% confidence intervals: 1.54–7.47, 1.32–6.35, and 1.64–7.75, respectively; P<0.05).
Conclusions
SCB‐induced VTAs and ST‐segment augmentation are associated with an increased risk of the development of ventricular tachycardia/ventricular fibrillation events during follow‐up in patients with Brugada syndrome.
Keywords: Brugada syndrome, risk stratification, sodium channel blocker, ventricular fibrillation
Subject Categories: Ventricular Fibrillation, Sudden Cardiac Death
Clinical Perspective
What Is New?
Remarkable ST elevation and ventricular tachyarrhythmia induced by a challenge test with a sodium channel blocker were associated with arrhythmic events during follow‐up in patients with Brugada syndrome.
The prognostic value of a sodium channel blocker is applicable to patients with spontaneous type 1 ECG.
The present study indicated the usefulness of a sodium channel blocker test in patients with spontaneous type 1 ECG for the first time.
What Are the Clinical Implications?
A sodium channel blocker test can be used for (1) diagnosis of patients with non–type 1 ECG; (2) risk stratification in asymptomatic patients with spontaneous type 1 ECG; and (3) risk stratification in patients with spontaneous type 1 ECG and syncope of unknown cause.
Introduction
A sodium channel blocker (SCB) unmasks and augments type 1 ST elevation of Brugada syndrome (BrS). An SCB challenge is usually used to detect manifestation of type 1 ECG for diagnosis of BrS in patients with non–type 1 ECG.1 The extents of PQ prolongation and QRS widening during the SCB test can be a clue for the existence of SCN5A mutation.2, 3, 4 Although the SCB test is essential for diagnosis in non–type 1 patients, an unexpected response to administration of an SCB, such as atrioventricular block or ventricular tachyarrhythmias (VTAs), occasionally emerges in some patients.5, 6
The prognostic value of the results of an SCB challenge is limited in patients with BrS. Patients who have drug‐induced type 1 ECG, with the exception of patients who have already experienced cardiac arrest, show a relatively benign clinical course compared with that for patients with spontaneous type 1 ECG.7, 8, 9 Patients in whom ECG was not converted to type 1 ECG by an SCB had a very good prognosis compared with that for patients with drug‐induced type 1 ECG.10 SCB challenge only has diagnostic value in patients without spontaneous type 1 ECG. Moreover, the prognostic significance of an SCB challenge in patients with spontaneous type 1 ECG has not been evaluated. In fact, most investigators believe that an SCB test is contraindicated in patients with spontaneous type 1 ECG.
Recently, an SCB challenge has been used for detecting abnormal potentials on the epicardial surface of the right ventricle during epicardial catheter ablation. Symptomatic patients who have experienced arrhythmic syncope or documented VTA events have more advanced arrhythmogenic substrate on the epicardium.11 If an SCB challenge can unmask concealed substrate in patients, ECG change and VTAs induced by the SCB will indicate progression of the substrate.
We hypothesized that remarkable ECG changes and VTAs provoked by an SCB challenge are associated with advanced arrhythmogenic substrate and that such changes are correlates of future VTA events in patients with BrS.
Methods
The authors declare that all supporting data are available within the article and its online supplementary files.
The subjects of the present study were 245 consecutive patients with BrS who underwent a drug provocation test with pilsicainide in Okayama University Hospital (males: 240 patients, mean age: 46±13 years). At the time of diagnosis, 154 patients were asymptomatic, 79 had syncope, and 12 had ventricular fibrillation (VF) (Table 1). We excluded obvious reflex syncope as a symptom and considered patients with reflex syncope as being asymptomatic. BrS was diagnosed when a type 1 ST‐segment elevation appeared either spontaneously or after administration of an SCB. We defined spontaneous type 1 ECG as the appearance of type 1 ECG without any stress such as stress from fever or exercise. Type 1 ECG was defined as coved ST‐segment elevation ≥2 mm in at least 1 right precordial lead in the second, third, or fourth intercostal space.12 All 245 patients had spontaneous (n=181) or drug‐induced type 1 ECG (n=64). To clarify the prognosis of patients with negative SCB and non–type 1, we also analyzed an additional 30 patients (29 males, age: 46±15 years) without positive SCB test who were suspected of having BrS (asymptomatic: 20 patients, syncope: 10 patients). There were no patients from the same family. Echocardiography was performed in all patients, and no structural abnormalities were found.
Table 1.
Characteristics of Patients With Spontaneous and Drug‐Induced Type 1 ECG
| Overall, n=245 | P Valuea | |
|---|---|---|
| Clinical parameters | ||
| Male | 240 (98%) | ··· |
| Age, y | 46.2±13.0 | ··· |
| Symptomatic patients | 91 (37%) | ··· |
| Syncope | 79 (32%) | ··· |
| VT/VF | 12 (5%) | ··· |
| Family history of SD | 72 (29%) | ··· |
| SCN5A mutation | 16/139 (12%) | ··· |
| VT/VF during follow‐up | 31 (13%) | ··· |
| ECG parameters | ||
| Spontaneous type 1 ECG | 181 (74%) | ··· |
| PQ interval lead II (ms) | ||
| Pre SCB | 180±27 | <0.001 |
| Post SCB | 229±37 | |
| QRS width (ms) | ||
| V1 | ||
| Pre SCB | 106±14 | <0.001 |
| Post SCB | 133±23 | |
| V2 | ||
| Pre SCB | 107±14 | <0.001 |
| Post SCB | 135±23 | |
| ST level (mV) | ||
| V1 | ||
| Pre SCB | 0.158±0.106 | <0.001 |
| Post SCB | 0.270±0.172 | |
| V2 | ||
| Pre SCB | 0.294±0.160 | <0.001 |
| Post SCB | 0.591±0.277 | |
| QTc interval (ms) | ||
| V5 | ||
| Pre SCB | 388±27 | <0.001 |
| Post SCB | 427±35 | |
| Drug‐induced VTAs (n) | ||
| Overall | 24 (10%) | ··· |
| PVCs | 13 (5%) | ··· |
| VTs | 11 (4%) | ··· |
PVCs indicates premature ventricular contractions; SCB, sodium channel blocker; SD, sudden death; VTA, ventricular tachyarrhythmia; VT/VF, ventricular tachycardia/ventricular fibrillation.
P value: comparison of ECG parameters before and after the SCB test.
All of the study protocols were approved by the Ethics Committee on Human Research and Epidemiology of Okayama University and Human Genome Studies of the Ethics Committee of Okayama University. Informed consent regarding data acquisition was obtained from all patients. Clinical data, including data on age, sex, family history of sudden cardiac death, history of syncope episodes, history of VF episodes, and the presence of SCN5A gene mutation were obtained from patient records. Analysis of SCN5A mutation was performed in 139 patients in compliance with the above guidelines.
The primary end point of this study was the occurrence of fatal VTA events defined as the occurrence of sudden cardiac death, VT or VF, and appropriate implantable cardioverter‐defibrillator interventions during the follow‐up period.
Pharmacologic Challenge Test
We performed an SCB test in an ECG laboratory or during electrophysiological study with a standby defibrillator and an emergency cart with medicines and intubation kit during hospitalization. Pilsicainide chloride was administered intravenously at a dose of 1 mg/kg over a period of 5 to 10 minutes in all patients. The difference between ECG parameters before and 15 minutes after administration of pilsicainide was calculated: PQ interval in lead II, QRS interval and ST level in leads V1 and V2, and QTc interval in lead V5. ST level was measured at the J points in leads V1, V2, and V5. Occurrence of severe VTAs after administration of pilsicainide was also evaluated. Severe VTAs during the test included frequent occurrence of premature ventricular contractions (PVCs) (>1 bpm) and polymorphic VT (at least 3 continuous beats). We stopped administration of pilsicainide if patients had significant QRS widening (≥130%), second‐ or third‐degree atrioventricular block, or occurrence of PVCs. If patients had severe ventricular arrhythmias, we observed the patients overnight in a cardiac care unit with or without isoproterenol infusion.
Statistical Analysis
Statistical analysis was performed using JMP 11.0 for MAC (SAS Institute Inc, Cary, NC). Data are expressed as means±SD or medians (interquartile range). Continuous variables in the different subgroups were analyzed by the Wilcoxon signed‐rank test. We used the paired t test or the Wilcoxon signed‐rank test to compare the values before and after the SCB test in the same patients. Categorical data and percentage frequencies were analyzed by the χ2 test or Fisher test. Logistic regression analysis was conducted in order to identify predictive ECG parameters before and after the pilsicainide‐challenge test. Receiver‐operating characteristic curves were constructed for ECG parameters to determine the optimal cutoff value for identifying patients with VF during follow‐up. Event rate curves were plotted according to the Kaplan–Meier method and were analyzed by the log‐rank test. Univariate and multivariate Cox regression analyses were performed to assess whether each index can be a significant and independent predictor of fatal arrhythmic events. We used the following covariates for multivariable analysis: important baseline characteristics (symptoms and spontaneous type 1 ECG) and ECG parameters after the pilsicainide test (PQ and QRS intervals, ST level, and pilsicainide‐induced VTAs). A value of P<0.05 was considered statistically significant.
Results
Characteristics of Patients and Results of the Pilsicainide Test
Baseline characteristics of the patients according to clinical presentation are summarized in Table 1. Spontaneous type 1 ECG was observed in 74% of the patients. Thirty‐two percent of the patients had a history of syncope episodes and 5% of the patients had previous VF episodes. Gene analysis was performed in 139 patients, and SCN5A gene mutation was found in 12% of the patients.
The reasons for performing the pilsicainide test were diagnosis of BrS in patients without spontaneous type 1 ECG (n=62), confirmation of type 1 ECG in patients who transiently had type 1 ECG with or without specific conditions (such as fever, after exercise, or after taking medicine, n=2), detection of an abnormal endocardial or epicardial electrogram or induction of PVCs during electrophysiological study and/or catheter ablation (n=131), and possibility of risk stratification for detecting abnormal ECGs such as T‐wave alternans (n=50).13, 14 The reasons for performing the SCB test in patients with nonspontaneous type 1 ECG were existence of ECG abnormality (35 asymptomatic patients) and existence of syncope (26 patients) or VF (3 patients).
Administration of pilsicainide unmasked type 1 ECG in all of the 64 patients who did not have spontaneous type 1 ECG. ST level was significantly augmented after the pilsicainide test (Table 1). Pilsicainide prolonged PQ, QRS, and QTc intervals. Pilsicainide induced VTAs in 24 patients (Figure 1), including frequent PVCs in 13 patients (Figure 2A) and VT/VF in 11 patients (Figures 2B and 3, Tables 1 and 2). Cardioversion was required to terminate VT/VF in 4 patients (external defibrillator: n=3, implantable cardioverter‐defibrillator: n=1). None of the patients had prolonged VT/VF episodes. One patient developed transient complete atrioventricular block. Patients with pilsicainide‐induced VTA more frequently had spontaneous type 1 ECG, higher ST level after the test (V1), and longer QT interval than did patients without pilsicainide‐induced VTA (Table 3).
Figure 1.
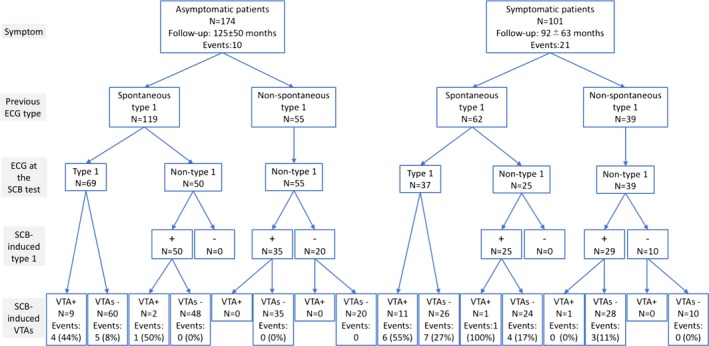
Results of pilsicainide tests and occurrence of cardiac events. The groups of patients consisted of 245 patients with spontaneous or drug‐induced type 1 ECG and 30 patients with non–type 1 ECG that was not converted to type 1 ECG by a sodium channel blocker (SCB). The results were divided according to the symptom, ECG type, ECG type at the pilsicainide test, result of the pilsicainide test, and occurrence of pilsicainide‐induced ventricular arrhythmias (VTAs).
Figure 2.
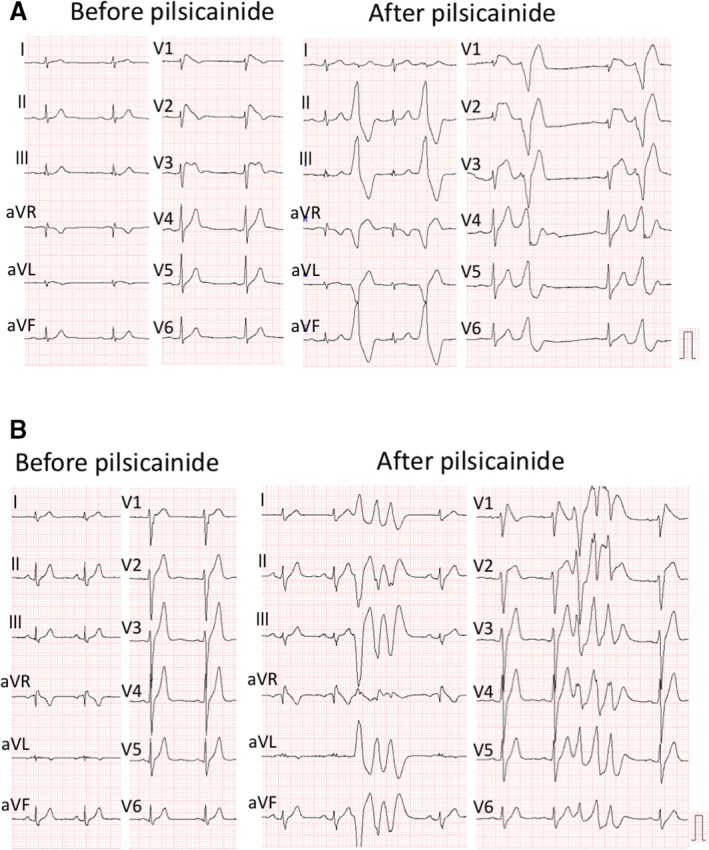
Pilsicainide‐induced ventricular arrhythmia. A, These ECGs were recorded in a patient with syncope (50 years old). The left panel shows ECG at baseline. Leads V1‐2 were located at the third intercostal space. The patient had spontaneous type 1 ECG only in the leads at high intercostal spaces. The right panel shows that pilsicainide provoked frequent occurrence of premature ventricular contractions and significant ST elevation. B, These ECGs were recorded in an asymptomatic patient (27 years old). The patient had fever‐induced type 1 ECG but did not have spontaneous type 1 ECG. The left panel shows non–type 1 ECG before the pilsicainide test. Leads V1‐2 were recorded at regular lead positions. The right panel shows that pilsicainide induced nonsustained polymorphic ventricular tachycardia. The patient died suddenly at night 6 years after the test.
Figure 3.
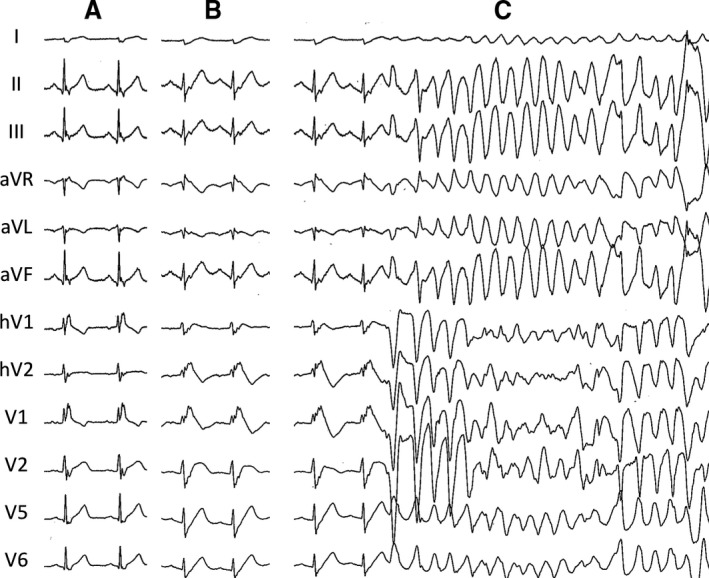
Pilsicainide‐induced polymorphic ventricular tachycardia and ventricular fibrillation. These ECGs were recorded in a 50‐year‐old patient with ventricular fibrillation (VF). A, ECG at baseline. The patient had spontaneous type 1 ECG, but ST elevation was diminished before the test. We performed a pilsicainide test to unmask the abnormal electrical substrate during electrophysiological study. Pilsicainide provoked type 1 ECG (B) and VF (C). A direct current shock was required to terminate VF.
Table 2.
Patients With Pilsicainide‐Induced Ventricular Arrhythmia
| Patients | Age (y) | Sex | Spontaneous Type 1 | Clinical Presentation | FH of SD | VF Induction by PES | SCN5A Mutation | Type of SCB‐VTA | ICD Implantation During Follow‐Up | VTA During Follow‐Up |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 50 | Male | Yes | Asymptomatic | Yes | Yes | No | Frequent PVC | No | Sustained VT |
| 2 | 27 | Male | Yes | Asymptomatic | No | Yes | No | Frequent PVC | No | None |
| 3 | 55 | Male | Yes | Syncope | No | Yes | No | VF | Yes | Appropriate ICD shock |
| 4 | 41 | Male | Yes | VF | No | Yes | No | NSVT | Yes | Appropriate ICD shock |
| 5 | 55 | Male | Yes | VF | Yes | Yes | No | Frequent PVC | Yes | Appropriate ICD shock |
| 6 | 42 | Male | No | VF | No | Yes | No | Frequent PVC | Yes | None |
| 7 | 41 | Male | Yes | Syncope | No | No | No | NSVTa | Yes | None |
| 8 | 57 | Male | Yes | Asymptomatic | No | No | No | Frequent PVC | No | None |
| 9 | 47 | Male | Yes | Syncope | Yes | No | Yes | Frequent PVC | Yes | Appropriate ICD shock |
| 10 | 29 | Male | Yes | Syncope | Yes | No | Yes | Sustained VTa | No | None |
| 11 | 40 | Male | Yes | Asymptomatic | Yes | Yes | No | NSVT | Yes | None |
| 12 | 50 | Male | Yes | Syncope | No | Yes | No | VF | Yes | Appropriate ICD shock |
| 13 | 42 | Male | Yes | Asymptomatic | No | Yes | No | Frequent PVC | Yes | Appropriate ICD shock |
| 14 | 38 | Male | Yes | Asymptomatic | Yes | Yes | No | Frequent PVC | No | None |
| 15 | 34 | Male | Yes | Syncope | Yes | Yes | No | Frequent PVC | Yes | Appropriate ICD shock |
| 16 | 38 | Male | Yes | Syncope | No | No | Yes | NSVT | No | None |
| 17 | 50 | Male | Yes | Asymptomatic | No | Yes | NA | NSVTa | Yes | None |
| 18 | 27 | Male | Yes | Asymptomatic | Yes | Yes | No | NSVT | No | SD |
| 19 | 50 | Male | Yes | Syncope | No | Yes | NA | Sustained VT | No | VF |
| 20 | 36 | Male | Yes | Syncope | Yes | Yes | No | NSVT | Yes | None |
| 21 | 74 | Male | Yes | Asymptomatic | Yes | Yes | NA | Frequent PVC | Yes | Sustained VT |
| 22 | 36 | Male | Yes | Asymptomatic | No | Yes | NA | Frequent PVC | Yes | Appropriate ICD shock |
| 23 | 25 | Male | Yes | Syncope | No | No | Yes | VTa/VF | Yes | Appropriate ICD shock |
| 24 | 41 | Male | Yes | Asymptomatic | No | Yes | NA | Frequent PVC | No | None |
FH indicates family history; ICD, implantable cardioverter defibrillator; NA, not assessed; NSVT, nonsustained ventricular tachycardia; PES, programmed electrical stimulation; PVC, premature ventricular contraction; SCB, sodium channel blocker; SD, sudden death; VF, ventricular fibrillation; VT, ventricular tachycardia; VTA, ventricular tachyarrhythmia.
VT with wide QRS complex and not significant polymorphic change.
Table 3.
Different Characteristics of Patients With and Those Without SCB‐Induced VTAs
| Pilsicainide‐Induced VTA+ (n=24) | Pilsicainide‐Induced VTA− (n=221) | P Valuea | |
|---|---|---|---|
| Clinical parameters | |||
| Male | 24 (100%) | 216 (98%) | 1.0000 |
| Age, y | 42.7±11.3 | 46.6±13.2 | 0.1478 |
| Symptomatic patients | 13 (54%) | 78 (35%) | 0.0782 |
| Syncope | 9 (38%) | 70 (32%) | 0.6464 |
| VT/VF | 4 (17%) | 8 (4%) | 0.0207 |
| Family history of SD | 10 (42%) | 62 (28%) | 0.1659 |
| SCN5A mutation | 4/20 (20%) | 12/119 (10%) | 0.2386 |
| VT/VF during follow‐up | 12 (50%) | 19 (9%) | <0.0001 |
| ECG parameters | |||
| Spontaneous type 1 ECG | 23 (96%) | 158 (71%) | 0.0068 |
| PQ interval in lead II (ms) | |||
| Pre SCB | 185±26 | 180±27 | 0.3227 |
| Post SCB | 242±43 | 227±36 | 0.0578 |
| QRS width (ms) | |||
| V1 | |||
| Pre SCB | 113±22 | 105±13 | 0.0969 |
| Post SCB | 145±36 | 131±21 | 0.0576 |
| V2 | |||
| Pre SCB | 114±21 | 106±13 | 0.0429 |
| Post SCB | 146±33 | 134±22 | 0.0748 |
| ST level (mV) | |||
| V1 | |||
| Pre SCB | 0.200±0.132 | 0.153±0.102 | 0.0307 |
| Post SCB | 0.385±0.219 | 0.257±0.162 | 0.0037 |
| V2 | |||
| Pre SCB | 0.307±0.194 | 0.293±0.157 | 0.9613 |
| Post SCB | 0.599±0.295 | 0.91±0.276 | 0.8236 |
| QTc interval (ms) | |||
| V5 | |||
| Pre SCB | 387±29 | 388±27 | 0.8371 |
| Post SCB | 450±43 | 424±33 | 0.0046 |
All patients had type 1 ECG spontaneously or by SCB. SCB indicates sodium channel blocker; SD, sudden death; VTA, ventricular tachyarrhythmia; VT/VF, ventricular tachycardia/ventricular fibrillation.
P value: comparison of ECG parameters in patients with and without pilsicainide‐induced VTAs.
During a mean follow‐up period of 113±57 months, fatal VTA events occurred in 31 patients. Three patients died suddenly, 26 experienced VF (implantable cardioverter‐defibrillator shock in 24 patients, aborted cardiac arrest in 2 patients), and 2 developed monomorphic VTs. The time to a fatal VTA event was shorter in patients with spontaneous type 1 ECG than in patients without spontaneous type 1 ECG (Figure 4A), and the same result was observed in patients’ subgroups according to symptoms (Figure 4B). There was no VTA event in patients without a positive SCB test. Patients with pilsicainide‐induced VTA had more frequent fatal VTA events during follow‐up (12/24, event ratio: 7.1%/y) than did patients without pilsicainide‐induced VTA (19/221, event ratio: 0.89%, P<0.0001) (Figure 4C). There was no difference in fatal VTA events during follow‐up between patients with pilsicainide‐induced VT/VF (5/11, event ratio: 6.3%) and patients with pilsicainide‐induced PVCs only (7/13, event ratio: 7.9%, P=0.6820).
Figure 4.
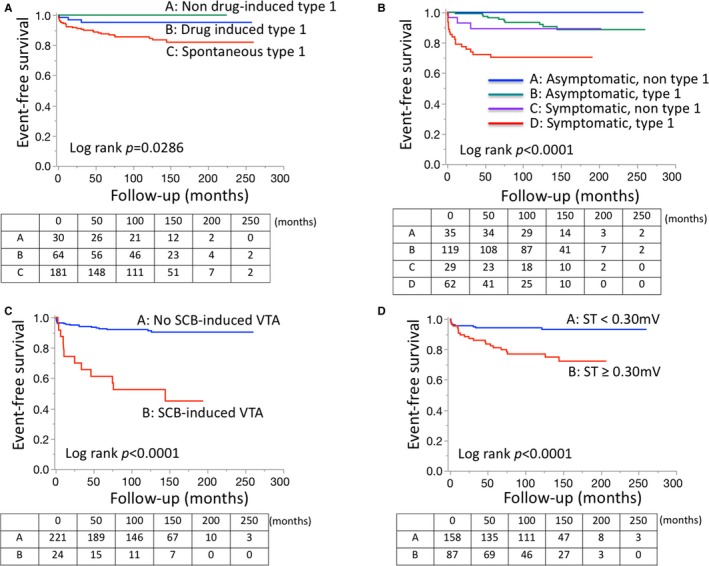
Kaplan–Meier analysis of fatal arrhythmic events. A, Event‐free survival by ECG types including non–type 1, drug‐induced type 1, and spontaneous type 1. Patients with spontaneous type 1 ECG had a worse prognosis than did patients without spontaneous type 1 ECG. No arrhythmic event occurred in patients without type 1 ECG. B, Event‐free survival by symptoms and ECG types in patients with spontaneous or drug‐induced type 1 ECG. Symptomatic patients more frequently experienced arrhythmic events than did asymptomatic patients. C, Event‐free survival by pilsicainide‐induced ventricular tachyarrhythmias (VTAs) in patients with spontaneous or drug‐induced type 1 ECG. Pilsicainide‐induced VTAs were associated with increased risk of fatal arrhythmic events. D, Event‐free survival by degree of ST elevation in patients with spontaneous or drug‐induced type 1 ECG. Patients with marked ST elevation (≥0.3 mV) in lead V1 after administration of pilsicainide had a significantly higher risk of fatal arrhythmic events than did patients with less ST elevation. Tables under the survival curve show the number of patients at risk. SCB indicates sodium channel blocker.
Changes in ECG Parameters and Occurrence of Ventricular Arrhythmias Induced by Pilsicainide in Different Subgroups of Patients
Pilsicainide significantly prolonged QRS interval and significantly augmented ST elevation in patients with spontaneous type 1 ECG compared with those in patients without spontaneous type 1 ECG (Table 4). At the time of the SCB test, 75 patients (41%) in whom spontaneous type 1 ECG was recorded previously did not show spontaneous type 1 ECG at the beginning of the test. Pilsicainide provoked type 1 ECG in those patients (Figure 1). PQ and QTc intervals before and after the pilsicainide test were not different between patients with and without spontaneous type 1 ECG. Pilsicainide more frequently induced VTAs in patients with spontaneous type 1 ECG than in patients without spontaneous type 1 ECG (Table 4).
Table 4.
Differences Between Patients With Spontaneous and Drug‐Induced Type 1 ECG
| Spontaneous Type 1 (n=181) | Drug‐Induced type1 (n=64) | P Valuea | |
|---|---|---|---|
| Clinical parameters | |||
| Male | 179 (99%) | 61 (95%) | 0.1135 |
| Age, y | 46.0±12.9 | 46.8±13.5 | 0.5918 |
| Symptomatic patients | 62 (34%) | 29 (45%) | 0.133 |
| Syncope | 53 (29%) | 26 (41%) | 0.1194 |
| VT/VF | 9 (5%) | 3 (5%) | 1.0000 |
| Family history of SD | 56 (31%) | 16 (25%) | 0.4265 |
| SCN5A mutation | 13/109 (12%) | 3/30 (10%) | 1.0000 |
| VT/VF during follow‐up | 28 (15%) | 3 (5%) | 0.0257 |
| ECG parameters | |||
| Spontaneous type 1 ECG | 181 (100%) | 0 | ··· |
| PQ interval in lead II (ms) | |||
| Pre SCB | 181±27 | 180±25 | 0.9877 |
| Post SCB | 230±38 | 226±35 | 0.4217 |
| QRS width (ms) | |||
| V1 | |||
| Pre SCB | 108±14 | 101±14 | 0.0004 |
| Post SCB | 134±23 | 128±22 | 0.0085 |
| V2 | |||
| Pre SCB | 108±14 | 102±14 | 0.0011 |
| Post SCB | 136±23 | 130±25 | 0.0041 |
| ST level (mV) | |||
| V1 | |||
| Pre SCB | 0.180±0.111 | 0.096±0.059 | <0.0001 |
| Post SCB | 0.303±0.182 | 0.177±0.094 | <0.0001 |
| V2 | |||
| Pre SCB | 0.331±0.163 | 0.190±0.094 | <0.0001 |
| Post SCB | 0.644±0.276 | 0.444±0.226 | <0.0001 |
| QTc interval (ms) | |||
| V5 | |||
| Pre SCB | 387±27 | 392±27 | 0.2183 |
| Post SCB | 427±36 | 425±31 | 0.7757 |
| Drug‐induced VTA (n) | |||
| Overall | 23 (13%) | 1 (2%) | 0.0068 |
| PVCs | 12 (7%) | 1 (2%) | 0.193 |
| VTs | 11 (6%) | 0 (0%) | 0.071 |
PVCs indicates premature ventricular contractions; SCB, sodium channel blocker; SD, sudden death; VTA, ventricular tachyarrhythmia; VT/VF, ventricular tachycardia/ventricular fibrillation.
P value: comparison of ECG parameters in patients with and those without spontaneous type 1 ECG.
Symptomatic patients had a longer PQ interval but had a lower ST level in V2 than did asymptomatic patients at baseline (Table 5). There were no differences in other ECG parameters between asymptomatic and symptomatic patients at baseline. Pilsicainide significantly prolonged PQ and QRS intervals in leads V1 and V2 in symptomatic patients compared with those in asymptomatic patients. ST level in lead V2 in asymptomatic patients was higher than that in symptomatic patients after pilsicainide administration. Pilsicainide‐induced VT/VF was more frequent in symptomatic patients than in asymptomatic patients (Table 5).
Table 5.
Characteristics of Patients With Symptoms at Initial Visit to the Hospital
| Symptoms | Asymptomatic (n=154) | Symptomatic (n=91) | P Valuea |
|---|---|---|---|
| Clinical parameters | |||
| Male | 151 (98%) | 89 (98%) | 1 |
| Age, y | 46.3±13.4 | 46.0±12.4 | 0.9576 |
| Symptomatic patients | 0 | 91 | ··· |
| Syncope | 0 | 79 | ··· |
| VT/VF | 0 | 12 | ··· |
| Family history of SD | 51 (33%) | 21 (23%) | 0.1110 |
| SCN5A mutation | 6/80 (8%) | 10/59 (17%) | 0.1121 |
| VT/VF during follow‐up | 10 (6%) | 21 (23%) | 0.0003 |
| ECG parameters | |||
| Spontaneous type 1 ECG | 119 (77%) | 62 (68%) | 0.133 |
| PQ interval in lead II (ms) | |||
| Pre SCB | 177±24 | 187±29 | 0.0084 |
| Post SCB | 223±34 | 238±40 | 0.0027 |
| QRS width (ms) | |||
| V1 | |||
| Pre SCB | 105±12 | 107±18 | 0.8629 |
| Post SCB | 130±20 | 137±27 | 0.02 |
| V2 | |||
| Pre SCB | 106±11 | 108±18 | 0.7396 |
| Post SCB | 131±21 | 140±26 | 0.0026 |
| ST level (mV) | |||
| V1 | |||
| Pre SCB | 0.162±0.109 | 0.151±0.102 | 0.4899 |
| Post SCB | 0.273±0.174 | 0.264±0.171 | 0.8308 |
| V2 | |||
| Pre SCB | 0.319±0.164 | 0.251±0.145 | 0.0012 |
| Post SCB | 0.634±0.282 | 0.520±0.256 | 0.0025 |
| QTc interval (ms) | |||
| V5 | |||
| Pre SCB | 386±28 | 392±26 | 0.1491 |
| Post SCB | 424±35 | 432±35 | 0.0837 |
| Drug‐induced VTA (n) | |||
| Overall | 11 (7%) | 13 (14%) | 0.0782 |
| PVCs | 8 (5%) | 5 (5%) | 1 |
| VTs | 3 (2%) | 8 (9%) | 0.0213 |
All patients had type 1 ECG spontaneously or by SCB. PVCs indicates premature ventricular contractions; SCB, sodium channel blocker; SD, sudden death; VTA, ventricular tachyarrhythmia; VT/VF, ventricular tachycardia/ventricular fibrillation.
P value: comparison of ECG parameters in asymptomatic patients and symptomatic patients.
Patients with SCN5A mutation (n=16) had longer PQ interval before the pilsicainide test than did patients without SCN5A mutation (n=123) (Table S1). After administration of pilsicainide, patients with SCN5A mutation had significantly longer PQ and QRS intervals than did patients without SCN5A mutation. There were no differences in prevalence of drug‐induced VTAs and other ECG parameters before and after the pilsicainide test between patients with and without SCN5A mutation.
Risk Factors for VT/VF Events During Follow‐Up
Table 6 shows results of univariable analysis of clinical and ECG parameters before and after the pilsicainide test to detect VTA events during follow‐up. Univariable analysis of clinical parameters showed that symptomatic patients, especially those with previous episodes of VT/VF, were associated with fatal arrhythmic events during follow‐up. In ECG parameters before the pilsicainide test, QRS intervals in leads V1 and V2 were associated with cardiac events. Univariable analysis of ECG parameters after the pilsicainide test to detect VTA events showed that PQ interval, QRS intervals (V1 and V2), and ST level (V1) were associated with fatal arrhythmic events during follow‐up. Among the differences between ECG parameters before and after the pilsicainide test, differences in PQ interval (ΔPQ) and ST level (ΔST) in V1 were predictors of VT/VF events. Drug‐induced VTAs were also associated with fatal arrhythmic events during follow‐up, but there was no difference in prediction of fatal events between drug‐induced PVCs and drug‐induced VT/VF.
Table 6.
HR for Predicting VTA Events
| HR | 95% CI | P Value | |
|---|---|---|---|
| Clinical parameters | |||
| Male | 0.62 | 0.13 to 10.98 | 0.6588 |
| Age, y | 0.99 | 0.96 to 1.02 | 0.5741 |
| Symptomatic patients | 4.35 | 2.10 to 9.67 | <0.0001 |
| Syncope | 1.49 | 0.70 to 3.05 | 0.2851 |
| VT/VF | 13.81 | 5.97 to 29.39 | <0.0001 |
| Family history of SD | 1.12 | 0.51 to 2.32 | 0.7657 |
| SCN5A mutation | 1.90 | 0.64 to 4.62 | 0.2253 |
| ECG parameters | |||
| Spontaneous type 1 ECG | 3.72 | 1.09 to 12.69 | 0.0279 |
| PQ interval in lead II | |||
| Pre SCB | 1.01 | 0.99 to 1.02 | 0.3054 |
| Post SCB | 1.01 | 1.00 to 1.02 | 0.0006 |
| ΔPQ | 1.02 | 1.01 to 1.03 | 0.0066 |
| QRS width | |||
| V1 | |||
| Pre SCB | 1.03 | 1.01 to 1.04 | 0.0109 |
| Post SCB | 1.01 | 1.00 to 1.02 | 0.0155 |
| ΔQRS | 1.01 | 0.99 to 1.02 | 0.2221 |
| V2 | |||
| Pre SCB | 1.03 | 1.01 to 1.04 | 0.0059 |
| Post SCB | 1.01 | 1.00 to 1.02 | 0.0157 |
| ΔQRS | 1.01 | 0.99 to 1.02 | 0.2798 |
| ST level | |||
| V1 | |||
| Pre SCB | 7.69 | 0.33 to 118.40 | 0.1914 |
| Post SCB | 11.43 | 2.03 to 54.72 | 0.0069 |
| ΔST | 12.14 | 1.55 to 66.11 | 0.0087 |
| V2 | |||
| Pre SCB | 0.78 | 0.07 to 6.84 | 0.8348 |
| Post SCB | 0.64 | 0.16 to to 2.34 | 0.512 |
| ΔST | 0.56 | 0.10 to 2.85 | 0.499 |
| QTc interval | |||
| V5 | |||
| Pre SCB | 1 | 0.99 to 1.01 | 0.8812 |
| Post SCB | 1.01 | 1.00 to 1.01 | 0.3075 |
| ΔQT | 1.01 | 0.99 to 1.02 | 0.1736 |
| Drug‐induced VTA | |||
| Overall | 6.95 | 3.28 to 14.19 | <0.0001 |
| PVCs | 6.36 | 2.53 to 14.05 | 0.0003 |
| VTs | 4.66 | 1.57 to 11.17 | 0.0082 |
HR of the ECG parameters represents risk increase/1 unit. CI indicates confidence interval; HR, hazard ratio for predicting VT/VF; PVCs, premature ventricular contractions; SCB, sodium channel blocker; SD, sudden death; VTA, ventricular tachyarrhythmia; VT/VF, ventricular tachycardia/ventricular fibrillation.
Cutoff points of ECG parameters after the pilsicainide test to detect fatal arrhythmic events during follow‐up were determined by receiver‐operating characteristic analysis: PQ interval ≥235 ms (area under the curve: 0.663), QRS interval in lead V1 ≥132 ms (area under the curve: 0.693), and ST level in lead V1 ≥0.3 mV (area under the curve 0.671) were optimal cutoff points (Figure S1). Univariable analysis of these parameters showed that they were associated with fatal VTA events: the hazard ratio (HR) of PQ interval ≥235 ms was 3.16 (95% confidence interval [CI], 1.54–6.85, P=0.0021), HR of QRS interval ≥132 ms was 4.22 (95% CI, 1.97–10.06, P=0.0005), and HR of ST level ≥0.3 mV was 4.03 (95% CI, 1.95–8.94, P=0.0003). When we focused on the asymptomatic patients, ST level after pilsicainide ≥0.3 mV (HR: 1.7, CI, 3.1–325.5, P=0.0002) and drug‐induced VTAs (HR: 15.6, CI, 4.3–56.1, P=0.0001) were also predictors of VT/VF events during follow‐up.
Multivariable analysis of baseline characteristics (symptoms and spontaneous type 1 ECG) and ECG parameters after the pilsicainide test (PQ and QRS intervals, ST level, and pilsicainide‐induced VTAs) showed that symptoms, ST level after the pilsicainide test, and drug‐induced VTAs were independent risk factors for fatal arrhythmic events during follow‐up (Table 7). Patients with high ST level in lead V1 after the pilsicainide test or drug‐induced VTAs had a shorter time to fatal events than did patients without these parameters (Figure 4C and 4D).
Table 7.
Multivariable Analysis of Clinical and ECG Parameters for Predicting VTA Events
| HR | 95% CI | P Value | |
|---|---|---|---|
| Baseline clinical parameters | |||
| Symptomatic patients | 3.28 | 1.54 to 7.47 | 0.0019 |
| Spontaneous type 1 ECG | 1.76 | 0.57 to 7.78 | 0.3496 |
| ECG parameters after SCB test | |||
| PQ interval ≥235 ms | 1.60 | 0.73 to 3.65 | 0.2399 |
| QRS interval ≥132 ms | 2.22 | 0.98 to 5.53 | 0.0559 |
| ST level ≥0.3 mV | 2.80 | 1.32 to 6.35 | 0.0067 |
| SCB‐induced VTAs | 3.62 | 1.64 to 7.75 | 0.0019 |
CI indicates confidence interval; HR, hazard ratio; SCB, sodium channel blocker; VTA, ventricular tachyarrhythmia.
Discussion
New Findings
The present study showed that high ST level in lead V1 after the pilsicainide test and drug‐induced VTAs were associated with VT/VF events. These risk factors detected by the SCB test were independent predictors of cardiac events even after adjustment by the presence of symptoms and spontaneous type 1 ECG. There has been no report of ECG changes after an SCB test other than the appearance of drug‐induced type 1 ECG having prognostic value. The results of the present study showed that an SCB test is useful as a risk stratification tool in patients with spontaneous type 1 ECG in addition to being a diagnostic tool in patients without spontaneous type 1 ECG.
Occurrence and Prognostic Value of SCB‐Induced Ventricular Arrhythmias
Previous studies showed that an SCB test induced VTAs in 0% to 25% of patients and VF in up to 4% of patients with BrS.13, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34 The incidence of SCB‐induced VTAs increased if the subjects of the study included subjects with spontaneous type 1 ECG. In the present study, 10% of the patients developed VT/VF or frequent PVCs after administration of pilsicainide, and the incidence of SCB‐induced VTAs coincided with that in previous studies that included subjects with spontaneous type 1 ECG.
We showed that pilsicainide‐induced VTA was a powerful predictor of VT/VF after adjustment of symptoms and ECG type. Some studies have shown that SCB‐induced VTAs failed to predict VT/VF events during follow‐up.19, 27, 34 However, those studies included a small number of patients or only patients without spontaneous type 1 ECG. The present study included patients with spontaneous type 1 ECG (74%), and the occurrence of SCB‐induced VTAs in patients without spontaneous type 1 ECG was less frequent than that in patients with spontaneous type 1 ECG. Then the prognostic value of SCB‐induced VTAs should be significant in patients with spontaneous type 1 ECG. Recently, an SCB test has been used to unmask concealed substrate at the time of epicardial ablation.11 Application of radiofrequency energy to all abnormal substrate is necessary to eliminate the arrhythmogenic area. ECG changes similar to those induced by an SCB test can appear during febrile illness,35 and VTA events also occur at that time. Thus, VTAs induced by an SCB test are not proarrhythmic effects but represent concealed arrhythmogenic substrate that can appear in daily life.
Some asymptomatic patients without spontaneous type 1 ECG might have false‐positive results of the SCB test.36, 37 This study included 35 asymptomatic patients with nonspontaneous type 1 ECG that was converted to type 1 ECG by the pilsicainide test (Figure 1). This group of patients was diagnosed as “possible” BrS by a new scoring system,38 and some of those patients might be false positive. However, those patients did not have pilsicainide‐induced VTAs and did not have cardiac events during follow‐up. Thus, SCB‐induced VTAs would indicate that the patients have “definite” BrS 38 with a more progressive arrhythmogenic substrate.
Risk and Safety of an SCB Test in Patients With Type 1 ECG
An SCB test is useful and safe for most patients, but some studies have shown that some patients develop severe VTAs requiring external defibrillation, implantable cardioverter‐defibrillator therapy, or an extracorporeal membrane oxygenator.6, 13, 15, 19, 23, 28, 31, 34 An SCB test should be performed during hospitalization, and continuous infusion of low‐dose isoproterenol after the test should be performed overnight for high‐risk patients. To avoid catastrophic events, it was stated in the Consensus report that an SCB test should be discontinued in cases of frequent PVCs and QRS widening.38 The present study showed that high ST level and prolonged QT interval after the test occurred in patients with pilsicainide‐induced VTAs (Table 3), and these ECG changes can be warning signs of drug‐induced VTAs. Since most of the pilsicainide‐induced VTAs occurred in patients with spontaneous type 1 ECG, an SCB test should be performed in such patients with meticulous caution regarding ECG changes during the test.
Based on the results of this study, we consider that the criteria for performing an SCB test are (1) diagnosis of patients with non–type 1 ECG; (2) risk stratification in asymptomatic patients with spontaneous type 1 ECG; and (3) risk stratification in patients with spontaneous type 1 ECG and syncope of unknown cause.
Limitations
Female sex is a possible risk for arrhythmic events during an SCB test.6 We could not determine sex risk of the SCB test in this study because we performed the test in only 5 female patients (2%). PVC/VT did not occur in all of the female patients. We did not avoid performing an SCB test for female patients. A high prevalence of males (>90% of the patients) with BrS was frequently observed in previous Japanese studies,27, 39 and it might be a racial characteristic of BrS.
Conclusion
VTAs and augmentation of ST‐segment elevation after an SCB challenge test were associated with an increased risk of the development of VT/VF events in patients with BrS, especially in patients with spontaneous type 1 ECG. An SCB challenge test can serve as not only a diagnostic tool in patients without spontaneous type 1 ECG but also a risk stratification tool for patients with spontaneous type 1 ECG.
Sources of Funding
This study was supported by JSPS KAKENHI (15K09082 to Morita) and Tailor‐made Medical Treatment Program with the BioBank Japan Project (BBJ) from Japan Agency for Medical Research and Development (AMED) (15km0305015h0101 to Morita).
Disclosures
Morita and Nishii are affiliated with the endowed department by Japan Medtronic Inc. The remaining authors have no disclosures to report.
Supporting information
Table S1. Different Characteristics of Patients With and Those Without SCN5A Mutations
Figure S1. Receiver operating curves (ROC) for fatal arrhythmic events during follow‐up. ROC curves of PQ interval (A), ST level in lead V1 (B), and QRS interval in lead V1 (C) after administration of pilsicainide.
(J Am Heart Assoc. 2018;7:e008617 DOI: 10.1161/JAHA.118.008617.)29748178
References
- 1. Antzelevitch C, Brugada P, Borggrefe M, Brugada J, Brugada R, Corrado D, Gussak I, LeMarec H, Nademanee K, Perez Riera AR, Shimizu W, Schulze‐Bahr E, Tan H, Wilde A. Brugada syndrome: report of the second consensus conference: endorsed by the Heart Rhythm Society and the European Heart Rhythm Association. Circulation. 2005;111:659–670. [DOI] [PubMed] [Google Scholar]
- 2. Smits JP, Eckardt L, Probst V, Bezzina CR, Schott JJ, Remme CA, Haverkamp W, Breithardt G, Escande D, Schulze‐Bahr E, LeMarec H, Wilde AA. Genotype‐phenotype relationship in Brugada syndrome: electrocardiographic features differentiate SCN5A‐related patients from non‐SCN5A‐related patients. J Am Coll Cardiol. 2002;40:350–356. [DOI] [PubMed] [Google Scholar]
- 3. Meregalli PG, Tan HL, Probst V, Koopmann TT, Tanck MW, Bhuiyan ZA, Sacher F, Kyndt F, Schott JJ, Albuisson J, Mabo P, Bezzina CR, Le Marec H, Wilde AA. Type of SCN5A mutation determines clinical severity and degree of conduction slowing in loss‐of‐function sodium channelopathies. Heart Rhythm. 2009;6:341–348. [DOI] [PubMed] [Google Scholar]
- 4. Hong K, Brugada J, Oliva A, Berruezo‐Sanchez A, Potenza D, Pollevick GD, Guerchicoff A, Matsuo K, Burashnikov E, Dumaine R, Towbin JA, Nesterenko V, Brugada P, Antzelevitch C, Brugada R. Value of electrocardiographic parameters and ajmaline test in the diagnosis of Brugada syndrome caused by SCN5A mutations. Circulation. 2004;110:3023–3027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Dobbels B, De Cleen D, Ector J. Ventricular arrhythmia during ajmaline challenge for the Brugada syndrome. Europace. 2016;18:1501–1506. [DOI] [PubMed] [Google Scholar]
- 6. Poli S, Toniolo M, Maiani M, Zanuttini D, Rebellato L, Vendramin I, Dametto E, Bernardi G, Bassi F, Napolitano C, Livi U, Proclemer A. Management of untreatable ventricular arrhythmias during pharmacologic challenges with sodium channel blockers for suspected Brugada syndrome. Europace. 2018;20:234–242. [DOI] [PubMed] [Google Scholar]
- 7. Probst V, Veltmann C, Eckardt L, Meregalli PG, Gaita F, Tan HL, Babuty D, Sacher F, Giustetto C, Schulze‐Bahr E, Borggrefe M, Haissaguerre M, Mabo P, Le Marec H, Wolpert C, Wilde AA. Long‐term prognosis of patients diagnosed with Brugada syndrome: results from the FINGER Brugada Syndrome Registry. Circulation. 2010;121:635–643. [DOI] [PubMed] [Google Scholar]
- 8. Priori SG, Gasparini M, Napolitano C, Della Bella P, Ottonelli AG, Sassone B, Giordano U, Pappone C, Mascioli G, Rossetti G, De Nardis R, Colombo M. Risk stratification in Brugada syndrome: results of the PRELUDE (PRogrammed ELectrical stimUlation preDictive valuE) registry. J Am Coll Cardiol. 2012;59:37–45. [DOI] [PubMed] [Google Scholar]
- 9. Sieira J, Ciconte G, Conte G, de Asmundis C, Chierchia GB, Baltogiannis G, Di Giovanni G, Saitoh Y, Casado‐Arroyo R, Julia J, La Meir M, Wellens F, Wauters K, Pappaert G, Brugada P. Long‐term prognosis of drug‐induced Brugada syndrome. Heart Rhythm. 2017;14:1427–1433. [DOI] [PubMed] [Google Scholar]
- 10. Brugada R, Brugada J, Antzelevitch C, Kirsch GE, Potenza D, Towbin JA, Brugada P. Sodium channel blockers identify risk for sudden death in patients with ST‐segment elevation and right bundle branch block but structurally normal hearts. Circulation. 2000;101:510–515. [DOI] [PubMed] [Google Scholar]
- 11. Brugada J, Pappone C, Berruezo A, Vicedomini G, Manguso F, Ciconte G, Giannelli L, Santinelli V. Brugada syndrome phenotype elimination by epicardial substrate ablation. Circ Arrhythm Electrophysiol. 2015;8:1373–1381. [DOI] [PubMed] [Google Scholar]
- 12. Priori SG, Wilde AA, Horie M, Cho Y, Behr ER, Berul C, Blom N, Brugada J, Chiang CE, Huikuri H, Kannankeril P, Krahn A, Leenhardt A, Moss A, Schwartz PJ, Shimizu W, Tomaselli G, Tracy C; Document R , Ackerman M, Belhassen B, Estes NA III, Fatkin D, Kalman J, Kaufman E, Kirchhof P, Schulze‐Bahr E, Wolpert C, Vohra J, Refaat M, Etheridge SP, Campbell RM, Martin ET, Quek SC; Heart Rhythm S, European Heart Rhythm A and Asia Pacific Heart Rhythm S . Executive summary: HRS/EHRA/APHRS expert consensus statement on the diagnosis and management of patients with inherited primary arrhythmia syndromes. Europace. 2013;15:1389–1406. [DOI] [PubMed] [Google Scholar]
- 13. Morita H, Morita ST, Nagase S, Banba K, Nishii N, Tani Y, Watanabe A, Nakamura K, Kusano KF, Emori T, Matsubara H, Hina K, Kita T, Ohe T. Ventricular arrhythmia induced by sodium channel blocker in patients with Brugada syndrome. J Am Coll Cardiol. 2003;42:1624–1631. [DOI] [PubMed] [Google Scholar]
- 14. Tada T, Kusano KF, Nagase S, Banba K, Miura D, Nishii N, Watanabe A, Nakamura K, Morita H, Ohe T. Clinical significance of macroscopic T‐wave alternans after sodium channel blocker administration in patients with Brugada syndrome. J Cardiovasc Electrophysiol. 2008;19:56–61. [DOI] [PubMed] [Google Scholar]
- 15. Therasse D, Sacher F, Petit B, Babuty D, Mabo P, Martins R, Jesel L, Maury P, Pasquie JL, Mansourati J, Dupuis JM, Kyndt F, Thollet A, Guyomarch B, Barc J, Schott JJ, Le Marec H, Redon R, Probst V, Gourraud JB. Sodium‐channel blocker challenge in the familial screening of Brugada syndrome: safety and predictors of positivity. Heart Rhythm. 2017;14:1442–1448. [DOI] [PubMed] [Google Scholar]
- 16. Ueyama T, Shimizu A, Yamagata T, Esato M, Ohmura M, Yoshiga Y, Kanemoto M, Kametani R, Sawa A, Suzuki S, Sugi N, Matsuzaki M. Different effect of the pure Na+ channel‐blocker pilsicainide on the ST‐segment response in the right precordial leads in patients with normal left ventricular function. Circ J. 2007;71:57–62. [DOI] [PubMed] [Google Scholar]
- 17. Hermida JS, Denjoy I, Jarry G, Jandaud S, Bertrand C, Delonca J. Electrocardiographic predictors of Brugada type response during Na channel blockade challenge. Europace. 2005;7:447–453. [DOI] [PubMed] [Google Scholar]
- 18. Batchvarov VN, Govindan M, Camm AJ, Behr ER. Significance of QRS prolongation during diagnostic ajmaline test in patients with suspected Brugada syndrome. Heart Rhythm. 2009;6:625–631. [DOI] [PubMed] [Google Scholar]
- 19. Conte G, Sieira J, Sarkozy A, de Asmundis C, Di Giovanni G, Chierchia GB, Ciconte G, Levinstein M, Casado‐Arroyo R, Baltogiannis G, Saenen J, Saitoh Y, Pappaert G, Brugada P. Life‐threatening ventricular arrhythmias during ajmaline challenge in patients with Brugada syndrome: incidence, clinical features, and prognosis. Heart Rhythm. 2013;10:1869–1874. [DOI] [PubMed] [Google Scholar]
- 20. Evain S, Briec F, Kyndt F, Schott JJ, Lande G, Albuisson J, Abbey S, Le Marec H, Probst V. Sodium channel blocker tests allow a clear distinction of electrophysiological characteristics and prognosis in patients with a type 2 or 3 Brugada electrocardiogram pattern. Heart Rhythm. 2008;5:1561–1564. [DOI] [PubMed] [Google Scholar]
- 21. Dubner S, Azocar D, Gallino S, Cerantonio AR, Muryan S, Medrano J, Bruno C. Single oral flecainide dose to unmask type 1 Brugada syndrome electrocardiographic pattern. Ann Noninvasive Electrocardiol. 2013;18:256–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Veltmann C, Wolpert C, Sacher F, Mabo P, Schimpf R, Streitner F, Brade J, Kyndt F, Kuschyk J, Le Marec H, Borggrefe M, Probst V. Response to intravenous ajmaline: a retrospective analysis of 677 ajmaline challenges. Europace. 2009;11:1345–1352. [DOI] [PubMed] [Google Scholar]
- 23. Rolf S. The ajmaline challenge in Brugada syndrome: diagnostic impact, safety, and recommended protocol. Eur Heart J. 2003;24:1104–1112. [DOI] [PubMed] [Google Scholar]
- 24. Morita H, Takenaka‐Morita S, Fukushima‐Kusano K, Kobayashi M, Nagase S, Kakishita M, Nakamura K, Emori T, Matsubara H, Ohe T. Risk stratification for asymptomatic patients with Brugada syndrome. Circ J. 2003;67:312–316. [DOI] [PubMed] [Google Scholar]
- 25. Kakihara J, Takagi M, Hayashi Y, Tatsumi H, Doi A, Yoshiyama M. Utility of 12‐lead and signal‐averaged Holter electrocardiograms after pilsicainide provocation for risk stratification in Brugada syndrome. Heart Vessels. 2017;32:1151–1159. [DOI] [PubMed] [Google Scholar]
- 26. Shimizu W, Antzelevitch C, Suyama K, Kurita T, Taguchi A, Aihara N, Takaki H, Sunagawa K, Kamakura S. Effect of sodium channel blockers on ST segment, QRS duration, and corrected QT interval in patients with Brugada syndrome. J Cardiovasc Electrophysiol. 2000;11:1320–1329. [DOI] [PubMed] [Google Scholar]
- 27. Chinushi M, Komura S, Izumi D, Furushima H, Tanabe Y, Washizuka T, Aizawa Y. Incidence and initial characteristics of pilsicainide‐induced ventricular arrhythmias in patients with Brugada syndrome. Pacing Clin Electrophysiol. 2007;30:662–671. [DOI] [PubMed] [Google Scholar]
- 28. Gasparini M, Priori SG, Mantica M, Napolitano C, Galimberti P, Ceriotti C, Simonini S. Flecainide test in Brugada syndrome: a reproducible but risky tool. Pacing Clin Electrophysiol. 2003;26:338–341. [DOI] [PubMed] [Google Scholar]
- 29. Wolpert C, Echternach C, Veltmann C, Antzelevitch C, Thomas GP, Spehl S, Streitner F, Kuschyk J, Schimpf R, Haase KK, Borggrefe M. Intravenous drug challenge using flecainide and ajmaline in patients with Brugada syndrome. Heart Rhythm. 2005;2:254–260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Zorzi A, Migliore F, Marras E, Marinelli A, Baritussio A, Allocca G, Leoni L, Perazzolo Marra M, Basso C, Buja G, Thiene G, Iliceto S, Delise P, Corrado D. Should all individuals with a nondiagnostic Brugada‐electrocardiogram undergo sodium‐channel blocker test? Heart Rhythm. 2012;9:909–916. [DOI] [PubMed] [Google Scholar]
- 31. Gandjbakhch E, Fressart V, Duthoit G, Marquie C, Deharo JC, Pousset F, Hebert JL, Simon F, Himbert C, Klug D, Charron P, Hidden‐Lucet F. Malignant response to ajmaline challenge in SCN5A mutation carriers: experience from a large familial study. Int J Cardiol. 2014;172:256–258. [DOI] [PubMed] [Google Scholar]
- 32. McMillan MR, Day TG, Bartsota M, Mead‐Regan S, Bryant R, Mangat J, Abrams D, Lowe M, Kaski JP. Feasibility and outcomes of ajmaline provocation testing for Brugada syndrome in children in a specialist paediatric inherited cardiovascular diseases centre. Open Heart. 2014;1:e000023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Meregalli PG, Ruijter JM, Hofman N, Bezzina CR, Wilde AA, Tan HL. Diagnostic value of flecainide testing in unmasking SCN5A‐related Brugada syndrome. J Cardiovasc Electrophysiol. 2006;17:857–864. [DOI] [PubMed] [Google Scholar]
- 34. Conte G, Dewals W, Sieira J, de Asmundis C, Ciconte G, Chierchia GB, Di Giovanni G, Baltogiannis G, Saitoh Y, Levinstein M, La Meir M, Wellens F, Pappaert G, Brugada P. Drug‐induced brugada syndrome in children: clinical features, device‐based management, and long‐term follow‐up. J Am Coll Cardiol. 2014;63:2272–2279. [DOI] [PubMed] [Google Scholar]
- 35. Mizusawa Y, Morita H, Adler A, Havakuk O, Thollet A, Maury P, Wang DW, Hong K, Gandjbakhch E, Sacher F, Hu D, Amin AS, Lahrouchi N, Tan HL, Antzelevitch C, Probst V, Viskin S, Wilde AA. Prognostic significance of fever‐induced Brugada syndrome. Heart Rhythm. 2016;13:1515–1520. [DOI] [PubMed] [Google Scholar]
- 36. Viskin S, Rosso R, Friedensohn L, Havakuk O, Wilde AA. Everybody has Brugada syndrome until proven otherwise? Heart Rhythm. 2015;12:1595–1598. [DOI] [PubMed] [Google Scholar]
- 37. Viskin S, Rosso R. Read my lips: a positive ajmaline test does not always mean you have Brugada syndrome. JACC Clin Electrophysiol. 2017;3:1409–1411. [DOI] [PubMed] [Google Scholar]
- 38. Antzelevitch C, Yan GX, Ackerman MJ, Borggrefe M, Corrado D, Guo J, Gussak I, Hasdemir C, Horie M, Huikuri H, Ma C, Morita H, Nam GB, Sacher F, Shimizu W, Viskin S, Wilde AA. J‐Wave syndromes expert consensus conference report: emerging concepts and gaps in knowledge. Heart Rhythm. 2016;13:e295–e324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Kamakura S, Ohe T, Nakazawa K, Aizawa Y, Shimizu A, Horie M, Ogawa S, Okumura K, Tsuchihashi K, Sugi K, Makita N, Hagiwara N, Inoue H, Atarashi H, Aihara N, Shimizu W, Kurita T, Suyama K, Noda T, Satomi K, Okamura H, Tomoike H; Brugada Syndrome Investigators in J . Long‐term prognosis of probands with Brugada‐pattern ST‐elevation in leads V1–V3. Circ Arrhythm Electrophysiol. 2009;2:495–503. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1. Different Characteristics of Patients With and Those Without SCN5A Mutations
Figure S1. Receiver operating curves (ROC) for fatal arrhythmic events during follow‐up. ROC curves of PQ interval (A), ST level in lead V1 (B), and QRS interval in lead V1 (C) after administration of pilsicainide.