

Abstract
Background
Lifestyle behaviors influence atherosclerotic cardiovascular disease (ASCVD) risk. We examined race and sex differences in the association of ASCVD risk with obesity and lifestyle behaviors.
Methods and Results
We used multivariable logistic regression to examine the association of race/ethnicity and sex with obesity and lifestyle behaviors among 12 351 adults in the National Health and Nutrition Examination Surveys cycles 2005 to 2014. Ten‐year ASCVD risk was estimated using the 2013 American College of Cardiology/American Heart Association pooled cohort equations. Among overweight/obese subjects, whites were more likely to consider themselves overweight, to report a desire to weigh less, and to report a healthy diet, and physical activity. Despite higher body mass index and/or ASCVD risk, black women (adj odds ratio [OR] 0.8, 95% confidence interval [CI], 0.7–0.9) were less likely to attempt weight loss, and Hispanic women (OR 0.8, 95% CI 0.6–0.9) were less likely to report physical activity than white women. Black women (adj OR 0.6, 95% CI 0.5–0.7) were less likely than white women, and Hispanics (women adj OR 0. 6, 95% CI 0.5–0.7; men adj OR 0.7, 95% CI 0.6–0.9) were less likely than whites to report a healthy diet. Among those with ASCVD risk >7.5%, there were even greater disparities in the likelihood of healthy diet between black and Hispanic versus white women, and among Hispanic versus white men.
Conclusions
Race/ethnic minorities are less likely to engage in healthy lifestyle behaviors despite higher body mass index and ASCVD risk. These findings underscore the need for culturally sensitive recommendations to improve cardiovascular outcomes in high‐risk populations, particularly minority women.
Keywords: lifestyle, obesity, race and ethnicity, risk factor, women
Subject Categories: Lifestyle, Obesity, Risk Factors, Race and Ethnicity, Women
Clinical Perspective
What Is New?
The likelihood of engaging in healthy lifestyle behaviors is more strongly influenced by body mass index and weight perception than by atherosclerotic cardiovascular disease risk scores.
Even among subjects with high atherosclerotic cardiovascular disease risk scores, the greatest differences in healthy lifestyle behaviors exist among black and Hispanic versus white women, and among Hispanic versus white men.
What Are the Clinical Implications?
Awareness of one's excess body weight may be a stronger motivator for healthy lifestyle behaviors than measured cardiovascular risk.
Desired weight and weight self‐perceptions vary by race/ethnicity and sex.
Thus, clinicians may need to tailor messages about heathy body mass index and body image to motivate engagement in healthy lifestyle behaviors, particularly among race/ethnic minority women.
Atherosclerotic cardiovascular disease (ASCVD) remains the leading cause of death in the United States, accounting for 31.3% of all deaths.1 Over the past few decades, a significant decline in age‐adjusted mortality from ASCVD has been observed in the United States, primarily related to improvements in medical and surgical treatments, as well as improvements in CVD risk factor burden. Between 2007 and 2013, death rates from CVD decreased for all race/ethnic groups in the United States. Despite these declines, disparities in the overall burden of ASCVD continue to exist according to race/ethnicity and sex. The overall rates of death attributable to CVD in 2013 were 356.7 per 100 000 for non‐Hispanic black men, 270.6 per 100 000 for non‐Hispanic white men, 197.4 per 100 000 for Hispanic men, and 246.6 per 100 000 for non‐Hispanic black women, 183.8 per 100 000 for non‐Hispanic white women, and 136.4 per 100 000 for Hispanic women.1
One explanation for the unequal decline in the rates of ASCVD by race/ethnicity is the high burden of CVD risk factors among race/ethnic minorities. Non‐Hispanic blacks in the United States have high rates of hypertension (untreated and uncontrolled), diabetes mellitus, obesity, and physical inactivity. Although rates of ASCVD are not as high in Hispanic Americans as in non‐Hispanic whites and blacks, the burden of traditional CVD risk factors including obesity, diabetes mellitus, and physical inactivity are also quite high in this group. The high prevalence of overweight and obesity in race/ethnic minority groups is particularly worrisome, since excess body weight contributes to most major CVD risk factors. The prevalence of obesity is highest among non‐Hispanic black adults (48.1%), followed by Hispanic (42.5%), non‐Hispanic white (34.5%), and non‐Hispanic Asian adults (11.7%).2 Moreover, important race/ethnic disparities in healthy lifestyle behaviors exist, with ≈1.8 in 10 non‐Hispanic whites, 1.3 in 10 Hispanics, and 1 in 10 non‐Hispanic blacks having at least 5 cardiovascular health metrics at ideal levels. Moreover, racial/ethnic differences in overall cardiovascular health may be more prominent for women than for men.3
Estimates suggest that ≈44% of the decline in ASCVD death rates is attributable to improvements in CVD‐related lifestyle and behavior factors, including improvements in rates of smoking, physical inactivity, and control of systolic blood pressure and total cholesterol.4 However, declines in the prevalence of these risk factors are being offset by the increasing prevalence of obesity and diabetes mellitus. In fact, it is possible that we may see a plateau in the improvements in ASCVD death rates because of this phenomenon over time. Thus, promotion of healthy lifestyle behaviors is crucial to maintaining the successes thus far achieved in ASCVD death.
In 2013, the American Heart Association and American College of Cardiology published a novel, comprehensive Pooled Cohort risk equation for the prediction of the 10‐year risk of developing ASCVD in non‐Hispanic blacks and whites age 40 to 79 years.5 This risk score does not incorporate data on overweight or obesity, and studies that have attempted to incorporate body mass index (BMI) into the ASCVD risk prediction models have found conflicting results.6, 7 Given that poor lifestyle behaviors are strong contributors to the risk of death, it is critical to continue to examine the association of CVD risk factors with patients’ lifestyle‐related risk factors. Moreover, it is necessary to perform race/ethnic‐ and sex‐ specific analyses, to determine whether the higher baseline cardiovascular risk in certain race/ethnic groups has a differential association with healthy lifestyle behaviors than in other groups. In this analysis, we utilized data from the National Health and Nutrition Examination Survey to examine the association between prevalence of overweight and obesity, ASCVD risk scores, and healthy lifestyle behaviors according to race/ethnicity and sex.
Methods
The data and study materials are publicly available.8 The analytic methods have been made available within the article to other researchers for purposes of reproducing the results or replicating the procedure.
Study Population
We analyzed data from the National Health and Nutrition Examination Survey (NHANES) from 2005 to 2014. NHANES is a continuous, annual survey involving participants from a nationally representative sample of noninstitutionalized US residents. NHANES includes a detailed household interview, physical examination, and laboratory information obtained through mobile examination centers. Informed consent is obtained from all NHANES participants by the mobile interviewer. To produce estimates with statistical reliability, we combined five 2‐year cycles of the continuous NHANES 2005 to 2006, 2007 to 2008, 2009 to 2010, 2011 to 2012, and 2013 to 2014. Unless otherwise noted, survey questions and methods were consistent in all 5 waves. NHANES 2003–2008 oversampled lower income people, adolescents 12 to 19 years, people >60 years of age, blacks, and Mexican Americans. Beginning in 2007, the entire Hispanic population was oversampled.9 Sampling weights for each respondent are provided by the National Center for Health Statistics and statistically take into account the unequal probabilities of selection because of sample design, nonresponse, planned oversampling, and the known US population distribution. Full details of the NHANES are available at http://www.cdc.gov/nchs/nhanes.htm. This study was approved by the Emory Institutional Review Board.
For this analysis, we included anyone with age >40 years or <79 years with self‐reported race/ethnicity of non‐Hispanic white, non‐Hispanic black, or Hispanic (Mexican American or other Hispanic) (N=15 241). We then excluded subjects for (1) self‐reported history of coronary heart disease, myocardial infarction, or stroke (N=1626), and (2) missing data on total cholesterol or high‐density lipoprotein cholesterol values (N=1264), leaving N=12 351 for the final analysis.
Physical Examination Variables
Blood pressure, body weight, and height were measured by certified examiners during the mobile examination center evaluation according to the NHANES study protocol. Mean systolic and diastolic blood pressure were calculated as the average of at least 3 separate measurements. BMI was calculated by dividing weight in kilograms by height in meters squared. BMI was further categorized as normal weight (BMI <25 kg/m2), overweight (BMI 25–29.99 kg/m2), or obese (BMI ≥30 kg/m2).
Questionnaire Variables
Trained interviewers questioned participants about their medical history, weight control, and healthy lifestyle behaviors using a computer‐assisted personal interviewing system. To assess medical history, participants were asked: “Has a doctor or other health professional ever told you that you (1) have high blood pressure, (2) have high cholesterol, (3) have diabetes mellitus, or (4) were overweight?” To assess history of smoking, participants were asked: “Have you smoked at least 100 cigarettes in your life?” To assess weight perception and weight control practices, participants were asked: (1) “How do you consider your weight—overweight, underweight, or about the right weight?”, (2) “Would you like to weigh more, less, or stay about the same?”, and (3) “Have you tried to lose weight in the past year?”. To assess diet quality, participants were asked “How healthy is the diet?”,rating from Excellent to Poor. To assess levels of physical activity, participants were asked: “In a typical week, do you do any vigorous‐ or moderate‐intensity sports, fitness, or recreational activities that cause large increases in breathing or heart rate for at least 10 minutes continuously?” Participants were asked to give a list of their prescription medications, and any antihypertensive medication was included as treatment for hypertension.
Calculation of ASCVD Risk Score
Estimated 10‐year ASCVD risk was calculated by using the 2013 American College of Cardiology/American Heart Association sex‐ and race‐specific pooled cohort equations.5 We used the following self‐reported information: age, sex, race/ethnicity, and smoking status, and current antihypertensive drug treatment. Systolic blood pressure was based on an average of 3 or more readings, as measured at the NHANES examination. Total cholesterol, and high‐density lipoprotein cholesterol measurements were available for all examined participants. Participants with an ASCVD score >7.5% were classified as having high ASCVD risk.
Statistical Analysis
Analyses were stratified by race/ethnicity and sex to assess differences in baseline characteristics, as well as healthy lifestyle behaviors. Data are presented as means±SE for continuous variables, and as N (%) for categorical variables. Appropriate 10‐year sample weights were incorporated, which accounted for the complex, multistage, probability sampling design of the NHANES.10 In order to determine predictors of the healthy behaviors of interest, we created dichotomous variables to identify participants who were pursuing weight control if they reported they had tried to lose weight in the past year, who had a healthy diet if they reported “excellent” or “very good” diet quality, and who were participating in any vigorous or moderate‐intensity physical activity. Multivariable logistic regression modeling was used to determine the relationship of race/ethnicity and sex with each healthy behavior variable. Model 1 adjusted for education, income, and marital status, Model 2 adjusted for Model 1+ASCVD risk score, Model 3 adjusted for Model 2+BMI, and Model 4 adjusted for Model 3+self‐perception as overweight. Interaction terms between race and sex were added separately to each model to evaluate whether associations differed by race/ethnicity and sex. To investigate these relationships among those with high cardiovascular disease risks, subgroup analyses were performed in the participants with ASCVD scores >7.5%, and the estimated associations between race/ethnicity and each healthy behavior variable were reported for men and women. We further investigated variable importance for the 8 variables included in Model 4 by measuring each predictor's contribution as the difference in the Akaike Information Criterion value between the full model and the model without that variable (∆Akaike Information Criterion). The relative importance weight for each variable was calculated as the ∆Akaike Information Criterion divided by the sum of ∆Akaike Information Criterion from the candidate models, such that the relative importance weight for each variable can range from 0 to 1 and weights for all 8 variables add up to 1. The relative importance weight can be considered as the relative contribution (importance) of each variable to the model fit, while taking into account the possible intercorrelations among predictors. The higher the relative importance weight is, the more important a variable is to the model fit. To account for the complex sampling design, all analyses were performed using “proc survey” commands in SAS software version 9.4 (SAS Institute Inc, Cary, NC).
Results
The final sample for analysis included 12 351 participants, who represent ≈104.4 million Americans. Of these, 53.0% were female, 77.6% were non‐Hispanic whites, 10.8% were non‐Hispanic blacks, and 11.5% were Hispanics. The sociodemographic and clinical characteristics within each sex and race/ethnic group are shown in Table 1. Compared with non‐Hispanic whites, Hispanics and blacks were younger, less educated, and had lower income. Compared with whites and Hispanics, blacks were more likely to have high blood pressure and be on treatment for hypertension. Blacks and Hispanics were more likely to have diabetes mellitus. Black and Hispanic women were more likely than white women to have been told they were overweight, while white men were more likely than black or Hispanic men to have been told they were overweight. Men had higher 10‐year ASCVD risk scores than women, and blacks had higher 10‐year ASCVD risk scores than whites or Hispanics.
Table 1.
Baseline Characteristics of the Study Sample According to Race/Ethnicity and Sex
| Males (N=5889) | Females (N=6462) | |||||||
|---|---|---|---|---|---|---|---|---|
| White (N=2864) | Hispanic (N=1622) | Black (N=1403) | P Value | White (N=3122) | Hispanic (N=1819) | Black (N=1521) | P Value | |
| Age, y | 54.9±0.2 | 51.7±0.2 | 53.7±0.2 | <0.0001 | 56.0±0.2 | 52.7±0.2 | 54.0±0.3 | <0.0001 |
| Education | <0.0001 | <0.0001 | ||||||
| ≤High school | 1154 (34.9) | 1141 (68.0) | 778 (53.4) | 1252 (34.7) | 1258 (66.0) | 718 (45.1) | ||
| Some college | 816 (29.0) | 302 (20.3) | 386 (28.8) | 989 (31.9) | 372 (22.3) | 506 (34.3) | ||
| ≥College grad | 893 (36.0) | 177 (11.7) | 238 (17.6) | 878 (33.4) | 186 (11.7) | 297 (20.6) | ||
| Income | <0.0001 | <0.0001 | ||||||
| ≤$24 999K | 632 (13.4) | 443 (31.2) | 347 (28.1) | 822 (18.3) | 567 (35.5) | 475 (34.9) | ||
| $25 to 54 999K | 720 (26.4) | 504 (37.6) | 412 (34.5) | 833 (29.6) | 549 (35.4) | 466 (35.4) | ||
| >$55 000K | 1160 (60.2) | 414 (31.1) | 433 (37.4) | 1112 (52.1) | 403 (29.1) | 394 (29.7) | ||
| Never married | 225 (7.2) | 98 (6.8) | 200 (16.4) | <0.0001 | 187 (5.5) | 134 (7.6) | 278 (19.4) | <0.0001 |
| High blood pressurea | 1153 (37.6) | 529 (29.1) | 716 (46.1) | <0.0001 | 1271 (37.9) | 704 (33.8) | 885 (55.2) | <0.0001 |
| High cholesterola | 1258 (48.2) | 606 (47.0) | 526 (41.7) | 0.003 | 1300 (44.3) | 727 (44.2) | 598 (41.5) | 0.3 |
| Diabetes mellitusa | 326 (9.7) | 273 (15.0) | 273 (17.1) | <0.0001 | 291 (7.7) | 337 (16.6) | 301 (17.8) | <0.0001 |
| Overweighta | 1061 (37.0) | 485 (29.5) | 430 (29.9) | <0.0001 | 1310 (40.9) | 826 (45.7) | 773 (50.8) | <0.0001 |
| Smoker | 1685 (54.2) | 936 (55.2) | 811 (54.8) | 0.8 | 1507 (45.5) | 523 (28.7) | 579 (37.6) | <0.0001 |
| BMI, kg/m2 | 29.2±0.1 | 29.2±0.1 | 29.3±0.2 | 0.8 | 28.9±0.2 | 30.4±0.2 | 32.7±0.2 | <0.0001 |
| BMI category | <0.0001 | <0.0001 | ||||||
| Normal weight | 616 (20.4) | 280 (16.5) | 358 (25.1) | 1006 (34.4) | 319 (18.8) | 255 (16.9) | ||
| Overweight | 1174 (42.6) | 750 (46.7) | 479 (35.1) | 877 (28.7) | 626 (34.0) | 394 (26.6) | ||
| Obese | 1035 (37.0) | 576 (36.9) | 539 (39.7) | 1198 (36.9) | 857 (47.2) | 861 (56.5) | ||
| SBP, mm Hg | 124.9±0.4 | 125.5±0.5 | 130.4±0.7 | <0.0001 | 122.8±0.4 | 123.3±0.6 | 128.9±0.5 | <0.0001 |
| DBP, mm Hg | 73.1±0.3 | 73.3±0.4 | 74.4±0.5 | 0.09 | 70.3±0.3 | 69.5±0.4 | 70.9±0.4 | 0.04 |
| Treated hypertension | 961 (30.1) | 381 (19.7) | 599 (36.8) | <0.0001 | 1159 (33.9) | 563 (25.6) | 775 (47.3) | <0.0001 |
| 10‐y ASCVD risk, % | 11.8±0.2 | 10.9±0.3 | 14.2±0.3 | <0.0001 | 7.4±0.2 | 5.9±0.2 | 9.7±0.3 | <0.0001 |
Data are mean+SEM, or N (%). ASCVD indicates atherosclerotic cardiovascular disease; BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure.
Indicates a yes response to the question “Has a doctor ever told you that you have the following condition…?”
Weight Perception and Healthy Lifestyle Behaviors
Black men and white women were most likely to be normal weight by BMI (Table 1). Approximately 80%, 84%, and 75% of white, Hispanic, and black men were overweight or obese by BMI, while 66%, 81%, and 83% of white, Hispanic, and black women were overweight or obese by BMI. Participant responses to perceived weight and healthy lifestyle behaviors are shown in Table 2. White men were more likely than Hispanics or black men to consider themselves overweight, to report a desire to weigh less, and to report having tried to lose weight in the past year. The proportion of women who consider themselves overweight was roughly equivalent by race/ethnicity. However, a slightly higher proportion of white women reported a desire to weigh less, and having tried to lose weight in the past year. White men and women were the most likely to report either excellent or very good diet quality (healthy diet). There were no differences between men in likelihood of engaging in vigorous‐intensity physical activity, but white men were more likely to report engaging in moderate‐intensity physical activity. White women were more likely to report engaging in vigorous‐ or moderate‐intensity physical activity than Hispanic or black women. Even after adjustment for education, income, marital status, and BMI, Hispanic and black men and women were less likely to perceive themselves as overweight or report a desire to weigh less compared with white men and women.
Table 2.
Participant Responses to Questions About Weight Self‐Perception and Healthy Lifestyle Behaviors
| Males (N=5889) | Females (N=6462) | |||||||
|---|---|---|---|---|---|---|---|---|
| White (N=2864) | Hispanic (N=1622) | Black (N=1403) | P Value | White (N=3122) | Hispanic (N=1819) | Black (N=1521) | P Value | |
| Do you consider yourself… | <0.0001 | 0.009 | ||||||
| Overweight | 1639 (59.1) | 765 (48.0) | 612 (45.0) | 2158 (69.5) | 1218 (68.4) | 1054 (70.0) | ||
| Underweight | 123 (3.9) | 56 (3.2) | 104 (7.5) | 95 (2.4) | 61 (3.0) | 63 (4.4) | ||
| About right | 1095 (37.0) | 796 (48.7) | 680 (47.5) | 862 (28.1) | 526 (28.6) | 403 (25.6) | ||
| Would you like to weigh… | <0.0001 | <0.0001 | ||||||
| Less | 1845 (67.3) | 861 (55.3) | 681 (50.2) | 2437 (80.0) | 1304 (72.8) | 1127 (74.9) | ||
| More | 156 (5.3) | 79 (4.8) | 163 (12.7) | 84 (1.9) | 52 (2.7) | 88 (5.8) | ||
| Stay same | 857 (27.4) | 680 (40.0) | 554 (37.1) | 595 (18.1) | 455 (24.5) | 305 (19.3) | ||
| Have tried to lose weight in the past year? | 749 (31.0) | 362 (25.9) | 322 (28.0) | 0.006 | 1223 (48.8) | 686 (44.5) | 566 (45.8) | 0.017 |
| How healthy is your diet? | <0.0001 | <0.0001 | ||||||
| Excellent | 300 (9.4) | 121 (7.5) | 173 (11.6) | 317 (10.2) | 116 (6.1) | 115 (7.0) | ||
| Very good | 723 (24.8) | 247 (14.5) | 281 (18.9) | 885 (29.7) | 274 (14.6) | 266 (17.1) | ||
| Good | 1211 (43.5) | 706 (43.9) | 602 (43.3) | 1268 (40.6) | 746 (40.7) | 673 (43.6) | ||
| Fair | 516 (18.9) | 486 (30.0) | 278 (21.0) | 495 (15.2) | 581 (32.4) | 366 (24.9) | ||
| Poor | 112 (3.4) | 61 (4.0) | 69 (5.3) | 156 (4.3) | 101 (6.2) | 101 (7.4) | ||
| Engage in vigorous‐intensity physical activity | 610 (24.9) | 291 (21.0) | 312 (25.8) | 0.09 | 494 (19.1) | 184 (12.3) | 209 (15.7) | 0.0004 |
| Engage in moderate‐intensity physical activity | 1299 (48.8) | 531 (34.1) | 549 (40.1) | <0.0001 | 1487 (52.2) | 572 (32.9) | 576 (38.5) | <0.0001 |
Association of Weight Perception and Healthy Lifestyle Behaviors With ASCVD Risk Score
Table 3 reexamines the participant responses pertaining to weight perception and healthy lifestyle behaviors according to BMI category and ASCVD risk score. Among overweight and obese participants, white men and women were more likely to consider themselves overweight, to report a desire to weigh less, to report a healthy diet, and to report being physically active. Overweight/obese Hispanic men and women were the least likely to report having tried to lose weight in the past year. Among participants with high ASCVD risk, or those who were overweight/obese in addition to having high ASCVD risk, similar patterns were observed where white men and women were more likely to consider themselves overweight, to report a desire to weigh less, to report a healthy diet, and to report being physically active. However, among participants with high ASCVD risk, or those who were overweight/obese in addition to having high ASCVD risk, there were no differences based on race/ethnicity or sex in the likelihood of reporting having tried to lose weight in the past year.
Table 3.
Participant Responses to Questions About Weight Self‐Perception and Healthy Lifestyle Behaviors in High‐Risk Subgroups
| Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|
| White | Hispanic | Black | P Value | White | Hispanic | Black | P Value | |
| Overweight or obese (N=9366) | ||||||||
| Perception as overweight | 1572 (72.5) | 742 (56.4) | 590 (59.0) | <0.0001 | 1865 (90.8) | 1135 (79.0) | 1008 (81.2) | <0.0001 |
| Desire to weigh less | 1730 (80.3) | 830 (64.5) | 649 (65.5) | <0.0001 | 1935 (94.7) | 1182 (81.5) | 1053 (84.7) | <0.0001 |
| Have tried to lose weight in the past year | 694 (37.5) | 348 (30.7) | 303 (37.8) | 0.003 | 931 (57.9) | 629 (51.1) | 534 (53.2) | 0.0006 |
| Healthy diet | 742 (31.6) | 273 (19.5) | 315 (28.9) | <0.0001 | 681 (33.0) | 283 (17.8) | 281 (21.6) | <0.0001 |
| Physically active | 1148 (56.0) | 526 (41.0) | 490 (50.5) | <0.0001 | 955 (49.8) | 503 (35.7) | 531 (43.7) | <0.0001 |
| ASCVD >7.5% (N=6322) | ||||||||
| Perception as overweight | 1087 (63.4) | 493 (51.6) | 446 (44.5) | <0.0001 | 860 (71.5) | 335 (60.1) | 502 (70.2) | 0.002 |
| Desire to weigh less | 1190 (69.4) | 521 (55.0) | 493 (49.7) | <0.0001 | 939 (78.9) | 355 (62.9) | 520 (72.2) | <0.0001 |
| Have tried to lose weight in the past year | 465 (30.5) | 227 (26.4) | 238 (28.3) | 0.1 | 418 (41.7) | 174 (36.3) | 253 (42.4) | 0.2 |
| Healthy diet | 688 (35.7) | 245 (24.0) | 333 (29.8) | <0.0001 | 508 (43.1) | 117 (19.1) | 186 (24.2) | <0.0001 |
| Physically active | 853 (51.0) | 383 (41.6) | 453 (46.2) | 0.004 | 505 (44.3) | 165 (30.8) | 280 (39.4) | 0.002 |
| Overweight or Obese+ASCVD >7.5% (N=4993) | ||||||||
| Perception as overweight | 1042 (75.1) | 477 (59.9) | 428 (58.1) | <0.0001 | 778 (88.2) | 318 (67.1) | 484 (79.5) | <0.0001 |
| Desire to weigh less | 1128 (81.1) | 505 (63.8) | 468 (64.4) | <0.0001 | 810 (92.2) | 330 (69.2) | 496 (80.9) | <0.0001 |
| Have tried to lose weight in the past year | 431 (35.6) | 218 (31.2) | 224 (38.1) | 0.1 | 350 (48.9) | 167 (41.8) | 246 (49.3) | 0.1 |
| Healthy diet | 520 (33.3) | 187 (21.1) | 233 (28.8) | <0.0001 | 343 (39.2) | 95 (18.2) | 141 (21.7) | <0.0001 |
| Physically active | 686 (51.4) | 320 (40.8) | 342 (48.4) | 0.003 | 341 (40.7) | 140 (30.6) | 234 (39.0) | 0.04 |
ASCVD indicates atherosclerotic cardiovascular disease.
Determinants of Healthy Lifestyle Behaviors
Data from the multivariable regression models are shown in Table 4. Interaction terms between race and sex were significant for each fully adjusted model (data not shown). After adjustment for sociodemographic factors, ASCVD risk score, and BMI, black women were 33% less likely than white women to have attempted weight loss in the past year. Further adjustment for overweight self‐perception attenuated some of the difference in attempted weight loss between black and white women; however, the association remained significant. After adjustment for overweight self‐perception, black men were 31% more likely than white men to have attempted weight loss in the past year. There was no difference between Hispanics and whites in the likelihood of attempted weight loss in the past year. Black women were 18% less likely than white women to have engaged in vigorous or moderate‐intensity physical activity after adjustment for sociodemographic factors and ASCVD risk. However, further adjustment for BMI eliminated the difference in likelihood of engaging in physical activity between black and white women. In fully adjusted models, Hispanic women were 25% less likely than white women to have engaged in vigorous or moderate‐intensity physical activity. There was no difference between men in the likelihood of engaging in physical activity. In fully adjusted models, black and Hispanic women were 39% and 44% less likely, respectively, than white women, and Hispanic men were 29% less likely than white men to report a healthy diet. There was no difference between black and white men in the likelihood of reporting a healthy diet.
Table 4.
Multivariable Logistic Regression for Healthy Lifestyle Practices
| Weight Loss Attempt | Physically Active | Healthy Diet | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | P Value | OR (95% CI) | P Value | OR (95% CI) | P Value | |
| Males | ||||||
| Black | ||||||
| Model 1 | 1.07 (0.88–1.30) | 0.5 | 1.06 (0.86–1.31) | 0.6 | 1.01 (0.87–1.20) | 0.8 |
| Model 2 | 1.07 (0.88–1.30) | 0.5 | 1.08 (0.88–1.33) | 0.5 | 0.99 (0.84–1.17) | 0.9 |
| Model 3 | 1.12 (0.92–1.35) | 0.2 | 1.07 (0.87–1.31) | 0.5 | 0.98 (0.83–1.16) | 0.8 |
| Model 4 | 1.31 (1.08–1.59) | 0.006 | 1.08 (0.88–1.33) | 0.5 | 0.92 (0.77–1.09) | 0.3 |
| Hispanic | ||||||
| Model 1 | 1.03 (0.85–1.23) | 0.8 | 0.96 (0.80–1.15) | 0.7 | 0.69 (0.57–0.83) | 0.0001 |
| Model 2 | 1.02 (0.85–1.22) | 0.8 | 0.91 (0.76–1.09) | 0.3 | 0.72 (0.59–0.87) | 0.0008 |
| Model 3 | 1.07 (0.89–1.30) | 0.4 | 0.92 (0.77–1.10) | 0.4 | 0.73 (0.60–0.88) | 0.001 |
| Model 4 | 1.15 (0.94–1.40) | 0.2 | 0.92 (0.77–1.10) | 0.4 | 0.71 (0.58–0.86) | 0.0004 |
| Females | ||||||
| Black | ||||||
| Model 1 | 0.97 (0.84–1.11) | 0.6 | 0.80 (0.65–0.98) | 0.03 | 0.56 (0.48–0.67) | <0.0001 |
| Model 2 | 0.97 (0.84–1.11) | 0.6 | 0.82 (0.67–1.00) | 0.05 | 0.55 (0.46–0.65) | <0.0001 |
| Model 3 | 0.67 (0.58–0.78) | <0.0001 | 0.93 (0.75–1.14) | 0.5 | 0.66 (0.55–0.79) | <0.0001 |
| Model 4 | 0.79 (0.67–0.93) | 0.0047 | 0.93 (0.75–1.14) | 0.5 | 0.61 (0.51–0.73) | <0.0001 |
| Hispanic | ||||||
| Model 1 | 1.03 (0.89–1.21) | 0.7 | 0.75 (0.60–0.94) | 0.01 | 0.51 (0.43–0.61) | <0.0001 |
| Model 2 | 1.02 (0.87–1.19) | 0.8 | 0.72 (0.57–0.89) | 0.003 | 0.54 (0.45–0.65) | <0.0001 |
| Model 3 | 0.88 (0.74–1.04) | 0.1 | 0.74 (0.60–0.93) | 0.0085 | 0.59 (0.49–0.72) | <0.0001 |
| Model 4 | 0.95 (0.80–1.13) | 0.5 | 0.75 (0.60–0.93) | 0.009 | 0.56 (0.47–0.69) | <0.0001 |
White race is the reference group. Model 1=adjusted for education, income, and marital status (never married). Model 2=model 1+ASCVD risk score. Model 3=model 2+body mass index. Model 4=model 3+self‐perception as overweight. ASCVD indicates atherosclerotic cardiovascular disease; CI, confidence interval; OR, odds ratio.
In the fully adjusted models, ASCVD risk and BMI were significantly associated with weight loss attempts, physical activity, and healthy diet. Participants with high ASCVD risk had a lower odds of attempted weight loss in the past year (odds ratio [OR] 0.78, 95% confidence interval [CI], 0.69–0.88; P<0.0001), a lower odds of engaging in physical activity (OR 0.82, 95% CI, 0.73–0.91; P=0.0002), and a higher odds of reporting a healthy diet (OR 1.45, 95% CI, 1.26–1.67; P<0.0001). Each 1 kg/m2 increase in the BMI was associated with a higher odds of attempted weight loss in the past year (OR 1.11, 95% CI, 1.10–1.13; P<0.0001), a lower odds of engaging in physical activity (OR 0.96, 95% CI, 0.95–0.97: P<0.0001), and a lower odds of reporting a healthy diet (OR 0.93, 95% CI, 0.92–0.94; P<0.0001). Higher education levels and higher income were associated with a higher likelihood for weight loss attempts, physical activity, and healthy diet. Marital status (never married) was associated with a lower likelihood of weight loss attempts in the past year and lower likelihood of healthy diet, but was not associated with physical activity.
Each variable's importance in the full model is illustrated in Figure. Self‐perceived overweight, sex, and BMI were the 3 most important variables that contribute to attempted weight loss among whites and Hispanics, while self‐perceived overweight, BMI, and education were the 3 most important variables among blacks. Education and BMI are the 2 most important variables that contribute to being physically active among all race/ethnicities. Education, BMI, and self‐perceived overweight are the 3 most important variables for reporting a healthy diet among blacks and Hispanics, while education, BMI, and ASCVD score were the 3 most important variables among whites. Notably, ASCVD score is shown to be the third and fourth contributor for physical activity and diet among whites and Hispanics, but ranked fifth in importance among blacks.
Figure 1.
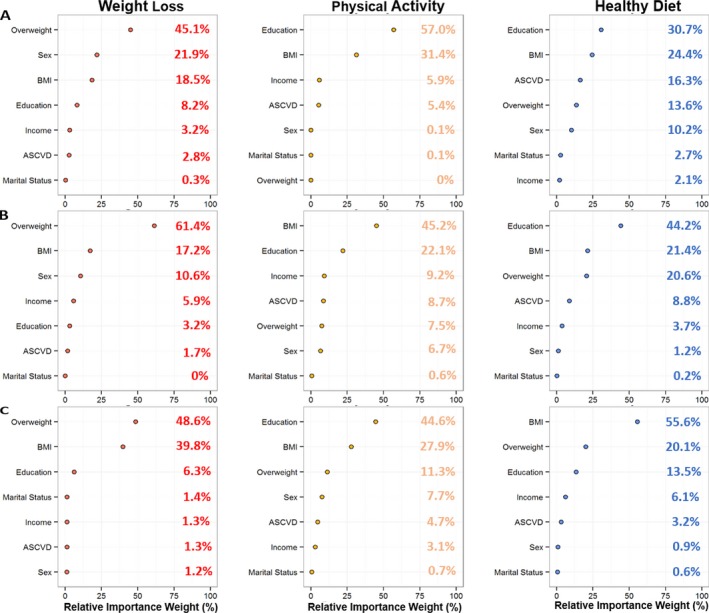
The relative importance of variables included in the full model is shown in whites (A), Hispanics (B), and blacks (C). Importance is measured as the difference in the Akaike Information Criterion value between the full model and the model without that specific variable, scaled to provide a weight for each variable that ranges from 0 to 1. ASCVD indicates atherosclerotic cardiovascular disease; BMI, body mass index.
We performed a sensitivity analysis to determine whether the associations between race/ethnicity and healthy behaviors were similar in participants with high ASCVD risk. In men with high ASCVD risk, blacks and Hispanics were 47% (OR 1.47, 95% CI, 1.15–1.89; P=0.002) and 26% (OR 1.26, 95% CI, 1.00–1.60; P<0.05) more likely than whites to report attempted weight loss. Hispanic men were 35% (OR 0.65, 95% CI, 0.50–0.86; P=0.002) less likely than white men to report healthy diet. In women with high ASCVD risk, blacks and Hispanics were 51% (OR 0.49, 95% CI, 0.38–0.63; P<0.0001) and 61% (OR 0.39, 95% CI, 0.30–0.52; P<0.0001) less likely than white women to report healthy diet. There were no differences by race/ethnicity in women in the likelihood of attempted weight loss. There were no differences by race/ethnicity in men or women in the likelihood of physical activity.
Discussion
In this cross‐sectional analysis of a nationally representative sample, we found important differences in the likelihood of engaging in healthy lifestyle behaviors according to race/ethnicity and sex. Despite higher BMI and higher ASCVD risk scores, black women are less likely than white women to have attempted weight loss, or to report a healthy diet. Despite higher BMI, Hispanic women are less likely than white women to engage in physical activity, or to report a healthy diet. Moreover, in women with ASCVD risk >7.5%, there were even greater disparities in the likelihood of healthy diet between blacks and Hispanics compared with whites. Hispanic men are less likely than white men to report a healthy diet. Although the relative importance weights differed somewhat according to race/ethnicity, self‐perception of overweight, measured BMI, and education are important variables in predicting likelihood of engaging in healthy lifestyle behaviors. These data suggest that awareness of one's excess body weight may be a stronger motivator for healthy lifestyle behaviors than measured cardiovascular risk.
Our findings must be interpreted with caution, since we have no information on whether subjects were counseled specifically on their 10‐year risk of ASCVD using available risk scores. However, any history of cardiovascular risk factors was defined by subjects being told so by a doctor or other health professional. So although we cannot definitively conclude that healthy behaviors were poorer in Hispanics and black women despite a higher “unknown” calculated risk score, our findings highlight that patients’ motivation for healthy behaviors may be based more on measured weight and self‐perception as overweight or obese. Indeed, prior studies in women have shown that increased knowledge and awareness of CVD risk factors does not necessarily translate into healthier lifestyle behaviors.11, 12 Thus, in the setting of a growing obesity epidemic, it is crucial that health professionals continue to educate patients about heathy BMI and body image to motivate engagement in healthy lifestyle behaviors.
Multiple prior studies have demonstrated that desired weight and weight self‐perceptions vary by race/ethnicity and sex. These differences are likely related to important cultural differences in body image ideals and comparisons within an individual's social circles. For instance, Maynard et al found that Hispanic men have a lower desired body weight as compared with white and black men, while black women have a much higher desired body weight than white or Hispanic women.13 Langellier et al used data from 37 050 adult NHANES participants to examine race/ethnic differences in weight self‐perceptions and how those differences have changed over time in the setting of the obesity epidemic.14 Despite significant increases in mean BMI and prevalence of overweight and obesity, blacks became even less likely to perceive themselves as overweight compared with whites in the setting of the obesity epidemic, resulting in worsening disparities in weight self‐perception over time. There were smaller differences in overweight self‐perceptions between US‐born Mexican American men and women compared with whites. These findings are similar to ours, in that both black and Hispanic men and women were less likely to perceive themselves as overweight or report a desire to weigh less compared with white men and women. Compared with Langellier et al, we may have found larger differences in weight self‐perception between Hispanics and whites because we limited our sample to older adults, and prior studies15 have documented that overweight self‐perception is age dependent.
Prior studies have also demonstrated conflicting results on whether awareness of one's cardiovascular risk profile influences healthy lifestyle behaviors. Ramirez et al examined how CVD risk factors influenced individuals’ perceived need to improve their health and adopt healthy lifestyle behaviors in 45 443 Canadian residents.16 Smoking, obesity, and low physical activity were most strongly associated with perceived need to improve health behaviors, while hypertension and diabetes mellitus had no association. Importantly, ≈20% of those at highest cardiac risk did not have a perceived need to improve their lifestyle. Similarly, Vähäsarja et al found that physical inactivity and obesity were associated with perceived need to change health behavior in 10 149 Finnish men and women, but that smoking, hypertension, and dyslipidemia were not associated with a need to change.17 Koniak‐Griffin et al randomized Hispanic women (N=90) to an intervention designed to improve knowledge of risk factors for CVD and skills to improve healthy lifestyle behaviors.12 Despite a significant improvement in heart disease knowledge after the intervention, there was no significant association between knowledge scores and overall dietary habits, BMI, or physical activity. In our study, CVD risk factors as measured by a higher ASCVD risk predicted a lower odds of attempted weight loss and physical activity, but a higher odds of healthy diet. Although these associations did not appear to differ by race/ethnicity, there was an even lower likelihood for black women and Hispanics to report healthy diet. It is unclear whether subjects with more cardiovascular risk factors perceive themselves as being unable to exercise because of physical or functional limitations. However, since physical activity is recommended in older adults and those with chronic medical conditions,18 it is important to continue to counsel patients on the importance of physical activity and other maneuvers to control excess weight.
Similar to our findings, multiple other analyses have confirmed lower prevalence of physical activity and healthy diet among race/ethnic minorities.19, 20 In addition to differences in weight perception, other barriers may be present that negatively impact these and other healthy lifestyle practices in minority groups. Powell et al documented that commercial physical activity–related facilities were less likely to be present in lower‐income neighborhoods and in neighborhoods with higher proportions of blacks, Hispanics, and other race/ethnic minorities.21 Morland et al confirmed that low‐income and predominantly black neighborhoods have fewer supermarkets or specialty food stores than high‐income or predominantly white neighborhoods.22 Interestingly, we found that black men were more likely than white men to have engaged in weight loss attempts. Likewise, Gavin et al found that among adults with diabetes mellitus, black and Hispanic men were more likely than white men to report physical activity.23
There are some important limitations to our findings that are worth noting. The Pooled Cohort risk equation was validated in a cohort primarily composed of blacks and whites. Since the estimated 10‐year risk of ASCVD is generally lower in Hispanics,1 use of the risk equation may overestimate risk for this population.5 Still, we felt it was important to include Hispanics in our analysis since this group is at such high risk of obesity and unhealthy lifestyle behaviors. Although we used the ASCVD risk score as an aggregate estimate of cardiovascular risk, NHANES participants were not counseled on their cardiovascular risk per se. Thus, it is impossible to infer that knowledge of their ASCVD risk score has anything to do with their likelihood of engaging in healthier behaviors. However, participants were aware of their individual risk factors as told to them by a healthcare professional. Finally, all questionnaire data are based on self‐report and are subject to recall bias. Dietary assessment is particularly error prone, and prior studies have identified important race and sex differences in dietary recall,24 suggesting that even well‐validated dietary questionnaires may have limited accuracy to assess nutrient intake among minority women. Similarly, smoking history was assessed based on participants reporting having smoked at least 100 cigarettes in their life. However, this definition would miss “causal smokers” who had smoked <100 cigarettes in their life.
In summary, we confirmed important differences in the likelihood of engaging in healthy lifestyle behaviors in race/ethnic minorities despite a higher burden of CVD risk factors. These differences were more pronounced in women than in men, and the associations between race/ethnicity and healthy lifestyle behaviors were influenced more strongly by BMI and weight perception than by ASCVD risk. Given that healthy lifestyle behaviors are associated with lower CVD risk, it is crucial to provide culturally sensitive recommendations, particularly in high‐risk populations, in order to continue to improve CVD risk.
Sources of Funding
Morris is supported by funding from the National Institutes of Health/National Heart, Lung, and Blood Institute (K23 HL124287) and the Robert Wood Johnson Foundation (Harold Amos Medical Faculty Development Program).
Disclosures
None.
(J Am Heart Assoc. 2018;7:e008250 DOI: 10.1161/JAHA.117.008250.)29728015
A portion of the results of this work were presented as an oral abstract at the American Heart Association Scientific Sessions, November 11 to 15, 2017, in Anaheim, CA.
References
- 1. Benjamin EJ, Blaha MJ, Chiuve SE, Cushman M, Das SR, Deo R, de Ferranti SD, Floyd J, Fornage M, Gillespie C, Isasi CR, Jiménez MC, Jordan LC, Judd SE, Lackland D, Lichtman JH, Lisabeth L, Liu S, Longenecker CT, Mackey RH, Matsushita K, Mozaffarian D, Mussolino ME, Nasir K, Neumar RW, Palaniappan L, Pandey DK, Thiagarajan RR, Reeves MJ, Ritchey M, Rodriguez CJ, Roth GA, Rosamond WD, Sasson C, Towfighi A, Tsao CW, Turner MB, Virani SS, Voeks JH, Willey JZ, Wilkins JT, Wu JH, Alger HM, Wong SS, Muntner P; American Heart Association Statistics Committee and Stroke Statistics Subcommittee . Heart disease and stroke statistics—2017 update: a report from the American Heart Association. Circulation. 2017;135:e146–e603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ogden C, Carroll M, Fryar C, Flegal K. Prevalence of Obesity Among Adults And Youth: United States, 2011–2014. NCHS Data Brief, No 219. Hyattsville, MD: National Center for Health Statistics; 2015. [PubMed] [Google Scholar]
- 3. Pool LR, Ning H, Lloyd‐Jones DM, Allen NB. Trends in racial/ethnic disparities in cardiovascular health among US adults from 1999–2012. J Am Heart Assoc. 2017;6:e006027 DOI: 10.1161/JAHA.117.006027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, Kottke TE, Giles WH, Capewell S. Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med. 2007;356:2388–2398. [DOI] [PubMed] [Google Scholar]
- 5. Goff DC, Lloyd‐Jones DM, Bennett G, Coady S, D'Agostino RB, Gibbons R, Greenland P, Lackland DT, Levy D, O'Donnell CJ, Robinson JG, Schwartz JS, Shero ST, Smith SC Jr, Sorlie P, Stone NJ, Wilson PW, Jordan HS, Nevo L, Wnek J, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Curtis LH, DeMets D, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Smith SC Jr, Tomaselli GF; American College of Cardiology/American Heart Association Task Force on Practice Guidelines . 2013 ACC/AHA guideline on the assessment of cardiovascular risk. Circulation. 2014;129:S49. [DOI] [PubMed] [Google Scholar]
- 6. Wormser D, Kaptoge S, Di Angelantonio E, Wood AM, Pennells L, Thompson A, Sarwar N, Kizer JR, Lawlor DA, Nordestgaard BG, Ridker P, Salomaa V, Stevens J, Woodward M, Sattar N, Collins R, Thompson SG, Whitlock G, Danesh J. Separate and combined associations of body‐mass index and abdominal adiposity with cardiovascular disease: collaborative analysis of 58 prospective studies. Lancet. 2011;377:1085–1095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Pencina MJ, Agostino RB, Larson MG, Massaro JM, Vasan RS. Predicting the 30‐year risk of cardiovascular disease. Circulation. 2009;119:3078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Centers for Disease Control and Prevention. National Health and Examination Nutrition Survey . Continuous NHANES Data, Questionnaires and Related Documentation. Available at: https://wwwn.cdc.gov/nchs/nhanes/Default.aspx. Accessed April 9, 2018.
- 9. Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey . 2013. Available at: https://www.cdc.gov/nchs/tutorials/NHANES/SurveyDesign/SampleDesign/Info1.htm Accessed May 30, 2017.
- 10. Centers for Disease Control and Prevention . Continuous NHANES Web tutorials. Specifying weight parameters. 2013. Available at: https://www.cdc.gov/nchs/tutorials/nhanes/SurveyDesign/Weighting/intro.htm. Accessed May 25, 2017.
- 11. Konicki AJ. Knowledge of cardiovascular risk factors, self‐nurturance, and heart‐healthy behaviors in women. J Cardiovasc Nurs. 2012;27:51–60. [DOI] [PubMed] [Google Scholar]
- 12. Koniak‐Griffin D, Brecht M‐L. Awareness of cardiovascular disease and preventive behaviors among overweight immigrant Latinas. J Cardiovasc Nurs. 2015;30:447–455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Maynard LM, Serdula MK, Galuska DA, Gillespie C, Mokdad AH. Secular trends in desired weight of adults. Int J Obes. 2006;30:1375–1381. [DOI] [PubMed] [Google Scholar]
- 14. Langellier BA, Glik D, Ortega AN, Prelip ML. Trends in racial/ethnic disparities in overweight self‐perception among U.S. adults, 1988–1994 and 1999–2008. Public Health Nutr. 2015;18:2115–2125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Chang VW, Christakis NA. Self‐perception of weight appropriateness in the United States. Am J Prev Med. 2003;24:332–339. [DOI] [PubMed] [Google Scholar]
- 16. Ramirez FD, Chen Y, Di Santo P, Simard T, Motazedian P, Hibbert B. Association between self‐reported potentially modifiable cardiac risk factors and perceived need to improve physical health: a population‐based study. J Am Heart Assoc. 2017;6:e005491 DOI: 10.1161/JAHA.117.005491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Vähäsarja K, Salmela S, Villberg J, Rintala P, Vanhala M, Saaristo T, Peltonen M, Keinänen‐Kiukaanniemi S, Korpi‐Hyövälti E, Kujala UM, Moilanen L, Niskanen L, Oksa H, Poskiparta M. Perceived need to increase physical activity levels among adults at high risk of type 2 diabetes. A cross‐sectional analysis within a community‐based diabetes prevention project FIN‐D2D. BMC Public Health. 2012;12:514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. U.S. Department of Health and Human Services . 2008 physical activity guidelines for Americans. Available at: https://health.gov/paguidelines/pdf/paguide.pdf. Accessed June 9, 2017.
- 19. Hiza HAB, Casavale KO, Guenther PM, Davis CA. Diet quality of Americans differs by age, sex, race/ethnicity, income, and education level. J Acad Nutr Diet. 2013;113:297–306. [DOI] [PubMed] [Google Scholar]
- 20. August KJ, Sorkin DH. Racial/ethnic disparities in exercise and dietary behaviors of middle‐aged and older adults. J Gen Intern Med. 2011;26:245–250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Powell LM, Slater S, Chaloupka FJ, Harper D. Availability of physical activity‐related facilities and neighborhood demographic and socioeconomic characteristics: a national study. Am J Public Health. 2006;96:1676–1680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Morland K, Wing S, Diez Roux A, Poole C. Neighborhood characteristics associated with the location of food stores and food service places. Am J Prev Med. 2002;22:23–29. [DOI] [PubMed] [Google Scholar]
- 23. Gavin JR, Fox KM, Grandy S. Race/Ethnicity and gender differences in health intentions and behaviors regarding exercise and diet for adults with type 2 diabetes: a cross‐sectional analysis. BMC Public Health. 2011;11:533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Olendzki B, Procter‐Gray E, Magee MF, Youssef G, Kane K, Churchill L, Ockene J, Li W. Racial differences in misclassification of healthy eating based on food frequency questionnaire and 24‐hour dietary recalls. J Nutr Health Aging. 2017;21:787–798. [DOI] [PMC free article] [PubMed] [Google Scholar]