

Abstract
Introduction:
Foam roller is a device used as a massage intervention for rehabilitation and fitness performance.
Objective:
To examine the effects on the ankle dorsiflexion mobility of the foam roller as well as the combination of foam roller and vibration applied to the ankle plantarflexors muscles, and to observe the possible cross-effect.
Methods:
Thirty-eight undergraduate students participated in the study (19 males and 19 females). This study investigated. Three conditions (3 sets of 20 s) were performed in a randomized order (independent variables): 1) foam roller (Roller), 2) foam roller and vibration (Roller+VIB), and 3) no foam roller or vibration (Control). to determine whether of foam roller with or without vibration would benefit ankle dorsiflexion mobility. Ankle dorsiflexion ROM and plantar flexor were measured in both legs before and immediately after the treatment.
Results:
A cross-effect was found in the non-stimulated leg. There was a significant effect on ankle mobility of Roller and Roller+VIB conditions (6% and 7%, p<0.001).
Conclusion:
Foam roller massage and vibration stimulus’ foam roller massage increase ankle mobility producing a cross-effect.
Keywords: Massage, Self-Miofascial Release Mobility, Strength
Introduction
Foam rolling is a popular technique used as a self-massage intervention. The principal use of this type of self-massage release is for rehabilitation and fitness performance to enhance myofascial mobility. Previous evidence has reported foam rolling can increase joint range of motion (ROM)[1] and improve the recovery process[2]. Regular, intense or unaccustomed exercise can evoke a possible pain effect on muscle, where foam rolling has been shown to reduce delayed onset muscle soreness (DOMS)[3] and decrease perceived fatigue[4]. Currently, there are two commercial foam rollers that have been used in previous research, such as the standard model (15.24 cm x 91.44 cm)[2-8] and half size model (15.24 cm x 45.72 cm)[9] where body weight of the individual is used to apply pressure to soft tissues during the rolling motion[10].
Foam rolling is an effective intervention for enhancing joint range of movement in pre- and post-exercise muscle performance10 but currently there is no defined program of foam roller massage due to the heterogeneity of methods reported in previous studies[10]. To increase ROM various methods of stretching are often employed, such as, static, ballistic, and dynamic stretching as along with proprioceptive neuromuscular facilitation[11]. Static stretching is commonly utilized, however when it is implemented as part of warm up, muscular power and performance decreases[12]. If the myofascia is injured, inactive, or inflamed it can restrict ROM and decrease strength and endurance[1]. Currently there is a plethora of practitioner-partnered techniques to treat fascia such as, osteopathic soft-tissue manipulations, structural integration, massage, muscle energy techniques, and Graston[13]. However, an alternative technique that is independent of a practitioner, is self-induced myofascial release, which can be facilitated with a foam roller or roller massager[11]. In several studies foam rolling has demonstrated an increase in ROM measure[8,13-14].
Another training method that has been popular over the last decade is vibration therapy. The vibration stimulus can be applied directly to the muscle or tendon or indirectly to the whole body where the stimuli enters via the feet while standing on a vibration platform[15]. The use of direct vibration therapy as a recovery modality to reducing muscle soreness and fatigue is gaining a lot of interest. For instance, applying direct vibration therapy to elbow flexors following strenuous eccentric exercise has been shown to attenuate muscle soreness and improve ROM[16]. However, little is known about the efficacy of combining foam roller with vibration to enhance ROM improvements. In most instances unilateral foam rolling occurs, however there is paucity of information whether unilateral exposure to foam rolling can improve performance of the other leg. Previous studies have observed strength changes in the non-trained limb[17] of knee extensors[18-20] and elbow flexors[21,22]. Likewise, Shima et al.[23] found that after 6 weeks training of single leg calf raises and plantar flexion a cross-effect was apparent in ankle plantarflexors of the contralateral leg.
Currently, there is a lack of knowledge about the use of concurrent vibration and roller and its efficacy to elicit a cross-effect on the contralateral leg to improve ROM. Therefore, the main purpose of this study was to examine the effects on the ankle dorsiflexion mobility of the foam roller as well as the combination of foam roller and vibration applied to the ankle plantarflexors muscles, and to observe the possible cross-effect. We hypothesized that vibration combined with foam roller would induce an increase in ankle dorsiflexion mobility for the leg that receives the stimulus and the contralateral limb.
Materials and methods
Experimental design
This study investigated whether 3 sets of 20 s of foam roller with or without vibration would benefit ankle dorsiflexion mobility. Ankle dorsiflexion ROM and plantar flexor were measured in both legs before and immediately after the treatment. Three conditions were performed in a randomized order (independent variables): 1) foam roller (Roller), 2) foam roller and vibration (Roller+VIB), and 3) no foam roller or vibration (Control). All treatment conditions were applied to the dominant leg and were separated by at least 48 hours and were conducted at the same time of day to take into account for daily biorhythms. The preference for kicking a ball was the criteria to determine participant’s dominant leg.
Participants
Thirty-eight undergraduate students participated in the study, 19 females (19.5±7.2 y, 167.8±0.1 cm, 59.2±2.2 kg) and 19 males (21.8±2.7 y, 178.9±0.1 cm, 73.7±9.1 kg). One female and 5 males indicated left leg dominance. Each participant performed all 3 conditions to minimize inter-individual variance in muscle response. All participants were recreationally active but none were involved in a systematic exercise-training program at the time of data collection or for at least 2 months prior to the study. Prior to data collection participants were informed of the requirements associated with participation and provided written informed consent. Exclusion criteria were diabetes, epilepsy, gallstones, kidney stones, cardiovascular diseases, joint implants, recent thrombosis, as well as musculoskeletal problems. Participants were encouraged to maintain their dietary, sleeping, and drinking habits during the study. Two to three days before the testing sessions, participants attended one familiarization session. The study was conducted according to the Declaration of Helsinki and was approved by the University Review Board for use of Human Subjects.
Foam rolling and vibration
A commercial foam roller (Vyper®, Hyperice, Irvine, USA) with three different vibration frequencies that produced uniform oscillations was used in the current study. The roller was set at the medium setting with the following parameters; a frequency of 49 Hz with and an amplitude of 1.95 mm (distance from peak-to-peak). Using a three-axial accelerometer (Vibration Datalogger DT-178A, Ruby Electronics, Saratoga, USA) with 60 kg on foam roller it generated an acceleration of 92.6 m·s-2. This was obtained via the vector sum of the accelerations and data analysis was performed using specific software (Vibration Datalogger DT-178A, Ruby Electronics, Saratoga, USA). During all the conditions, participants did not wear any clothing on the calf or socks.
Ankle ROM test
The ROM of ankle dorsiflexion was assessed using Leg Motion system (Check your MOtion®, Albacete, Spain), which is a portable tool used to measure ankle dorsiflexion during a weight-bearing lunge[24]. Participants were tested before (Pre) and after (Post) for each condition (Figure 1). All assessments were conducted by the same researcher according to the reliability protocol established by Ortega and colleagues[25]. The leg motion ankle dorsiflexion test was preceded by two warm-up attempts with the third attempt recorded. Each participant started with their hands on their hips, where the assigned foot was located on the middle of the longitudinal line just behind the transversal line on the platform. The contralateral foot was positioned to the side of the platform. While maintaining this position, participants were instructed to perform a lunge where the knee was flexed with the goal of making contact between the anterior knee and the perpendicular metal stick. When participants were able to maintain heel and knee contact, the metal stick was progressed away from knee. The distance achieved was recorded in centimeters. Three trials were performed for each ankle (dominant and non-dominant) with 10 seconds of passive recovery between trials. The third value from each ankle was selected for subsequent analysis of weight-bearing dorsiflexion ROM (DF ROM)[26].
Figure 1.

Ankle ROM test.
Maximal voluntary isometric contraction
A custom-made ankle strength device was used to measure maximal voluntary isometric contraction (MVIC) plantarflexion (PF) and dorsiflexion (DF) force. Participants were seated on a chair, with their trunk, thighs, lower thighs, and foot fastened to the chair and the force meter device. The DF and PF were calculated as the tensile and compressive force of a strain gauge (Winlaborat V4.20, Buenos Aires, Argentina).
Participants then performed three trials at maximal effort of 4 seconds with a 1-min rest period between trials to minimize muscle fatigue. The average of three measures was calculated. DF ROM, PF, and DF were re-measured on a different day to determine the test-retest repeatability of such measurements, by calculating intraclass correlation coefficient (ICC).
Treatment protocol
Participants began all experimental sessions with a warm-up consisting of 10 bilateral heel rises at a duration of one second to rise the heels and 1 second to for the heels to make contact with the ground. Each participant performed three separate conditions in a randomized order in barefoot. 1) Roller (roller only), 2) Roller+Vibration (roller and vibration at 32 Hz), 3) Control (sitting on a chair). The Roller consisted of 3 sets of 20 seconds in duration with a 10-second rest between sets[27]. Thus, the volume of work performed in the Sham condition was equalized. Foam rolling was performed in a seated position with the legs extended and the foot relaxed as shown in [Figure 2]. Participants were instructed to use their arms to propel their body back and forward, from popliteal fossa to Achilles tendon, in a smooth and continuous motion of 3 seconds forward and 1 second backward and then vice versa from Achilles tendon to popliteal fossa. The first set was performed on the lateral side of the triceps sural, the second set on the center and the third set on the medial side of the triceps sural. They were also instructed to exert as much pressure on the dominant leg, whilst the contralateral leg was placed on a body-mass scale to avoid exerting additional pressure. The measures of DF ROM, PF, and DF were made before and immediately (less than 10s between condition and measure) after the treatment in both legs in a randomized order.
Figure 2.

Foam rolling technique.
Statistical analysis
Data were analyzed using PASW/SPSS Statistics 20 (SPSS Inc, Chicago, IL) and significance level was set at P≤0.05. All the measures were normally distributed, as determined by the Kolmogorov-Smirnov test. Sphericity was tested by the Greenhouse-Geisser method.
Dependent variables (DF ROM, PF, and DF) were evaluated with a two-way repeated measures analysis of variance (ANOVA) of condition x time. Where significant F values were achieved, pairwise comparisons were performed using the Bonferroni post hoc procedure. Effect size statistic, η[2], was analyzed to determine the magnitude of the effect independent of sample size. Values are presented as mean ± standard deviation (SD).
Results
The ICCs of DF ROM, PF, and DF were 0.98, 0.87 and 0.89, respectively.
Ankle ROM
Ankle dorsiflexion ROM was higher in Roller and Roller+VIB compared to Control for both legs (p<0.001; η[2]=0.394). After Roller condition, dominant leg and non-dominant leg reported a 6% of improvement of ankle dosrsiflexion ROM, while for Roller+VIB condition dominant leg increase 7% and non-dominant leg 5% (Figure 3a and 3b). A significant time effect (p<0.001; η[2]=0.762) was observed in all conditions, and a leg effect was found (p<0.05; η[2]=0.099) (Figure 3a and 3b).
Figure 3.
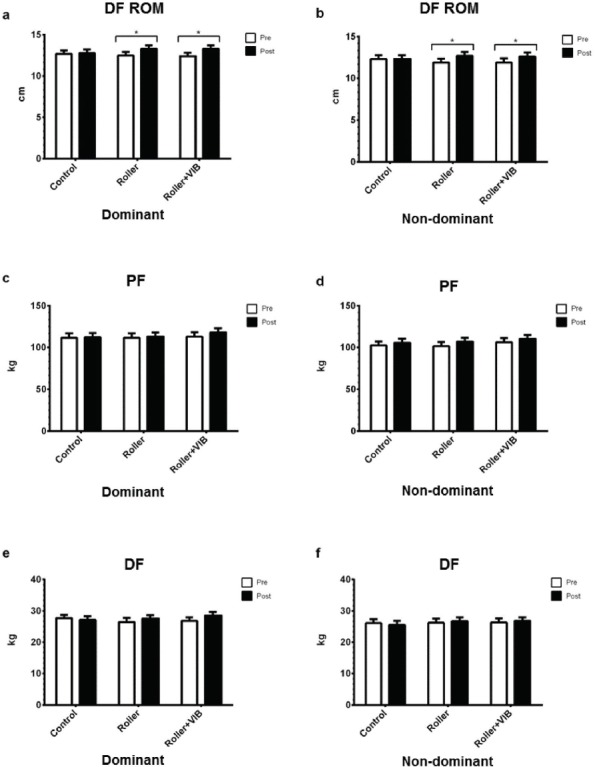
a & b - DF ROM of dominant and non-dominat limb; c & d - PF of dominant and non-dominat limb; e & f - DF of dominant and non-dominat limb of control, roller and roller + vib conditions. DF ROM = dorsiflexion range of motion; PF = plantarflexion force; DF = dorsiflexion force.
Maximal voluntary isometric contraction
There was no significant difference in the PF (Figure 3c and 3d) or DF (Figure 3e and 3f) between conditions (p>0.05).
Discussion
The main finding of the present study was foam roller or foam roller and vibration stimulus of the dominant calf muscle elicited an increase in ankle dorsiflexion ROM in the treated and contralateral limb. In contrast, MVIC was not affected by foam roller. To the best of our knowledge, this is the first study to assess the effects of foam rolling with foam roller combined with vibration, as well as the first study to observe the effects of this treatment on the contralateral limb. Moreover, previous studies have reported that foam rolling can have a positive influence on ankle dorsiflexion ROM and it is capable of eliciting cross-over effect on the contralateral limb[9,27].
Pellegrini et al.[28] investigated the acute effect of whole body vibration (WBV, 26 Hz, 4-4.5 mm amplitude) on the voluntary activation of the ankle plantar flexors in healthy young adults and reported that after 5 sets of 1 minute of stretching of the plantar flexors with WBV that plantar flexor force increased. In contrast, the present study found no significant increase in plantarflexor MVIC. Our current results used a higher frequency vibration stimulus (49 Hz) compared to a lower frequency in previous work (26 Hz). Our work also used a different vibration device, a vibration roller versus a vibration platform. However, the methodology may explain the dissonance, in the current study we analyzed isometric muscle action but Pellegrini et al.[28] study used an isokinetic exercise protocol. Furthermore, Harwood et al.[29] revealed that isometric plantar flexor performance decreased immediately following five 60-seconds bouts of WBV (45 Hz, 2 mm amplitude) and as a result of consecutive acute bouts of vibration the authors suggested the Ia pathway was compromised.
In support of the current findings a recent study analyzed the effects of foam rolling on muscle recovery after exercise-induced muscle damage (EIMD), and concluded that foam rolling had no effect on plantar flexor performance, morphology, and oxygenation recovery after EIMD, except for muscle pain pressure threshold[30]. Furthermore, the present findings indicate the Roller increased ankle dosrsiflexion ROM of dominant and non-dominant leg by 6%, while Roller+VIB increased ROM in the dominant leg (7%) and non-dominant (5%). This is similar to 4-10% ROM improvement reported by previous studies of the hamstrings1 and ankle dorsiflexion[31].
However, the additive effect of vibration with foam rolling did not significantly improve ROM compared to foam rolling alone. Additionally, it did not enhance plantarflexion and dorsiflexion isometric strength. Although the foam roller was acting directly on the triceps sural, it is possible that the current rolling duration of 3 seconds forward and 1 sec backward for 20 seconds may have not been substantial for the vibration stimulus to elicit the appropriate responses to enhance muscle performance. Therefore, a higher vibration frequency and amplitude, along with a slower rolling duration may be required to ensure that the additive component of vibration can be realized. Moreover, it is plausible that the force applied during foam rolling may have nullified the additive effect of vibration. Further research is required to determine if an optimal force is required on the muscle group when vibration is combined with foam rolling.
Despite the ROM increase being similar in both conditions (Roller and Roller+VIB) it is difficult to ascertain the mechanism(s) for its improvement, as there may be various aspects that are involved. Without direct evidence it is difficult to substantiate, however one may speculate that changes occurred in the viscoelastic elements of the musculotendinous unit[32,33] and that stretching tolerance of ROM improved[34].
The concept of cross-over effect has been well documented in unilateral resistance training where neural adaptations are the likely mechanism[35] to eliciting changes on contralateral strength[17]. The findings of the present study indicate that ROM was enhanced in the affected and the contralateral limb. This is supported by Jay et al.[36] who reported that following exercise induced DOMS, acute muscle soreness was reduced and pain threshold was increased from 10 minutes from foam rolling the hamstrings of the ipsilateral limb; additionally, there was a tendency of reduced muscle soreness in the contralateral limb. The authors postulate that central pathways may be a potential source to eliciting the cross-over transfer. In contrast, the current results showed that combining vibration with foam rolling had little effect on ROM, therefore it is likely that the participant’s force applied to the roller of the ipsilateral limb may have caused a global response of stimulating the mechanoreceptors, which supports the idea of a cross-over effect of the contralateral limb[27].
In conclusion, the present study documents for the first time that foam rolling combined with vibration increases dorsiflexion ROM and a cross-over transfer effect was observed in the contralateral limb. However, the addition of the vibration stimulus with foam rolling did not further increase ROM compared to foam rolling alone. Thus, there seems little benefit of including vibration with foam rolling to increase ROM, however further research is required to determine its prophylactic or therapeutic recovery ability to deter muscle fatigue and accelerate muscle performance.
Footnotes
The authors have no conflict of interest.
Edited by: F. Rauch
References
- 1.Sullivan KM, Silvey DB, Button DC, Behm DG. Roller-massager application to the hamstrings increases sit-and-reach range of motion within five to ten seconds without performance impairments. Int J Sports Phys Ther. 2013;8(3):228–36. [PMC free article] [PubMed] [Google Scholar]
- 2.Macdonald GZ, Button DC, Drinkwater EJ, Behm DG. Foam rolling as a recovery tool after an intense bout of physical activity. Med Sci Sports Exerc. 2014;46(1):131–42. doi: 10.1249/MSS.0b013e3182a123db. [DOI] [PubMed] [Google Scholar]
- 3.Pearcey GE, Bradbury-Squires DJ, Kawamoto JE, Drinkwater EJ, Behm DG, Button DC. Foam rolling for delayed-onset muscle soreness and recovery of dynamic performance measures. J Athl Train. 2015;50(1):5–13. doi: 10.4085/1062-6050-50.1.01. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Healey KC, Hatfield DL, Blanpied P, Dorfman LR, Riebe D. The effects of myofascial release with foam rolling on performance. J Strength Cond Res. 2014;28(1):61–8. doi: 10.1519/JSC.0b013e3182956569. [DOI] [PubMed] [Google Scholar]
- 5.Bushell JE, Dawson SM, Webster MM. Clinical Relevance of Foam Rolling on Hip Extension Angle in a Functional Lunge Position. J Strength Cond Res. 2015;29(9):2397–403. doi: 10.1519/JSC.0000000000000888. [DOI] [PubMed] [Google Scholar]
- 6.Curran PF, Fiore RD, Crisco JJ. A comparison of the pressure exerted on soft tissue by 2 myofascial rollers. J Sport Rehabil. 2008;17(4):432–42. doi: 10.1123/jsr.17.4.432. [DOI] [PubMed] [Google Scholar]
- 7.MacDonald GZ, Penney MD, Mullaley ME, Cuconato AL, Drake CD, Behm DG, Button DC. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J Strength Cond Res. 2013;27(3):812–21. doi: 10.1519/JSC.0b013e31825c2bc1. [DOI] [PubMed] [Google Scholar]
- 8.Mohr AR, Long BC, Goad CL. Effect of foam rolling and static stretching on passive hip-flexion range of motion. J Sport Rehabil. 2014;23(4):296–9. doi: 10.1123/jsr.2013-0025. [DOI] [PubMed] [Google Scholar]
- 9.Skarabot J, Beardsley C, Stirn I. Comparing the effects of self-myofascial release with static stretching on ankle range-of-motion in adolescent athletes. Int J Sports Phys Ther. 2015;10(2):203–12. [PMC free article] [PubMed] [Google Scholar]
- 10.Cheatham SW, Kolber MJ, Cain M, Lee M. The Effects of Self-Myofascial Release Using a Foam Roll or Roller Massager on Joint Range of Motion, Muscle Recovery, and Performance:A Systematic Review. Int J Sports Phys Ther. 2015;10(6):827–38. [PMC free article] [PubMed] [Google Scholar]
- 11.Couture G, Karlik D, Glass SC, Hatzel BM. The Effect of Foam Rolling Duration on Hamstring Range of Motion. Open Orthop J. 2015;9:450–5. doi: 10.2174/1874325001509010450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Behm DG, Chaouachi A. A review of the acute effects of static and dynamic stretching on performance. Eur J Appl Physiol. 2011;111(11):2633–51. doi: 10.1007/s00421-011-1879-2. [DOI] [PubMed] [Google Scholar]
- 13.Simmonds N, Miller P, Gemmell H. A theoretical framework for the role of fascia in manual therapy. J Bodyw Mov Ther. 2012;16(1):83–93. doi: 10.1016/j.jbmt.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 14.Junker DH, Stoggl TL. The Foam Roll as a Tool to Improve Hamstring Flexibility. J Strength Cond Res. 2015;29(12):3480–5. doi: 10.1519/JSC.0000000000001007. [DOI] [PubMed] [Google Scholar]
- 15.Cochrane DJ. Vibration exercise:the potential benefits. Int J Sports Med. 2011;32(2):75–99. doi: 10.1055/s-0030-1268010. [DOI] [PubMed] [Google Scholar]
- 16.Cochrane DJ. Effectiveness of using wearable vibration therapy to alleviate muscle soreness. Eur J Appl Physiol. 2017;117(3):501–9. doi: 10.1007/s00421-017-3551-y. [DOI] [PubMed] [Google Scholar]
- 17.Munn J, Herbert RD, Gandevia SC. Contralateral effects of unilateral resistance training:a meta-analysis. J Appl Physiol (1985) 2004;96(5):1861–6. doi: 10.1152/japplphysiol.00541.2003. [DOI] [PubMed] [Google Scholar]
- 18.Bernardo-Filho M, de Sa-Caputo Dda C, Marin PJ, Chang S. The mechanism of auriculotherapy:a case report based on the fractal structure of meridian system. Afr J Tradit Complement Altern Med. 2014;11(3):30–7. doi: 10.4314/ajtcam.v11i3.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Evetovich TK, Housh TJ, Housh DJ, Johnson GO, Smith DB, Ebersole KT. The effect of concentric isokinetic strength training of the quadriceps femoris on electromyography and muscle strength in the trained and untrained limb. J Strength Cond Res. 2001;15(4):439–45. [PubMed] [Google Scholar]
- 20.Hortobagyi T, Scott K, Lambert J, Hamilton G, Tracy J. Cross-education of muscle strength is greater with stimulated than voluntary contractions. Motor Control. 1999;3(2):205–19. doi: 10.1123/mcj.3.2.205. [DOI] [PubMed] [Google Scholar]
- 21.Khouw W, Herbert R. Optimisation of isometric strength training intensity. Aust J Physiother. 1998;44(1):43–6. doi: 10.1016/s0004-9514(14)60364-0. [DOI] [PubMed] [Google Scholar]
- 22.Shaver LG. Cross transfer effects of conditioning and deconditioning on muscular strength. Ergonomics. 1975;18(1):9–16. doi: 10.1080/00140137508931435. [DOI] [PubMed] [Google Scholar]
- 23.Shima N, Ishida K, Katayama K, Morotome Y, Sato Y, Miyamura M. Cross education of muscular strength during unilateral resistance training and detraining. Eur J Appl Physiol. 2002;86(4):287–94. doi: 10.1007/s00421-001-0559-z. [DOI] [PubMed] [Google Scholar]
- 24.Calatayud J, Martin F, Gargallo P, Garcia-Redondo J, Colado JC, Marin PJ. The validity and reliability of a new instrumented device for measuring ankle dorsiflexion range of motion. Int J Sports Phys Ther. 2015;10(2):197–202. [PMC free article] [PubMed] [Google Scholar]
- 25.Ortega FB, Artero EG, Ruiz JR, Vicente-Rodriguez G, Bergman P, Hagstromer M, Ottevaere C, Nagy E, Konsta O, Rey-López JP, Polito A, Dietrich S, Plada M, Béghin L, Manios Y, Sjöström M, Castillo MJ HELENA Study Group. Reliability of health-related physical fitness tests in European adolescents. The HELENA Study. Int J Obes (Lond) 2008;32(Suppl 5):S49–57. doi: 10.1038/ijo.2008.183. [DOI] [PubMed] [Google Scholar]
- 26.Gonzalo-Skok O, Serna J, Rhea MR, Marin PJ. Relationships between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players. Int J Sports Phys Ther. 2015;10(5):628–38. [PMC free article] [PubMed] [Google Scholar]
- 27.Kelly S, Beardsley C. Specific and Cross-over Effects of Foam Rolling on Ankle Dorsiflexion Range of Motion. Int J Sports Phys Ther. 2016;11(4):544–51. [PMC free article] [PubMed] [Google Scholar]
- 28.Pellegrini MJ, Lythgo ND, Morgan DL, Galea MP. Voluntary activation of the ankle plantar flexors following whole-body vibration. Eur J Appl Physiol. 2010;108(5):927–34. doi: 10.1007/s00421-009-1304-2. [DOI] [PubMed] [Google Scholar]
- 29.Harwood B, Scherer J, Brown RE, Cornett KM, Kenno KA, Jakobi JM. Neuromuscular responses of the plantar flexors to whole-body vibration. Scand J Med Sci Sports. 2016 doi: 10.1111/sms.12803. [DOI] [PubMed] [Google Scholar]
- 30.Casanova N, Reis JF, Vaz JR, Machado R, Mendes B, Button DC, Pezarat-Correia P, Freitas SR. Effects of roller massager on muscle recovery after exercise-induced muscle damage. J Sports Sci. 2017:1–8. doi: 10.1080/02640414.2017.1280609. [DOI] [PubMed] [Google Scholar]
- 31.Halperin I, Aboodarda SJ, Button DC, Andersen LL, Behm DG. Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int J Sports Phys Ther. 2014;9(1):92–102. [PMC free article] [PubMed] [Google Scholar]
- 32.Morse CI, Degens H, Seynnes OR, Maganaris CN, Jones DA. The acute effect of stretching on the passive stiffness of the human gastrocnemius muscle tendon unit. J Physiol. 2008;586(1):97–106. doi: 10.1113/jphysiol.2007.140434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Ryan ED, Herda TJ, Costa PB, Defreitas JM, Beck TW, Stout J, Cramer JT. Determining the minimum number of passive stretches necessary to alter musculotendinous stiffness. J Sports Sci. 2009;27(9):957–61. doi: 10.1080/02640410902998254. [DOI] [PubMed] [Google Scholar]
- 34.Weppler CH, Magnusson SP. Increasing muscle extensibility:a matter of increasing length or modifying sensation? Phys Ther. 2010;90(3):438–49. doi: 10.2522/ptj.20090012. [DOI] [PubMed] [Google Scholar]
- 35.Lee M, Carroll TJ. Cross education:possible mechanisms for the contralateral effects of unilateral resistance training. Sports Med. 2007;37(1):1–14. doi: 10.2165/00007256-200737010-00001. [DOI] [PubMed] [Google Scholar]
- 36.Jay K, Sundstrup E, Sondergaard SD, Behm D, Brandt M, Saervoll CA, Jakobsen MD, Andersen LL. Specific and cross over effects of massage for muscle soreness:randomized controlled trial. Int J Sports Phys Ther. 2014;9(1):82–91. [PMC free article] [PubMed] [Google Scholar]