

Abstract
Atrial fibrillation (AF) is the most common clinical arrhythmia and is associated with increased morbidity and mortality. There is growing evidence that numerous cardiovascular diseases and risk factors are associated with incident AF and that lone AF is rare. Beyond oral anticoagulant therapy, rate and rhythm control, therapy targeting risk factors and underlying conditions is an emerging AF management strategy that warrants better implementation in clinical practice. This review describes current evidence regarding the association between known modifiable risk factors and underlying conditions and the development and progression of AF. It discusses evidence for the early management of underlying conditions to improve AF outcomes. It also provides perspective on the implementation of tailored AF management in daily clinical practice.
Keywords: Atrial fibrillation, risk factors, lifestyle modification, prevention, integrated management
Atrial fibrillation (AF) is the most common clinical arrhythmia worldwide and is expected to increase in the coming decades.[1,2] It currently affects up to 3 % of Western populations aged 20 years or older, and the number of affected individuals in the EU will increase from about 7 million to almost 13 million by 2030.[3–5] This growing epidemic is not only caused by the natural ageing of the population, but also by the accumulation of chronic cardiovascular diseases and risk factors, and thus at least in part is caused by inadequate lifestyle.[5–7]
AF is a chronic condition and is independently associated with increased morbidity and mortality, including ischaemic stroke, dementia, cognitive dysfunction, heart failure (HF), MI and all-cause mortality.[8–14] Stroke and HF can even be the first manifestation of AF. Although AF can be completely asymptomatic, about two-thirds of patients experience at least intermittent symptoms, which can be disabling and markedly impair health-related quality of life.[15,16] AF-related symptoms and complications, as well as underlying cardiovascular diseases, lead to unplanned hospital admissions in a substantial number of patients every year.[17,18] Therefore, it is not surprising that inpatient AF care accounts for more than two-thirds of the annual direct costs of AF and is the major cost driver.[19–21]
Contemporary AF Management
AF treatment has largely focused on the prevention of stroke and HF as well as symptom control, as reflected in previous European and current American guidelines for the management of AF.[22–24] However, these guidelines make only narrow recommendations on upstream therapy in selected patient groups, e.g. treatment with angiotensin-converting enzyme (ACE) inhibitors or angiotensin Il-receptor blockers (ARBs) in patients with HF or hypertension, or statin treatment in patients with postoperative AF. In contrast, contemporary AF management as outlined in the current European guidelines pursues an integrated approach with five domains that have to be individually addressed according to the needs of each patient.[25] These five domains include: acute rhythm management in patients presenting with hemodynamic instability; detection and treatment of underlying predisposing conditions; stroke risk assessment and oral anticoagulation for stroke prevention; rate control; and rhythm control. The second domain now puts upstream therapy into a much broader perspective. The present review focuses on the detection and treatment of associated diseases and risk factors, i.e. the targeting of underlying conditions.[26]
Early Detection and Treatment of Underlying Conditions
AF is commonly considered a progressive disease - developing from a paroxysmal, self-terminating form through persistent to permanent AF -and is perpetuated by on-going electrical and structural remodelling of the atria.[27–29] Some patients already have persistent AF at the time of first diagnosis.[30] Registry data showed that patients with progression from paroxysmal to more sustained AF were more frequently admitted to hospital due to cardiovascular causes and had more strokes, but were also older and had a larger number of underlying comorbidities such as hypertension, HF, coronary artery disease (CAD) and previous stroke or transient ischaemic attack (TIA).[31,32] A pooled analysis of the non-anticoagulated populations from the Atrial Fibrillation Clopidogrel Trial with Ibersartan for Prevention of Vascular Events (ACTIVE-A) and Apixaban Versus Acetylsalicyclic Acid to Prevent Stroke in Atrial Fibrillation Patients Who Have Failed or Are Unsuitable for Vitamin K Antagonist Treatment (AVERROES) trials found that patients with persistent or permanent AF at baseline had significantly higher stroke rates than those with paroxysmal AF. Findings from recent population-based studies and registries also demonstrated that at least 25-30 % of all patients with an ischaemic stroke and >80 % of those with cardioembolic ischaemic stroke also had AF, suggesting a strong association between these two entities.[3,33–40] Another important finding in this context was that stroke was the first manifestation of previously unknown AF in >25 % of AF-related strokes.[3,33–35,41] This association was even higher if prolonged noninvasive or invasive monitoring was performed following a stroke.[42,43] Taken together, these findings call for earlier diagnosis and comprehensive treatment of AF to reduce stroke risk and improve outcomes.[30]
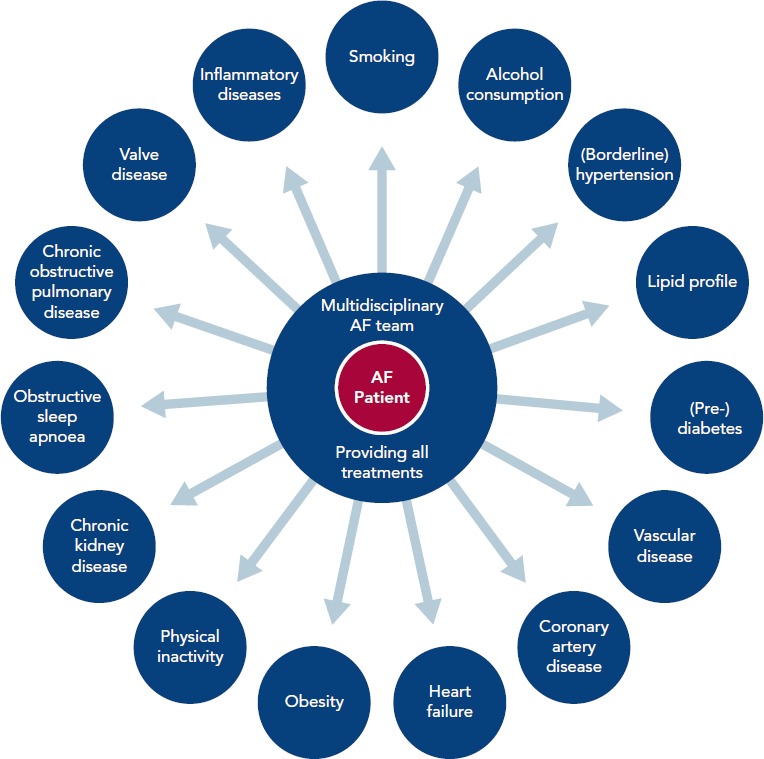
In recent years, a number of risk factors and conditions have been identified that are associated with the development and progression of AF.[7,44–46] A few of these risk factors and predisposing conditions cannot be modified, such as advancing age, gender, ethnicity and genetic predisposition; however, most are modifiable or can at least be optimally treated (Table 1; Figure 1). Many risk factors and underlying conditions predisposing to AF are also risk factors for other cardiovascular conditions such as CAD, vascular disease and HF. Targeting these risk factors and underlying conditions as early as possible - ideally before AF becomes clinically manifest - would not only prevent or reverse atrial remodelling and thus prevent or limit AF progression but also improve the underlying conditions themselves and in turn reduce strokes and other cardiovascular adverse events.[47–49] This becomes even more important in patients with HF, in whom new-onset AF has a marked effect on mortality compared to patients without HF.[50] Moreover, patients with HF who later develop AF have a worse prognosis than those with AF who then develop HF.[51]
Table 1: Modifiable Risk Factors Associated with Atrial Fibrillation that can be Targeted Through Optimal Treatment and Lifestyle Intervention.
| Conventional Risk Factors | Less Established Risk Factors | Emerging Risk Factors |
|---|---|---|
| Coronary heart disease | Chronic obstructive pulmonary disease | Subclinical atherosclerosis |
| Hypertension (>140/90 mmHg) | Left atrial dilatation | Borderline hypertension (between 120/80 mmHg and 140/90 mmHg) |
| Heart failure (with reserved and preserved ejection fraction) | Atrial conduction delay/PR interval | Chronic kidney disease |
| Left ventricular diastolic dysfunction | Subclinical hyperthyroidism | |
| Diabetes | Left ventricular hypertrophy | Inflammation |
| Hyperthyroidism | Elevated natriuretic peptides | |
| Obesity | Obstructive sleep apnoea syndrome | Widened pulse pressure |
| Valvular heart disease | Excessive endurance exercise, physical inactivity, excessive alcohol intake, smoking, caffeine intake |
Source: Adapted from J Am Coll Cardiol, 63, Wyse DG, Van Gelder IC, Ellinor PT, et al, Lone atrial fibrillation: does it exist?, 1715–23, 2014, with permission from Elsevier.[45]
Figure 1: Risk Factors and Underlying Comorbidities to be Addressed in Chronic Comprehensive Atrial Fibrillation Management.
Targeting Risk Factors and Underlying Conditions
Due to our increasing knowledge about AF aetiologies and mechanisms, there are questions as to whether lone AF exists, as a substantial number of patients who would previously have been classified as having lone AF actually have risk factors (Table 1).[45,52] Thoroughly searching for modifiable risk factors and cardiovascular diseases associated with incident AF and initiating treatment as early as possible to prevent or at least delay the development of AF seems prudent (Figure 2).[45] For this reason, AF management should also no longer solely address single domains such as stroke prevention, symptom relief or preservation of left ventricular function, but increasingly rely on a broader individual and complete approach with timely detection and optimal treatment of risk factors and underlying conditions to improve outcomes and reduce AF burden by targeting the substrate for AF in a more fundamental way.[25,53] As patients with AF have different unfavourable risk factor profiles and many have more than one subclinical or clearly elevated modifiable risk factor,[45,54] interventions aiming at risk factor management - including lifestyle modification and treatment and targeting underlying conditions - need to be patient-centred and tailored to individual needs. Thus, targeted therapy of risk factors and underlying conditions has becomes the fourth pillar of integrated AF.[25,55] This was recently investigated in the Routine Versus Aggressive Upstream Rhythm Control for Prevention of Early Atrial Fibrillation in Heart Failure (RACE 3) trial.[26]
Figure 2: Time-dependent Atrial Remodelling and Development of Atrial Fibrillation.
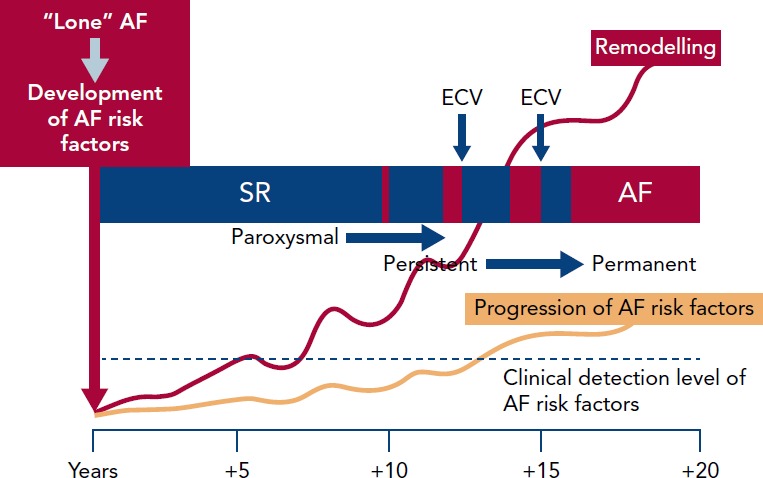
A hypothetic construct over time indicating the interrelationship between time, risk factors for atrial fibrillation (AF), atrial remodelling, detection of risk factors for atrial remodelling and progression from sinus rhythm (SR) through paroxysmal and persistent to permanent AF. ECV = electrical cardioversion. Source: J Am Coll Cardiol, 63, Wyse DG, Van Gelder IC, Ellinor PT, et al, Lone atrial fibrillation: does it exist?, 1715–23, 2014, with permission from Elsevier.[45]
Hypertension
Hypertension is one of the major risk factors for AF. The reported prevalence rates of hypertension in AF studies range from 49 to 90 %.[56] In the Framingham Heart Study, not only stage II-IV hypertension (systolic blood pressure (BP) >160 mmHg and diastolic BP >95 mmHg) was significantly associated with the risk of AF with an odds ratio (OR) of 1.5 for men and 1.4 for women,[57] but also borderline systolic BP was associated with a slightly increased risk of incident AF.[7] Data from the Atherosclerotic Risk in Communities (ARIC) study showed that hypertension (systolic BP ≥140 mmHg or diastolic BP ≥90 mmHg and/or treatment for hypertension) accounted for about 22 % of incident AF. The proportion was even higher (24.5 %) if borderline BP values (systolic BP of 120-139 mmHg or diastolic BP of 80-90 mmHg) were included, meaning that even slightly elevated BP is a clear risk factor for AF.[54] Similar results were reported from the Women’s Health Initiative (WHI) observational study in postmenopausal women, where an elevated systolic (≥140 mmHg) or diastolic (≥90 mmHg) BP accounted for almost one-third of the population-attributable risk of incident AF.[58] In the recently published community-based Prevention of REnal and Vascular ENd-stage Disease (PREVEND) study, use of antihypertensive drugs as a proxy for hypertension more than doubled the risk of incident AF. Likewise, every 10-mmHg increase in systolic BP increased risk for incident AF (HR 1.11).[46]
The first evidence that optimal treatment of hypertension may prevent AF and improve outcomes came from intervention trials in hypertensive patients. In the Losartan Intervention for Endpoint Reduction in Hypertension (LIFE) study, which compared the use of ARB losartan with the beta-blocker atenolol, losartan prevented more cardiovascular morbidity and death than atenolol for a similar reduction in BP.[59] A post-hoc analysis from this trial showed that the greatest reduction (40 %) in risk of incident AF occurred in patients who achieved optimal systolic BP levels of <130 mmHg, compared to those with systolic BP ≥142 mmHg. Moreover, incident AF occurred less frequently in patients treated with losartan than in those treated with atenolol, although there was no significant difference in BP reduction.[60] A Danish nationwide nested case-control study also found less new-onset AF in patients with hypertension treated with ARBs or ACE inhibitors compared to beta-blockers or diuretics.[61] These findings suggest that inhibition of the renin-angiotensin system itself might have a beneficial effect on the reduction of incident AF besides BP control. In a small, randomised study in patients with AF and drug-resistant hypertension undergoing pulmonary vein isolation (PVI) for AF, optimisation of BP treatment by renal denervation on top of PVI significantly reduced AF recurrence at 12 months compared with PVI alone in addition to markedly improved BP.[62] A more comprehensive treatment approach was investigated in the RACE 3 trial, where patients with early persistent AF and mild to moderate HF were randomised to causal treatment of AF and HF alone or targeted treatment with mineralocorticoid receptor antagonists (MRAs), statins, ACE inhibitors or ARBs with a BP target of <120/80 mmHg and cardiac rehabilitation on top of causal treatment. Targeted treatment led not only to significantly improved sinus rhythm maintenance but also better BP control at 1 year.[26]
Heart failure
Beyond age, HF is the most important risk factor for incident AF, increasing the risk by two- to threefold.[9,31,57,63–67] Despite this, HF only accounts for a modest proportion of the population-attributable risk of incident AF and has decreased over recent decades, as demonstrated by data from the Framingham Heart Study.[7,54,58] These reductions could be ascribed to improvements in HF therapy.
Compared to other risk factors and underlying conditions, HF and AF frequently coexist and have a complex interrelationship. They share many fundamental predisposing factors and pathophysiological pathways, promoting each other and mutually leading to a worse prognosis.[50,51,68–70] Data from the PREVEND study have demonstrated that HF is associated with incident AF and that adverse outcomes including HF are associated with AF.[46] In daily practice it is often difficult to determine whether AF is a major contributor to shortness of breath, impaired quality of life, clinical signs and worse prognosis or just a coexisting condition. This is because HF - particularly HF with preserved ejection fraction (HFpEF) - and AF share many common clinical signs and symptoms.[69,70] Optimisation of HF treatment may prevent AF or at least improve sinus rhythm maintenance. Adding MRA treatment to otherwise optimal HF therapy in patients with mild systolic HF leads to a significant reduction of new-onset AF, as shown in an analysis from the Eplerenone in Mild Patients Hospitalization And Survival Study in Heart Failure (EMPHASIS-HF) trial.[71] In addition to improved maintenance of sinus rhythm, comprehensive targeted treatment in the RACE 3 study resulted in improvement of HF, as reflected by a significantly greater decrease in brain natriuretic peptide levels at 1 year compared to baseline.[26]
Coronary and Vascular Disease
CAD is an established risk factor for incident AF. Data from the Framingham Heart Study demonstrated that a history of MI was significantly associated with incident AF in men (OR 1.4), but not women.[57] A later analysis from this study found a significant association when adjusting for age and gender.[65] Krahn et al. found a 3.6-fold increase in the relative risk of AF after MI.[9] Previous MI was also a predictor of incident AF in elderly patients (mean age 75 years; HR 2.2),[63] which was confirmed by the ARIC study[66] and in a combined analysis from the ARIC and Cardiovascular Health Studies.[64] The PREVEND study also found a significant association between previous MI and stroke and incident AF, with incidence rates of AF comparable to those described in several of the studies mentioned above, although these studies recruited patients much earlier than PREVEND and the treatment of patients with MI and stroke has markedly improved over time. However, incident AF was associated with an increased risk of all forms of vascular disease, HF and death.[46] According to data from the Framingham Heart Study, the population-attributable risk of MI remained unchanged over 5 decades despite substantial improvements in the treatment of MI during this time.[7] Weijs et al. found a surprisingly high proportion of patients with subclinical CAD in a relatively young (mean age 55 years) cohort of patients with an original diagnosis of lone AF compared to matched controls with sinus rhythm.[72] Some of these patients had already developed advanced CAD. Taking into account that patients with AF and vascular disease are at increased risk of fatal and non-fatal cardiovascular events, it seems prudent to screen patients with AF for vascular diseases because treatment in an early stage could reduce AF and improve their prognosis.[73] Hypercoagulability may also lead to fibroblast activation, cellular hypertrophy and fibrosis; in this way it may be involved in the creation of a substrate for AF.[29,52,74] The contribution of hypercoagulability to the progression of AF is currently being investigated in the RACE V study (ClinicalTrials.gov, NCT03124576).
Obesity
The evidence that obesity is an independent risk factor for incident AF has grown in recent years. Data from the ARIC study showed that overweight and obesity (BMI ≥25 kg/m2) accounted for about 18 % of incident AF, making obesity the second strongest risk factor for AF.[54] Comparable results were found in the WHI observational study, where these conditions accounted for 12 % of the population-attributable risk.[58] Interestingly, obesity is not only a risk factor for incident AF in postmenopausal women but also in young and essentially healthy women.[75] Data from the Framingham Heart Study demonstrated a 4 % increase in AF risk for each unit increase in BMI. Obesity (BMI ≥30 kg/m2) was significantly associated with incident AF in men and women.[76] There has been an increase in the population-attributable risk of obesity for incident AF in the past 50 years[7] and numerous cohort and case-control studies have confirmed the strong and consistent association between obesity and AF.[46,58,77–82] A recent meta-analysis found not only a 29 % and 19 % increase in incident AF risk for every 5 additional BMI units, respectively, but also a 10 % increase in postoperative AF and a 13 % increase in post-ablation AF.[83] The PREVEND study found similar results, with an increased rate of incident AF for every 5 additional BMI units.[46] Taking these results into account and the fact that overweight is associated with increased risk of fatal and non-fatal coronary heart disease outcomes, it seems prudent to implement fitness and weight reduction in AF therapy.[84,85] Cardiac rehabilitation, including regular physical activity, dietary restrictions and scheduled counselling, should be part of a comprehensive targeted treatment approach. In the RACE 3 trial, this approach led to a slight reduction in BMI and weight at 1 year as well as improved sinus rhythm maintenance.[26] These figures also demonstrate that a substantial improvement requires long-term patient involvement and persistent adherence to treatment.
Diabetes
Diabetes and elevated blood glucose (BG) levels are also significant risk factors for incident AF, as demonstrated in several studies. However, the results are conflicting and difficult to compare due to differences in methodology, e.g. adjustment for confounding variables which was not performed in all studies. Data from the ARIC study showed that diabetes and poor glycaemic control, reflected by elevated HbA1c levels, were independently associated with an increased risk of incident AF.[86] However, another analysis from the same study demonstrated that only 3 % of incident AF was attributable to diabetes.[54] The same population-attributable risk was seen in the in WHI observational study.[58] The population-attributable risk of diabetes increased over time despite improvements in treatment.[7] In a recent Danish nationwide cohort study, the risk for incident AF was most pronounced in diabetes patients aged 18-39 years.[87] Poor glycaemic control and longer duration of diabetes were also associated with incident AF in a population-based case-control study that identified a 3 % higher risk of incident AF for each year of diabetes duration.[88] In a meta-analysis, individuals with diabetes had 39 % greater risk of incident AF than unaffected individuals.[89] Interestingly, AF in patients with diabetes is associated with 61 % greater risk of all-cause mortality and a comparable higher risk of cardiovascular death, stroke and HF.[90] The pathophysiological mechanisms implicated in promoting AF in individuals with diabetes are complex and include autonomic, electrical, electromechanical and structural remodelling, oxidative stress, connexin remodelling and glycaemic fluctuations.[91] In general, patients with metabolic disorders including diabetes already have an increased risk of fatal and non-fatal coronary heart disease outcomes.[84] Taking all these findings together, the vicious combination of AF and diabetes warrants timely evaluation and treatment. In a population-based study, metformin use was associated with a significant reduction in new-onset AF in patients with type 2 diabetes who were not taking other antidiabetic medications.[92]
Physical Inactivity and Cardiorespiratory Fitness
It is generally accepted that physical activity considerably lowers cardiovascular mortality and morbidity, which is why it is also recommended in current cardiovascular disease prevention guidelines.[93] Greater cardiorespiratory fitness (CRF) reduces all-cause mortality and cardiovascular events.[94] Results from a large cohort study also showed a graded inverse relationship between CRF and the development of AF, especially in obese patients: every additional metabolic equivalent achieved during exercise testing was associated with a 7 % lower risk of incident AF.[95] Similar results were found in a large Swedish cohort study in middle-aged and elderly women that compared self-reported levels of leisure activity. The risk of developing AF decreased with increasing levels of leisure-time exercise at study entry.[96] However, the relationship between the amount of exercise and incident AF does not seem to be linear but U-shaped - at least in older adults. This was demonstrated by data from the Cardiovascular Health Study, where individuals doing moderate-intensity exercise developed less AF than those doing high-intensity exercise or no exercise.[97] A similar U-shaped relationship has also been found between CRF and incident AF.[98] Currently, no exact dose-response relationship has been established between physical activity and reduction of incident AF, but evidence suggests that >220 minutes of moderate-intensity exercise per week or a CRF >8 metabolic equivalents carries a lower risk of AF; whereas high-intensity exercise and endurance training might be harmful and increase this risk.[99,100] In practice, routine exercise testing to determine CRF and identify patients at higher risk of AF as well as recommending 150-200 minutes of moderate-intensity exercise per week could be an appropriate solution and should be implemented in the management of AF.[85,93,101] This strategy has been investigated as part of a comprehensive targeted treatment approach in the RACE 3 trial, which improved sinus rhythm maintenance.[26]
Renal Dysfunction
Beyond the established risk factors and conditions associated with AF such as age, hypertension, DM, HF and obesity, renal dysfunction has also been related to incident AF. In the ARIC study, reduced renal function and the presence of albuminuria were strongly associated with incident AF independent of other risk factors.[102] Similar results were found in the PREVEND study, where microalbuminuria - as a measure of renal vascular dysfunction - was related to incident AF independent of cardiovascular risk factors.[103] Likewise, in the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, renal dysfunction - regardless of severity - was associated with increased prevalence of AF.[104] On the other hand, patients with AF have a higher risk of chronic kidney disease, as demonstrated by a large population-based study from the UK and a meta-analysis including approximately 10 million patients from 104 studies.[105,106]
Reduced renal function is associated with increased risk of adverse cardiovascular outcomes, such as stroke and HF.[107,108] It has also been associated with increased risk of stroke and systemic embolism in patients with non-valvular AF.[109] The coexistence of both conditions results in a marked increase in both thromboembolic and haemorrhagic risk.[110] AF and chronic kidney disease not only share risk factors such as DM, hypertension and HF;111 there is growing evidence that both diseases share underlying pathophysiological mechanisms, such as left ventricular hypertrophy, inflammation, hypercoagulability and activation of the renin-angiotensin-aldosterone system.[112–116] Timely treatment of risk factors and underlying conditions could lead to improvement of both conditions and reduce adverse outcomes.
Obstructive Sleep Apnoea
In recent years, obstructive sleep apnoea (OSA) has emerged as one of the novel risk factors for AF.[45] Sleep-disordered breathing is a common condition: at least mild OSA affects one in five adults; whereas one in 15 has moderate or severe OSA.[117] Moreover, there is a higher prevalence of OSA in men and obese adults, while advancing age and increasing BMI also are risk factors for incident OSA.[118] Among patients with AF, the prevalence of OSA is estimated at about 50 % or even higher.[119,120] Patients with OSA have a significantly higher risk of developing AF, especially those with severe disease.[121,122] A study in patients with OSA and symptomatic AF undergoing AF ablation showed that arrhythmia-free survival was better in those receiving continuous positive air pressure treatment than in those not on this treatment.[123] It is important to note that OSA and AF share several characteristics - hypertension, diabetes, obesity and advancing age are common in both conditions. Screening for OSA is regarded as important when evaluating patients with AF, particularly in those with obesity and hypertension. This can be achieved by using simple scoring systems, e.g. the NoSAS score.[124]
Alcohol Consumption
Acute heavy alcohol consumption has long been known as a cause of AF and is commonly called “holiday heart” syndrome.[125] Binge drinking was associated with increased risk of incident AF in an analysis of pooled data from two antihypertensive drug treatment trials.[126] Several prospective cohort studies have also looked at the association between chronic alcohol consumption and incident AF. However, the issue with such studies is that, in contrast to other risk factors for AF that can be objectively measured, the quantities of alcohol intake are usually self-reported by the enrolled individuals. Data from the Framingham Heart Study suggested that heavy alcohol consumption of >36 g/day (>3 drinks/day) was associated with a significantly increased risk of incident AF, but also showed that heavy alcohol consumption has decreased over time.[7,127] Similar results were reported from the Copenhagen City Heart Study.[128] Women who consumed ≥2 drinks/ day also had an increased risk of AF, as shown in an analysis from the Women’s Health Study.[129] More recently, data form a prospective Swedish cohort study demonstrated that consumption of even small quantities of alcohol was associated with increased risk of AF.[130] Furthermore, two meta-analyses showed a linear dose-response relationship between alcohol intake and risk of AF, with a significant 8 % increase in the relative risk of incident AF for each standard drink per day compared to no drinks a day.[130,131] These results suggest that there is no safe level of chronic alcohol intake with regard to the development of AF.
Smoking
Numerous cohort studies have investigated the association between smoking and incident AF. Some of them found an increase in risk -ranging from 32 % to more than a doubling in current smokers and 32-49 % in former smokers[9,54,132–135] - while other studies did not.[77,136–139] An analysis from the ARIC study showed that current smoking accounted for about 10 % of incident AF.[54] Moreover, there might also be a dose-response relationship, in that current smokers with the longest duration of smoking and those with the highest number of cigarettes per day had the highest risk of AF.[132,133] Generally, smoking cessation is recommended, but data on AF prevention are lacking.
Dyslipidaemia
Current data on the association between dyslipidaemia and incident AF are inconsistent. Unlike ischaemic heart disease, which is clearly associated with elevated LDL cholesterol, it seems that there is an inverse correlation between LDL levels and the development of AF, as shown in several epidemiological studies.[138,140–142] Analysis of a pooled dataset from the Multi-ethnic Study of Atherosclerosis (MESA) and the Framingham Heart Study did not find any association between LDL levels and AF, but higher levels of HDL cholesterol and lower levels of triglycerides were associated with lower AF risk.[143] The association between higher HDL levels and lower AF risk was also found in two other studies,[142,144] whereas no such association was found in an analysis of data from the Women’s Health Study.[141] A recent post-hoc analysis from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial showed that patients with AF and higher levels of apolipoprotein A1 had a lower risk of adverse outcomes, i.e. ischaemic stroke, systemic embolism, MI and cardiovascular death, suggesting that interventions increasing HDL levels could have a beneficial effect.[145]
Data on the effect of lipid-lowering therapy on AF predominantly come from retrospective and small randomised studies investigating statins in patients with post-operative AF (POAF) and their results are mixed.[146] A large randomised, controlled trial of rosuvastatin in patients with POAF did not show any beneficial effect of statin treatment in AF prevention.[147] Nevertheless, a comprehensive treatment strategy targeting vascular diseases including lipid-lowering therapy with statins could prevent AF progression and improve sinus rhythm maintenance, as shown in the RACE 3 trial.[26]
Comprehensive Management of Risk Factors and Underlying Conditions
While substantial improvements have been achieved in the field of anticoagulation to reduce stroke and its associated disease burden in patients with AF, important unmet therapeutic needs remain, particularly regarding the prevention of cardiovascular death, HF, unplanned cardiovascular hospitalisations and rhythm control.[25,52,148–155] This has led to the concept that “upstream therapy” or “prevention of atrial remodelling” could improve the outcome of rhythm control therapy and possibly also prognosis in patients with AF.[30,53,156] Several early retrospective and observational studies on upstream therapy with ACE inhibitors, ARBs and statins have produced encouraging results in terms of reduction in AF recurrences, but larger prospective randomised placebo-controlled trials have failed to show any significant reduction in AF recurrences and adverse cardiovascular outcomes, possibly because these studies only addressed a single risk factor.[147,157–161]
More recently, evidence has become available that comprehensive interventions that aim to reduce risk factors and underlying conditions of AF are able to reduce AF recurrence and burden in addition to improving the underlying conditions (Table 2). In a small randomised study in overweight or obese patients with symptomatic paroxysmal or persistent AF structured weight management and regular exercise in addition to intensive cardiometabolic risk-factor management led to greater weight reduction, greater reduction of the severity and burden of AF symptoms, and fewer and shorter AF episodes on Holter monitoring compared with general lifestyle advice and cardiometabolic risk-factor management.[162] Structured weight management also led to a significant decline in left atrial volumes and pericardial adipose tissue compared with controls.[163] Two other non-randomised studies from the same group also showed that aggressive risk-factor management including a structured weight management programme had beneficial effects in terms of AF recurrence, severity and burden of AF symptoms and global well-being in patients with symptomatic AF who were medically managed and underwent catheter ablation for AF.[164,165] Importantly, greater weight fluctuations also led to a significantly increased risk of AF recurrence.[164] Similar results were reported from a retrospective Italian study in patients with AF - those with higher and increasing BMI had a greater risk of AF recurrence during long-term follow-up.[166]
Table 3: Studies Investigating Risk Factor Management for Secondary Atrial Fibrillation Prevention.
| Study | Design | Subjects n (% women) | AF | Follow-up (months) | Intervention | Outcomes |
|---|---|---|---|---|---|---|
| Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation[162] | Prospective, randomised controlled study | 150 (33 %) | Paroxysmal or persistent AF, BMI ≥27 kg/m2 | 15 | Structured weight management versus general lifestyle advice | Significantly greater reduction in weight (14.3 versus 3.6 kg); AF symptom burden scores (11.8 versus 2.6 points); symptom severity scores (8.4 versus 1.7 points); AF episodes (2.5 versus no change); cumulative AF duration (692 min decline versus 419 min increase) |
| LEGACY164 | Prospective observational cohort study | 355 (34 %) | Paroxysmal or persistent AF, BMI ≥27 kg/m2 | 60 | Structured weight management; tailored risk-factor management | Significantly greater decrease in AF burden and symptom severity in WL ≥10 %; WL ≥10 % with sixfold greater probability of freedom from AF; weight fluctuation >5 % with twofold increased AF recurrence |
| BMI Reduction Decreases AF Recurrence Rate in a Mediterranean Cohort[166] | Retrospective cohort study | 258 (n/r) | Paroxysmal or permanent AF; BMI >25 kg/m2 | 602 patient-years (overall) | Diet and/or moderate exercise | AF recurrence most frequent in patients with BMI >25 kg/m2 and weight gain ≥2 units |
| ARREST-AF165 | Prospective cohort study with control group | 149 (36 %) | Symptomatic AF scheduled for ablation; BMI ≥27 kg/m2 plus ≥1 other risk factor(s) | 42 (mean) | Structured weight management; aggressive risk-factor management versus information and risk-factor management by treating physician | Significant decrease in AF frequency, duration, symptoms and symptom severity versus controls; single-procedure AF-free survival off drugs markedly better than in controls |
| CARDIO-FIT167 | Prospective cohort study | 308 (51 %) | Symptomatic paroxysmal or persistent AF; BMI ≥27 kg/m2 | 49 (mean) | Risk-factor management and tailored exercise programme | AF-free survival greatest in patients with highest cardiorespiratory fitness; AF burden and symptom severity decreased significantly in patients with cardiorespiratory fitness gain ≥2 METs; AF-free survival greatest in patients with cardiorespiratory fitness gain ≥2 METs |
| RACE 326 | Prospective, randomised controlled trial | 245 (21 %) | Early persistent AF and mild-to-moderate HF | 12 | Conventional therapy (causal treatment of AF and HF and rhythm control therapy) versus conventional therapy plus medical therapy with MRAs, statins, ACE-Is and/or ARBs, and cardiac rehabilitation including physical activity, dietary restriction, and counselling | Significantly more patients in sinus rhythm at 1 year follow-up with targeted therapy of underlying conditions compared to conventional therapy; significantly more successful modification of blood pressure, NT-proBNP, weight, BMI and lipid profile with targeted therapy of underlying conditions compared to conventional therapy; AF symptoms decreased more with targeted therapy |
ACE-I = angiotensin-converting enzyme inhibitor; ARB = angiotensin II-receptor blocker; ARREST AF = Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation; CARDIO-FIT = CARDIOrespiratory FITness on Arrhythmia Recurrence in Obese Individuals With Atrial Fibrillation; HF = heart failure; LEGACY = Long-Term Effect of Goal-Directed Weight Management in an Atrial Fibrillation Cohort: A Long-Term Follow-Up Study; METs = metabolic equivalents; MRA = mineralocorticoid receptor antagonist; NT-proBNP = N-terminal pro-brain natriuretic peptide; n/r = not reported; RACE 3 = Routine Versus Aggressive Upstream Rhythm Control for Prevention of Early Atrial Fibrillation in Heart Failure; WL = weight loss.
In the CARDIOrespiratory FITness on Arrhythmia Recurrence in Obese Individuals With Atrial Fibrillation (CARDIO-FIT) study, risk factor management and a comprehensive exercise programme led to the greatest reduction in AF recurrence in individuals who had the highest CRF at baseline, and those with the greatest CRF gain and weight loss, suggesting an additional benefit of CRF on top of weight loss.[167] Overall, the findings of CARDIO-FIT suggest that fitness might be even more important than weight loss. It is important to recognise that all Australian studies used an aggressive risk-factor management approach in very motivated patients, which might be difficult to apply in daily clinical practice (Table 2).
There is a lack of prospective randomised trials investigating the effect of comprehensive risk-factor management in patients with AF. The RACE 3 trial investigated whether targeted therapy of underlying conditions on top of causal treatment of AF and HF and rhythm control therapy was superior for the prevention of AF in patients with HF compared to causal treatment of AF and HF and rhythm control alone.[26] The primary endpoint was sinus rhythm on 7-day Holter monitoring at 12 months. Inclusion criteria were a history of HF <12 months and early symptomatic persistent AF of <6 months duration, not more than one direct current cardioversion, and history of AF <5 years. Targeted therapy included treatment with MRA, statins and ACE inhibitors or ARBs as well as cardiac rehabilitation including supervised physical training two to three times a week, dietary restrictions and counselling.[53] At 12 months, significantly more patients in the targeted therapy group had sinus rhythm compared to conventional therapy alone. Moreover, targeted therapy of the underlying conditions led to significantly more successful modification of BP, N-terminal pro-brain natriuretic peptide, weight, BMI and lipid profile. Additionally, AF symptoms assessed by European Heart Rhythm Association symptom score decreased more in the targeted therapy group.
Contemporary Integrated AF Management
Patients with AF commonly have multiple risk factors and underlying conditions to deal with. This is why AF care becomes increasingly complex and is ideally delivered through an integrated multidisciplinary approach,[25,52,151] where medical or invasive treatments and management of risk factors and underlying conditions are tailored and adjusted over time according to the individual needs of patients. As lifestyle interventions and treatment adherence are recognised as being increasingly important, patient involvement in the care process is central in AF management. Key elements of this process are the provision of tailored information about the disease, advice and education on lifestyle modification and risk-factor management, empowerment for self-management, and patient involvement in all treatment decisions, e.g. through shared medical decision-making. Given encouraging data on integrated AF care interventions, a dedicated multidisciplinary AF team or clinic systematically coordinating the patient care and determining individual treatment goals according to current recommendations is key (Table 3).[168–171] In the future, early and comprehensive management of risk factors and underlying conditions targeting the substrate of AF together with optimal oral anticoagulation and early targeted and direct treatment of electrical drivers of AF provided by a multidisciplinary AF team could slow progression and improve the outcomes of AF.[154,172]
Table 3: Risk Factor Management Strategies and Treatment Goals.
| Risk Factor | Treatment Goal | Comments |
|---|---|---|
| Hypertension | Blood pressure <140/90 mmHg93 Blood pressure <130/80 mmHg173 |
For atrial fibrillation prevention consider angiotensin-converting enzyme inhibitor, angiotensin II-receptor blocker,[174] beta-blocker or mineralocorticoid receptor antagonist |
| Obesity | BMI 20-25 kg/m2;93 BMI 18.5-24.9 kg/m2, weight loss 5-10 % baseline weight if BMI ≥25 kg/m2 174 |
Avoid weight fluctuations |
| Diabetes | HbA1c ≤7.0 %93,[176] | Metformin as first-line therapy[93,174] |
| Physical inactivity | Physical activity of moderate intensity 150-200 min/week93 Aerobic exercise 90-150 min/week173 |
|
| Obstructive sleep apnoea | Appropriate screening, particularly in high-risk patients (hypertension, obesity), manage with continuous positive airway pressure | |
| Alcohol consumption | Maximum of two glasses per day (20 g/day of alcohol) for men and one glass per day (10 g/day of alcohol) for women[93,173] | |
| Smoking | Complete cessation | |
| Dyslipidaemia | LDL cholesterol <2.6 mmol/l or at least 50 % if baseline LDL cholesterol 2.6-5.1 mmol/l in patients at high cardiovascular risk[93] No specific LDL cholesterol targets[175] |
Use statins |
Conclusion
Common cardiovascular risk factors - such as hypertension, DM, obesity, OSA, physical inactivity and alcohol consumption - as well as underlying conditions like HF and CAD significantly contribute to the development of AF. Optimal and timely management targeting these conditions is feasible, reduces AF and improves quality of life. However, it remains to be proven whether these interventions also have an impact on other outcomes, such as mortality, cerebrovascular events and cardiovascular hospitalisations.
Acknowledgments
Netherlands Cardiovascular Research Initiative: an initiative with support of the Dutch Heart Foundation, CVON 2014-9: Reappraisal of Atrial fibrillation: interaction between hyperCoagulability, Electrical remodeling, and Vascular destabilisation in the progression of AF (RACE V).
References
- 1.Chugh SS, Havmoeller R, Narayanan K et al. Worldwide epidemiology of atrial fibrillation: a Global Burden of Disease 2010 Study. Circulation. 2014;129:837–47. doi: 10.1161/CIRCULATIONAHA.113.005119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Colilla S, Crow A, Petkun W et al. Estimates of current and future incidence and prevalence of atrial fibrillation in the U.S. adult population. Am J Cardiol. 2013;112:1142–7. doi: 10.1016/j.amjcard.2013.05.063. [DOI] [PubMed] [Google Scholar]
- 3.Bjorck S, Palaszewski B, Friberg L, Bergfeldt L. Atrial fibrillation, stroke risk, and warfarin therapy revisited: a population-based study. Stroke. 2013;44:3103–8. doi: 10.1161/STROKEAHA.113.002329. [DOI] [PubMed] [Google Scholar]
- 4.Haim M, Hoshen M, Reges O et al. Prospective national study of the prevalence, incidence, management and outcome of a large contemporary cohort of patients with incident non-valvular atrial fibrillation. J Am Heart Assoc. 2015;4:e001486. doi: 10.1161/JAHA.114.001486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Krijthe BP, Kunst A, Benjamin EJ et al. Projections on the number of individuals with atrial fibrillation in the European Union, from 2000 to 2060. Eur Heart J. 2013;34:2746–51. doi: 10.1093/eurheartj/eht280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chao TF, Liu CJ, Chen SJ et al. CHADS2 score and risk of new-onset atrial fibrillation: a nationwide cohort study in Taiwan. Int J Cardiol. 2013;168:1360–3. doi: 10.10/j.ijcard.2012.12.011. [DOI] [PubMed] [Google Scholar]
- 7.Schnabel RB, Yin X, Gona P et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: a cohort study. Lancet. 2015;386:154–62. doi: 10.1016/S0140-6736(14)61774-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–8. doi: 10.1161/01.str.22.8.983. [DOI] [PubMed] [Google Scholar]
- 9.Krahn AD, Manfreda J, Tate RB et al. The natural history of atrial fibrillation: incidence, risk factors, and prognosis in the Manitoba Follow-Up Study. Am J Med. 1995;98:476–84. doi: 10.1016/S0002-9343(99)80348-9. [DOI] [PubMed] [Google Scholar]
- 10.de Bruijn RF, Heeringa J, Wolters FJ et al. Association between atrial fibrillation and dementia in the general population. JAMA Neurol. 2015;72:1288–94. doi: 10.1001/jamaneurol.2015.2161. [DOI] [PubMed] [Google Scholar]
- 11.Miyasaka Y, Barnes ME, Petersen RC et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: data from a community-based cohort. Eur Heart J. 2007;28:1962–7. doi: 10.1093/eurheartj/ehm012. [DOI] [PubMed] [Google Scholar]
- 12.Soliman EZ, Safford MM, Muntner P et al. Atrial fibrillation and the risk of myocardial infarction. JAMA Intern Med. 2014;174:107–14. doi: 10.1001/jamainternmed.2013.11912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Soliman EZ, Lopez F, O’Neal WT et al. Atrial fibrillation and risk of ST-segment-elevation versus non-ST-segment-elevation myocardial infarction: The Atherosclerosis Risk in Communities (ARIC) Study. Circulation. 2015;131:1843–50. doi: 10.1161/CIRCULATIONAHA.114.014145. PubMed Central. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Benjamin EJ, Wolf PA, D’Agostino RB et al. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946–52. doi: 10.1161/01.cir.98.10.946. [DOI] [PubMed] [Google Scholar]
- 15.Nieuwlaat R, Capucci A, Camm AJ et al. Atrial fibrillation management: a prospective survey in ESC member countries: the Euro Heart Survey on Atrial Fibrillation. Eur Heart J. 2005;26:2422–34. doi: 10.1093/eurheartj/ehi505. [DOI] [PubMed] [Google Scholar]
- 16.Dorian P, Jung W, Newman D et al. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: implications for the assessment of investigational therapy. J Am Coll Cardiol. 2000;36:1303–9. doi: 10.1016/s0735-1097(00)00886-x. [DOI] [PubMed] [Google Scholar]
- 17.Steinberg BA, Kim S, Fonarow GC et al. Drivers of hospitalization for patients with atrial fibrillation: Results from the Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT-AF) Am Heart J. 2014;167:735–42 e2. doi: 10.1016/j.ahj.2014.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Healey JS, Oldgren J, Ezekowitz M et al. Occurrence of death and stroke in patients in 47 countries 1 year after presenting with atrial fibrillation: a cohort study. Lancet. 2016;388:1161–9. doi: 10.1016/S0140-6736(16)30968-0. [DOI] [PubMed] [Google Scholar]
- 19.Stewart S, Murphy NF, Walker A et al. Cost of an emerging epidemic: an economic analysis of atrial fibrillation in the UK. Heart. 2004;90:286–92. doi: 10.1136/hrt.2002.008748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kim MH, Johnston SS, Chu BC et al. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes. 2011;4:313–20. doi: 10.1161/CIRCOUTCOMES.110.958165. [DOI] [PubMed] [Google Scholar]
- 21.Wolowacz SE, Samuel M, Brennan VK et al. The cost of illness of atrial fibrillation: a systematic review of the recent literature. Europace. 2011;13:1375–85. doi: 10.1093/europace/eur194. [DOI] [PubMed] [Google Scholar]
- 22.European Heart Rhythm Association, European Association for Cardio-Thoracic Society. Camm AJ, Kirchhof P, Lip GY et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Eur Heart J. 2010;31:2369–429. doi: 10.1093/eurheartj/ehq278. [DOI] [PubMed] [Google Scholar]
- 23.Camm AJ, Lip GY, De Caterina R et al. 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J. 2012;33:2719–47. doi: 10.1093/eurheartj/ehs253. [DOI] [PubMed] [Google Scholar]
- 24.January CT, Wann LS, Alpert JS et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:e199–267. doi: 10.1161/CIR.0000000000000041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kirchhof P, Benussi S, Kotecha D et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–962. doi: 10.1093/eurheartj/ehw210. [DOI] [PubMed] [Google Scholar]
- 26.Rienstra M, Hobbelt AH, Alings M Targeted therapy of underlying conditions improves sinus rhythm maintenance in patients with persistent atrial fibrillation: results of the RACE 3 trial. Eur Heart J. 2018. epub ahead of press. [DOI] [PubMed]
- 27.Kerr CR, Humphries KH, Talajic M et al. Progression to chronic atrial fibrillation after the initial diagnosis of paroxysmal atrial fibrillation: results from the Canadian Registry of Atrial Fibrillation. Am Heart J. 2005;149:489–96. doi: 10.1016/j.ahj.2004.09.053. [DOI] [PubMed] [Google Scholar]
- 28.Andrade J, Khairy P, Dobrev D, Nattel S. The clinical profile and pathophysiology of atrial fibrillation: relationships among clinical features, epidemiology, and mechanisms. Circ Res. 2014;114:1453–68. doi: 10.1161/CIRCRESAHA.114.303211. [DOI] [PubMed] [Google Scholar]
- 29.Schotten U, Verheule S, Kirchhof P, Goette A. Pathophysiological mechanisms of atrial fibrillation: a translational appraisal. Physiol Rev. 2011;91:265–325. doi: 10.1152/physrev.00031.2009. [DOI] [PubMed] [Google Scholar]
- 30.Nattel S, Guasch E, Savelieva I et al. Early management of atrial fibrillation to prevent cardiovascular complications. Eur Heart J. 2014;35:1448–56. doi: 10.1093/eurheartj/ehu028. [DOI] [PubMed] [Google Scholar]
- 31.de Vos CB, Pisters R, Nieuwlaat R et al. Progression from paroxysmal to persistent atrial fibrillation clinical correlates and prognosis. J Am Coll Cardiol. 2010;55:725–31. doi: 10.1016/j.jacc.2009.11.040. [DOI] [PubMed] [Google Scholar]
- 32.De Vos CB, Breithardt G, Camm AJ et al. Progression of atrial fibrillation in the REgistry on Cardiac rhythm disORDers assessing the control of Atrial Fibrillation cohort: clinical correlates and the effect of rhythm-control therapy. Am Heart J. 2012;163:887–93. doi: 10.10/j.ahj.2012.02.015. [DOI] [PubMed] [Google Scholar]
- 33.Leyden JM, Kleinig TJ, Newbury J et al. Adelaide stroke incidence study: declining stroke rates but many preventable cardioembolic strokes. Stroke. 2013;44:1226–31. doi: 10.1161/STROKEAHA.113.675140. [DOI] [PubMed] [Google Scholar]
- 34.Friberg L, Rosenqvist M, Lindgren A et al. High prevalence of atrial fibrillation among patients with ischemic stroke. Stroke. 2014;45:2599–605. doi: 10.1161/STROKEAHA.114.006070. [DOI] [PubMed] [Google Scholar]
- 35.Yiin GS, Howard DP, Paul NL et al. Recent time trends in incidence, outcome and premorbid treatment of atrial fibrillation-related stroke and other embolic vascular events: a population-based study. J Neurol Neurosurg Psychiatry. 2017;88:12–8. doi: 10.1136/jnnp-2015-311947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Jannou V, Timsit S, Nowak E et al. Stroke with atrial fibrillation or atrial flutter: a descriptive population-based study from the Brest stroke registry. BMC Geriatr. 2015;15:63. doi: 10.1186/s12877-015-0067-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Palm F, Kleemann T, Dos Santos M et al. Stroke due to atrial fibrillation in a population-based stroke registry (Ludwigshafen Stroke Study) CHADS(2), CHA(2) DS(2) -VASc score, underuse of oral anticoagulation, and implications for preventive measures. Eur J Neurol. 2013;20:117–23. doi: 10.1111/j.1468-1331.2012.03804.x. [DOI] [PubMed] [Google Scholar]
- 38.Hannon N, Sheehan O, Kelly L et al. Stroke associated with atrial fibrillation-incidence and early outcomes in the north Dublin population stroke study. Cerebrovasc Dis. 2010;29:43–9. doi: 10.1159/000255973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Bejot Y, Ben Salem D, Osseby GV et al. Epidemiology of ischemic stroke from atrial fibrillation in Dijon, France, from 1985 to 2006. Neurology. 2009;72:346–53. doi: 10.1212/01.wnl.0000341280.31919.bd. [DOI] [PubMed] [Google Scholar]
- 40.Marini C, De Santis F, Sacco S et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke. 2005;36:1115–9. doi: 10.1161/01.STR.0000166053.83476.4a. [DOI] [PubMed] [Google Scholar]
- 41.Yiin GS, Howard DP, Paul NL et al. Age-specific incidence, outcome, cost, and projected future burden of atrial fibrillation-related embolic vascular events: a population-based study. Circulation. 2014;130:1236–44. doi: 10.1161/CIRCULATIONAHA.114.010942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gladstone DJ, Spring M, Dorian P et al. Atrial fibrillation in patients with cryptogenic stroke. N Engl J Med. 2014;370:2467–77. doi: 10.1056/NEJMoa1311376. [DOI] [PubMed] [Google Scholar]
- 43.Sanna T, Diener HC, Passman RS et al. Cryptogenic stroke and underlying atrial fibrillation. N Engl J Med. 2014;370:2478–86. doi: 10.1056/NEJMoa1313600. [DOI] [PubMed] [Google Scholar]
- 44.Kirchhof P, Lip GY, Van Gelder IC et al. Comprehensive risk reduction in patients with atrial fibrillation: emerging diagnostic and therapeutic options--a report from the 3rd Atrial Fibrillation Competence NETwork/European Heart Rhythm Association consensus conference. Europace. 2012;14:8–27. doi: 10.1093/europace/eur241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Wyse DG, Van Gelder IC, Ellinor PT et al. Lone atrial fibrillation: does it exist? J Am Coll Cardiol. 2014;63:1715–23. doi: 10.10/j.jacc.2014.01.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Vermond RA, Geelhoed B, Verweij N et al. Incidence of Atrial Fibrillation and Relationship With Cardiovascular Events, Heart Failure, and Mortality: A Community-Based Study From the Netherlands. J Am Coll Cardiol. 2015;66:1000–7. doi: 10.1016/jjacc.2015.06.1314. [DOI] [PubMed] [Google Scholar]
- 47.Cosio FG, Aliot E, Botto GL et al. Delayed rhythm control of atrial fibrillation may be a cause of failure to prevent recurrences: reasons for change to active antiarrhythmic treatment at the time of the first detected episode. Europace. 2008;10:21–7. doi: 10.1093/europace/eum276. [DOI] [PubMed] [Google Scholar]
- 48.Group SR, Wright JT, Jr, Williamson JD et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103–16. doi: 10.1056/NEJMoa1511939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Yusuf S, Lonn E, Pais P et al. Blood-pressure and cholesterol lowering in persons without cardiovascular disease. N Engl J Med. 2016;374:2032–43. doi: 10.1056/NEJMoa1600177. [DOI] [PubMed] [Google Scholar]
- 50.Santhanakrishnan R, Wang N, Larson MG et al. Atrial fibrillation begets heart failure and vice versa: temporal associations and differences in preserved versus reduced ejection fraction. Circulation. 2016;133:484–92. doi: 10.1161/CIRCULATIONAHA.115.018614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Smit MD, Moes ML, Maass AH et al. The importance of whether atrial fibrillation or heart failure develops first. Eur J Heart Fail. 2012;14:1030–40. doi: 10.1093/eurjhf/hfs097. [DOI] [PubMed] [Google Scholar]
- 52.Lau DH, Schotten U, Mahajan R et al. Novel mechanisms in the pathogenesis of atrial fibrillation: practical applications. Eur Heart J. 2016;37:157–381. doi: 10.1093/eurheartj/ehv375. [DOI] [PubMed] [Google Scholar]
- 53.Alings M, Smit MD, Moes ML et al. Routine versus aggressive upstream rhythm control for prevention of early atrial fibrillation in heart failure: background, aims and design of the RACE 3 study. Neth Heart J. 2013;21:354–63. doi: 10.1007/s12471-013-0428-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Huxley RR, Lopez FL, Folsom AR et al. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123:1501–8. doi: 10.1161/CIRCULATIONAHA.110.009035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lau DH, Nattel S, Kalman JM, Sanders P. Modifiable risk factors and atrial fibrillation. Circulation. 2017;136:583–96. doi: 10.1161/CIRCULATIONAHA.116.023163. [DOI] [PubMed] [Google Scholar]
- 56.Manolis AJ, Rosei EA, Coca A et al. Hypertension and atrial fibrillation: diagnostic approach, prevention and treatment. Position paper of the Working Group ‘Hypertension Arrhythmias and Thrombosis’ of the European Society of Hypertension. J Hypertens. 2012;30:239–52. doi: 10.1097/HJH.0b013e32834f03bf. [DOI] [PubMed] [Google Scholar]
- 57.Benjamin EJ, Levy D, Vaziri SM et al. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA. 1994;271:840–4. [PubMed] [Google Scholar]
- 58.Perez MV, Wang PJ, Larson JC et al. Risk factors for atrial fibrillation and their population burden in postmenopausal women: the Women’s Health Initiative Observational Study. Heart. 2013;99:1173–8. doi: 10.1136/heartjnl-2013-303798. [DOI] [PubMed] [Google Scholar]
- 59.Dahlof B, Devereux RB, Kjeldsen SE et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet. 2002;359:995–1003. doi: 10.1016/S0140-6736(02)08089-3. [DOI] [PubMed] [Google Scholar]
- 60.Wachtell K, Lehto M, Gerdts E et al. Angiotensin II receptor blockade reduces new-onset atrial fibrillation and subsequent stroke compared to atenolol: the Losartan Intervention For End Point Reduction in Hypertension (LIFE) study. J Am Coll Cardiol. 2005;45:712–9. doi: 10.1016/jjacc.2004.10.068. [DOI] [PubMed] [Google Scholar]
- 61.Marott SC, Nielsen SF, Benn M, Nordestgaard BG. Antihypertensive treatment and risk of atrial fibrillation: a nationwide study. Eur Heart J. 2014;35:1205–14. doi: 10.1093/eurheartj/eht507. [DOI] [PubMed] [Google Scholar]
- 62.Pokushalov E, Romanov A, Katritsis DG et al. Renal denervation for improving outcomes of catheter ablation in patients with atrial fibrillation and hypertension: early experience. Heart Rhythm. 2014;11:1131–8. doi: 10.1016/j.hrthm.2014.03.055. [DOI] [PubMed] [Google Scholar]
- 63.Tsang TS, Gersh BJ, Appleton CP et al. Left ventricular diastolic dysfunction as a predictor of the first diagnosed nonvalvular atrial fibrillation in 840 elderly men and women. J Am Coll Cardiol. 2002;40:1636–44. doi: 10.1016/s0735-1097(02)02373-2. [DOI] [PubMed] [Google Scholar]
- 64.Marcus GM, Alonso A, Peralta CA et al. European ancestry as a risk factor for atrial fibrillation in African Americans. Circulation. 2010;122:2009–15. doi: 10.1161/CIRCULATIONAHA.110.958306. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Schnabel RB, Sullivan LM, Levy D et al. Development of a risk score for atrial fibrillation (Framingham Heart Study): a community-based cohort study. Lancet. 2009;373:739–45. doi: 10.1016/S0140-6736(09)60443-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Chamberlain AM, Agarwal SK, Folsom AR et al. A clinical risk score for atrial fibrillation in a biracial prospective cohort (from the Atherosclerosis Risk in Communities [ARIC] study) Am J Cardiol. 2011;107:85–91. doi: 10.1016/j.amjcard.2010.08.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Gammage MD, Parle JV, Holder RL et al. Association between serum free thyroxine concentration and atrial fibrillation. Arch Intern Med. 2007;167:928–34. doi: 10.1001/archinte.167.9.928. [DOI] [PubMed] [Google Scholar]
- 68.Maisel WH, Stevenson LW. Atrial fibrillation in heart failure: epidemiology, pathophysiology, and rationale for therapy. Am J Cardiol. 2003;91:2D–8D. doi: 10.1016/s0002-9149(02)03373-8. [DOI] [PubMed] [Google Scholar]
- 69.Kotecha D, Lam CS, Van Veldhuisen DJ et al. Heart failure with preserved ejection fraction and atrial fibrillation: vicious twins. J Am Coll Cardiol. 2016;68:2217–28. doi: 10.1016/jjacc.2016.08.048. [DOI] [PubMed] [Google Scholar]
- 70.Verma A, Kalman JM, Callans DJ. Treatment of patients with atrial fibrillation and heart failure with reduced ejection fraction. Circulation. 2017;135:1547–63. doi: 10.1161/CIRCULATIONAHA.116.026054. [DOI] [PubMed] [Google Scholar]
- 71.Swedberg K, Zannad F, McMurray JJV et al. Eplerenone and Atrial Fibrillation in Mild Systolic Heart Failure Results From the EMPHASIS-HF (Eplerenone in Mild Patients Hospitalization And SurvIval Study in Heart Failure) Study. J Am Coll Cardiol. 2012;59:1598–603. doi: 10.1016/jjacc.2011.11.063. [DOI] [PubMed] [Google Scholar]
- 72.Weijs B, Pisters R, Haest RJ et al. Patients originally diagnosed with idiopathic atrial fibrillation more often suffer from insidious coronary artery disease compared to healthy sinus rhythm controls. Heart Rhythm. 2012;9:1923–9. doi: 10.1016/j.hrthm.2012.08.013. [DOI] [PubMed] [Google Scholar]
- 73.Goto S, Hatt DL, Rother J et al. Prevalence, clinical profile, and cardiovascular outcomes of atrial fibrillation patients with atherothrombosis. Am Heart J. 2008;156:855–63. doi: 10.1016/j.ahj.2008.06.029. PubMed. [DOI] [PubMed] [Google Scholar]
- 74.Spronk HMH, De Jong AM, Verheule S et al. Hypercoagulability causes atrial fibrosis and promotes atrial fibrillation. Eurn Heart J. 2017;38:38–50. doi: 10.1093/eurheartj/ehw119. [DOI] [PubMed] [Google Scholar]
- 75.Karasoy D, Bo Jensen T, Hansen ML et al. Obesity is a risk factor for atrial fibrillation among fertile young women: a nationwide cohort study. Europace. 2013;15:781–6. doi: 10.1093/europace/eus422. [DOI] [PubMed] [Google Scholar]
- 76.Wang TJ, Parise H, Levy D et al. Obesity and the risk of new-onset atrial fibrillation. JAMA. 2004;292:2471–7. doi: 10.1001/jama.292.20.2471. [DOI] [PubMed] [Google Scholar]
- 77.Frost L, Hune LJ, Vestergaard P. Overweight and obesity as risk factors for atrial fibrillation or flutter: the Danish Diet, Cancer, and Health Study. Am J Med. 2005;118:489–95. doi: 10.1016/j.amjmed.2005.01.031. [DOI] [PubMed] [Google Scholar]
- 78.Dublin S, French B, Glazer NL et al. Risk of new-onset atrial fibrillation in relation to body mass index. Arch Intern Med. 2006;166:2322–8. doi: 10.1001/archinte.166.21.2322. [DOI] [PubMed] [Google Scholar]
- 79.Smith JG, Platonov PG, Hedblad B et al. Atrial fibrillation in the Malmo Diet and Cancer study: a study of occurrence, risk factors and diagnostic validity. Eur J Epidemiol. 2010;25:95–102. doi: 10.1007/s10654-009-9404-1. [DOI] [PubMed] [Google Scholar]
- 80.Tedrow UB, Conen D, Ridker PM et al. The long- and short-term impact of elevated body mass index on the risk of new atrial fibrillation the WHS (women’s health study) J Am Coll Cardiol. 2010;55:2319–27. doi: 10.1016/jjacc.2010.02.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Long MJ, Jiang CQ, Lam TH et al. Atrial fibrillation and obesity among older Chinese: the Guangzhou Biobank Cohort Study. Int J Cardiol. 2011;148:48–52. doi: 10.1016/jjjcard.2009.10.022. [DOI] [PubMed] [Google Scholar]
- 82.Frost L, Benjamin EJ, Fenger-Gron M et al. Body fat, body fat distribution, lean body mass and atrial fibrillation and flutter. A Danish cohort study. Obesity (Silver Spring). 2014;22:1546–52. doi: 10.1002/oby.20706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Wong CX, Sullivan T, Sun MT et al. Obesity and the risk of incident, post-operative, and post-ablation atrial fibrillation - a meta-analysis of 626,603 individuals in 51 studies. J Am Coll Cardiol EP. 2015;1:139–52. doi: 10.1016/jjacep.2015.04.004. [DOI] [PubMed] [Google Scholar]
- 84.Lassale C, Tzoulaki I, Moons KGM et al. Separate and combined associations of obesity and metabolic health with coronary heart disease: a pan-European case-cohort analysis. Eur Heart J. 2018;39:397–406. doi: 10.1093/eurheartj/ehx448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Van Gelder IC, Hobbelt AH, Brugemann J, Rienstra M. Time to implement fitness and reduction of fatness in atrial fibrillation therapy. Europace. 2017;19:513–4. doi: 10.1093/europace/euw287. [DOI] [PubMed] [Google Scholar]
- 86.Huxley RR, Alonso A, Lopez FL et al. Type 2 diabetes, glucose homeostasis and incident atrial fibrillation: the Atherosclerosis Risk in Communities study. Heart. 2012;98:133–8. doi: 10.1136/heartjnl-2011-300503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Pallisgaard JL, Schjerning AM, Lindhardt TB et al. Risk of atrial fibrillation in diabetes mellitus: A nationwide cohort study. Eur J Prev Cardiol. 2016;23:621–7. doi: 10.1177/2047487315599892. [DOI] [PubMed] [Google Scholar]
- 88.Dublin S, Glazer NL, Smith NL et al. Diabetes mellitus, glycemic control, and risk of atrial fibrillation. J Gen Intern Med. 2010;25:853–8. doi: 10.1007/s11606-010-1340-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Huxley RR, Filion KB, Konety S, Alonso A. Meta-analysis of cohort and case-control studies of type 2 diabetes mellitus and risk of atrial fibrillation. Am J Cardiol. 2011;108:56–62. doi: 10.1016/j.amjcard.2011.03.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Du X, Ninomiya T, de Galan B et al. Risks of cardiovascular events and effects of routine blood pressure lowering among patients with type 2 diabetes and atrial fibrillation: results of the ADVANCE study. Eur Heart J. 2009;30:1128–35. doi: 10.1093/eurheartj/ehp055. [DOI] [PubMed] [Google Scholar]
- 91.Goudis CA, Korantzopoulos P, Ntalas IV et al. Diabetes mellitus and atrial fibrillation: Pathophysiological mechanisms and potential upstream therapies. Int J Cardiol. 2015;184:617–22. doi: 10.1016/jjjcard.2015.03.052. [DOI] [PubMed] [Google Scholar]
- 92.Chang SH, Wu LS, Chiou MJ et al. Association of metformin with lower atrial fibrillation risk among patients with type 2 diabetes mellitus: a population-based dynamic cohort and in vitro studies. CardiovascDiabetol. 2014;13:123. doi: 10.1186/s12933-014-0123-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Piepoli MF, Hoes AW, Agewall S et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Eur Heart J. 2016;37:2315–81. doi: 10.1093/eurheartj/ehw106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Kodama S, Saito K, Tanaka S et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301:2024–35. doi: 10.1001/jama.2009.681. [DOI] [PubMed] [Google Scholar]
- 95.Qureshi WT, Alirhayim Z, Blaha MJ et al. Cardiorespiratory Fitness and Risk of Incident Atrial Fibrillation: Results From the Henry Ford Exercise Testing (FIT) Project. Circulation. 2015;131:1827–34. doi: 10.1161/CIRCULATIONAHA.114.014833. [DOI] [PubMed] [Google Scholar]
- 96.Drca N, Wolk A, Jensen-Urstad M, Larsson SC. Physical activity is associated with a reduced risk of atrial fibrillation in middle-aged and elderly women. Heart. 2015;101:1627–30. doi: 10.1136/heartjnl-2014-307145. [DOI] [PubMed] [Google Scholar]
- 97.Mozaffarian D, Furberg CD, Psaty BM, Siscovick D. Physical activity and incidence of atrial fibrillation in older adults: the cardiovascular health study. Circulation. 2008;118:800–7. doi: 10.1161/CIRCULATIONAHA.108.785626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Khan H, Kella D, Rauramaa R et al. Cardiorespiratory fitness and atrial fibrillation: A population-based follow-up study. Heart Rhythm. 2015;12:1424–30. doi: 10.1016/j.hrthm.2015.03.024. [DOI] [PubMed] [Google Scholar]
- 99.Drca N, Wolk A, Jensen-Urstad M, Larsson SC. Atrial fibrillation is associated with different levels of physical activity levels at different ages in men. Heart. 2014;10:1037–42. doi: 10.1136/heartjnl-2013-305304. [DOI] [PubMed] [Google Scholar]
- 100.Abdulla J, Nielsen JR. Is the risk of atrial fibrillation higher in athletes than in the general population? A systematic review and meta-analysis. Europace. 2009;11:1156–9. doi: 10.1093/europace/eup197. [DOI] [PubMed] [Google Scholar]
- 101.Elliott AD, Maatman B, Emery MS, Sanders P. The role of exercise in atrial fibrillation prevention and promotion: Finding optimal ranges for health. Heart Rhythm. 2017;1:1713–20. doi: 10.1016/j.hrthm.2017.07.001. [DOI] [PubMed] [Google Scholar]
- 102.Alonso A, Lopez FL, Matsushita K et al. Chronic kidney disease is associated with the incidence of atrial fibrillation: the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2011;123:2946–53. doi: 10.1161/CIRCULATIONAHA.111.020982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Marcos EG, Geelhoed B, Van Der Harst P et al. Relation of renal dysfunction with incident atrial fibrillation and cardiovascular morbidity and mortality: The PREVEND study Europace. 2017;19:1930–6. doi: 10.1093/europace/euw373. [DOI] [PubMed] [Google Scholar]
- 104.Baber U, Howard VJ, Halperin JL et al. Association of chronic kidney disease with atrial fibrillation among adults in the United States: REasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Circ Arrhythm Electrophysiol. 2011;4:26–32. doi: 10.1161/CIRCEP110.957100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Emdin CA, Anderson SG, Salimi-Khorshidi G et al. Usual blood pressure, atrial fibrillation and vascular risk: evidence from 4.3 million adults. Int J Epidemiol. 2017;46:162–72. doi: 10.1093/ije/dyw053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Odutayo A, Wong CX, Hsiao AJ et al. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: systematic review and meta-analysis. BMJ. 2016;354:i4482. doi: 10.1136/bmj.i4482. [DOI] [PubMed] [Google Scholar]
- 107.Lee M, Saver JL, Chang KH et al. Low glomerular filtration rate and risk of stroke: meta-analysis. BMJ. 2010;341:c4249. doi: 10.1136/bmj.c4249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Kottgen A, Russell SD, Loehr LR et al. Reduced kidney function as a risk factor for incident heart failure: the atherosclerosis risk in communities (ARIC) study. J Am Soc Nephrol. 2007;18:1307–15. doi: 10.1681/ASN.2006101159. [DOI] [PubMed] [Google Scholar]
- 109.Piccini JP, Stevens SR, Chang Y et al. Renal dysfunction as a predictor of stroke and systemic embolism in patients with nonvalvular atrial fibrillation: validation of the R(2)CHADS(2) index in the ROCKET AF (Rivaroxaban Once-daily, oral, direct factor Xa inhibition Compared with vitamin K antagonism for prevention of stroke and Embolism Trial in Atrial Fibrillation) and ATRIA (AnTicoagulation and Risk factors In Atrial fibrillation) study cohorts. Circulation. 2013;127:224–32. doi: 10.1161/CIRCULATIONAHA.112.107128. [DOI] [PubMed] [Google Scholar]
- 110.Lau YC, Proietti M, Guiducci E et al. Atrial fibrillation and thromboembolism in patients with chronic kidney disease. J Am Coll Cardiol. 2016;68:1452–64. doi: 10.1016/jjacc.2016.06.057. Epub 2016/09/24. [DOI] [PubMed] [Google Scholar]
- 111.Jha V, Garcia-Garcia G, Iseki K et al. Chronic kidney disease: global dimension and perspectives. Lancet. 2013;382:260–72. doi: 10.1016/S0140-6736(13)60687-X. [DOI] [PubMed] [Google Scholar]
- 112.Kloosterman M, Rienstra M, Crijns HJ et al. The left atrium: An overlooked prognostic tool. Eur J Prev Cardiol. 2017;24:389–91. doi: 10.1177/2047487316686633. [DOI] [PubMed] [Google Scholar]
- 113.Goette A, Kalman JM, Aguinaga L et al. EHRA/HRS/APHRS/SOLAECE expert consensus on atrial cardiomyopathies: definition, characterization, and clinical implication. Europace. 2016;18:1455–90. doi: 10.1093/europace/euw161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Hirsh BJ, Copeland-Halperin RS, Halperin JL. Fibrotic atrial cardiomyopathy, atrial fibrillation, and thromboembolism: mechanistic links and clinical inferences. J Am Coll Cardiol. 2015;65:2239–51. doi: 10.1016/jjacc.2015.03.557. [DOI] [PubMed] [Google Scholar]
- 115.Kottkamp H. Human atrial fibrillation substrate: towards a specific fibrotic atrial cardiomyopathy. Eur Heart J. 2013;34:2731–8. doi: 10.1093/eurheartj/eht194. [DOI] [PubMed] [Google Scholar]
- 116.Stehouwer CD, Smulders YM. Microalbuminuria and risk for cardiovascular disease: Analysis of potential mechanisms. J Am Soc Nephrol. 2006;17:2106–11. doi: 10.1681/ASN.2005121288. [DOI] [PubMed] [Google Scholar]
- 117.Somers VK, White DP, Amin R et al. Sleep apnea and cardiovascular disease: an American Heart Association/ american College Of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council On Cardiovascular Nursing. In collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health) Circulation. 2008;118:1080–111. doi: 10.1161/CIRCULATIONAHA.107.189375. [DOI] [PubMed] [Google Scholar]
- 118.Peppard PE, Young T, Barnet JH et al. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. 2013;177:1006–14. doi: 10.1093/aje/kws342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 119.Gami AS, Pressman G, Caples SM et al. Association of atrial fibrillation and obstructive sleep apnea. Circulation. 2004;110:364–7. doi: 10.1161/01.CIR.0000136587.68725.8E. [DOI] [PubMed] [Google Scholar]
- 120.Stevenson IH, Teichtahl H, Cunnington D et al. Prevalence of sleep disordered breathing in paroxysmal and persistent atrial fibrillation patients with normal left ventricular function. Eur Heart J. 2008;29:1662–9. doi: 10.1093/eurheartj/ehn214. Epub 2008/06/03. [DOI] [PubMed] [Google Scholar]
- 121.Gami AS, Hodge DO, Herges RM et al. Obstructive sleep apnea, obesity, and the risk of incident atrial fibrillation. J Am Coll Cardiol. 2007;49:565–71. doi: 10.1016/jjacc.2006.08.060. [DOI] [PubMed] [Google Scholar]
- 122.Cadby G, McArdle N, Briffa T et al. Severity of OSA is an independent predictor of incident atrial fibrillation hospitalization in a large sleep-clinic cohort. Chest. 2015;148:945–52. doi: 10.1378/chest.15-0229. [DOI] [PubMed] [Google Scholar]
- 123.Fein AS, Shvilkin A, Shah D et al. Treatment of obstructive sleep apnea reduces the risk of atrial fibrillation recurrence after catheter ablation. J Am Coll Cardiol. 2013;62:300–5. doi: 10.1016/jjacc.2013.03.052. [DOI] [PubMed] [Google Scholar]
- 124.Marti-Soler H, Hirotsu C, Marques-Vidal P et al. The NoSAS score for screening of sleep-disordered breathing: a derivation and validation study. Lancet Respir Med. 2016;4:742–8. doi: 10.1016/S2213-2600(16)30075-3. [DOI] [PubMed] [Google Scholar]
- 125.Ettinger PO, Wu CF, De La Cruz C, Jr et al. Arrhythmias and the “Holiday Heart”: alcohol-associated cardiac rhythm disorders. Am Heart J. 1978;95:555–62. doi: 10.1016/0002-8703(78)90296-x. [DOI] [PubMed] [Google Scholar]
- 126.Liang Y, Mente A, Yusuf S et al. Alcohol consumption and the risk of incident atrial fibrillation among people with cardiovascular disease. CMAJ. 2012;184:E857–66. doi: 10.1503/cmaj.120412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Djousse L, Levy D, Benjamin EJ et al. Long-term alcohol consumption and the risk of atrial fibrillation in the Framingham Study. Am J Cardiol. 2004;93:710–3. doi: 10.1016/j.amjcard.2003.12.004. [DOI] [PubMed] [Google Scholar]
- 128.Mukamal KJ, Tolstrup JS, Friberg J et al. Alcohol consumption and risk of atrial fibrillation in men and women: the Copenhagen City Heart Study. Circulation. 2005;112:1736–42. doi: 10.1161/CIRCULATIONAHA.105.547844. [DOI] [PubMed] [Google Scholar]
- 129.Conen D, Tedrow UB, Cook NR et al. Alcohol consumption and risk of incident atrial fibrillation in women. JAMA. 2008;300:2489–96. doi: 10.1001/jama.2008.755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Larsson SC, Drca N, Wolk A. Alcohol consumption and risk of atrial fibrillation: a prospective study and dose-response meta-analysis. J Am Coll Cardiol. 2014;64:281–9. doi: 10.1016/jjacc.2014.03.048. [DOI] [PubMed] [Google Scholar]
- 131.Kodama S, Saito K, Tanaka S et al. Alcohol consumption and risk of atrial fibrillation: a meta-analysis. J Am Coll Cardiol. 2011;57:427–36. doi: 10.1016/jjacc.2010.08.641. [DOI] [PubMed] [Google Scholar]
- 132.Heeringa J, Kors JA, Hofman A et al. Cigarette smoking and risk of atrial fibrillation: the Rotterdam Study. Am Heart J. 2008;156:1163–9. doi: 10.1016/j.ahj.2008.08.003. [DOI] [PubMed] [Google Scholar]
- 133.Chamberlain AM, Agarwal SK, Folsom AR et al. Smoking and incidence of atrial fibrillation: results from the Atherosclerosis Risk in Communities (ARIC) study. Heart Rhythm. 2011;8:1160–6. doi: 10.1016/j.hrthm.2011.03.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Friberg J, Buch P, Scharling H et al. Rising rates of hospital admissions for atrial fibrillation. Epidemiology. 2003;14:666–72. doi: 10.1097/01.ede.0000091649.26364.c0. [DOI] [PubMed] [Google Scholar]
- 135.Pfister R, Bragelmann J, Michels G et al. Performance of the CHARGE-AF risk model for incident atrial fibrillation in the EPIC Norfolk cohort. Eur J Prev Cardiol. 2015;22:932–9. doi: 10.1177/2047487314544045. [DOI] [PubMed] [Google Scholar]
- 136.Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998;82:2N–9N. doi: 10.1016/s0002-9149(98)00583-9. [DOI] [PubMed] [Google Scholar]
- 137.Stewart S, Hart CL, Hole DJ, McMurray JJ. Population prevalence, incidence, and predictors of atrial fibrillation in the Renfrew/Paisley study. Heart. 2001;86:516–21. doi: 10.1136/heart.86.5.516. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 138.Psaty BM, Manolio TA, Kuller LH et al. Incidence of and risk factors for atrial fibrillation in older adults. Circulation. 1997;96:2455–61. doi: 10.1161/01.cir.96.7.2455. [DOI] [PubMed] [Google Scholar]
- 139.Knuiman M, Briffa T, Divitini M et al. A cohort study examination of established and emerging risk factors for atrial fibrillation: the Busselton Health Study. Eur J Epidemiol. 2014;29:181–90. doi: 10.1007/s10654-013-9875-y. [DOI] [PubMed] [Google Scholar]
- 140.Lopez FL, Agarwal SK, Maclehose RF et al. Blood lipid levels, lipid-lowering medications, and the incidence of atrial fibrillation: the atherosclerosis risk in communities study. Circ Arrhythm Electrophysiol. 2012;5:155–62. doi: 10.1161/CIRCEP111.966804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Mora S, Akinkuolie AO, Sandhu RK et al. Paradoxical association of lipoprotein measures with incident atrial fibrillation. Circ Arrhythm Electrophysiol. 2014;7:612–9. doi: 10.1161/CIRCEP113.001378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Watanabe H, Tanabe N, Yagihara N et al. Association between lipid profile and risk of atrial fibrillation. Circ J. 2011;75:2767–74. doi: 10.1253/circj.cj-11-0780. [DOI] [PubMed] [Google Scholar]
- 143.Alonso A, Yin X, Roetker NS et al. Blood lipids and the incidence of atrial fibrillation: the Multi-Ethnic Study of Atherosclerosis and the Framingham Heart Study. J Am Heart Assoc. 2014;3:e001211. doi: 10.1161/JAHA.114.001211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 144.Haywood LJ, Ford CE, Crow RS et al. Atrial fibrillation at baseline and during follow-up in ALLHAT (Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial) J Am Coll Cardiol. 2009;54:2023–31. doi: 10.1016/jjacc.2009.08.020. [DOI] [PubMed] [Google Scholar]
- 145.Pol T, Held C, Westerbergh J et al. Dyslipidemia and Risk of Cardiovascular Events in Patients With Atrial Fibrillation Treated With Oral Anticoagulation Therapy: Insights From the ARISTOTLE (Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation) Trial. J Am Heart Assoc. 2018;7 doi: 10.1161/JAHA.117.007444. epub ahead of press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Savelieva I, Kakouros N, Kourliouros A, Camm AJ. Upstream therapies for management of atrial fibrillation: review of clinical evidence and implications for European Society of Cardiology guidelines. Part I: primary prevention. Europace. 2011;13:308–28. doi: 10.1093/europace/eur002. [DOI] [PubMed] [Google Scholar]
- 147.Zheng Z, Jayaram R, Jiang L et al. Perioperative Rosuvastatin in Cardiac Surgery. N Engl J Med. 2016;374:174–453. doi: 10.1056/NEJMoa1507750. [DOI] [PubMed] [Google Scholar]
- 148.Camm AJ, Amarenco P, Haas S et al. XANTUS: a real-world, prospective, observational study of patients treated with rivaroxaban for stroke prevention in atrial fibrillation. Eur Heart J. 2016;37:1145–53. doi: 10.1093/eurheartj/ehv466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 149.Kirchhof P, Ammentorp B, Darius H et al. Management of atrial fibrillation in seven European countries after the publication of the 2010 ESC Guidelines on atrial fibrillation: primary results of the PREvention oF thromboemolic events - European Registry in Atrial Fibrillation (PREFER in AF) Europace. 2014;16:6–14. doi: 10.1093/europace/eut263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 150.Lip GY, Laroche C, Ioachim PM et al. Prognosis and treatment of atrial fibrillation patients by European cardiologists: one year follow-up of the EURObservational Research Programme-Atrial Fibrillation General Registry Pilot Phase (EORP-AF Pilot registry) Eur Heart J. 2014;35:3365–76. doi: 10.1093/eurheartj/ehu374. [DOI] [PubMed] [Google Scholar]
- 151.Kirchhof P The future of atrial fibrillation management: integrated care and stratified therapy. Lancet. 2017;390:1873–87. doi: 10.1016/S0140-6736(17)31072-3. [DOI] [PubMed] [Google Scholar]
- 152.Ganesan AN, Shipp NJ, Brooks AG et al. Long-term outcomes of catheter ablation of atrial fibrillation: a systematic review and meta-analysis. J Am Heart Assoc. 2013;2:e004549. doi: 10.1161/JAHA.112.004549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Teh AW, Kistler PM, Lee G et al. Long-term effects of catheter ablation for lone atrial fibrillation: progressive atrial electroanatomic substrate remodeling despite successful ablation. Heart Rhythm. 2012;9:473–80. doi: 10.1016/j.hrthm.2011.11.013. [DOI] [PubMed] [Google Scholar]
- 154.Pavlovic D, Kirchhof P, Fabritz L. The RACE-3 is on: double-locking sinus rhythm by upstream and downstream therapy. Eur Heart J. 2018. epub ahead of press. [DOI] [PMC free article] [PubMed]
- 155.Kirchhof P, Curtis AB, Skanes AC et al. Atrial fibrillation guidelines across the Atlantic: a comparison of the current recommendations of the European Society of Cardiology/ European Heart Rhythm Association/European Association of Cardiothoracic Surgeons, the American College of Cardiology Foundation/American Heart Association/Heart Rhythm Society, and the Canadian Cardiovascular Society. Eur Heart J. 2013;34:1471–4. doi: 10.1093/eurheartj/ehs446. [DOI] [PubMed] [Google Scholar]
- 156.Nattel S, Harada M. Atrial remodeling and atrial fibrillation: recent advances and translational perspectives. J Am Coll Cardiol. 2014;63:2335–45. doi: 10.1016/jjacc.2014.02.555. [DOI] [PubMed] [Google Scholar]
- 157.Savelieva I, Kakouros N, Kourliouros A, Camm AJ. Upstream therapies for management of atrial fibrillation: review of clinical evidence and implications for European Society of Cardiology guidelines. Part II: secondary prevention. Europace. 2011;13:610–25. doi: 10.1093/europace/eur023. [DOI] [PubMed] [Google Scholar]
- 158.Disertori M, Latini R, Barlera S et al. Valsartan for prevention of recurrent atrial fibrillation. N Engl J Med. 2009;360:1606–17. doi: 10.1056/NEJMoa0805710. GISSI-AF Investigators. [DOI] [PubMed] [Google Scholar]
- 159.Yusuf S, Healey JS, Pogue J, Chrolavicius S, Flather M et al. Irbesartan in patients with atrial fibrillation. N Engl J Med. 2011;364:928–38. doi: 10.1056/NEJMoa1008816. ACTIVE I Investigators. [DOI] [PubMed] [Google Scholar]
- 160.Goette A, Schon N, Kirchhof P et al. Angiotensin II-antagonist in paroxysmal atrial fibrillation (ANTIPAF) trial. Circ Arrhythm Electrophysiol. 2012;5:43–51. doi: 10.1161/CIRCEP111.965178. [DOI] [PubMed] [Google Scholar]
- 161.Almroth H, Hoglund N, Boman K et al. Atorvastatin and persistent atrial fibrillation following cardioversion: a randomized placebo-controlled multicentre study. Eur Heart J. 2009;30:827–33. doi: 10.1093/eurheartj/ehp006. [DOI] [PubMed] [Google Scholar]
- 162.Abed HS, Wittert GA, Leong DP et al. Effect of weight reduction and cardiometabolic risk factor management on symptom burden and severity in patients with atrial fibrillation: a randomized clinical trial. JAMA. 2013;310:2050–60. doi: 10.1001/jama.2013.280521. [DOI] [PubMed] [Google Scholar]
- 163.Abed HS, Nelson AJ, Richardson JD et al. Impact of weight reduction on pericardial adipose tissue and cardiac structure in patients with atrial fibrillation. Am Heart J. 2015;169:655–62 e2. doi: 10.1016/j.ahj.2015.02.008. [DOI] [PubMed] [Google Scholar]
- 164.Pathak RK, Middeldorp ME, Meredith M et al. Long-Term Effect of Goal-Directed Weight Management in an Atrial Fibrillation Cohort: A Long-Term Follow-Up Study (LEGACY) J Am Coll Cardiol. 2015;65:2159–69. doi: 10.1016/jjacc.2015.03.002. [DOI] [PubMed] [Google Scholar]
- 165.Pathak RK, Middeldorp ME, Lau DH et al. Aggressive risk factor reduction study for atrial fibrillation and implications for the outcome of ablation: the ARREST-AF cohort study. J Am Coll Cardiol. 2014;64:2222–31. doi: 10.1016/jjacc.2014.09.028. [DOI] [PubMed] [Google Scholar]
- 166.Fioravanti F, Brisinda D, Sorbo AR, Fenici R. BMI reduction decreases AF recurrence rate in a Mediterranean cohort. J Am Coll Cardiol. 2015;66:2264–5. doi: 10.1016/jjacc.2015.07.084. [DOI] [PubMed] [Google Scholar]
- 167.Pathak RK, Elliott A, Middeldorp ME et al. Impact of CARDIOrespiratory FITness on Arrhythmia Recurrence in Obese Individuals With Atrial Fibrillation: The CARDIO-FIT Study. J Am Coll Cardiol. 2015;66:985–96. doi: 10.1016/jjacc.2015.06.488. [DOI] [PubMed] [Google Scholar]
- 168.Berti D, Hendriks JM, Brandes A et al. A proposal for interdisciplinary, nurse-coordinated atrial fibrillation expert programmes as a way to structure daily practice. Eur Heart J. 2013;34:2725–30. doi: 10.1093/eurheartj/eht096. [DOI] [PubMed] [Google Scholar]
- 169.Hendriks JM, de Wit R, Crijns HJ et al. Nurse-led care vs. usual care for patients with atrial fibrillation: results of a randomized trial of integrated chronic care vs. routine clinical care in ambulatory patients with atrial fibrillation. Eur Heart J. 2012;33:2692–9. doi: 10.1093/eurheartj/ehs071. [DOI] [PubMed] [Google Scholar]
- 170.Stewart S, Ball J, Horowitz JD et al. Standard versus atrial fibrillation-specific management strategy (SAFETY) to reduce recurrent admission and prolong survival: pragmatic, multicentre, randomised controlled trial. Lancet. 2015;385:775–84. doi: 10.1016/S0140-6736(14)61992-9. [DOI] [PubMed] [Google Scholar]
- 171.Carter L, Gardner M, Magee K et al. An integrated management approach to atrial fibrillation. J Am Heart Assoc. 2016;5:pii:e002950. doi: 10.1161/JAHA.115.002950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 172.Kirchhof P, Breithardt G, Camm AJ et al. Improving outcomes in patients with atrial fibrillation: rationale and design of the Early treatment of Atrial fibrillation for Stroke prevention Trial. Am Heart J. 2013;166:442–8. doi: 10.1016/j.ahj.2013.05.015. [DOI] [PubMed] [Google Scholar]
- 173.Whelton PK, Carey RM, Aronow WS et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;pii(17):S0735–1097. doi: 10.1016/j.jacc.2017.11.006. 41518-X. [DOI] [PubMed] [Google Scholar]
- 174.Jensen MD, Ryan DH, Apovian CM et al. 2013 AHA/ACC/TOS guideline for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and The Obesity Society. J Am Coll Cardiol. 2014;63:2985–3023. doi: 10.1016/jjacc.2013.11.004. [DOI] [PubMed] [Google Scholar]
- 175.Stone NJ, Robinson JG, Lichtenstein AH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;6:2889–934. doi: 10.1016/jjacc.2013.11.002. [DOI] [PubMed] [Google Scholar]
- 176.Smith SC, Benjamin EJ, Bonow RO et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation endorsed by the World Heart Federation and the Preventive Cardiovascular Nurses Association. J Am Coll Cardiol. 2011;58:2432–46. doi: 10.1016/j.jacc.2011.10.824. [DOI] [PubMed] [Google Scholar]